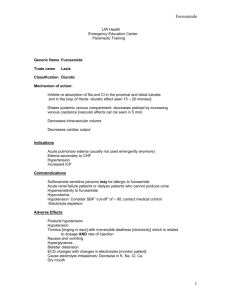
Lasix (furosemide) for Renal Scan Orders
advertisement
 for Renal Scan Orders")
PLACE LABEL HERE LASIX (furosemide) for RENAL SCAN ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). ALLERGIES: _____________________________________________________________________ 1. Start INT 2. Obtain vital signs pre and post administration of Lasix (furosemide) 3. Lasix (furosemide) 0.5 mg/kg IV push over 2 – 3 min Patient weight = ______ kg x 0.5 mg/kg = _______ mg (maximum dose 40 mg) 4. Remove INT prior to discharge 5. Discharge home if criteria met (Outpatients) OR Return to floor (Inpatients) ADDITIONAL ORDERS: ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________ Date ___________________ Time _________________________________ Physician Signature __________ PID Number Send copy to pharmacy *1-33216* FORM 1-33216 INITIATED 04/2013 Page 1 of 1