Mental State Examination Form (MSE)
advertisement
")
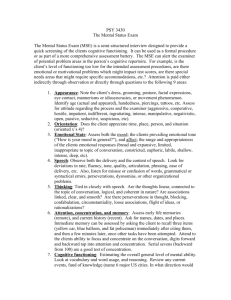
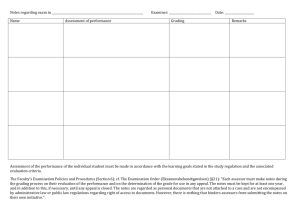
MENTAL STATE EXAMINATION FORM _____________________________________________________________________ Appearance and behaviour: Physical appearance? Reaction to situation? _____________________________________________________________________ Speech: Rate, volume and quantity of information? _____________________________________________________________________ Mood and affect: Mood? Affect? _____________________________________________________________________ Form of thought: Amount and rate of thought? Continuity of ideas? _____________________________________________________________________ Though content: Delusions? Suicidal thoughts? Other? _____________________________________________________________________ Perception: Hallucinations? Other perceptual disturbances? _____________________________________________________________________ Sensorium and cognitions: Level of consciousness? Memory? Orientation? Concentration? Abstract thoughts? _____________________________________________________________________ Insight _____________________________________________________________________ OVERVIEW OF THE MENTAL STATE EXAMINATION (MSE) 1. Appearance and behaviour Appearance eg grooming, hygiene, clothing, hair, nails, other significant features Attitude to situation and examiner eg hostile, withdrawn, seductive Motor behaviour eg slowed down, restless, tremors, bizarre ( include description) 2. Speech Rate eg slow, pressured (very rapid), monotonous Volume eg loud, quiet, slurred Quantity of information eg restricted amount of spontaneous speech 3. Mood and affect Mood eg depressed, euphoric, suspicious, labile - (alternating between extremes) Affect eg restricted, flattened (absence of emotional expression) inappropriate 4. Form of thought Amount of thought and rate of production eg hestitant thinking, vague, flight of ideas Continuity of ideas - refers to logical order of the flow of ideas Disturbance in language or meaning eg uses words that don't exist or word salad 5. Content of thought Delusions (particular problems arise from delusions of persecution, poisoning) Suicidal thoughts, plans or intent Other - eg obsessions, compulsions, hypochondriacal preoccupations 6. Perception Hallucinations relating to sounds heard, visions, smells, tastes, tactile or somatic sensations. Note in particular any command hallucinations. Does the patient think that he or she may act upon these? Other perceptual disturbances (derealisation, depersonalisation, heightened/dulled perception) 7. Sensorium and cognition Level of consciousness eg abnormal drowsiness, delirium, clouding of consciousness Memory: immediate, recent, remote Orientation: time, place, person Concentration: ask the individual to subtract serial 7s from 100 Abstract thinking 8. Insight Extent of individual's awareness of problem. Compliance with treatment. The Mental State Examination is designed to obtain information about specific aspects of the individual's mental experiences and behaviour at the time of the interview. The MSE may also be used if the clinician feels that an individual under his or her care may be experiencing a relapse of illness. This book does not attempt to explain how to carry out a mental state examination. None-the-less, the following general guidance can be given: The mental state exam form provides a structure that encourages the examiner to record his or her observations of the patient. The form is often filled in after the conversation with the patient has been completed. The actual conversation that the examiner has with the patient, while carrying out these observations, should not consist of a series of direct questions. More than a few direct questions turns the conversation into an interrogation and may be counter-productive. Mental state examinations are normally carried out where the person examined is distressed. The first part of the conversation must indicate that the examiner understands that the patient is distressed and that the reasons for the distress will be listened to sympathetically. Whether the conversation is exploring the patient's history or present distress, it is about topics that are meaningful and personal to the patient (their story). The patient needs to understand that the purpose of the exercise is for help to be arranged for him or her by the person carrying out the examination. An atmosphere must be created that will encourage the patient to feel free to share his/her inner feelings, and be able to talk without fear of being criticised or judged. Privacy is of great importance in creating this atmosphere and so is confidentiality. The limits of confidentiality should be explained to the patient. If the patient is reluctant to discuss his or her feelings and thoughts, direct questions are not likely to produce further results. Indirect probes may help, for example - "If you could have three wishes granted right now, what would they be?' Most patients will respond to this kind of indirect, open-ended question and provide the examiner with conversational points which can be explored further. "Why's that?" is a useful further question to keep the conversation going when blocks occur. Where possible, mental state examinations are better carried out over two or three interviews rather than all at once. Except in an acute emergency (for example, where it is thought that the patient may be harbouring ideas of serious violence) where persistence will be necessary, the most important outcome of any mental state examination is that, at the end, the examiner has a better idea of what the patient is thinking and feeling and the patient trusts the examiner and is willing to continue the conversation at a later date.