Y5 Preparation for Practice - Central Manchester University
advertisement

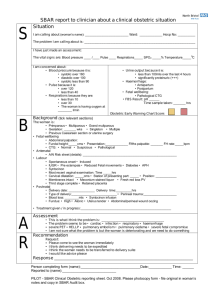
PREPARATION FOR PRACTICE LEARNING HOW TO COMMUNICATE AND MANAGE SITUATIONS AS A FOUNDATION DOCTOR, WITH PATIENTS, RELATIVES AND COLLEAGUES. A COMMUNICATION TEACHING SESSION FOR YEAR 5 MEDICAL STUDENTS Original author: C Chew-Graham Revisions: Mark Perry on behalf of the Communication Education team and others June 2012 Please send any suggestions for changes to: communication. admin@manchester.ac.uk 1 CONTENTS and SCENARIO / CASE SUMMARY LIST pages Introduction, ILOs, outline, materials Session 1 Session 2 Case 1. Shift Handover using SBAR: student worksheets – copies for all Case 2: Apology and Negotiate Admission student instructions SP role Case 3: Telephone Negotiation with colleague Doctor instructions Radiographer instructions Case 4A: Emergency Handover student instructions F1 task Nurse task (4 copies of EACH for students) 3-4 5-9 10-11 12 Case 4B: Adverse Event student instructions SP role Case 5: Breaking Bad News and Informed Consent (stent) student instructions SP role LUNCH Case 6: Confidentiality and Relatives student instructions SP role Case 7 DNAR discussion Case 8: Breaking Bad News – Death student instructions SP role Case 9: Team handling of Complaint / Coroner discussion student instructions SP role Case 10: SELF CARE Discussion – see also session plan Resource Sheet for tutors and students SBAR handout 12-14 15 16 17 18 19 20 21-22 23 24 25 26 27 28 29 30 31 32 33 34 2 Introduction: In the two-session Year 5 Foundation Dr course (usually done in one full day), the tutor should meet specific learning objectives (below and listed in the session plan) while also attending to additional needs. The day follows a patient journey. It should consolidate students’ communication, and introduce new aspects needed as a foundation trainee. Each session should be time-tabled over 3 hours 15 minutes Changes for 2012-13 (shown in bold) Since students should now get more practice Breaking Bad News in Cancer elsewhere, case 3 (am) We introduce 2 scenarios on Handover and Students should have prepared for SBAR discussion. So the day now opens with a Shift handover (was in afternoon 2011-12), before we meet an irritated patient whose investigation has not been pre-booked. Later Case 4 is on emergency Handover using SBAR (see student handouts p34) and exploring drug concordance and managing adverse events (resource sheet p33). We introduce an Adverse event in order to initiate discussion on ‘Open Disclosure’ in a less threatening way. It is more important to consider how we can learn from and prevent such events in an often unfriendly or ‘blame’ culture than to focus on labels like ‘error’. There are minor changes to the story timing. Intended learning outcomes: Specific Intended Learning Outcomes for year 5 Clinical Communication teaching are: Learning to communicate as a Foundation Dr with patients, carers, colleagues Developing personal management skills in clinical work Development of telephone skills Preventing and managing adverse events / ‘critical incidents’ Taking appropriate responsibility for adverse events / error within teams Ability to give and receive Handover (both planned and emergency) Using peer review and self-audit eg. on sensitisation to ‘blame cultures’ These come from the Communication ILOs as follows: Y 5.1 demonstrate consultation behaviour that ensures information needed for clinical decision-making will be obtained whilst respecting the patient's autonomy, dignity and privacy. [S.2,S.3,S.4,A.5, A.9] Y 5.2 demonstrate the ability to communicate under pressure and in emergency situations. [A.5] Y5.3 demonstrate consultation behaviour that ensures the patient and/or a carer is in concordance with the nature of the problem and the plan to manage it [S.7, A.5] Y5.8 demonstrate a commitment to self-analysis and peer review of professional status and personal communication throughout a medical career [A.1, A.2, A.3, A.4] Yr 5.10 demonstrate the attitude, even when under pressure, that all patients have a right to respect however difficult they are to communicate with. [A.5, A.8,A.9] There may be outstanding objectives from earlier years which also need to be addressed: shared decision-making, explaining risk and negotiating management breaking bad news coping with personal feelings 3 Course outline Lead Tutor: Briefing for Tutors and SPs: To highlight changes and timing. Lead Tutor: (Introductory plenary – Optional, as may be done in small groups): Outline the format of the day, following a patient ‘journey’ and objectives (Powerpoint): to review previous learning and add some team skills, especially on Handover. Describe the methods - using role-play and simulated patients. Give a reminder of rules of group-work and feedback. Group forming (up to 10 students per group, with one facilitator). Each group will have a 10 minute introduction and ice breaker followed by 10 minutes to encourage students to express their own learning needs. The tutor reviews the learning methods. It is helpful to list the objectives as ‘tasks’ – (see Page 2 or facilitator’s session plan pages 5-11) link students to the tasks throughout the day. The issues of confidentiality and safety should be raised, as well as "house-keeping". Watch out for students’ personal feelings! Discussion of situations in which students may have experienced difficulties should occur naturally through the day. Following the feedback after each scenario, all the group tasks should be covered by discussion. Facilitators should keep the focus on communication, but students may note ethical issues to explore related learning needs later. Role play. Attached are the scenarios. 1 – 5 to be covered using an SP ‘patient’ in the morning session, while a ‘relative’ enters the scene for the afternoon session, scenarios 6 - 10. At this stage students often value increasing challenge in role play, such as strong emotions from the SP; this should be negotiated with each student in advance. All scenarios require preparatory discussion by the group and/or input of resources by the tutor. Preparation: Tutors to prepare using the resources eg handout on SBAR and DNAR article (with tutor pack) Please watch the student preparatory material on Handover, a short series of film clips demonstrating communication, first without SBAR and then when using it, http://www.institute.nhs.uk/safer_care/safer_care/situation_background_assessment_recommend ation.html. Final discussion within each group to review the learning, reflect on issues raised, prioritise future learning needs and plan how to address them. NB Students may want to attend a Morbidity / Mortality or Critical Incident review in hospital or GP practice. Foundation Doctors should now discuss anonymised adverse events in small groups from February to July each year in all Trusts in the NW Deanery under ‘Lessons Learnt’. Preparation and Materials required Email students with the resource sheet and SBAR: Dear Student. The F1 day starts with the group work and it is very important that you prepare for this session. Please watch the materials on SBAR (Situation Background Recommendation Assessment) especially the Escalation scenarios and Acute handover at the link below. Ensure you know how Escalation and Readback work. http://www.institute.nhs.uk/safer_care/safer_care.html One tutor per approx 10 students, an older simulated patient for the morning and a different younger one as the son / daughter for the afternoon Room with flipchart/pens Sticky labels for name badges Copies of doctor roles/student instructions – pages 12, 13, 15, 16, 17, 18, 19, 21, 23, 26, 27, 29 Resource and SBAR sheet for tutors and students (pages 33 & 34 )DNAR article Hospital/ DoH consent form (see page 8, case 5) Copies of SP roles – pages 14, 20, 22, 24, 28, 30 4 Copies of: Both Nurse and F1 roles p 17 and p18 and Handover Practice cases p26 & 27 Evaluation forms 4 Group work SESSION 1 TIME CASE TYPE Start 0 Takes 20 mins INDIVIDUAL TASK for student roleplaying F1 Into groups GROUP TASK / TUTOR NOTES and RESOURCES (italicised) Tutor to ice-break and negotiate individual learning objectives and connect to listed tasks for the day. Negotiate how students want to give and receive feedback – (as long as they are constructive, include positives, are specific, use detailed description, offer alternatives and own their feedback). They can use Pendleton’s rules (positives then do differently), or chronological feedback or gut reaction. Remind group of the use of the PAUSE BUTTON – a positive tool that shows they are really thinking about what they are doing. 5 Start +20 Takes 20 mins To introduce SBAR and practice a shift handover Introduce SBAR – (check that students have looked at pre-course material). So ask them to explain and for learning from the NHS institute material and personal experiences: observations of Team Handover? Use of printed lists? Systems used? Pages The SBAR routine provides 1. structure for the ‘giver’ and a way to escalate urgency. 2. enables the handover ‘recipient’ to mentally check and then challenge incomplete or unclear details How? Clarify SBAR (see student Handout p34: Identify the elements: Situation (Identify self and patient, location, then immediate problem) – Background (relevant history) – Assessment (observations, signs and any urgent results) – Recommendation / Readback (Explain what you need be specific about request and time frame; Make suggestions; Clarify expectations ) Put students into Trios or fours, outline task below and give out copies of patient data - next two pages one per student. EXPLAIN CONTEXT: As Giver you are just ending your shift and have been busy admitting several patients. You want to agree priorities with your colleague. Receiver: You have just arrived at hospital and are coming on to the a.m. shift. You are taking Handover from your colleague (Then going to clerk new patients under your Consultant - Case 2) NB BOTH Giver and Receiver to use SBAR, to clarify they have all the information that they need. The Receiver should check Recommendation by using Readback REPEAT so 2/3 students have practiced and made notes on peer feedback. REMIND that they will all do more practice later on. 6 Start +40 takes 30 mins to negotiate admission with Patient Case 1 SP pages 12-14 Start +70 to negotiate with Takes 20 Radiographer to appreciate a mins colleague’s Case 2 Role-play perspective Two students pages 15 -16 Tea break 10 mins Start 100 Takes 30 mins Case 3 Pair into F1 and Nurse roles with rest to observe Here and throughout, ask student who is interviewing to read out the scenario, Give out student script and GP letter – (NB the latter is also needed in cases 3/4 to identify causes of an ‘adverse event’). Discuss their approach and clarify any factual points and problem solve ahead e.g. What options exist to ensure partner’s care? Increased nurse visits; social service input – carer; respite admission to nursing home Instruct observers: Take notes + After scenario (and during if they pause) feedback to discuss: Revision of SPIKES (if appropriate) Patient’s expectations Negotiating skills: The student should apologise for planning deficiencies – (1. the Ultrasound has not been pre-booked and 2. the patient is unprepared for admission). Reassure the patient that a package of care for the partner will be put in place urgently. The patient will go home to their partner but return later the same day Feedback to discuss: Request for urgent US scan. Use SBAR framework here, especially to ‘Escalate’. First try using telephone – start with students seated back to back. Then see if students suggest Dr standing and phoning –more assertive. Discuss / try alternative ‘personal’ approach Related issues: Teamwork; Priorities and resources in NHS, interpersonal influencing skills, Personal management skills Handover To apply and understand SBAR principles in Emergency handover of patient care to another team member Pages 17-18: Explain that you are now practicing SBAR in an emergency: taking and acting on an urgent call from a nurse Start by reading out to all the Nurse script to include SITUATION. Explain students also need to problem solve the emergency management, so it’s best to do some of this first!* The scenario could evolve, so fold the student instructions over. At least start above the line! Ask the students to work in trios/4’s to practice an urgent Nurse to F1 Dr ‘back to back’ telephone ‘handover’ of Mr/Mrs Smith, giving each pair the different role play scripts. Link 1-2 Observers to share ‘nurse’ script – It’s best if ‘F1 Dr(s)’ leave room briefly. If necessary either party can pause to ask observers for management advice, get data from ‘below the line’, or restart to ‘escalate’ the urgency. Observers to make notes on BOTH parties use of SBAR elements and 7 feedback on Clarity of ‘call’ and repetition, escalation. Clarity of ‘response’ and checking by Readback. Then debrief the whole group focusing on communication! *[Management: treat hypoglycaemia with bolus glucose IV and then drip (NB patient to stay till morning – negotiate) GCS – students have more details in their script and can review any of this themselves later ] Start 130 takes 40 mins To do both tasks Case 4 task 1 To explore the reasons for poor Adherence to medication with the patient Pages 19 and 20 First explore the likely causes of Hypoglycaemia here: (missed breakfast, but more important then to query an excess dose of medication – student notes). So return to the GP letter: what are potential causes of this adverse event? Case 4 task 2 To manage an ‘adverse event’ and discuss how to learn from error / ‘open disclosure’ Discussion 15 mins: Preventing and Managing Adverse Events Learning objectives: Developing an understanding that error is unavoidable – but not easily discussed! Case 4 SP Role play with the ‘recovered’ SP, debrief for 25 mins Debrief the group on understanding the patient’s reasons for non-adherence, being honest about causes: Try to reach agreed solutions and explain to patient how you and the organisation can learn from the incident. Involve SP later in debrief specifically on the adverse event, as this is the main focus for this Case. (see student Resource for details on Concordance) In working out the causes of this Adverse event, the immediate problem should have emerged. Root Cause (s) – these are often multiple as here*: Both Consultant AND F1 doctor copied a dose of Gliclazide 160mg from the GP’s letter. This was the prescribed dose, not 40mg (1/2 a tablet), the dose the patient was actually taking. So both the GP and administering nurse contributed too. 1. Personal Learning: Consider Prevention: To include the patient by cross checking data. If the patient had been asked about the dose and was unclear, then the F1 could fax the GP. The GP Repeat prescription record might have revealed the lower level of use. 2 ‘A Learning Organisation’: to what extent can we be ‘Open’ and what is ‘open disclosure’? – Transparency on facts AND Reflection later Ask: What further actions are needed to prevent a repetition of this? How will you document this in the notes? How do you RESPOND when the nurse suggests that you complete an Incident (IR 1) form? What 8 if you HAD accidentally written an excessive dose ? (i.e. Your ‘error’). How will you cope and how can teams manage error? (Personal AND safe group reflection) Reflect on ‘no blame’ / ‘fair’ blame cultures? Suggest revisit in review of learning in pm session * Start 160 Takes 35 mins Case 5 SP Ends 195 NB: THE ROLE NOW JUMPS AHEAD IN TIME! Bad news has already been broken by consultant, but the student must continue the process IF your group has completed the Cancer ‘block’ (THEY MAY NOT HAVE YET!) they should be prepared to maintain Hope / discuss disease progression (months - not years, stent blockage) dignity in dying and symptom + pain control To talk to a dying patient – use SPIKES Remind the student role-player this could be challenging and to Pause as required To START a process of consent. Explore benefit/risk of stent procedure with patient. How to begin to obtain consent for ERCP? - BUT stress That full responsibility to complete this remains with the Consultant, discuss role of Foundation Dr in team – emphasise process page 21= student role 45 mins NB: FIRST: The patient asks the ambiguous question (s): ‘What’s going to happen?’ …How long have I got? Is it worth it? Sharing information re stent – see reference and checking understanding Resources: Use a hospital or D of Health consent form +/- patient information leaflets see links p33 Summarise the morning’s learning: go round group Lunch 9 SESSION 2 TIME INDIVIDUAL CASE TASK TYPE for student role-playing F1 Start 0 Confidentiality dilemmas: to respond to takes daughter/son’s 40 mins request for information Case 6 SP page 23 GROUP TASK Get the group to explore the options here, before running the scenario: Preparation: What's gone before? How do they judge the relationship? Can they balance these principles? Keep disclosures to the minimum necessary; inform patients about any disclosure or check that they have already received information about it. You must be considerate to relatives, carers, partners and others close to the patient, and be sensitive and responsive in providing information and support. If the patient cannot give consent, share information with those close to the patient who need/want it (unless you suspect patient would object) Resources: MDU and GMC booklets: [GMC website] Start 40 Case 7 Student led takes 20 mins To discuss DNAR Case 7 page 26 Feedback on scenario to discuss: How to limit information given and use assertive behaviour to stop a cyclical discussion; Dealing with anger; Strategies to use in difficult situations, and house-keeping (i.e. self care) afterwards. DNAR: Do Not Attempt Resuscitation: Ask a student to lead the discussion and give them the scenario Student prompts How do you respond to the nurse? How is a decision reached? What happens on the wards? What are the barriers to reaching DNAR agreements? Reflect on their own experiences - terminology: ‘pink forms’! How do they feel about being part of such decision-making? Can the process be harmful to patients? See: Three words that can change a life: "Allow natural death" versus "do not resuscitate": S S Venneman, P Narnor-Harris, M Perish and M Hamilton J. Med. Ethics 2008;34;2-6 Consequences of decision; Involvement of patient/relatives; Current policy/guidelines Resources: DNAR algorithm at www.ethics-network.org.uk (Also good for other issues in this course) Advance directives: http://www.ageconcern.org.uk/AgeConcern/is5.asp See also ‘BMJ Learning’ module – good for tutors! Highlight the ethical issues raised. Ask students to explore other scenarios and queries later. 10 Start 60 Takes 30 mins Case 8 SP BBN : to inform daughter/son of their parent’s death page 27 10 mins Start 90 Takes 30 mins Case 9 SP Role-play Two students Start 120 Takes 20 mins Case 10 Discussion Start 140 Takes 15 mins 155 mins Feedback on scenario to discuss: Reaction to bad news Dealing with own feelings Note for scenario 8 *Local policies on reporting post-operative deaths vary. Because this death might not be "natural" but due to post-operative complications (eg PE, MI), the Coroner’s officer needs to be informed, but will not necessarily ask for a post-mortem. Tea break The group should discuss responses to complaints. To manage anger and resolve complaint To respond to request for Death Certificate + need for report to Coroner page 29 Discussion about personal feelings page 31 Revisit sensitive topics that have arisen: A doctor and a ‘nurse’ then prepare to meet the relative together to discuss what happened: – saying ‘Sorry’ is not an admission of fault. Reporting to the Coroner’s officer: How could this best be managed?* Possibility of post-mortem? Highlight the use of case as a critical event Peer review and support Self-audit Resources: ‘Deaths Reportable to a Coroner’ Discussion of coping strategies Teamwork / support “Burn-out” Where to seek help e.g. see morning notes on ‘Blame culture’ - scenario 4 * Blame implies judgement and looking back - are there better terms? eg. consider ‘contribution’ systems – analysis and looking forward Also opportunities: see page 4 Students may want to attend a Morbidity / Mortality or Critical Incident / Adverse Event review. It may be difficult for students to access sensitive reviews, so they may learn more by talking to Foundation doctors during Assistantships. Ending & Evaluation, take away points and one thing to look up? End Attend tutor debrief – especially if you have anything to pass on. Hand in register! Thank you for tutoring on this session – we hope you have enjoyed it. Mark Perry and Rosie Illingworth Communication Team Manchester Medical School 11 CASE 1. SHIFT HANDOVER PRACTICE CONTEXT: As Handover ‘Giver’ you are just ending your shift and have been busy admitting several patients, you want to agree priorities with your colleague, or ‘Receiver’. Receiver: You have just arrived at hospital and are coming on to the morning shift. You are taking Handover from your colleague and then going to clerk new patients under Mr Holmes in the Investigation Unit. You should make notes and clarify using ‘Readback’. NB BOTH Giver and Receiver should use SBAR, to check that they have all the information that they need. Task: The information is initially mixed up for you - as if given by a stressed out and disorganised colleague! So sort the information on 2 patients in the boxes at the bottom of the page into SBAR order, one patient each (7 mins). The Main patient for today’s session (Mr or Mrs Smith) is shown here at the top as an Example of using this method, but you will need to personalise this as a ‘script’ to use it yourself! Discuss your overview of these three patients and prioritise the order for handover (3 mins). Then act as Giver for your patient, one group member to act as Receiver and the other as Observer of BOTH Drs in the SBAR handover. Rotate till 2 or 3 have had practice in one role . ( 5 mins each with feedback) Situation Background Assessment Recommendation 1. Mrs / Mr Smith: A 64 year old with Obstructive Jaundice – awaiting admission for tests Nurse in MIU has just called you to report 1. That an urgent Ultrasound that should have been booked for today via Outpatients has not been pre-booked 2. That the patient is upset about this. Patient may self -discharge Please come within 30 minutes. See patient, book US for today if possible. Priority 1 PATIENT: Situation Background Assessment Recommendation Priority 2 PATIENT: Situation Background Assessment Recommendation Priority 3 PATIENT: Situation Background Assessment Recommendation 2. Lisa Ball woman 75, In ward 11 No previous history of DVT or FH 3. James Prentice male 70 year old Attend now to assess Investigations: fbc, U+E normal. 18 hours post op. Transurethral prostatectomy. 5 days post op. defunctioning colostomy for Diverticular abscess. On ward 7. Check results within next hour. No PMH of note. Patient noted swollen tender left calf this am. Immobile prior to admission. Had uncomplicated TURP under spinal yesterday. If D-dimer test is positive, Medical registrar requests urgent Normal blood loss in catheter bag – no clots. LMW Heparin Enoxaparin (Clexane). Seen by on call Medical team 1 hour ago, no shock or pyrexia. Physical signs ?DVT L calf. Nurse has just paged you reporting BP dropped from 110/80 P90 to BP 90/60 - P100. Apyrexial. Blood pressure has dropped in past 2 hours ?Cause You await result of D-dimer (done 10 mins ago) 12 Case 2 INSTRUCTIONS TO STUDENT You are a Foundation Dr. It is Wednesday morning. You are on the Investigation unit (“5-day ward”) where patients attend for planned investigations. Mr(s) Smith was seen by your Consultant, Mr Holmes last week and this admission booked. Attached is the referral letter from the GP to Mr Holmes. Your Consultant (Mr Holmes) has written the following in the records: 2/52 history of jaundice, itch, pale stools. ?weight loss. PMH Type 2 Diabetes 1year, on medication 9 months SH non-smoker DH: Gliclazide as per GP letter, Gaviscon o/e jaundiced, thin, Abdo Tender epigastrium, No mass, No LKKS ? GS ? Ca Needs Investigation ASAP – Admit PIU Your task: To arrange for the patient to be admitted to the Unit and to stay for 2-3 days for investigations. The patient gave a history in outpatients last week and you would normally confirm this by further ‘clerking’. You can defer this at present. Your priority is to address any concerns this patient has now, apologising that investigations have not yet been pre-booked. 13 Dr G Platt The Health Centre New Street Manchester M14 3PQ URGENT APPOINTMENT PLEASE Dear Mr Holmes, re: J Smith I would be grateful if you would see this 64 year old who has developed jaundice. This was noted 10 days ago, and following today’s consultation with him/her I felt that an urgent referral to you was appropriate. The jaundice has been accompanied by anorexia and itching as well as pale stools. On examination I feel there is evidence of weight loss and I wondered if I could feel an epigastric mass. I feel urgent investigation is required. Mr(s) Smith’s wife/husband has severe rheumatoid arthritis and is housebound. The couple have a son and daughter who live down South. The neighbours, I believe, are quite helpful, and our District Nurse visits weekly. I have told the patient that (s)he will need some tests. No questions were forthcoming from Mr(s) Smith, but I believe (s)he may know something is amiss. (S)he is a very stoical person, having had to care for his/her spouse for many years. The patient has Type 2 Diabetes, diagnosed one year ago and now controlled on Gliclazide 160mg am. Many thanks for seeing him/her so quickly Yours sincerely Dr G Platt REPEAT PRESCRIPTION: Drug Monthly quantity Dose Gliclazide tablets Gaviscon 2 a.m. (160mg) with food. 10mls pc and at night prn 80mg 56 500mls 14 Simulated Patient Script Patient’s name John/Joan Smith Setting Investigation Unit Wednesday am Course Session Case Age Sex Other info Yr 5 1 2 64 M/F You are 64 years old and live with your wife/husband who has severe Rheumatoid arthritis and is housebound. Situation Since you retired you have devoted yourself to looking after your spouse who has RA. He/she is housebound and relies on you for help with very basic activities of daily living. Your neighbours often pop in and offer to do bits of shopping and gardening (although you like to potter in the garden). The District Nurse visits weekly to check your spouse's pressure areas and has a chat. Your son lives in London and your daughter lives in Cornwall and you don't see them much. While speaking on the phone frequently, you do not / will NOT discuss your medical problems. Apart from Diabetes, diagnosed a year ago and for which you take ½ a tablet with breakfast in the morning, you have always been well (NB NEW See Case 4 The doctor wanted you to take a higher dose, but you are afraid to admit that you have not increased it! Do NOT disclose this here.) Now You are in the Investigation Unit (“5-day ward”). You have seen a nurse who has said a doctor is going to come and talk with you and you are waiting to see what happens next. Past You noticed your skin was yellow about 2 weeks ago. You also noticed your stools were pale and wouldn't flush away. Your skin has been itchy for about a week. You went to see your GP who was concerned because you said you may have lost some weight over the last couple of months. He said you should come to the hospital and phoned up for an appointment whilst you were with him. Last week you attended the outpatient clinic and saw Mr Holmes. He seemed concerned about your symptoms and said he would get you seen in the “Day Unit” as soon as possible. His secretary phoned you yesterday to ask you to come today at 10am. A neighbour is looking after your spouse. You assume you will be going home this afternoon. You want to ensure you don't have to stay in hospital overnight as you couldn't possibly leave your wife/husband. Now: You are waiting to be told what will happen next. A nurse has told you that your scan has not been booked for today. Role Player Task Think about how hard it would be for this person to come into hospital. You are quite worried about your symptoms. You are annoyed that the tests have not already been arranged and are adamant that no-one will force you to stay overnight in hospital until you can be certain that your spouse will be OK. If the doctor listens to your concerns and is empathic then you can negotiate a way through this and how to sort out things at home. eg. Go home and come back later. If the doctor is dismissive, doesn’t listen or if he/she tries to bully you, then be a stubborn mule! For the NEXT scenario you now come BACK on Wednesday evening 15 CASE 2 INSTRUCTIONS TO DOCTOR You are a Foundation Dr. Mr/Mrs Smith has been admitted this morning to the Investigation Unit for investigation of obstructive jaundice. It is Thursday lunchtime. You have sent off blood to the lab and need to arrange an urgent abdominal Ultrasound scan. You would really like to get all the tests done today so that Mr/Mrs Smith can go home to care for their partner, who has severe RA and is, you believe, housebound. Task: To arrange the Ultrasound scan, for today if possible. To arrange the appointment by telephone with the Radiographer Ask your colleagues for suggestions and try different approaches. How can you use SBAR to ‘escalate’ your request? 16 CASE 2 INSTRUCTIONS TO RADIOGRAPHER It is Thursday lunchtime. The Foundation Dr phones you to ask for an urgent scan. There are no routine Ultrasound scan appointments until next Monday. You don’t really see why this scan is so urgent. Feel free to improvise from your own experience. Don’t be a push-over. Do they really make out a case for an urgent scan? How can you use SBAR to check the urgency of this request? Can you reach a clear agreement? If you don’t feel convinced, how would you react if the doctor comes down? 17 CASE 4A INSTRUCTIONS TO STUDENTS: F1 Doctor roles One day later (Friday 12 MIDDAY) You are a Foundation Dr. You know Mr(s) Smith (who has Type 2 Diabetes on tablets) is on the ward this morning having just had an urgent CT for suspected Ca. Head of Pancreas (Ultrasound yesterday required clarification). You are just clerking another patient on a nearby ward and should be free in 10 minutes A nurse pages you TO CALL THE WARD You will need to use the SBAR system to ‘Receive’, READBACK - Check and Respond to the Nurse’s Recommendation. What do you do? If necessary, PAUSE and discuss with your Observer. Based on YOUR clarification of the nurse’s SBAR report on Mr(s) Smith make your own ASSESSMENT and RECOMMENDATION back to the ‘Nurse’ FOLD HERE _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ Background Data that you may require: PAUSE if you are uncertain about the management of Hypoglycaemia and clarify with the ‘Observer’ 1. A BM stick shows glucose 2.0 mmol/l. 2. Some nurses may be able to site a Venflon and administer IV Glucose, IM Glucagon also offers a short term solution, but you would need to check the patient’s response in 5- 10 minutes 3. GCS – You might want more detail of changes in the patient’s conscious level: Glasgow Coma Scale: 8 / 15 BUT 7/15 later IF management is delayed for Dr to arrive: Best Responses to mild pain in 3 domains: Motor / Verbal / Eyes. So patient may withdraw arm 4/6; Moan – no words 2/5; Eyes open if Called 2/4 initially, or after a delay as a response to Pain 1/4 or Not at all 0/4 18 CASE 4A INSTRUCTIONS TO STUDENTS: ‘NURSE’ roles One day later (Friday 12 MIDDAY) You are a Ward Sister / Charge Nurse: SITUATION You note that the patient has become progressively pale, sweaty and confused, worsening over 15mins… and is now becoming less responsive. BACKGROUND Mr(s) Smith who has Type 2 Diabetes on tablets, returned to the ward 30 minutes ago after having had an urgent CT for suspected Ca. Head of Pancreas (Ultrasound yesterday required clarification). Mr(s) Smith is not yet aware of the diagnosis. You recall that the patient was anxious before the CT and did not eat, but she was still given her tablets. PAUSE in setting scene for whole group: Ask all – what is likely cause? ASSESSMENT (DO NOT READ OUT YET!) Decreasing conscious level. Apyrexial, but pale and sweaty. P120. BP100/60. A BM stick shows glucose 2.0 mmol/l. You have just paged the F1 Doctor and the phone is now ringing. Task for yourself in role and observers: What do you do? RECOMMENDATION: Think of both Nurse and Doctor roles here. You will now need to use the SBAR system to: Make a RECOMMENDATION to the F1 Doctor. If the Doctor does not appreciate the urgency, ESCALATE both your concern and request. Then to CHECK on the F1’s response and if needed CLARIFY their recommendation BOTTOM 1/2 PAGE: Further Background Data here and below that you may require: PAUSE if you are uncertain about the management and clarify with the ‘Observers’ NB: No qualified nurse is available to site a Venflon and administer IV Glucose (some can do so) IM Glucagon also offers a short term solution, but you would need to check the patient’s response in 5-10 minutes *(If detail is requested Glasgow Coma Scale: ‘GCS 8’: Responses to mild pain: Motor - withdraws arm / Verbal - moans / Eyes open – when called. See below for more detail ) FOLD HERE _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ SITUATION: Identify self and patient: I am Nurse X on X Ward, calling about Mr(s) Smith. He/she is HYPOGLYCAEMIC!!! BM stick shows Glucose is only 2mmol/l He/she has become pale, sweaty and increasingly confused over 15 mins. BACKGROUND Mr(s) Smith aged 64, has Type 2 Diabetes on tablets, returned to the ward 30 minutes ago after an urgent CT for suspected Ca. Head of Pancreas. The patient did not eat this morning but I have checked: (S)/He was still given Gliclazide tablets. ASSESSMENT: Decreasing conscious level*. Apyrexial, but pale and sweaty. P120. BP100/60 IMPORTANT: BM stick shows Glucose is only 2mmol/l RECOMMENDATION: The patient needs URGENT! i.v Glucose. Come now to site Venflon GCS: Glasgow Coma Scale: 8 / 15 BUT 7/15 later IF management is delayed for Dr to arrive: Best Responses to mild pain in 3 domains: Motor / Verbal / Eyes. So patient may withdraw arm 4/6; Moan – no words 2/5; Eyes open if Called 2/4 initially, or after a delay as a response to Pain 1/4 or Not at all 0/4 19 CASE 4B INSTRUCTIONS TO STUDENTS: Doctor role Task 1 You are the same FY1 from case 3 The patient responds to your management (i.v. glucose) and an hour later you decide to explore the reasons for the hypoglycaemia with patient over a cup of sweet tea. How do you approach this? You recall that you were busy on Wednesday evening and wrote up the patient’s drug chart using the details on the GP letter. Consider the root causes of this patient’s hypoglycaemia with your group. Look beyond the immediate ‘cause’ You may also need to PAUSE during the role play to discuss this further with the group Task now: Decide how to explore and then resolve this with the patient. He/she can go home tomorrow (Saturday am) if there are no further episodes, but should return for the scan results in 2 days (Sunday night/Monday morning for Mr Holmes’s ward round) Clues – DO NOT READ THESE OUT yet unless the group really needs prompts! A missed meal alone would not often cause hypoglycaemia for a patient on a normal dose of Gliclazide Given the recent weight loss, the patient now requires a minimum dose of Gliclazide 40mg till readmission. Task 2 GROUP: Later the ward sister (who has been supportive) recommends filling in an Incident form. How are adverse events handled at your Hospital site? e.g. at Salford Royal this is done electronically through the site intranet. When is there anonymity? Discuss your feelings about ‘adverse events’. How would these differ if you HAD accidentally written an excessive dose ? (i.e. Your ‘error’). How will you cope as an individual and how can teams manage error? What is ‘open disclosure’? 20 Simulated Patient Script Patient’s name John/Joan Smith Setting Medical ward (Investigation Unit) Course Session Case Yr 5 1 4B Age Sex Other info 64 M/F Two days later, Friday late morning Since you were reluctantly admitted on Wednesday, you have had an ultrasound scan on your tummy yesterday and another type of ‘scan’ this morning (one where you had to lie still and go into a big tunnel). The Dr has said (s)he will come to see you when the scan results are back with clearer picture of the problem. You are unsure when this will be, but you are keen to go home in the meantime. This morning you were so worried about the scans that you did not eat any breakfast. The nurse still gave you 2 tablets as she has done each morning since you were admitted. You presumed that these tablets are for your diabetes even though they were a different shape from your usual tablets. You are beginning to suspect there is something seriously wrong. . When you returned from your scan this morning, you suddenly felt unsteady, muddled, sweaty and sick. This lasted for a few minutes and then you suddenly slumped. When you came round, you looked at a watch and realized that it was an hour later, and you had little memory of the last hour! It is now an hour AFTER treatment and the doctor has come to talk to you about what has just happened over a cup of sweet tea. He/she will explain that your blood sugar had become very low and will want to explore the reasons why. Information to be given if asked: When your diabetes was discovered, the GP prescribed Gliclazide 40mg (half an 80mg tablet) and warned you that this medication COULD cause unpleasant side effects and so must always be taken with food in the morning, After 6 months of taking the medication along with a low sugar/fat diet to reduce your weight, the GP told you that your blood sugar was still too high and increased your dose of Gliclazide to a full 80mg tablet. 3 months following that, the dose was doubled again to 160mg (2 tablets) HOWEVER - you never took more than the original prescribed dose of 40mg of Gliclazide as it made you constipated. You did not tell the GP the dose you were taking because, a) he might not approve and b) it seemed trivial compared with other worries. Please offer your account tentatively, to allow students to explore the causes. If the group is slow you can say ‘these tablets here are different – mine have a line down the middle’. Even add ’..so they can be split in half’. 21 Role Player Task: to explore with you how you came to have a hypoglycaemic ( Blood sugar too low) incident to establish reasons why patients make their own decisions re medication levels to understand the dangers of assuming that patients are taking the medication as prescribed/recommended by their GP. In this situation you have been taking 4 times your usual dose for the last 2 days!! This is what has caused your attack and it is important that the students discover this. You can agree a solution: the prescription will be reduced with the GP being informed. NB You will then realize that you have contributed to the attack, but it is important to say that ‘I don’t want the same mistake to affect others in future.’ You may also want reassurance that you have not caused yourself any long term damage. Feedback: Has the doctor explored and explained the problem in an honest manner? Do you know what dose to take now? The Learning Objectives here are the problem solving the causes and honesty with you, NOT details of treatment. Your role is in the discussion that follows this incident, so the tutor should bring you back in - as if you are now recovered at the bedside. There would still be a tube (IV line) in your forearm. 22 CASE 5 INSTRUCTIONS TO STUDENT Tuesday late morning: The CT scan was finally reported on by Monday morning. You are one of two Foundation Drs working with Mr Holmes and you need your lunch break! You know from the ward round yesterday morning that (s)he has Ca head of pancreas with liver metastases and is awaiting stenting, which is a palliative procedure. Mr Holmes stayed after the ward round to ‘break the news’ Mr Holmes has decided that ERCP is indicated to insert a stent under IV sedation. The operating list is in 2 days time. After the last ward round you did a quick Medline search finding 2 review papers on palliation of jaundice in malignancy. These indicate that Teflon stents have a 90% success rate, most being successfully placed at the first procedure. They relieve symptoms, but will only remain patent for 3 to 6 months.1 You now need to explain why this procedure is indicated and begin the preparation for consent. Your Consultant will finish the consent process on his rounds tomorrow. Tasks: To explore and respond to the concerns the patient has. Remember SPIKES. You may want to brainstorm symptom control in advanced or terminal cancer with your group. PAUSE during the roleplay as required. Then to begin a consent process for a palliative procedure and To explain the need for the procedure and check the patient understands 1 F.J.Brescia; Palliative Care in Pancreatic Cancer. Cancer Control, Jan/Feb 2004, 11, no.1 pp. 39-45. 23 Simulated Patient Script Patient’s name John/Joan Smith Setting Investigation Unit NB NOTE initial BBN has been covered Day 6 Tuesday late morning: Course Session Case Yr 5 1 5 Age 64 Sex Other info M/F DAY 6 CASE 5 It’s Tuesday lunchtime – not that you feel like eating anything. You came back in on Sunday night when you were happier with your partner’s care and to go through all the results of the tests with Mr Holmes on his Monday morning ward round. It seems that you have a cancer in the pancreas which they can't remove - as it is also in the liver. You also saw Mr Holmes later yesterday and he offered an operation in three days to get rid of the jaundice, which would be something – as the itch is really upsetting. You were told this would be fully discussed with you, but he seemed busy. You feel that no-one cares about you. Last night, whilst you were lying awake, it sunk in that you are dying. Now You would like to know how long you've got - Mr Holmes wouldn't tell you. Why? Role Player Task You have realised that you are going to die. You are concerned that it will be unpleasant, painful, that you will lose control of your bladder, bowels etc. This thought upsets you. You need to know more about this proposed operation to get rid of the itch. Is it worth having done? 24 CASE 6 INSTRUCTIONS TO STUDENT It is now 2 days later and 8 days since the patient was admitted. You are a Foundation Dr on a surgical ward. You are trying to get your notes written up from yesterday’s ward round. Mr(s) Smith (you may recall him from the last session) has just been brought up to the ward from theatre following ERCP and remains drowsy from the sedation. You see from the operation note that a stent has been inserted to relieve the jaundice. Your consultant has written that the "outlook is poor". The staff nurse informs you that Mr(s) Smith’s son / daughter is here and wishes to have a word with you. Task: To address the concerns of Mr(s) Smith’s relative. To end the interaction satisfactorily. 25 Simulated Patient Script Name in role Setting Paul or Paula Smith Quiet room off main ward Course Yr 5 Session 2 Case 6 Patient’s name John or Joan Smith, parent age 64 Age yours! 30s Sex M/F You You are Mr John/ Mrs. Joan Smith's son/daughter. You live and work in London and have a very busy life. Your partner works in the City. Since your parent (the patient) retired they have devoted themselves to looking after your other parent who has Rheumatoid Arthritis. He/she is housebound and needs help with very basic activities of daily living. Their neighbours often pop in and offer to do bits of shopping and gardening (although your parent who is now the patient likes to potter in the garden). The District Nurse visits weekly to check your housebound parent’s pressure areas and has a chat. You don't see your parents very much but speak on the phone fairly frequently. Your only sibling (Patricia or Patrick Smith) lives in Cornwall. Unfortunately, your parents see even less of him/her as they don’t approve of his/her partner and that has become a barrier between them. Situation You have travelled up from London to see your sick parent. Before your journey your housebound parent had rung to say your parent was about to have an operation and now you want to know what has been done. Your parent at home was a bit vague about why the hospital admission happened (8 days ago) - something about being jaundiced and then a funny turn in hospital - they didn't seem to know much. S/he's been able to see his/her spouse only once when s/he came out for the weekend after that. You hope to drive him/her up the hospital this evening, but only after you’ve got some information from the doctors. You’ve not been to your parental home yet. Your housebound parent has been receiving a package of care since your other parent has been in hospital*. You believe you parent in hospital has just come out of theatre and have asked a nurse if you can speak to the doctor who's looking after him/her, anticipating you'll see the consultant if this problem is serious. You’ve not seen your sick parent yet. Now You have been told to wait in a side room. Role Player Task - Build up a work and social picture. You drove up early this morning and are very tired. You are feeling stressed by the increasing burden of elderly parents who live at a distance from you. You are concerned about the management of your sick parent so far – why haven’t you been informed of the diagnosis and prognosis?* Be manipulative – when they explain confidentiality rules try –‘ I won’t tell anyone – just give me the information.’ What might you be worried about? Role player feedback: Handling confrontation/manipulation and handling confidentiality issues. Do they need to stand firmer with you to stop the discussion going round in circles? *please check with the group facilitator what contact you have had with the hospital since your parent's admission (usually none). 26 GROUP SCENARIOS CASE 7 Do Not Attempt Resuscitation - DNAR TASK FOR FULL GROUP The nurse caring for Mr/Mrs Smith asks if s/he is for resuscitation. How do you respond to the nurse? How is such a decision reached? What, in practice, happens on the wards? - ask your colleagues to reflect on their experiences. How do they feel about being part of such decision-making? What are the barriers to reaching DNAR agreements? Can the process be harmful to patients? Have you considered whether the adoption of ‘Allow Natural Death’ (AND) would be acceptable on wards? See: Three words that can change a life "Allow natural death" versus "do not resuscitate": S Venneman, P Narnor-Harris, M Perish and M Hamilton J. Med. Ethics 2008; 34:2-6 27 CASE 8 INSTRUCTIONS FOR STUDENT You are a Foundation Dr. Mr/Mrs. Smith, a 64 year old, had palliative surgery for Ca pancreas 3 days ago. You don't really know them or their family, but last night you were told over the telephone that the patient was vomiting repeatedly and you remember that you did authorise an IM injection of an anti-emetic using an IT link. The Foundation Dr normally responsible is seeing a patient in A&E. Mr/Mrs Smith arrested an hour ago. The crash team was called but resuscitation was unsuccessful and s/he was pronounced dead 45minutes ago. Whilst resus was underway a nurse rang and got hold of the son/daughter to inform them that things had taken a “turn for the worse” and were told the son/daughter was coming in to hospital. Their daughter/son has just arrived onto the ward. You have been asked by the staff nurse to talk to the relative. Mr/Mrs Smith had told the son/daughter all about the illness and the outlook. Task: To inform a relative of their parent’s death. To manage their reactions and handle strong emotions 28 Simulated Patient Script Name in role Setting Patient’s name Patient’s age Paul or Paula Smith Quiet room off main ward John/Joan Smith 64years Course Session Case Age – yours! Sex Other info Yr 5 2 8 30s M/F You are …(as in scenario 6). Situation You travelled up from London 3 days ago to look after your housebound parent whilst your now ill parent is in hospital. Following that first visit when they wouldn’t tell you anything you now know about the cancer and the stent. You have seen your parent daily and they have been able to have a few words with you. You have not been able to bring in your housebound parent yet, as they’ve had a chest infection. You came to visit hospital last night and s/he looked very poorly, s/he was yellow and very weak and vomiting repeatedly. You simply sat with your mother/father and held their hand – they were not up to talking. The ward seemed understaffed and after you called over a nurse she made a phone call to request an intra-muscular injection to stop the vomiting. It seemed about an hour later when the nurse gave this hurriedly without any other apparent discussion or checks. Your parent eventually settled, but on going back to your parents’ house you were concerned about the quality of care. You had a telephone call from a nurse one hour ago to say that your parent in hospital "had taken a turn for the worse". You came straight away. On your arrival onto the ward you are ushered into a sitting room to wait. Now You remain rather concerned that the medicine your parent had been given last night appeared to be ordered by phone. Role Player Task : You wonder what they're going to tell you and what a ‘turn for the worse’ means. Though you saw your parent last night you don’t feel as if you have made your peace with them yet. The issue of the injection remains in the background at present but you might mention the long wait your parent endured just to illustrate your unhappiness with their care. Don’t get angry here – be upset for your parent and concerned on how you will tell your housebound parent and what the longer term implications will be for their care. Let them practice BBN using SPIKES. Be emotional – let’s see how they cope with tears - sobs even. Feedback BBN and handling emotion 29 CASE 9 INSTRUCTIONS FOR STUDENT Next day As the usual Foundation Dr, you have not completed the Death Certificate yet as you know you need to find the time to contact the Coroner’s office and report the death of Mr/Mrs Smith. You know that as they died within three days of surgery, the local policy is that you should speak to the Coroner's officer to report the death.* Your colleague told you that he/she chose not to mention this yesterday as the relative was in shock and it seemed inappropriate – it is likely that the Coroner's team accepts the death with out further question. It might be that they require a post mortem. You are just about to get yourself into an office to catch up on such admin when Mr/Mrs Smith’s relative drops in and wants a word. The ward sister spoke to you earlier to say that the relative had been upset about the standard of nursing care the evening before your patient died, particularly the delay in giving medication. The nursing notes record that the on-call doctor was busy in theatre when phoned. But the drug was prescribed by the doctor on-line. An hour after the injection Mr/Mrs Smith stopped vomiting. The ward sister has already used the charts to confirm that the correct medication was given. Task Prepare for this meeting as a group – Please meet the son / daughter with a ‘nursing colleague’. Objectives To find out facts from other team members and then respond to the relative. Could the drug be authorized by telephone or instead remotely using online prescription? To manage anger and a potential complaint Explain the need to report to the Coroner with the possibility of post mortem. Ensure that the relative understands your duty to 'report' the death. You will fax the records and discus the events. The relative might also wish to speak to the Coroner’s office as an independent authority, Provided all agree you should then be able to sign the certificate immediately: so 30-60 minutes * Please note that this rule is not universal and the policy you may use as a resource is just one local example. 30 Simulated Patient script Name in role Paul or Paula Smith Setting Quiet room off main ward Patient’s name John/Joan Smith Patient’s age 64years Course Yr 5 Session 2 Case Age – yours! Sex Other info 9 30s M/F Next day You have brought your housebound parent in to the hospital Bereavement Centre You need the Death Certificate so that you can proceed with the funeral arrangements. You discover that the Bereavement Centre hasn’t had the signed paper from the doctor yet and so cannot issue the Death Certificate. You leave your parent and you nip up to the ward to find the doctor and the Death Certificate. (You will be told that the Coroner needs to be informed of the death) – become angry that there has been another error that the hospital is now trying to cover up. You know how important it was for your parent to die at home and feel they were cheated of that. You also remain concerned that your parent died so suddenly and wonder if someone made a mistake during or after the operation. More than this you are upset at the delay in getting the nurse to give an injection for your parent’s vomiting. You become more concerned that this appeared to be ordered by phone and even wonder whether the wrong drug was given. Role Player Task To collect Death Certificate To react to information. The Certificate has not yet been signed - another delay. (if they don’t mention it ask – does this mean a post mortem?) With all this stuff in the papers about hospitals, the last thing you would normally agree to is a postmortem. But because of your anger and concerns about the quality of care you are ambivalent about the post mortem. You want the doctor to be honest and take responsibility for what has happened. If sensitively handled, you will accept that the doctor has a duty to speak to the Coroner's team. Feedback Were you treated sensitively? Do you understand why the Coroner's team needs to be informed? Do you feel the staff are being empathetic and open with you? Are they open to considering your complaint/concerns? Do you receive a satisfactory explanation about the injection? 31 Case 10 Discussion: Coping with personal feelings: Discussion on normal / abnormal (healthy vs. unhealthy) strategies Morbidity in the medical profession Burn-out Where to seek help Use of difficult situations as "Significant Events" (critical incidents) Also refer with Tutor to session plan for further ideas). Use of difficult situations as prompts for peer review, to audit and stimulate change. 32 PREPARATION FOR PRACTICE: Resource Sheet for Tutors and Students Prescribing and Concordance Between a third and a half of medicines that are prescribed for long-term conditions are not used as recommended. (NICE guideline 76 medicines adherence 2009). Definitions: Compliance: the extent to which a patient’s behaviour matches (adheres to) the prescriber’s recommendation Adherence: the extent to which the patient’s behaviour matches AGREED recommendations from the prescriber. So this shared planning with patients is to improve future Concordance: There are many reasons why patients do not adhere to medication plans: What are they? What have you experienced? How can it be improved? Britten et al (2000) Misunderstandings in prescribing decisions in general practice: qualitative study BMJ 320;484-488 2000 Glyn E et al (2003) Doing prescribing: how doctors can be more effective, BMJ ;327;864-7). NICE guidance 76; medicines adherence available from http://guidance.nice.org.uk/CG76 Consent forms should be available on any ward ! Confidentiality http://www.gmc-uk.org/guidance/current/library/confidentiality.asp DNAR agreements http://www.bma.org.uk/ap.nsf/Content (search resuscitation) http://www.ethics-network.org.uk/ethical-issues/end-of-life/end-of-life-decisions Three words that can change a life: "Allow natural death" versus "do not resuscitate": S S Venneman, P Narnor-Harris, M Perish and M Hamilton J. Med. Ethics 2008;34;2-6 http://jme.bmj.com/cgi/content/full/34/1/2 Advance directives http://www.ageconcern.org.uk/AgeConcern/is5.asp Deaths reportable to the coroner See as an example (local policies vary slightly) http://www.manchester.gov.uk/site/scripts/download_info.php?fileID=6145 Patient Safety and Handover See handout: There are SBAR resources at http://www.institute.nhs.uk/safer_care/safer_care.html Guidance on shifts and teamwork: Safe handover Safe patients: BMA Junior Doctors Committee. 2004 www.bma.org.uk/employmentandcontracts/working_arrangements/Handover.jsp OR http://www.bma.org.uk/images/safehandover_tcm41-20983.pdf Of general use www.gmc-uk.org Self Care for the F1! Iversen, A., Rushforth, B. & Forrest, K. (2009) How to handle stress and look after your mental health. BMJ, 338, b1368. 33 1 HOW CAN SBAR HELP YOU? Student resource: Inadequate verbal and written communication is recognised as being the most common root cause of serious errors – both clinically and organisationally. There are some fundamental barriers to communication across different disciplines and levels of staff. These include hierarchy, gender, ethnic background and differences in communication styles between disciplines and individuals. Communication is more effective in teams where there are standard communication structures in place. This is where SBAR can add real value: • SBAR takes the uncertainty out of important communications. It prevents the use of assumptions, vagueness or reticence that sometimes occur – particularly when staff are uncomfortable about making a recommendation due to inexperience or their position in the hierarchy. In short, SBAR prevents the hit and miss process of ‘hinting and hoping’. • SBAR helps prevent breakdowns in verbal and written communication by creating a shared mental model around all patient handovers and situations requiring escalation, or critical exchange of information. • SBAR is an effective way of levelling the traditional hierarchy between doctors and other care givers by building a common language for communicating critical events and reducing communication barriers between different healthcare professionals. • SBAR is easy to remember and encourages staff to think and prepare before communicating. • SBAR can make handovers quicker yet more effective, thereby releasing more time for clinical care. How does SBAR work? SBAR allows staff to communicate assertively and effectively, reducing vagueness and the need for repetition. The SBAR process consists of four standardised stages or ‘prompts’ that help staff to anticipate the information needed by colleagues and formulate important communications with the right level of detail. Situation – Background – Assessment – Recommendation with Readback Situation (Identify self and patient, location, then immediate problem / concern) Background (current problem + relevant history) Assessment (observations, vital signs and any urgent results. YOUR Diagnosis / concern / ‘hunch’) Recommendation from the ‘Giver’/ Readback from the Receiver: Explain what you need - be specific about request and time frame; Make suggestions; Clarify expectations NB If you are unhappy with the communication, be prepared to Escalate your concern ) Recommended uses and settings for SBAR: • Urgent or non-urgent communications • Verbal or written exchanges • Emails • Escalation and handove • Clinical or managerial environments Training materials to be watched before the session: http://www.institute.nhs.uk/safer_care/safer_care.html The above extract is adapted from: Safer Care: SBAR NHS Institute for Innovation and Improvement http://www.institute.nhs.uk/safer_care/safer_care/situation_background_assessment_recommendation.html 34 35