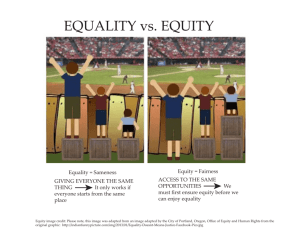
Health inequity:
advertisement

HEALTH EQUITY AND SOCIAL JUSTICE: DEFINITIONS HEALTH EQUITY I “[Health equity is] the absence of systematic and potentially remediable differences in one or more aspects of health across populations or population groups defined socially, economically, demographically, or geographically.” Source: The International Society for Equity in Health HEALTH EQUITY II [Health equity is] “the absence of systematic disparities in health (or in major social determinants of health) between groups with different levels of underlying social advantage or disadvantage—that is wealth, power, or prestige. Inequities in health put groups of people who are already social disadvantaged (for example, by virtue of being poor, female, and/or members of a disenfranchised racial, ethnic, or religious group) at further disadvantage with respect to their health….Equity is an ethical principle; it also is consonant with and closely related to human rights principles. Assessing health equity requires comparing health and its social determinants between more and less advantaged groups. These comparisons are essential to assess whether national and international policies are leading toward or away from greater social justice in health.” Source: Paula Braveman and Sophia Gruskin, “Defining Equity in Health,” Journal of Epidemiology and Community Health 57 (2003): 258. HEALTH INEQUITY I Health inequity refers to differences in population health status and mortality rates that are systemic, patterned, unfair, unjust, and actionable, as opposed to random or caused by those who become ill. Source: see Margaret M. Whitehead, “The Concepts and Principles of Equity and Health,” 22(3) International Journal of Health Services (1992): 429-445. HEALTH INEQUITY II Health inequity refers to “unfair or unjust differences in health determinants or outcomes within or between defined populations.” Source: Alex Scott-Samuel, 2009. Comment These definitions suggest that the root causes of health inequity derive from fundamental social disadvantage (e.g., the ability or lack of ability to influence investment and social policy), based on imbalances in political power or privilege. The implications are that eliminating the inequity requires changing the conditions, structures, and systems of privilege that produce inequity, rather than merely treating its consequences, through programs or social services. Why should we care about health equity? “…Health [is] a special good, which has both intrinsic and instrumental value….Health is regarded as being critical because it directly affects a person’s well-being and is a prerequisite to her functioning as an agent. Inequalities in health are thus closely tied to inequalities in the most basic freedoms and opportunities that people can enjoy.” Source: Sudhir Anand, “The Concern for Equity in Health,” in Sudhir Anand, et al. (eds) Health, Ethics and Equity (Oxford University Press, 2004): 16. “Health equity cannot be concerned only with health, seen in isolation. Rather, it must come to grips with the larger issue of fairness and justice in social arrangements, including economic allocations, paying appropriate attention to the role of health in human life and freedom. Health equity is most certainly not just about the fair distribution of health.” Source: Amartya Sen, “Why Health Equity,” in Anand, p.21. HEALTH DISPARITIES Health disparities are merely variations or differences in health between groups of people that do not specify which differences matter. Comment According to Olivia Carter-Pokras, “Health disparities should be viewed as [the result of] a chain of events signified by a difference in: 1) environment, 2) access to, utilization of, and quality of care, 3) health status or 4) a particular health outcome that deserves scrutiny. Such a difference should be evaluated in terms of both inequality and inequity, since what is unequal is not necessarily inequitable.” Source: “What Is a ‘Health Disparity’” Public Health Reports 117 (September-October, 2002): 426 “The terms ‘health inequalities’ and ‘health disparities’ are widely used as a concise substitute for more precise terminology such as ‘social inequalities in health,’ which can be cumbersome…” Source: Paula Braveman, “Measuring Health Inequalities: the Politics of the World Health Report, 2000,” in Health and Social Justice: Politics, Ideology, and Inequity in the Distribution of Disease, Richard Hofrichter, ed. San Francisco: Jossey-Bass, 2003: 306. NACCHO’s Health Equity and Social Justice Strategic Direction Team prefers not to use the term disparities since disparities can refer to any difference in health status, without specifying the kinds of differences that might be important. Health equity, as NACCHO uses it, refers to fairness in the distribution of resources and the freedom to achieve healthy outcomes between groups with differing levels of social disadvantage. SOCIAL DETERMINANTS OF HEALTH “Social determinants of health are the economic and social conditions that influence the health of individuals, communities, and jurisdictions as a whole. [They]…determine the extent to which a person possesses the physical, social, and personal resources to identify and achieve personal aspirations, satisfy needs, and cope with the environment…Social determinants of health are about the quantity and quality of a variety of resources that a society makes available to its members. These resources include—but are not limited to—conditions of childhood, income, availability of food, housing, employment and working conditions, and health and social services.” Source: Dennis Raphael, “Introduction to the Social Determinants of Health,” in Social Determinants of Health: Canadian Perspectives, Dennis Raphael, ed. Toronto: Scholars Press, 2004. SOCIAL JUSTICE Two central features define social justice—social and democratic equality. The first, social and economic equality, is based on recognition of common human interests. According to Philip Green, in Equality and Democracy, equality refers to “the systematic treatment of representative persons viewed in the abstract as members (subjects) of some organized social whole, rather than with the treatment of particular individuals with unique, individual needs and interests…..’Similar treatment for all who find themselves in relevantly similar circumstances’ is therefore the general definition of social justice as equality.” In this respect, social justice demands an equitable distribution of public goods (mass transportation, access to quality schools, clean water, etc), institutional resources (e.g., social wealth), and life opportunities. (Beyond distributional questions, economist Amartya Sen in Inequality Reexamined defines a just society as one that ensures the development and the capacities of all of its members.) Equality, more than a formal category such as equality before the law or equal opportunity, means equalizing the circumstances of life over which people have no control, and access to conditions that enable people to realize themselves. The second feature concerns democracy (political equality), which refers to enhancing the collective empowerment of (giving voice to) whole classes of people—women, minorities, workers, youth, the aged, and so on, along with transparent structures to forward social goals. Well beyond voting, it refers to cooperation and participation in all institutions that direct society and shape people’s lives. These institutions include the family, schools, and businesses, as well as greater popular control over and access to basic decision-making processes that determine what gets produced and distributed and for whom. Democracy’s roots in this regard derive from principles of inclusion rather than exclusion. Greater democracy means subjecting more issues and investment decisions to public decision-making. Achieving democracy is about ensuring that claims for freedom and equality receive adequate expression. Comment Eliminating health inequity based on principles of social justice means focusing on the underlying injustices that originate with racism, class, and gender discrimination embedded in society’s structure and institutions. Such an approach provides a framework and adds a value or moral judgment to the empirical findings of social inequality that cause health inequity. Thus, it is not the mere fact of unequal health outcomes but their basis within unjust social, political, and economic institutions that is of concern. Such a perspective will emphasize necessary social change that tackles the accumulation of conditions, based on a long legacy of injustices leading to poor health outcomes, in addition to exploring remedies for diseases. Stated another way, “the pursuit of health equity [is viewed as] embedded in and interlinked with the pursuit of social justice….[D]ifferences in health outcomes [are] inequitable if they are the result of unjust social arrangements. The emphasis thus lies not on the pattern of distribution of health outcomes but on the broader social processes underlying health inequalities.” Source: Fabienne Peter, “Health Equity and Social Justice,” in Sudhir Anand, et al. Public Health, Ethics, and Equity (Oxford University Press, 2004):94-95. “Social justice is the foundation of public health. This powerful proposition—still contested—first emerged around 150 years ago during the formative years of public health as both a modern movement and a profession. It is an assertion that reminds us that public health is indeed a public matter, that societal patterns of disease and death, of health and well-being, of bodily integrity and disintegration, intimately reflect the workings of the body politic for good and for ill. It is a statement that asks us, pointedly, to remember that worldwide dramatic declines—and continued inequalities—in mortality and morbidity signal as much the victories and defeats of social movements to create a just, fair, caring, and inclusive world as they do the achievement s and unresolved challenges of scientific research and technology.” Source: Nancy Krieger, “Comment, A Vision of Social Justice as the Foundation of Public Health: Commemorating 150 Years of the Spirit of 1848,” 88(11) American Journal of Public Health (November, 1998): 1603. “Social inequalities (or inequities) in health refer to health disparities, within and between countries, that are judged to be unfair, unjust, avoidable, and unnecessary (meaning: are neither inevitable nor un-remediable) and that systemically burden populations rendered vulnerable by underlying social structures and political, economic, and legal institutions. As such, social inequalities (or inequities) in health are not synonymous with ‘health inequalities,’ as this latter term can be interpreted to refer to any difference and not specifically to unjust disparities. For example, recently proposed measures of ‘health inequalities’ deliberately quantify distributions of health in populations without reference to either social groups or social inequalities in health….Promoting equity and diminishing inequity requires not only a ‘process of continual equalization’ but also a ‘process of abolishing or diminishing privileges.’ Thus pursuing social equity in health entails reducing excess burden of ill health among groups most harmed by social inequities in health, thereby minimizing social inequalities in health and improving average levels overall.” Source: Nancy Krieger, “A Glossary for Social Epidemiology,” Journal of Epidemiology and Community Health, 55 (2001): 693.