The CCG Organization
advertisement

0
CPCRA
Community
Handbook
DRAFT
10/24/03
Community Programs for Clinical Research on AIDS
1
GETTING STARTED........................................................................................................................................................ 3
INTRODUCTION .................................................................................................................................................................. 4
HISTORY OF THE TERRY BEIRN COMMUNITY PROGRAMS FOR CLINICAL RESEARCH ON AIDS ......................................... 5
THE CPCRA ORGANIZATION...................................................................................................................................... 9
CPCRA BYLAWS ............................................................................................................................................................ 11
CPCRA ORGANIZATION CHART ..................................................................................................................................... 32
THE CCG ORGANIZATION ......................................................................................................................................... 33
WHAT IS THE COMMUNITY CONSTITUENCY GROUP? ...................................................................................................... 35
CCG ORGANIZATIONAL CHART ...................................................................................................................................... 36
CCG MISSION AND BYLAWS ........................................................................................................................................... 36
CCG MISSION AND BYLAWS ........................................................................................................................................... 37
CAB ORGANIZATION .................................................................................................................................................. 57
CAB SUGGESTED GUIDELINES ........................................................................................................................................ 59
CAB MEMBER ORIENTATION.......................................................................................................................................... 61
CAB ACTION PLAN ......................................................................................................................................................... 63
MECHANISMS FOR VOLUNTEER RECRUITMENT: LOCAL CABS....................................................................................... 64
ORGANIZATIONS & CONTACTS .............................................................................................................................. 65
CCG MEMBERSHIP DIRECTORY ...................................................................................................................................... 67
CLINICAL TRIAL CONTACTS ............................................................................................................................................ 78
NATIONAL AIDS ORGANIZATIONS AND RELATED ORGANIZATIONS ............................................................................... 79
AIDS PUBLICATIONS CONTACTS .................................................................................................................................... 80
RESOURCES.................................................................................................................................................................... 83
CPCRA MEETINGS: HELPFUL HINTS FOR ATTENDEES ................................................................................................... 84
CPCRA TALKING POINTS FOR CCG/CAB MEMBERS ..................................................................................................... 85
GETTING STARTED: BEING A COMMUNITY ADVOCATE .................................................................................................. 86
SITTING AT THE TABLE.................................................................................................................................................... 87
HOW TO CRITICALLY (AND QUICKLY) READ A PROTOCOL ............................................................................................. 89
ADDITIONAL CPCRA RESOURCES .................................................................................................................................. 90
POPULATIONS ............................................................................................................................................................... 91
HIV/AIDS CLINICAL TRIALS & WOMEN ........................................................................................................................ 93
HIV/AIDS CLINICAL TRIALS AND YOUTH ...................................................................................................................... 95
HIV/AIDS CLINICAL TRIALS AND PEOPLE OF COLOR .................................................................................................... 97
HIV/AIDS CLINICAL TRIALS AND THE TRANSGENDER COMMUNITY ............................................................................. 99
HIV/AIDS CLINICAL TRIALS & AND SENIORS .............................................................................................................. 101
HISTORICAL PERSPECTIVES ................................................................................................................................. 103
HISTORY OF MEDICAL RESEARCH ................................................................................................................................. 105
COMMUNITY-BASED RESEARCH—HISTORY OF CLINICAL TRIALS................................................................................ 107
HISTORY OF CABS ........................................................................................................................................................ 109
HIGHLIGHTS IN THE HISTORY OF INFORMED PATIENT CONSENT ................................................................................... 110
TOOLS ............................................................................................................................................................................ 114
COMMON ABBREVIATIONS AND ACRONYMS ................................................................................................................. 115
MEDICAL ABBREVIATIONS ............................................................................................................................................ 117
FORMAT FOR SUBMITTING CPCRA RESEARCH IDEAS .................................................................................................. 121
HOW TO REVIEW A RESEARCH CONCEPT/PROTOCOL .................................................................................................... 123
DENVER CAB RESEARCH TRAINING ............................................................................................................................. 128
SAMPLES & LOCAL CAB MATERIALS ................................................................................................................. 141
2
Community Programs for Clinical Research on AIDS
3
Getting Started
Introduction
History of the Terry Beirn Community
Programs for Clinical Research on AIDS
4
Introduction
Purpose
The purpose of the CPCRA Community Handbook is to provide materials needed by CPCRA unit’s
Community Advisory Board (CAB) and Community Constituency Group (CCG) representatives and alternates
in order for them to be informed and effective contributors to the CPCRA. This handbook is a result of two
CPCRA CAB Training Conferences held in December 1994 and June 1995 and the efforts of the CCG
Internal Committee.
The “Local CAB Materials” section is for the use of unit CAB and CCG members who are encouraged to add
any materials that they believe will enhance their members’ knowledge and participation in the CPCRA (i.e.,
local membership directory, list of local organizations, list of available local training opportunities, etc.).
Most CPCRA units conduct some type of local CAB training, particularly orientation sessions for new
members. If your unit has not conducted such training or if you would like suggestions on how to improve
your training, you may wish to contact fellow CCG representatives at other units for suggestions on training
agendas and what types of local materials to include.
How to Use This Handbook
The handbook has been copied on three-hole paper to make it easy to replace pages and/or sections in the
future. A copy of the handbook is provided to each CPCRA CCG representative and alternate. Units should
make additional copies, as needed, for their CAB members.
Contents of this handbook will be updated and distributed as needed. Updates of items such as the CCG
Membership Directory will be revised and distributed prior to each CPCRA group meeting. Questions
regarding this handbook should be directed to: Ms. Ljudmila M. Petrovic, CPCRA Operations Center, 8757
Georgia Avenue, 12th Floor, Silver Spring, MD 20910; Phone: (301) 628-3357; Fax: (301) 628-9906; E-Mail:
lpetrovic@s-3.com.
Acknowledgments
The following persons/groups are thanked for their contributions to this handbook: CCG Members (especially
Ryland Roane, B.S.; David Munroe, B.S., M.A.; Kiyoshi Kuromiya; Bob Munk, Ph.D.; Claire Rappoport, M.A.);
CCG Internal Committee (Mark Baker, B.A.; Stanley Estoll, B.S.; Castilla McNamara, B.A., M.P.A.; Tim Day;
Hugh Segner, M.A.; Ryland Roane, B.S.); C. Lynn Besch, M.D.; Lawrence R. Deyton, M.S.P.H., M.D.; Donald
I. Abrams, M.D.; Reginald Caldwell, L.C.S.W.; Lisa Cox, M.S.W., L.C.S.W.; CPCRA Community Advisory
Boards (CC, CHI, DEN, FIGHT, NJCRI, and RAC units); Gay Men’s Health Crisis (GMHC); Critical Path AIDS
Project; Elizabeth Finley, R.N., A.N.P.; Margaret Matula, R.N., M.G.A.; Ljudmila Petrovic, B.A.; and David
Mariner, B. A.
Community Programs for Clinical Research on AIDS
5
History of the Terry Beirn Community Programs for Clinical
Research on AIDS
The Community Programs for Clinical Research on AIDS (CPCRA) was established in 1989 in order to
broaden the scope of the AIDS research effort of the National Institute of Allergy and Infectious Diseases
(NIAID). The goal of the CPCRA is to conduct clinical research in a wide variety of primary care settings in
areas hard hit by HIV, with an emphasis on inclusion of persons previously underrepresented in clinical
trials—women, injection drug users, and people of color. The focus of CPCRA research has been on
questions that are of relevance to the day-to- day clinical care of persons with AIDS and HIV. Through an act
of Congress passed in 1991, the program was renamed the Terry Beirn CPCRA (Mr. Beirn himself had HIV
and was a special health policy consultant to Senator Edward M. Kennedy and a manager at the American
Foundation for AIDS Research).
Since the very beginning of the program, each CPCRA unit has had a mandate to document a wide base of
support from the community it serves. In the effort to design and conduct clinical trials that are relevant to the
CPCRA constituent communities, each unit has developed its own Community Advisory Board (CAB). The
national CPCRA’s Community Constituency Group (CCG) consists of elected members from each local CAB.
The CCG is an integral part of the decision making structure of the CPCRA: its members serve on each
concept and protocol team, as well as on all standing CPCRA committees and subcommittees.
CPCRA Units
The CPCRA is an established clinical trials program that conducts research through a national network of
community-based clinical research units. The CPCRA {currently} includes the 16 units listed below, with more
than 160 collaborating sites that provide HIV primary care for approximately 60,000 patients. Additionally,
Associate Sites collaborate with the CPCRA network to enroll participants in targeted studies.
AIDS Research Alliance-Chicago (ARAC)
Bronx AIDS Research Consortium (BARC)
Community Consortium (CC)
Denver CPCRA (DEN)
Harlem AIDS Treatment Group (HATG)
Henry Ford Hospital (HFH)
Houston AIDS Research Team (HART)
Louisiana Community AIDS Research Program (LaCARP)
New England Programs for AIDS Clinical Trials (ProACT)
New Jersey Community Research Initiative (NJCRI)
Philadelphia FIGHT (FIGHT)
Research and Education Group (REG)
Richmond AIDS Consortium (RAC)
Southern New Jersey AIDS Clinical Trials (SNJACT)
Temple University (TEMPLE)
Washington Regional AIDS Program (WRAP)
Wayne State University (WSU/DMC)
Chicago, Illinois
Bronx, New York
San Francisco, California
Denver, Colorado
New York, New York
Detroit, Michigan
Houston, Texas
New Orleans, Louisiana
New Haven, CT/Boston, MA
Newark, New Jersey
Philadelphia, Pennsylvania
Portland, Oregon
Richmond, Virginia
Camden, New Jersey
Philadelphia, PA
Washington, D.C.
Detroit, Michigan
The Collaborating Centers
Assistance and technical resources for the CPCRA unit staff and the CPCRA governing structure are
provided by the following two collaborating centers:
CPCRA Operations Center
Social & Scientific Systems, Inc. of Silver Spring, Maryland currently holds the CPCRA Operations Center
contract. The CPCRA Operations Center, with offices in Silver Spring, Maryland, provides operations and
logistical support for the CPCRA, as follows:
6
The clinical support section coordinates concept and protocol team activities and develops protocol
drafts, research reports, and literature reviews.
The education/training section develops general and protocol-specific education and training
materials and provides technical assistance for CPCRA clinicians conducting clinical research. The
education/training section also develops patient education materials and is responsible for developing
and distributing the CPCRA Quality Improvement Manual and the CPCRA Investigator’s Handbook.
The administrative support section provides writing, editorial, and word processing support for
meetings and conference calls of CPCRA committees and concept/protocol teams; edits and
manages the production of protocols, educational materials, and reports for distribution; provides
logistical planning and onsite support for meetings and conferences; maintains and distributes the
CPCRA Directory; and edits and produces procedures manuals.
The communications systems section maintains a nationwide electronic mail system and a
computerized management information system (MIS). The MIS tracks the development of protocols,
the membership of protocol teams and committees, the publications and presentations of CPCRA
members, and contact information on all CPCRA members.
CPCRA Statistical Center
The CPCRA Statistical Center is located at the Coordinating Centers for Biometric Research, Division of
Biostatistics, School of Public Health, at the University of Minnesota in Minneapolis and provides senior
scientific statistical leadership for the CPCRA. The responsibilities of the CPCRA Statistical Center include
the design and analysis of CPCRA protocols and the administrative reporting of data from CPCRA studies;
the establishment and administration of a data management system; and the design and implementation of
education and training activities involving statistical and data management issues. Protocol-specific case
report forms, a manual of operations for each protocol, a variety of data collection forms and data reports, the
CPCRA Data Collection Handbook, and the Clinical Events Handbook are among the resources developed
and distributed by the CPCRA Statistical Center.
Funding Source
National Institutes of Health (NIH)
National Institute of Allergy and Infectious Diseases (NIAID)
Division of AIDS (DAIDS)
The Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA)
The Role of the DAIDS
The Division of AIDS (DAIDS) is the funding agency for the CPCRA and, therefore, bears ultimate fiscal,
regulatory, and scientific accountability for all CPCRA activities. In support of these responsibilities, the
DAIDS works with the CPCRA Steering Committee to facilitate the activities of the CPCRA and to
communicate the DAIDS’ priorities and perspectives. Specifically, the DAIDS:
Identifies issues at the NIH, the Department of Health and Human Services (DHHS), and the Public
Health Service (PHS) that are pertinent to the conduct of NIAID-supported community-based clinical
research;
Serves as a liaison between NIAID and organizations or individuals interested in or actively
conducting community-based research on HIV, such as community-based organizations, health
organizations, advocacy groups, and local, state, and federal health and legislative agencies;
Serves as an information resource on activities related to CPCRA research and functioning;
Community Programs for Clinical Research on AIDS
7
Provides a broad framework of the DAIDS’ research priorities and delineates the role of CPCRA
research, particularly as it relates to other DAIDS or PHS-sponsored research and shifts in priorities;
Coordinates drug supply and distribution;
Ensures that all research activities are conducted in accordance with appropriate federal regulations;
Provides review and approval of the CPCRA strategic plan as it relates to the scientific mission and
priorities of the DAIDS/NIAID;
Acts on the CPCRA Steering Committee recommendations related to standards described in the
statement of agreement of each CPCRA cooperative agreement by adjustment of funding,
withholding of support, or suspension or termination of the award; and
Manages all CPCRA budget issues within NIH and DHHS regulations.
DAIDS Contracted Resource Support of the CPCRA
Regulatory Operations Center
The Regulatory Operations Center (ROC) provides extensive technical, research and regulatory support
services for the AIDS Clinical Trials Groups (ACTGs), the CPCRA, and the DAIDS. The ROC provides
support services that are critical to the development and implementation of clinical trials. These include
Investigational New Drug (IND) applications and serious adverse experience (SAE) reporting, maintaining a
system for administering protocol concept sheet and protocol review, and organizing Data Safety and
Monitoring Board (DSMB) support.
The ROC provides the Pharmaceutical and Regulatory Affairs Branch (PRAB) of DAIDS with services that are
critical to the implementation of and distribution to the CPCRA clinical trials:
Compiling and assembling data for submission to the Food and Drug Administration (FDA) for original
IND submissions and subsequent amendments, and individual safety and summary toxicity reports;
Adverse experience data collection and tracking;
Tracking and dissemination of safety reports;
Maintenance of regulatory reports;
Site registration including informed consent review;
Establishing, organizing and maintaining IND, drug company, and related files;
Maintaining inventory and distributing informational materials such as clinical brochures to
investigators and DAIDS personnel; and
Training at CPCRA meetings for serious adverse experience reporting, site registration and informed
consent requirements.
Clinical Site Monitoring Group
The DAIDS Clinical Site Monitoring Group (CSMG) monitors data quality and assures compliance with
Federal regulations with respect to research involving human subjects. Specific services provided by the
CSMG include the following:
Clinical Site Monitoring
The CSMG provides assurance of data accuracy through the conduct of monitoring visits to the
clinical sites. Safety and regulatory issues addressed by the clinical site monitors include review of
informed consents, adverse experiences and regulatory files, and investigational pharmacy audits
and site operations. Full chart reviews on a sampling of protocol-specific research records, as well as
targeted reviews of specific data elements (critical events, inclusive of serious adverse events,
deaths, and clinical endpoints) are conducted at the regularly scheduled site visits. Monitors
participate on numerous protocol development teams and CPCRA committees and subcommittees.
8
The CSMG is responsible for external monitoring of the CPCRA. Monitors visit each main unit every
quarter and more frequently if necessary. Sites are visited twice a year. However, the size of the
site, the number of subjects enrolled, the degree of complexity of the protocols, and the number and
kinds of problems encountered by the staff determine if additional visits are necessary.
CSMG Training
CSMG Training activities focus on protocol-specific sessions conducted at the unit/site to assist
unit/site personnel with the conduct of CPCRA protocols while maintaining the DAIDS policies and
procedures, regulatory guidelines, and good clinical practices. The CSMG, under the direction of the
DAIDS, also collaborates with the CPCRA Operations Center and the CPCRA Statistical Center to
develop specialized programs to meet the education and training needs of CPCRA personnel.
Clinical Research Products Management Center (CRPMC)
The CRPMC stores and distributes investigational products used in clinical investigations sponsored by
the DAIDS. Current support services include:
Receiving investigational products from a variety of sources and storing them under required
conditions;
Shipping and distributing investigational products upon receipt of appropriate order forms
from a site pharmacist, for an authorized investigator;
Performing physical inventories and monitoring use rates of investigational products;
Disposing of returned investigational products as required by local, state, and federal
regulations; and
Establishing a dedicated computerized data processing system to maintain inventory and
distribution records.
Scientific Advisory Board (SAB)
The SAB is an independent board that conducts an external review of the CPCRA science agenda and
the actual science of CPCRA protocols. Their “fresh eyes” provide a unique critique of the CPCRA giving
guidance on our direction. The SAB helps to identify scientific opportunites that the CPCRA may be
uniquely suited to pursue. It also independently evaluates the progress of the CPCRA in meeting its
scientific goals.
CPCRA Meetings and Calls
CPCRA Meetings
CPCRA group meetings are held in the Washington, D.C. area twice each year (usually in the Fall and in the
Spring). The CCG usually meets for a training session on the day preceding the group meeting and
additional sessions are held on the days of the group meeting. The CPCRA Operations Center sends
meeting registration information to all units, CCG members listed in the CPCRA Directory, and other invitees.
CPCRA CCG Conference Calls
The CPCRA Operations Center send notices to CCG members for conference calls via e-mail or fax. The full
CCG usually conducts a conference call on the first Tuesday of each month at 5:00 PM Eastern Standard
Time. Additional standing CCG conference calls for the CCG Steering Committee, National Committee and
Internal Committee are held as needed and times are arranged by the members of those committees.
Annotated List of CPCRA Articles
There is an annotated list of CPCRA protocol-specific, cross-protocol and methodological/ancillary
publications on the CPCRA website at: http://www.cpcra.org.
Community Programs for Clinical Research on AIDS
9
The CPCRA Organization
CPCRA Organizational Chart
CPCRA Bylaws
10
Community Programs for Clinical Research on AIDS
11
CPCRA Bylaws
CPCRA Bylaws
The Terry Beirn Community Programs for Clinical Trials on AIDS
adopted August 8, 1995
revised May 11, 1999
revised April 11, 2000
revised July 8, 2002
12
CPCRA Bylaws
Contents
Introduction
13
CPCRA Mission
13
The CPCRA Organization
Group Leader/Steering Committee Chair
Management Group
Operations Center
Statistical and Data Management Center (SDMC)
Units, Affiliates, and Associates
Laboratories
13
44
15
15
16
16
16
CPCRA Committees and Subcommittees
Steering Committee
Standing Committees
Science Planning Committee (SPC)
Science Advisory Board (SAB)
Publications & Presentations (P&P) Subcommittee
Clinical Events Subcommittee (CES)
Unit Performance Committee (UPC)
Unit Operations Committee (UOC)
Community Constituency Group (CCG)
17
20
21
23
24
26
27
29
31
CPCRA Committee Organization Chart
32
Community Programs for Clinical Research on AIDS
13
Introduction
The Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA) was established in
1989 in order to broaden the scope of the AIDS research effort of the National Institute of Allergy
and Infectious Diseases (NIAID) to include clinical trials conducted in community-based settings.
CPCRA investigators support the design and conduct of long-term strategy trials. The network has
access to a large cohort of patients whose demographics reflect those of the current HIV epidemic.
This approach yields study results that translate into improved clinical care for a wide range of
patients.
1.
CPCRA Mission
To conduct large, efficient, randomized studies, which are broadly generalizable,
and that compare the long-term impact of different strategies for therapeutic
intervention on HIV-1 on viral load, HIV drug resistance, CD4+ cell count,
quality of life, morbidity, and mortality.
The CPCRA Organization
The CPCRA includes a Group Leader/Steering Committee chair, research units throughout the
United States, and a Statistical and Data Management Center. A Coordinating and Operations
Research Center (CORC) oversees fiscal and administrative management of the CPCRA and
includes and Operations Center. These components of the CPCRA, funded through a cooperative
agreement by the Division of AIDS, NIAID, are organized into a clearly defined committee structure
in order to address specific goals. The CPCRA carries out its mission and provides oversight of
ongoing research through the work of the Group Leader, assisted by a Management Group, a
Steering Committee, a Community Constituency Group (CCG), and several standing committees.
These committees are responsible for monitoring performance of the group and enforcing standards,
ensuring the efficient and timely implementation of CPCRA research studies, and assessing unit
activities and providing technical assistance. The CPCRA develops and implements a research
agenda that is consistent with its mission, establishes quality control and performance evaluation
procedures, designs and implements education/training programs for clinicians and patients, and
ensures that there is community representation in CPCRA activities.
14
Group Leader/Steering Committee Chair
The Group Leader/Steering Committee Chair of the CPCRA is a principal investigator of a clinical
research unit and is elected by the CPCRA Steering Committee for the term of the grant award. The
Group Leader has overall responsibility and accountability for the performance of the CPCRA, for
the efficient use of the group’s resources, and for recommending to NIAID the annual funding levels
of all of the CPCRA components. He/she is the day-to-day manager of the group’s activities,
supported by a Management Group. He/she represents the CPCRA in official interactions with
NIAID, regulatory agencies, representatives of other research organizations, and with industry
representatives. The Group Leader is also the principal investigator of the Coordinating and
Operations Research Center (CORC) and is responsible for managing the day-to-day functions of the
CORC, establishing its annual budget, and overseeing the performance of the Operations Center.
With the active support of the members of the Management Group, he/she has the primary
responsibility for developing the scientific, financial, and managerial guidelines for the network.
The Group Leader is responsible for:
Overseeing the development of the CPCRA science agenda and ensuring that studies are
appropriate, use group resources to best advantage, and are implemented, completed, and
reported in a timely way;
Planning, monitoring, and adjusting funds allocated to the CPCRA components and approving
discretionary fund expenditures;
Chairing the Steering Committee and assuring appropriate functioning and coordination of
all CPCRA committees;
Initiating and coordinating activities with collaborating entities, scientific collaborations and
international partners;
Approving standard operating procedures (SOPs);
Ensuring that federally and internationally mandated regulatory and ethical requirements are
met; and
Ensuring the timely submission of grant reports.
Community Programs for Clinical Research on AIDS
15
Management Group
Role of the Management Group
The Management Group advises and assists the Group Leader in carrying out the responsibilities
listed above. These responsibilities include developing and revising policy and the conduct of all
day-to-day activities of the network. Any non-budgeted expenditure of CORC funds in excess of
$5,000 must be approved by the Management Group.
The Management Group will constitute working groups in specialized areas as necessary to support
the implementation of the CPCRA agenda. These working groups are directed by the Management
Group to carry out specific objectives, in a defined timeframe and report directly to the Group
Leader via the Management Group. The Management Group will develop a written statement of
work for each active working group.
The Management Group will review/approve documents as needed, including the executive
summaries from completed protocols; review/approve new associate sites and requests from units to
add sites before being submitted to DAIDS for final approval.
The Management Group Membership consists of:
Group Leader
Steering Committee Vice-Chair
Director of the Operations Center
Principal Investigator of the Statistical and Data Management Center
Chair of the Science Planning Committee
A minimum of two others, as designated by the Group Leader
Operations Center
The CPCRA Operations Center serves as the administrative and fiscal management group for the
CORC and the CPCRA. Operations Center staff will process and track information and
communications between and among the components and members of the group, coordinate and
distribute the group funds, and provide support for the standing committees, subcommittees, and
concept and protocol teams. The Operations Center is also responsible for general education and
training. Further responsibilities include provision of communications support for the CPCRA units
and maintenance of the CPCRA website for the dissemination of information.
16
Statistical and Data Management Center (SDMC)
The CPCRA Statistical and Data Management Center provides the statistical design and analysis of
protocols, data management, and the design and implementation of protocol-specific education and
training activities. The SDMC is also responsible for quality assurance and interim analysis of the
study data.
Units, Affiliates, and Associates
CPCRA units are funded by DAIDS through cooperative agreements for each grant period.
CPCRA affiliate units are funded through the CPCRA CORC to participate in all CPCRA studies
and activities.
CPCRA associate sites are selected by the Management Group to participate in specific studies and
committees.
CPCRA nonenrolling (defunded) units participate in followup of patients in specific studies.
The Principal Investigator of each CPCRA unit, affiliate, and associate is directly responsible for the
performance of the unit/site in terms in terms of recruitment, followup, regulatory issues, the quality
of the data, and adherence to performance standards. Each unit is required to have an active
community advisory board.
Laboratories
The CPCRA Management Group is authorized to use CORC funds to provide central laboratory
support for CPCRA trials. The Group Leader is responsible, with the assistance of the Management
Group, for monitoring laboratory performance.
Community Programs for Clinical Research on AIDS
17
CPCRA Committees and Subcommittees
Steering Committee
Role of the Steering Committee
The Steering Committee serves as the principal policy-making body of the group and is responsible
for the overall CPCRA policy development, making decisions on issues outside of the procedures for
standard day-to-day operations of the group. These authorities are detailed below.
Steering Committee Membership
Voting members of the Steering Committee include:
One representative from each CPCRA unit (Principal Investigator or a designee)
The unit from which the chair is elected will have a vote on the Steering Committee through
an appointed unit representative.
One representative from each CPCRA affiliate (Principal Investigator or a designee)
Director of the Operations Center
Principal Investigator of the Statistical and Data Management Center
Two representatives from the Community Constituency Group (CCG)
One representative from DAIDS
The chair of the Steering Committee will vote only in case of ties. When not acting in the
capacity of the chair, the vice-chair may vote for his/her unit or affiliate. When presiding,
the vice-chair will have a vote on the Steering Committee through an appointed
representative.
Non-voting members of the Steering Committee include:
Principal Investigator of CSMG (or designee)
One representative from each CPCRA nonenrolling unit (Principal Investigator or designee)
(See definition of nonenrolling units on page 6.)
Chair of the standing committees, if not otherwise voting members of the Steering
Committee
Functions of the Steering Committee
The Steering Committee will:
1. Serve as the principal policy approval body of the CPCRA.
2. Elect the Group Leader/Steering Committee chair and evaluate his/her performance on a biannual basis, with the ability to take corrective action or remove him/her for poor performance.
3. Ensure that the operations of the CPCRA are consistent with its mission.
4. Approve the CPCRA Bylaws and revise as necessary.
18
5. Approve major collaborations with other research entities, expansion of associate sites, and
approve scientific partnerships with international partners.
6. Assure community input into the development and implementation of the CPCRA science
agenda, and ensure demographic diversity of the CPCRA study population.
7. Approve the initiation or termination of protocols.
8. Approve the annual CPCRA budget.
9. Approve line-item changes to the approved CPCRA budget in excess of $50,000.
Chair and Vice-Chair of the Steering Committee
Election and Selection Process, and Terms of Office
Election of CPCRA Group Leader/Steering Committee Chair
The CPCRA Group Leader/Steering Committee Chair is elected from the Steering Committee
membership through a process of nomination, followed by a majority vote of the Steering
Committee, with runoff votes as necessary. The chair must be the Principal Investigator of a
CPCRA clinical research unit. The chair may be re-elected for consecutive terms.
Selection of CPCRA Steering Committee Vice-chair
The CPCRA Steering Committee Vice-chair will be chosen by the chair. The vice-chair
must be the Principal Investigator of a CPCRA clinical research unit or an affiliate.
Terms of Office
The term of office for the chair will be the length of the award cycle. The chair will be evaluated
on a bi-annual basis and can be removed by the Steering Committee.
The term of office for the vice-chair is two years. The vice-chair may serve consecutive terms.
The vice-chair will not necessarily succeed the chair.
Responsibilities of the Steering Committee Chair
1. Organize and chair Steering Committee meetings and conference calls;
2. Provide a liaison between DAIDS and the Steering Committee and be a spokesperson for the
CPCRA with DAIDS;
3. Provide a liaison between the CPCRA and other research organizations, government agencies,
and industry representatives;
4. Represent the CPCRA as required;
Community Programs for Clinical Research on AIDS
19
5. Provide oversight of the standing committees;
6. Report to the Steering Committee on group performance, fiscal status, and adherence with
timelines/milestones; and
7. Review and approve reports, meeting summaries, and other formal committee output.
8. Appoint the chair of each standing committee and approve the group vice-chair with the
assistance of the Management Group.
Responsibilities of the Vice-Chair
1. Provide backup for the chair;
2. Attend and chair meetings and conference calls in the absence of the chair;
3. Lead specific efforts/projects as designated by the chair;
4. Serve as a member of the Management Group.
Responsibilities of Steering Committee Members
1. Must attend Steering Committee conference calls or appoint a designee;
2. Must attend meetings in their entirety or appoint a designee;
3. Must review materials in advance of calls and meetings;
4. Must communicate relevant information from meetings and calls to their staff.
Steering Committee Meetings/Conference Calls
The Steering Committee convenes via standing, monthly conference calls and via face-to-face
meetings at each national CPCRA group meeting (a minimum of once per year) and at other times as
deemed necessary by the chair or the Steering Committee.
The following rules will govern Steering Committee meetings:
1. The Steering Committee chair, or in his/her absence the vice-chair, will oversee the
meeting/conference call.
2. Robert’s Rules of Order will be used to govern meetings.
3. Steering Committee meetings will be open meetings, but it is expected that most of the
discussion of issues will be by members of the committee. The Steering Committee may choose,
from time to time, to meet in Executive Session.
4. A two-thirds majority of the voting membership of the Steering Committee will be required to
start or stop CPCRA studies.
20
5. A two-thirds majority of the voting membership of the Steering Committee will be required to
change the CPCRA Bylaws.
6. A two-thirds majority of the voting members of the Steering Committee will be required to
remove the chair.
7. All decisions, except those specified above, will be made by a simple majority vote. A quorum
of members must be present for a vote to take place.
8. If a Steering Committee member is unable to attend a meeting/conference call, he/she may
appoint an alternate to attend the meeting/conference call and vote his/her proxy.
9. Minutes will be taken of each meeting/conference call and circulated to all voting and non-voting
members of the Steering Committee, Principal Investigators (PIs) and Project Coordinators of
units in a timely manner.
CPCRA Standing Committees
The following standing committees have been established by the CPCRA: Science Planning
Committee (SPC) and its Publications and Presentations (P&P) Subcommittee and Clinical Events
Subcommittee, the Unit Performance Committee (UPC), the Unit Operations Committee (UOC), the
Community Constituency Group (CCG). The standing committees report to, and are accountable to,
the CPCRA Group Leader. Each committee has a specific mission that is an integral part of the
function of the entire CPCRA; and these functions will be coordinated by the Group Leader, with the
assistance of the Management Group, thus eliminating duplication of effort.
Standing committees can appoint working groups to focus on specific functions and task forces to
work on short-term specific tasks, with the approval of the Group Leader. The working groups and
task forces will report back to the parent committee with recommendations for action.
Selection Process, Terms of Office, and Evaluation of
Standing Committee Chairs and Members
Chairs of each standing committee will be chosen by the Group Leader, with the assistance of the
Management Group. Vice-chairs and committee members will be chosen by the Group Leader with
the assistance of the committee chair, based on indication of interest and on qualifications for
membership. The UOC will nominate three members for chair and submit the nominations to the
Group Leader. The CCG will elect its chair and vice-chair.
Terms of office for chairs, vice-chairs, and committee members will be 2 years, with the possibility
of reappointment for consecutive terms.
The Group Leader with the Management Group will set standards for effectiveness and participation
on standing committees. On an annual basis, the participation and effectiveness of the committee
chairs, vice-chairs, and members will be evaluated. Chairs, vice-chairs, and members who do not
function effectively may be replaced, and may also be replaced for poor performance at any time at
the discretion of the Group Leader and the Management Group.
Community Programs for Clinical Research on AIDS
21
Science Planning Committee (SPC)
Membership of the SPC
Voting members of the SPC include:
A chair, appointed by the Group Leader, assisted by the Management Group)
A vice-chair, who may be a CPCRA PI, physician, or investigator (appointed by the SPC
chair and the Group Leader)
A Statistical and Data Management Center representative
Three to six additional members, who may be CPCRA PIs, physicians, or investigators
(appointed by the SPC chair, vice-chair, and the Group Leader)
One representative from the Community Constituency Group (CCG) (chosen by the CCG).
(Two CCG members will be chosen to participate and to provide backup for each other, but
they will have one vote on the committee.)
Non-voting members includes:
An Operations Center representative
A DAIDS representative and alternate
(See Selection Process, Terms of Office, and Evaluation of Standing Committee Chairs and
Members on page 11 of these Bylaws.)
Role of the SPC
The SPC has the primary responsibility for developing and carrying out the CPCRA science agenda
and for ensuring the timely dissemination of study results such as publications and presentations and
internal communications.
Functions of the Science Planning Committee
The Science Planning Committee will:
1. Develop and provide scientific oversight for the CPCRA science agenda and provide oversight
of protocol teams, subcommittees, working groups, the Science Advisory Board (SAB),
scientific collaboration, and outside consultants, including the review of executive summaries
upon study completion.
2. Provide scientific oversight of the CPCRA laboratory system.
3. Review, approve/disapprove, and prioritize CPCRA science initiatives.
4. Provide recommendations to the Management Group for members of the SAB, outside
reviewers, and consultants to protocol teams and working groups.
5. Plan and conduct scientific plenary sessions at group meetings, SAB/LAB reviews of CPCRA
science, and science retreats to review current CPCRA science and address major science
initiatives.
22
6. Provide oversight of the Publications & Presentations Subcommittee to ensure timely
presentation and publication of CPCRA study results.
7. Provide general oversight for the function of the Clinical Events Subcommittee.
Responsibilities of the SPC Chair
1. Primary responsibility for planning, organizing, and chairing the science discussions on SPC
conference calls and at SPC meetings and for participating as a member on the Management
Group calls.
2. All protocol teams, SPC subcommittees, and science working groups are accountable to the
Management Group through the SPC chair.
3. Monitor all ongoing studies.
4. Initiate and coordinate scientific collaboration with other research entities.
5. Designate tasks and responsibilities for other SPC members.
Advisory Boards, Subcommittees, and Working Groups
The Science Planning Committee provides oversight of the Science Advisory Board, Publications &
Presentations Subcommittee, and Clinical Events Subcommittee. The SPC may establish ad hoc
working groups in specialized areas as necessary to support the CPCRA agenda, with approval of the
Group Leader. These working groups are directed by the SPC to carry out specific objectives, in a
defined timeframe, and to report periodically to the SPC chair. The membership and duration of
these groups are determined by the SPC, based on interest, expertise, and need relative to the
objective(s) of the group.
Community Programs for Clinical Research on AIDS
23
Science Advisory Board (SAB)
SAB Membership
The members of the SAB will be invited to serve by the CPCRA Science Planning Committee in
consultation with the Management Group. Members will be sought who have made significant
contributions in the field of HIV in the areas of retrovirology, statistical analysis, advocacy,
complications of HIV, and immunology.
Term of Office
Members will be asked to commit to serve a term of two years. (After completion of a term, SPC
may recommend to SC continuation or replacement of any member.)
Functions of the Science Advisory Board
The SAB will:
1. Serve as an ongoing external review panel for the CPCRA.
2. Provide feedback on the scientific merit of the ongoing and planned CPCRA science as well
as to provide input on scientific opportunities that might be addressed by the CPCRA within
the planned agenda.
3. Evaluate the progress of the CPCRA in meeting its scientific objectives.
4. Provide written recommendations and feedback to the SPC and CPCRA Management Group.
24
Publications & Presentations (P&P) Subcommittee
P&P Subcommittee Membership
Voting members of the P&P Subcommittee include:
A chair, who may be a CPCRA PI, physician, or investigator (appointed by the Group Leader
and the Science Planning Committee chair, assisted by the Management Group)
A vice-chair, who may be a CPCRA PI, physician, or investigator (appointed by the Group
Leader and Science Planning Committee chair)
Three to six representatives from CPCRA research units, including a minimum of two
CPCRA physicians (appointed by the Science Planning Committee chair and the Group
Leader)*
One representative from the CPCRA Statistical and Data management Center
One representative from the CPCRA Operations Center
One representative from the Community Constituency Group, chosen by the CCG
*One of the three representatives from CPCRA research units, the chair, or the vice-chair
must be a member of the SPC and will serve as a liaison to that committee.
Nonvoting members include:
Staff from CPCRA units/centers and representatives from DAIDS are welcome to participate
(See Selection Process, Terms of Office, and Evaluation of Standing Committee Chairs and
Members on page 11 of these Bylaws.)
Role of the P&P Subcommittee:
The P&P Subcommittee reports to the SPC and has responsibility for ensuring the timely publication
and presentation of CPCRA study results and for reviewing publications and abstracts prior to
publication/presentation.
Functions of the P&P Subcommittee
The P&P Subcommittee will:
1. Ensure and expedite the orderly and timely presentation to clinicians, HIV-infected patients, and
the scientific community of all pertinent data and conclusions resulting from CPCRA studies.
2. Ensure that all scientific publications and presentations involving CPCRA studies are accurate
and scientifically sound and adhere to the P&P authorship format.
3. Ensure that all CPCRA investigators and collaborating clinicians, professional and scientific
support individuals, and DAIDS staff have the opportunity to participate and be recognized in
CPCRA scientific publications and presentations, as appropriate.
4. Establish procedures that allow DAIDS to exercise its final review responsibility for all scientific
publications summarizing CPCRA study results.
Community Programs for Clinical Research on AIDS
25
5. Maintain a record of CPCRA scientific publications, abstracts, and presentations.
6. Review abstracts prior to the conference submission deadline.
7. Serve as arbitrator for the writing team when the writing team is unable to resolve issues related
to the preparation of a paper or abstract. Arbitration includes replacing the lead author (chair of
the writing team), if necessary.
8. Review and revise the P&P Policy & Procedures as needed.
9. Maintain, revise, and distribute a slide library of information on completed and open CPCRA
protocols.
(See the P&P Policy and Procedures for additional information.)
Role of the P&P Chair
1. Ensure that P&P Subcommittee functions are completed.
2. Designate assignments to subcommittee members.
3. Lead P&P Subcommittee conference calls and meetings.
4. Review data analysis requests, abstracts, and/or papers in the event that a P&P Subcommittee
review is not possible.
5. Prepare and submit an activity report to the Science Planning Committee.
6. Prepare and distribute letters and e-mail messages to authors and units/centers, as needed.
Responsibilities of the Vice-Chair
1. Provide backup for the chair.
2. Attend and chair meetings and conference calls in the absence of the chair.
3. Lead specific efforts/projects as designated by the chair.
26
Clinical Events Subcommittee (CES)
CES Membership
The CES membership consists of:
A chair, which may be a CPCRA PI, physician, or investigator (appointed by the Group
Leader and the Science Planning Committee chair, assisted by the Management Group).
Physician and expert members from both within the CPCRA and outside the CPCRA,
selected with consideration to their areas of expertise vis-à-vis the current needs of the
CPCRA (appointed by the Science Planning Committee chair and the Group Leader). While
it is expected that the subcommittee membership will be limited to approximately five to six
members, that number may be increased in response to future developments.
A coordinator from the CPCRA Statistical and Data Management Center.
One representative from the CPCRA Operations Center.
(See Selection Process, Terms of Office, and Evaluation of Standing Committee Chairs and
Members on page 11 of these Bylaws.)
Role of the CES
The CES reports to the SPC and has responsibility for (1) defining and periodically evaluating
the CPCRA clinical events definition and criteria, (2) reviewing documentation of events
reported as potential endpoints in CPCRA clinical trials to determine whether an endpoint has
been reached, and (3) providing clinical expertise to CPCRA protocol teams when requested.
Functions of the CES
The CES will:
1. Define and periodically evaluate the CPCRA clinical events definition and criteria and
recommend changes when necessary.
2. Ensure that endpoint information is collected and reviewed in a standardized manner across
clinical sites and protocols.
3. Review documentation of potential endpoints and provide an assessment as to the level of
diagnostic certainty of any event that does not meet the criteria for a confirmed diagnosis.
4. Report annually to the SPC on CES activities.
Community Programs for Clinical Research on AIDS
27
Unit Performance Committee (UPC)
UPC Membership
Voting members of the UPC will include:
A chair, who must be a CPCRA PI (appointed by the Group Leader, assisted by the Management
Group)
A vice-chair, who also must be a CPCRA PI (appointed by the UPC chair and the Group
Leader)
A minimum of two additional PIs or, at the discretion of the Group Leader, other CPCRA
physicians with relevant expertise (appointed by the UPC chair and the Group Leader)
Three nonphysician clinicians (appointed by the UPC chair and the Group Leader)
A Management Group Representative
Nonvoting members will include:
An Operations Center representative
An SDMC representative
A CSMG representative
A DAIDS representative
A CCG representative (either the chair or the vice-chair of CCG)
(See Selection Process, Terms of Office, and Evaluation of Standing Committee Chairs and
Members on page 11 of these Bylaws.)
Role of the UPC
The UPC will:
1. Establish standards of performance for the CPCRA units and affiliates, develop mechanisms for
evaluating performance, ensure review on a quarterly or as needed basis and provide written
feedback to the units on a semi-annual basis.
2. Ensure that all performance standards are documented and conveyed to members in advance of
their use.
3. Enforce these standards, acting in coordination with the Management Group.
4. Establish a mechanism for redress by any member challenging UPC assessment or planned
enforcement mechanisms.
5. Provide units and affiliates with documentation of deficiencies in need of correction with
timelines for response and correction.
6. Have primary responsibility for developing mechanisms for enforcing standards, up to, and
including, cessation of research/program activity. Enforcement of standards will be
accomplished in conjunction with the Management Group.
28
7. Evaluate cost-effectiveness of unit enrollment on an annual basis and recommend corrective
action where necessary. Following the UPC annual review, the committee will make
recommendations to the Management Group if they determine that a percentage of a unit’s
funding award should be withheld and possibly redistributed when annual funding adjustments
are made.
Role of the UPC Chair
1. Primary responsibility for planning, organizing, and leading the unit performance discussions on
UPC conference calls and UPC meetings, for participation on the Management Group calls, and
for providing reports during Steering Committee calls and meetings.
2. Coordinate revisions to UPC standards.
3. Coordinate UPC review of unit performance and make suggestions to the Management Group
regarding necessary action regarding enrollment.
4. Designate tasks and responsibilities for other UPC members.
5. Report committee concerns and activities to the Management Group.
Role of the UPC Vice-Chair
1. Provide backup for the chair.
2. Attend and chair meeting and conference calls in the absence of the chair.
3. Lead specific efforts/projects as designated by the chair.
Community Programs for Clinical Research on AIDS
29
Unit Operations Committee (UOC)
Membership of the UOC
Voting members of the UOC include:
The Project Coordinators from each active CPCRA unit/affiliate and from each
nonenrolling unit. Each will be expected to participate in standing conference calls and
meetings.
Nonvoting members will include:
An Operations Center representative
An SDMC representative
A DAIDS representative
A CSMG representative
A CCG representative
A Management Group representative
Candidates for the chair will be nominated by the voting membership. Three nominations will be
submitted to the Group Leader who will appoint the chair, assisted by the Management Group. The
vice-chair will be appointed by the UOC chair and the Group Leader.
(See Selection Process, Terms of Office, and Evaluation of Standing Committee Chairs and
Members on page 11 of these Bylaws.)
Role of the UOC
The UOC will:
1. Identify, discuss, and assist in resolving unit issues related to regulatory compliance, quality
assurance, personnel, unit management, fiscal and grant management; communications, and
support and facilitation of CAB development and function.
2. Provide a means of communication between the members of UOC, CORC, DAIDS and
SDMC. Identify, discuss, and resolve issues related to unit distribution of materials and
communications from CORC, CCG, DAIDS, CSMG, SDMC, and the other units. Address
issues related to communications equipment and staff access and training.
3.
Assist in the training and development of PCs
Development of PC orientation curriculum
Development of orientation educational materials
Structured mentoring program
Provision of tools for PC unit management.
4. Provide support for unit performance
Respond to cross unit performance issues as identified by UPC
30
Provide ongoing training and development for PCs
Develop and share tools for improved unit performance
Serve as a resource to UPC for unit specific issues as requested
5. Review sample informed consents prior to their distribution to the field for editorial
comments, implementation issues, or other concerns. These issues will be brought to the
attention of the Protocol Chair and team field representative by the UOC Chair.
6. Identify general cross-unit training needs (e.g., specimen collection and shipping problems,
IRB issues, regulatory compliance, quality assurance) and make recommendations for specific
training to the Management Group.
7. Provide an opportunity for units to identify areas where assistance is needed and offer peer
support with specific problems.
8. Serve as a resource to the Management Group as requested for network development issues
such as selection of new clinical sites and new site orientation.
Role of the UOC Chair
2. Organize and chair UOC committee meetings and conference calls.
3. Provide reports to the Steering Committee during conference calls and meetings.
4. Report committee concerns and activities to the Management Group.
Responsibilities of the Vice-Chair
1. Provide backup for the chair.
2. Attend and chair meetings and conference calls in the absence of the chair.
3. Lead specific efforts/projects as designated by the chair.
Community Programs for Clinical Research on AIDS
31
Community Constituency Group (CCG)
Mission Statement
The CPCRA Community Constituency Group (CCG):
exists to allow input to the CPCRA from communities infected/affected by HIV/AIDS;
exists to integrate the participation of people with HIV and their chosen advocates into the
CPCRA as partners;
represents diverse HIV communities in all aspects of CPCRA operations;
works to ensure the participation of traditionally underserved populations in the clinical research
process; and
provides community input to all aspects of the CPCRA through membership on the CPCRA
Steering Committee, CPCRA Science Planning Committee (and science working groups),
standing committees, and concept and protocol teams.
CCG Membership
CCG representatives become the voice and the link between the CPCRA unit Community Advisory
Board (CAB) and the CPCRA structure. Each CPCRA unit will organize a CAB that will include,
but not be limited to, members of the HIV-infected communities and their advocates. Efforts should
be made to see that the unit’s CAB reflects the local demographics of the HIV epidemic.
Each unit elects one member as a voting member to the CCG. The CCG will elect its leadership
from among its voting members.
Responsibilities of the CCG Representatives
CCG representatives will serve a minimum of a 1-year term, renewable indefinitely.
CCG representatives will attend unit’s CAB meetings and gather feedback on the issues under
discussion.
CCG representatives will communicate the concerns of the unit’s CAB to the other CPCRA
representative(s) and to the CPCRA in general, where appropriate, and will communicate the
decisions and concerns of the CPCRA CCG to the unit’s CAB.
CCG representatives will attend monthly CCG conference calls and CPCRA group meetings,
and will report back to their unit’s CABs. It is particularly important that either the CCG
representative or the alternate participate in the monthly CCG conference calls.
CCG representatives will make their notes, oral presentations/minutes and/or other circulated
materials available to the unit’s CAB Liaison who will make them available to unit CAB
members.
If the CCG representative cannot perform any of the duties expected of him/her, the alternate
will assist.
(See the CCG Mission & Bylaws for complete election and governance information.)
32
CPCRA Organization Chart
Community Programs for Clinical Research on AIDS
33
The CCG Organization
What is the Community Constituency Group?
CCG Organizational Chart
CCG Mission and Bylaws
34
Community Programs for Clinical Research on AIDS
35
What is the Community Constituency Group?
The Community Constituency Group (CCG) is a key CPCRA link to the community. It functions as a
representative body of the local Community Advisory Boards (CABs) from the national network of 16
CPCRA community-based clinical research
units.
Each unit CAB is a volunteer group of
community members that reflects the
demographic makeup of members of the
local HIV-infected community and their
advocates. The CAB provides community
input to its local clinical research unit on
developing and implementing clinical trials.
For people living with HIV,
participation in local CABs and the
CCG provides a real opportunity to
help advance the current level of
HIV/AIDS treatment knowledge.
____________________________________
The members of each unit CAB elect one
representative and one alternate to the CCG. CCG representatives serve for a minimum of a 1-year term,
renewable indefinitely.
CCG members carry out a number of tasks, including serving as representatives of their local CABs,
bringing CAB input to the full CCG, and participating in monthly CCG conference calls. CCG members
also serve on key CPCRA and CCG committees, and participate in CPCRA group meetings held twice a
year in the Washington D.C. area.
The Chair and Vice Chair of the CCG sit on the CPCRA Steering Committee, thus providing a direct
community voice in the governance of the CPCRA.
For people living with HIV, participation in local CABs and the CCG provides a real opportunity to help
advance the current level of HIV/AIDS treatment knowledge. CAB and CCG participation also provides
opportunities to talk to other people living with HIV about treatment issues, and to learn about new
treatment developments.
Some CAB and CCG members may also decide to participate as research subjects in specific CPCRA
AIDS clinical trials, coincidental to their participation in the CPCRA community process.
36
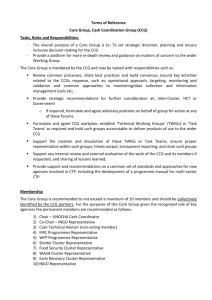
CCG Organizational Chart
CPCRA Steering Committee
Fred Gordin, M.D., Chair and Network Principal
Investigator
CPCRA Community Constituency Group (CCG)
CCG Steering Committee
David Munroe, Chair, CPCRA CCG
Reginald Jackson, Vice-chair, CPCRA CCG
Mark Baker, Chair, CCG Internal Committee
Tom Dionne, CCG Rep, Science Planning Committee
George Kelly, Chair, External Committee
Claire Rappoport, CCG Rep, Science Planning
Committee
CCG Internal Committee
CCG External Committee
Mark Baker, Chair
Harry Dohnert, Vice-chair
George Kelly, Chair
Kevin Pleasant, Vice-chair
Community Programs for Clinical Research on AIDS
37
CCG Mission and Bylaws
Community Constituency Group (CCG)
Mission & Bylaws
(Adopted 1996)
(Revised November 23, 1998; Approved January 5, 1999)
(Revised April 4, 2001, Approved August 7, 2001)
(Revised May 3, 2003; Approved August 7, 2003)
Table of Contents
I. Mission Statement……………………………………………………………………………...
39
II. Organizational Overview……………………………………………………………………….
39
III. CAB/CCG Responsibilities…………………………………………………………………….
40
A. Responsibilities of Individual Members to Their Unit’s CAB…………………………….
B. Responsibilities of the CAB to Their Unit…………………………………………………
C. Responsibilities of CCG Representatives to Their Unit CABs……………………………
40
40
40
IV. CCG Bylaws…………………………………………………………………………………...
41
A. CCG Membership and Voting………………………………………………………….….
41
1. Unit Membership………………………………………………………………………
a. CCG Representative and Alternate(s)..…………………………………………..
b. Unit CAB Liaisons………………………………………………………………...
41
41
41
2. Observers………………………………………………………………………………
41
3. At-Large Members …………………………………………………………………….
42
4. CCG Alumni ……………..………………………………….………………………..
42
5. Advisors ……………………………………………………………………………….
43
6. Liaisons………………………………………………………………………………...
• DAIDS…………………………………………………………………………….
• CPCRA…………………………………………………………………………….
• International……………………………………………………………………….
43
43
43
43
B. CCG Committee Structure…………………………………………………………………
43
1. CCG Steering Committee……………………………………………………………...
44
2. CCG Education & Training Committees……………………………………………...
a. CCG External Committee…………………………………………………………
b. CCG Internal Committee………………………………………………………….
44
44
45
38
C.
Election Process and Responsibilities of Chairs and Vice-chairs………………………….
46
1. CCG Chair and Vice-chair……………………………………………………………
2. CCG Committee Chairs and Vice-chairs……………………………………………..
46
46
Responsibilities of the CPCRA and Each Unit to CCG Representative.………………….
48
1. CPCRA………………………………………………………………………………...
2. Unit…………………………………………………………………………………….
48
48
Responsibilities of the CCG Representative to the CPCRA ………………………………
49
•
•
CPCRA Committees, Subcommittees, and Working Groups………………………...
CPCRA Concept/ Protocol Teams and CPCRA Science Planning Committee
Working Groups………………………………………………………………………..
CCG Committees………………………………………………………………………
CCG Science Representatives ………………………………………………………..
Forum for Collaborative HIV Research……………………………………….
49
Conference Calls and Meetings………………………………………………………….
51
1.
CCG Conference Calls……...……………………………………………………..
a. Purpose………………………………………………………………………..
b. Scheduled Conference Calls………………………………………………….
51
51
51
2.
CPCRA Conference Calls…………………………………………………………
51
3.
Responsibilities of Conference Call Participants…………………………………
51
a.
b.
c.
d.
Attendance…………………………………………………………………….
Responsibilities Prior to the Call……………………………………………...
Responsibilities During the Call……………………………………………...
Responsibilities Following the Call…………………………………………..
51
52
53
53
CPCRA and CCG Meetings and CCG Travel Funding…………………………...
53
a. Meetings………………………………………………………………………
b. CCG Travel Funding………………………………………………………….
53
53
G.
CCG Honorarium (Stipend) ………………………………………….………………....
54
H.
Review of CCG Mission & Bylaws……………………………………………………..
56
1.
2.
56
56
D.
E.
•
•
•
F.
4.
Review Schedule…………..………………………………………………………
Amendments……………………………………………..………………………..
Community Programs for Clinical Research on AIDS
49
49
49
50
39
I.
Mission Statement
The Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA) Community
Constituency Group (CCG):
•
exists to allow input to the CPCRA from communities infected/affected by HIV/AIDS;
•
exists to integrate the participation of people with HIV and their chosen advocates into the
CPCRA as partners;
•
represents diverse HIV communities in all aspects of CPCRA operations;
•
works to ensure the participation of traditionally underserved populations in the clinical
research process; and
•
provides community input to all aspects of the CPCRA through membership on the
CPCRA Steering Committee, CPCRA Science Planning Committee (and science working
groups), standing committees, and concept and protocol teams.
II. Organizational Overview
CCG Representatives become the voice and the link between the CPCRA unit Community
Advisory Board (CAB) and the CPCRA structure. Each CPCRA unit will organize a CAB that
will include, but not be limited to, members of the HIV-infected communities and their
advocates. Efforts should be made to see that the unit’s CAB reflects the local demographics
of the HIV epidemic.
Each unit will elect one member as a voting member to the CCG. The CCG will elect its
leadership from among its voting members.
The unit’s CAB will have an active role in providing input to:
•
•
•
•
Protocol development
Implementation issues
Questions that future research should address
Education and Training:
• • for unit CAB members and the community at large
• • outreach (the value and significance of clinical trial research and impact on care)
• • recruitment (as appropriate)
40
III.
CAB/CCG Responsibilities
A. Responsibilities of Individual Members to Their Unit’s CAB
1. Dedicated individuals are asked to be on their unit’s CAB as outlined in each unit’s
CAB’s Mission & Bylaws. Unit CAB members are asked to provide feedback on
issues regarding clinical trials. This might include ideas for treatments to be considered
in clinical trials, personal experiences in participation on trials, ways to make
participation easier on the patient, etc.
2. Individuals are responsible for attending unit CAB meetings (at the frequency and
timeframe that is agreed upon by the unit’s CAB) and performing other duties as
assigned by the unit’s CAB.
3. The recommended membership term for unit CAB representatives shall be a minimum
of one year (renewable indefinitely), if the unit’s CAB has no term regulations.
B. Responsibilities of the CAB to Their Unit
1. The unit’s CAB is responsible for reflecting and representing the demographic makeup
of the HIV-infected communities in the geographic area of the unit, and providing
community input into the CPCRA clinical trial development process.
2. The CAB of each unit shall elect or select one representative and one alternate to the
CPCRA CCG. Additional representatives and alternates may be named at the
discretion of the unit’s CAB.
C. Responsibilities of CCG Representatives to Their Unit CABs
1. CCG Representatives will serve a minimum of a one-year term, renewable indefinitely.
2. CCG Representatives will attend their unit’s CAB meetings and gather feedback on the
issues under discussion.
3. CCG Rrepresentatives will communicate the concerns of their unit’s CAB to the other
CCG Representatives and to the CPCRA in general, where appropriate, and will
communicate the decisions and concerns of the CPCRA CCG to the unit CAB.
4. CCG Representatives will attend monthly CCG conference calls (see item IV.F.) and
CPCRA group meetings two times per year, and will report back to their unit’s CAB. It
is particularly important that either the CCG Representative or the Alternate participate
in the monthly CCG conference calls.
5. CCG representatives will make their notes, oral presentations/minutes and/or other
circulated materials available to the unit’s CAB Liaison who will make them available
to unit CAB members.
Community Programs for Clinical Research on AIDS
41
6. If the CCG Representative cannot perform any of the duties expected of him/her, the
Alternate will assist.
IV. CCG Bylaws
A. CCG Membership and Voting
1. Unit Membership
a. CCG Representative and Alternate(s). CCG membership will be comprised of
one Representative and Alternate per unit. A unit may choose to name more than
one Alternate to the CCG. Only one vote per CPCRA unit will be allowed.
Representatives and Alternates will be listed on the CCG letterhead.
b. Unit CAB Liaisons. Since the CCG is a community voice and not a unit voice and,
in order to avoid possible conflicts of interest, paid unit staff (i.e., Unit PIs, PCs,
CAB Liaisons, or other Research Nurses or Assistants), who may also be CAB
members, cannot serve as voting representatives or alternates to the CPCRA CCG.
CAB members who are paid unit staff (other than those referenced above) can be
elected to serve and vote on the CCG with its permission. The Unit CAB Liaison’s
contribution as a member of a CCG committee is welcomed. Participation will be
restricted to membership only and not to the possibility of serving as Chair or Vicechair. Unit CAB Liaisons will be included in the CCG Membership Directory and
will receive all mailings and notices that are sent to CCG Representatives and
Alternates.
2. Observers
In order to provide additional expertise; a broader, diverse, and more balanced
perspective; enhance the collaborative effort; and include other research networks in the
CPCRA CCG membership; Observers will be included in the CCG membership. This
category allows an individual to participate without the commitment and
responsibilities of CCG Representatives and Alternates. Observers will be included in
the CCG Membership Directory under the heading CCG Distribution and will receive
call notices. Mailings will be sent to Observers at the discretion of the CCG Chair.
a. Eligibility, Term, and Voting. Observers can be anyone involved in the
HIV/AIDS community at large; and have education and/or personal experience with
HIV/AIDS. There is no term specified for Observers. Observers have no voting
privileges.
42
b. Responsibilities and Expectations. Observers, with prior authorization from the
CCG Chair or Vice-chair, may attend monthly CCG conference calls. Observers
are welcome to attend CPCRA group meetings at their own expense. Expressions
of views and ideas will be welcomed on conference calls and at group meetings,
where appropriate.
c. Miscellaneous. Observers, with prior authorization from the CCG Chair or Vicechair, will be provided with the toll-free telephone number and participant’s access
code for CCG conference calls.
3. At-Large Members
In order to ensure broad representation from people with expertise that is not
included in the CCG membership, the CCG Steering Committee may select up to
four At-Large Members that are approved by a majority vote of the CCG.
a. Voting and Term. At-Large Members will have voting privileges and will be
elected for a term of one year, renewable annually by a majority vote of the CCG.
b. Membership Criteria. At-Large Members may include former CCG members
and/or community advocates from all areas of the U.S.
c. Responsibilities and Expectations.
•
•
•
•
•
•
At-Large Members will communicate concerns of the broader HIV community
with regard to the mission of the CPCRA.
At-Large Members will attend monthly CCG conference calls and the CPCRA
group meeting two times per year.
At-Large Members must join at least one CCG committee.
At-Large Members are encouraged to participate in all aspects of the CPCRA
(i.e., as community representatives to CPCRA committees, subcommittees,
working groups, and concept/protocol teams).
Except as listed in the next item, At-Large Members will be accorded all rights
as that of CCG Representatives.
At-Large members are eligible to seek any elected CCG position with the
exception of the CCG Chair and/or Vice-chair.
4. CCG Alumni
In order to retain the involvement of past CCG members, as well as their accumulated
knowledge, experience, and institutional memory, former CCG members may be asked
to serve as CCG Alumni. The term is unlimited. CCG Alumni will be asked to serve
as such by the CCG Steering Committee. CCG Alumni will be listed on the CCG
letterhead.
While the CCG Alumni are not permitted to vote or hold office, they may be asked by
the CCG Steering Committee to serve on CPCRA committees, subcommittees, working
groups, and/or concept/protocol teams.
Community Programs for Clinical Research on AIDS
43
5. Advisors
In order to provide expertise on a long-term basis, people with HIV, people associated
with the CPCRA, and people outside the CPCRA may be asked to serve as Advisors to
the CCG. The term is unlimited. Advisors will be chosen by the CCG Steering
Committee. Advisors will be listed on the CCG letterhead. Comments from Advisors
are welcomed; however, they will have no voting privileges.
6. Liaisons
Liaisons are established and appointed by various organizations to enhance
communication and networking between various groups. Liaisons will be included in
the CCG Membership Directory and will receive all mailings and notices that are sent
to CCG representatives and alternates. Liaisons will have no voting privileges.
a. DAIDS. A liaison from the Division of AIDS (DAIDS) will coordinate the efforts
between the CPCRA CCG and DAIDS activities; facilitate communication between
the DAIDS, CPCRA, and CCG; and provide guidance when appropriate.
b. CPCRA. The Executive Coordinator of the CPCRA Steering Committee will act
as liaison between the CPCRA committees and the CPCRA CCG to help facilitate
communication between these CPCRA committees and the CPCRA CCG.
c. International. Liaisons with community members of other international clinical
trials groups will be established as needed to enhance the collaborative effort.
CCG Committee Structure
CCG committees were created in order to share the work of the CCG (reducing the
workload of the Chair and Vice-chair), to provide more opportunities for participation by
CCG members, and to make the CCG more effective in carrying out its responsibilities.
Every CCG member must participate on one of the CCG Education & Training
Committees if they are not a representative or alternate on a protocol team. Committee
membership will be open to unit CAB members; however, they may not be elected as Chair
or Vice-chair.
44
The CCG committees are as follows:
1. CCG Steering Committee
The CCG Steering Committee will be comprised of the CCG Chair, Vice-chair, and the
two CCG Education and Training Committee Chairs, and the two CCG Science
Representatives. The role of the CCG Steering Committee will be to oversee the work
flow and deal with logistical issues. The CCG Steering Committee will not make
decisions on behalf of the full CCG.
If participation by the CCG Representative, Alternate(s), or unit CAB members on
CCG committees is not evident, the CCG Steering Committee will report this to the
Unit CAB Liaison and may solicit new membership.
If a committee is not performing as needed, the officers will be evaluated by the CCG
Steering Committee which may suggest to the CCG voting membership that new
elections be held.
Performance of CCG representatives on CPCRA committees and concept/protocol
teams will also be evaluated by the CCG Steering Committee and replacements will be
assigned if needed.
2. CCG Education & Training Committees
a. CCG External Committee
The goal of the CCG External Committee is to develop concrete relationships on a
national/international level through workshop presentations at
conferences/organizations, and to effectively promote better HIV care, access to
treatment, support for AIDS clinical research, and sound public policy.
The committee will:
•
To actively participate with the Operations Center in the selection of
conferences where CCG representation/exposure would be appropriate pending
management approval (i.e., developing conference lists, cost analyses,
justifications, etc.).
• • Develop abstracts/workshop proposals for submission to the aforementioned
conferences for presentation.
• • Develop and revise media/displays for the aforementioned conferences.
• • Develop a mechanism/application process for selecting CCG/CAB members
for attending the aforementioned conferences.
•
To spearhead public policy campaigns to address issues which are sure to
impact the CPCRA in this era of SMART (i.e., the ADAP crisis, the Medicaid
crisis, etc.).
Community Programs for Clinical Research on AIDS
45
•• Develop a future CCG Group Meeting Training Day around these issues
(i.e., bring in a DAIDS and outside legal expert to advise the External
Committee on the fine line we have to walk when doing certain types of
advocacy/public policy work).
•• Develop tools to help CABs to effect change at their local level.
•
To collaborate closely with the Community Relations Coordinator (David
Mariner) at the Operations Center to avoid duplication of effort(s) related to
media exposure.
•
To develop and maintain ongoing relationships and alliances on a variety of
levels with other national organizations. (i.e., NMAC, NAPWA, AMFAR, etc.).
•
To maintain the focus and content of the community section of the CPCRA
website.
–
b. CCG Internal Committee
–
The committee will:
•
maintain the CPCRA CCG/CAB Handbook and keep track of outside
organizations that have requested and received a handbook;
•
identify and prioritize training needs, plan CCG training activities to take place
at group meetings or during conference calls, identify the training and
information needs of unit CABs, especially those that relate to new CAB
members;
•
review and revise the CCG Mission & Bylaws and coordinate the final review
by the full CCG; and
•
recommend improvements in CCG internal communications, including
hardware/software requirements for CCG Representatives and those Alternates
who are active in committee and/or protocol work.
46
C. Election Process and Responsibilities of Chairs and Vice-chairs
1. CCG Chair and Vice-chair
The CCG Chair and Vice-chair are responsible for coordinating the CCG group
activities and representing the CCG on the Steering Committee. An individual may not
be a Chair/Vice-chair of more than one CCG committee.
•
The CCG Chair and Vice-chair will be nominated from the CCG membership
(representatives and alternates) and elected by the CCG. The Chair will be
nominated and elected first, followed by the nomination and election of the Vicechair.
•
The term of office will be two years for both the Chair and Vice-chair.
•
The Vice-chair will not automatically succeed the Chair.
•
Chairs and Vice-chairs may be re-elected.
•
The Chair and Vice-chair will represent his/her unit on the CCG.
•
If the CCG Chair or Vice-chair is not performing as needed, the officer will be
evaluated by the CCG Steering Committee (without the participation of the officer
in question) which may suggest to the CCG voting membership that new elections
be held.
•
If participation by CCG Representatives or Alternates is not evident, the CCG Chair
or Vice-chair may ask the Unit CAB Liaison to facilitate the CAB's
election/selection of another CCG representative or alternate.
•
Unless otherwise specified, the Chair shall facilitate conference calls and meetings
of the full CCG.
•
The Chair and Vice-chair of the full CCG and all CCG committees will comprise
the CCG Steering Committee.
•
The Vice-chair will assist the Chair as needed.
2. CCG Committee Chairs and Vice-chairs
•
The Chairs and Vice-chairs of all CCG committees will be nominated from the
CCG membership (representatives and alternates) and elected by CCG members.
•
A CCG member may not be Chair/Vice-chair of more than one CCG committee.
•
The term of office for the Chair and Vice-chair will be two years for each position
(same timeframe as for the Chair and Vice-chair of the full CCG) and each will be
chosen through a process of nominations from the CCG membership, followed by a
majority vote of the CCG (one vote per unit), with runoff votes as necessary.
Community Programs for Clinical Research on AIDS
47
•
The Vice-chair will not automatically succeed the Chair.
•
Chairs and Vice-chairs may be re-elected.
•
The Chair and Vice-chair of the full CCG and both CCG Education and Training
Committee chairs will participate on the CCG Steering Committee.
•
Responsibilities of CCG Education and Training Committee Chairs
• • Oversee the activities of the committee he/she chairs.
• • The Chair of each CCG committee will attend CCG Steering Committee and
full CCG conference calls/meetings and will report on the activities of the
committee that he/she chairs.
• • Organize and lead CCG committee conference calls/meetings.
• • Act as liaison between the CCG and the CCG Steering Committee.
• • Ensure that committee objectives are met.
• • Make assignments to committee members.
• • Inform the Vice-chair of information from CCG Steering Committee conference
calls/meetings.
• • Represent the CCG committee within and outside the CPCRA as required.
•
Responsibilities of CCG Education and Training Committee Vice-chairs
• • Provide backup for and assistance to the Chair.
• • Attend CCG committee conference calls/meetings and chair CCG committee
conference calls/meetings in the absence of the chair.
• • Represent the CCG committee within and outside the CPCRA as required.
• • Participate in activities of the CCG Steering Committee, as required.
48
D. Responsibilities of the CPCRA and Each Unit to CCG
Representative
1. CPCRA
The Division of AIDS (DAIDS) and the CPCRA Operations Center coordinate and
support CCG travel to CPCRA meetings through the CPCRA Operations Center.
The CPCRA Operations Center funds travel for the following:
• The CCG member from each of the 17 CPCRA units to attend the two group
meetings.
• The Chair and Vice-chair of the CCG to attend any additional Steering Committee
meetings.
• Members or alternates on CPCRA committees, subcommittees, working groups,
and concept/protocol teams to attend special ad hoc meetings (e.g., CPCRA Science
Planning Committee meetings).
CPCRA support for CCG travel is intended to supplement rather than replace the
CPCRA units’ financial support of their CABs. DAIDS encourages the unit to use unit
funds to support the travel of CCG Alternates and other CAB members to CPCRA
group meetings.
Instructions regarding the travel process will be sent to the traveler by the CPCRA
Operations Center.
2. Unit
The unit will:
•
provide the necessary resources to enable the participation of the selected CCG
member;
•
facilitate the CCG Representative's participation in full CCG and CCG Committee
conference calls, CPCRA committee, subcommittee, working group, and
concept/protocol team conference calls;
•
be encouraged to include the unit’s CCG Alternate and/or other unit CAB member
in the list of persons from the unit traveling to group meetings and will provide
timely reimbursement of travel funds;
•
facilitate communication, in the fastest manner possible, between the CCG
Representatives/Alternates and the CPCRA committees, subcommittees,
concept/protocol teams, and working groups, especially when unexpected materials
are sent to the units for distribution;
•
provide computer availability (for e-mail and the CPCRA website) to the CCG
Representative and Alternate (where needed) and handle the cost of operation; and
Community Programs for Clinical Research on AIDS
49
•
E.
provide computers to the CCG Chair and Vice-chair and handle the cost of
operation.
Responsibilities of the CCG Representative to the CPCRA
CCG participation in the work of the CPCRA is to be understood as fully integrated and
vital. Each CCG Representative will participate in the activities of the CPCRA as a
function of his/her interests and skills and the needs/desires of their communities. CCG
representation on the CPCRA committees, subcommittees, working groups, and
concept/protocol teams will be determined through a nomination and voting process of
the CCG members. When voting, the CCG Representative and Alternate(s) will provide
one vote per unit.
•
CPCRA Committees, Subcommittees, and Working Groups. A CCG
Representative and Alternate will be appointed (per the CPCRA Bylaws) or elected
by the CCG to each CPCRA committee, subcommittee, or working group listed
below. The CCG will have the following voting privileges on CPCRA committees:
• • CPCRA Steering Committee - two votes (CCG Chair and Vice-chair)
• • CPCRA Science Planning Committee - one vote (two CCG Science
Representatives)
• • CPCRA Working Groups – one vote as needed
• • CPCRA Unit Performance Committee (UPC) - one vote
• • CPCRA Unit Operations Committee (UOC) - one vote
• • CPCRA Publications & Presentations (P&P) Subcommittee - one vote
– CCG Representatives will attend conference calls and group meeting sessions
and report back to the CCG and their unit’s CAB. The CCG Alternate to these
groups will be encouraged t attend conference calls and group meeting sessions but
are required to attend in the absence of the CCG Representative.
•
CPCRA Concept/Protocol Teams and Working Groups. A CCG Representative
and Alternate will be appointed by the CCG Science Representatives to each
Concept/Protocol Team. Representation on Working Groups will be as needed.
Unit CAB members who are not the unit’s representative or alternate to the CCG
may serve as representatives or alternates on concept and protocol teams.
•
CCG Committees. The CCG Representative will serve on one CCG Education &
Training Committee (CCG External Committee or the CCG Internal Committee).
The CCG Representative will attend conference calls and group meeting sessions
and report back to their CABs. Alternates may participate on these committees,
conference calls, and in group meetings.
•
CCG Science Representatives – The two CCG Science Representatives
will follow the activities of the CPCRA Science Planning Committee.
The CCG Science Representatives will be responsible for coordinating and
monitoring CCG participation in concept and protocol development. This
includes:
50
• • tracking research ideas, concepts, and protocols;
• • tracking which CCG members are interested in different scientific
topics;
• • proposing CCG Representatives to be members on concept/protocol teams and
on working groups;
• • ensuring that there is coverage for all concept/protocol team and
working group conference calls and meetings;
• • considering newer CCG members as alternates on concept/protocol
teams, as a training/mentoring mechanism; and
• • supporting the development of community-generated research ideas.
Committee members should consider ways to highlight community issues that come
up during protocol development, and how best to communicate those issues to the
full CCG and to the unit CABs.
The two CCG Science Representatives will be responsible for coordinating reports
to the full CCG during CCG conference calls on concepts and protocols ongoing
and in development. The CCG Science Representatives will cast one vote on the
CPCRA Science Planning Committee
•
Forum for Collaborative HIV Research (Forum). A CCG Representative or
Alternate will be elected by the CCG membership to serve on the Forum. This
representative will serve on the Forum’s Executive Committee and will participate
on four conference calls and will attend two meetings a year. Depending on the
interest of the representative, he/she may also attend conference calls and meetings
as needed on specific projects. The cost for participating on conference calls and
travel is taken care of by the Forum. The CCG Representative to the Forum will
provide a report at each CCG conference call.
Community Programs for Clinical Research on AIDS
51
F.
Conference Calls and Meetings
1.
CCG Conference Calls
a. Purpose
The full CCG conference calls will include reports from the CCG Chair and
Vice-chair, the Chairs of each CCG Education and Training Committee, the
CCG Science Representatives, the CCG Representative to the Forum, and the
CCG representatives on CPCRA committees, subcommittees, working groups,
and concept/protocol teams. Other CPCRA business will be discussed as
needed.
The CCG committees have established a schedule for their conference calls;
however, calls will be held only as needed to discuss specific business or to
work on assigned tasks.
b. Scheduled Conference Calls
Conference call notices are sent out by the CPCRA Operations Center.
Scheduled conference alls are held for the following committees:
•
•
•
•
Full CCG
CCG External Committee
CCG Internal Committee
CCG Steering Committee
2. CPCRA Conference Call Schedule
CPCRA conference calls are usually held once each month (a list of standing
conference calls is available on the Community Section of Members Website on the
CPCRA website). CPCRA concept/protocol teams and working groups hold
conference calls as needed.
The CCG Representative to CPCRA committees, subcommittees, concept/protocol
teams, and working groups are expected to attend scheduled conference calls.
3. Responsibilities of Conference Call Participants
a. Attendance
Attendance on conference calls is necessary to provide community input to
CPCRA committees, subcommittees, working groups, and concept/protocol
teams and to assist CCG committees in their work. Attendance of at least one
person per unit is necessary on full CCG conference calls. A majority of the
membership of the full CCG or CCG committee shall constitute a quorum for
voting purposes.
52
Absences from conference calls will be excused in the case of health, work
conflicts, conflicts with appointments (doctors, etc.), and conflicts with other
conference calls or meetings. After three unexcused absences in a row, without
the attendance of an alternate, the CCG will appoint another representative to
CPCRA committees, subcommittees, concept/protocol teams, and/or working
groups. After three unexcused absences in a row from full CCG conference
calls where the unit is not represented, the Unit CAB Liaison will be contacted
and asked to facilitate the unit’s election/selection of another CCG member or
alternate.
Every CCG member should participate in the conference calls and meetings of
the CCG group where they have volunteered to be a member.
Each concept/protocol team representative is responsible for covering his/her
concept/protocol team’s call and meetings. If the representative cannot
participate in a call or meeting, he/she must contact the alternate(s). If the
alternate(s) cannot participate, a CCG Science Representative should be
informed who will arrange for coverage. Also, out of courtesy, the
representative should contact the Chair/call facilitator or the CPCRA Operations
Center representative in the case of a call being missed.
b. Responsibilities Prior to the Call
•
Gather required information/input from others as needed (e.g., CAB,
Principal Investigator, research staff, IRB).
•
Read materials (e.g., agenda, minutes) and be prepared to ask/answer
questions, present requested information, and vote.
•
Assign an alternate to be on the call in case of absence. It is the
representative’s responsibility to brief the substitute so that the unit/group
will have adequate representation.
•
Notify the facilitator of the call (Chair and/or CPCRA Operations Center
representative) if nobody will be on the call. For CCG calls, CCG
representatives on a CPCRA committee, subcommittee, working group,
concept/protocol team, or Forum should send a brief report about that group
to the CCG Staff Representative at the CPCRA Operations Center that will
be read during the call and included in the call summary.
•
Respond to requests promptly to ensure representation of your unit/group.
•
Contact the person responsible for the group having a call or the CCG Staff
Representative at the CPCRA Operations Center if the call notice and/or
materials have been lost in order to obtain another copy prior to the call.
Community Programs for Clinical Research on AIDS
53
c. Responsibilities During the Call
•
The CCG participant should not take up valuable time with reviewing
material already discussed on previous calls (if those calls were missed).
The CCG Representative or Alternate who misses a call should first call the
CCG substitute who attended the call for an update. If nobody from the
CCG attended the call, then the Chair or Vice-chair of the group holding the
conference call should be contacted for an update after the call that was
missed.
•
During all calls, the Chair, Vice-chair, or the facilitator is responsible for
running the call. The Chair, Vice-chair, or facilitator will determine how
long a discussion on a particular topic should last, when a subject is closed,
when to call a vote, and when that vote is finished.
•
When you want to speak on a CCG call, introduce yourself by stating your
name and the name of your unit. If you are on a call other than the CCG
then give your name and say that you are from the CCG.
•
If you are volunteering for a position within the CCG or CPCRA, be
prepared to say a few words about why you want the job so that the CCG
representatives will be prepared when the time comes to vote.
d. Responsibilities Following the Call
4.
•
Share information from the call with unit staff and CAB members as
appropriate.
•
Move ahead with action items assigned to you.
•
Gather information needed for the next call.
•
Report activities to the appropriate CCG committee.
CPCRA and CCG Meetings and CCG Travel Funding
a. Meetings
CCG training is usually held on the day before each CPCRA group meeting.
During the group meeting, additional CCG sessions are held.
The CCG Chair and Vice-chair are asked to attend CPCRA Steering Committee
meetings.
The CCG Science Representatives are asked to attend meetings of the CPCRA
Science Planning Committee.
b. CCG Travel Funding
54
The CPCRA Operations Center coordinates and supports CCG travel to CPCRA
meetings through the CPCRA Operations Center as follows:
• One CCG Representative or Alternate from each CPCRA unit to attend the
two group meetings.
• The CCG Chair and Vice-chair to attend the two group meetings and each
additional CPCRA Steering Committee meeting.
• CCG members to attend special ad hoc meetings (e.g., CPCRA Science
Planning Committee meeting).
• One member to attend concept and protocol team meetings (if a CCG
representative, CCG alternate, or unit CAB member is on the team).
Support for CCG travel is intended to supplement rather than replace the
CPCRA units’ financial support of their CABs. Units are strongly encouraged
to use unit funds to support the travel of the CCG Alternate and/or additional
unit CAB members to CPCRA group meetings. CCG members who attend
special ad hoc meetings will be chosen by the CCG Steering Committee.
G. CCG Honorarium (Stipend)
1. Rationale
The CCG is of vital importance to the overall mission of the CPCRA. The CCG
provides community input at a variety of levels across the CPCRA. In addition to
having responsibilities at the national level each CCG Representative has local unit
responsibilities.
To effectively represent the community, numerous hours of preparation and
conference calls are required. The CCG is viewed as a community consultant, asked
to provide two-way information between the CCG and the CPCRA. In addition,
every CCG Representative is expected to attend two national meetings a year. CCG
Representatives and particularly the elected officers, spend considerable time
traveling and attending CPCRA-related committee and protocol meetings.
The honorarium (stipend) system is designed to acknowledge and reward CCG
participation at a variety of levels. CCG Representatives are eligible to receive
honorariums (stipends) in any of the categories outlined below.
CCG Representatives are not and should not be considered CPCRA paid staff. It is
essential to the integrity of the CCG that they are able to raise issues and use their
voices in a constructive, community oriented, sense.
2. Annual Honorarium (Stipend) Levels
a.
CCG Representatives and At-Large Members - $1000 annual
All CCG Representatives and At-Large Members would be required to meet the
Community Programs for Clinical Research on AIDS
55
expectations as outlined in the Administration Section (number 3 below) and the
CCG Bylaws, including active participation in a CCG committee and CCG
conference calls. CCG Alternates do not receive an honorarium (stipend) unless
they fall into a category listed below.
b.
CCG Elected Officers
•
•
•
•
•
•
•
CCG Chair - $3500 annual
CCG Vice-chair - $2500 annual
CCG Science Planning Committee Representatives - $3000 annual each
CCG Internal Committee Chair - $2500 annual
CCG Internal Committee Vice-chair - $1000 annual
CCG External Committee Chair - $2500 annual
CCG External Committee Vice-chair - $1000 annual
All CCG Elected Officers would be required to meet the expectations as
outlined in the Administration Section (number 3 below) and the CCG Bylaws,
including active participation in all CPCRA activities related to the particular
elected office.
c.
CCG Representatives, At-Large Members, and CCG Alumni
Serving on CPCRA Committees, Subcommittees, Concept/Protocol Teams,
and Working Groups - $500 annual
CCG Representatives, Alternates, CAB Members, At-Large Members, or CCG
Alumni who serve on CPCRA committees, concept/protocol teams, and science
working groups as community representatives would be eligible to receive an
annual honorarium (stipend). CCG elected officers are not eligible for an
additional honorarium when service on CPCRA committees is directly
associated with the elected position (i.e., CCG Chair and Vice-chair on the
CPCRA Steering Committee, CCG Science Representatives on the CPCRA
Science Planning Committee). Elected officers would be eligible to receive the
honorarium for CPCRA committee and protocol work which is considered apart
from the elected responsibilities (i.e., a CCG Science Representative who serves
as the community representative to a protocol team).
d.
CCG Representatives, At-Large Members, and CCG Alumni Invited to Ad
Hoc Meetings (as Speakers or Attendees) - $250 per meeting
CCG Representatives, Alternates, CAB Members, At-Large Members, and
CCG Alumni may be asked to represent the community as speakers (i.e.,
SMART Booster meetings).
3. Administration
The CCG Steering Committee will develop and approve minimum standards of
community participation based upon the CCG Bylaws.
Chairs of protocol teams and CPCRA committees will be asked to report to the CCG
56
Chair on the participation of CCG members. CCG Representatives, who meet the
minimum standard, will be certified on a quarterly basis by the CCG Chair that they
are eligible to receive the honorarium (stipend). The CCG Chair will have the
authority to deny any honorarium (stipend) based on the minimum standard of
community participation not being met by the individual CCG member.
The honorarium (stipend) will be processed and distributed by the CPCRA
Operations Center (Social & Scientific Systems, Inc.) within two weeks after the end
of the preceding quarter of the year. The honorarium (stipend) process became
effective with the last quarter of 2001.
Local CPCRA units elect the unit CCG Representative. The CCG will continue to
elect officers. The CCG Chair, in consultation with the CCG Steering Committee,
will appoint CCG members to participate in CPCRA committees, subcommittees,
working groups, and protocol teams.
H. Review of CCG Mission & Bylaws
1.
Review Schedule
The CCG Mission & Bylaws will be reviewed at least once every two years.
2.
Amendments
Amendments to the CCG Mission & Bylaws are approved at any CCG conference
call or meeting, provided that notice of the proposed change(s) and copy of the final
revision shall have been distributed for review at least one month prior to the date
of the conference call or meeting. The revised document should be reviewed and
approved by the unit’s CAB. If the CAB does not meet during the month allowed
for review and approval, the unit’s CCG Representative and Alternate(s) shall
review and approve the document and provide their vote as requested.
Community Programs for Clinical Research on AIDS
57
CAB Organization
CAB Suggested Guidelines
CAB Member Orientation
CAB Action Plan
Mechanisms for Volunteer Recruitment: Local
CABS
58
Community Programs for Clinical Research on AIDS
59
CAB Suggested Guidelines
These Suggested Guidelines were approved by the Recruitment, Outreach, Accrual and Retention Committee
on January 27, 1995, (now known as Unit Operations Committee).The CCG approved including the
guidelines in the CCG/CAB Handbook on November 20, 1997.
Background
In 1989, the National Institute of Allergy and Infectious Diseases (NIAID) awarded contracts to groups of
community clinicians, establishing the Community Program for Clinical Research on AIDS (CPCRA). This
program initiated a new level of clinical research in HIV/AIDS by extending the opportunity for participation in
research to primary care providers and patients traditionally underrepresented in clinical research.
Community Advisory Boards (CABs) are in place throughout the CPCRA in order to foster a partnership
between researchers and persons infected or affected by HIV/AIDS. In addition, community-appointed
representatives serve as members of the CPCRA Community Constituency Group (CCG). CCG
representatives also serve as members of local CABs. It is through this linkage of CABs and the CCG that
the affected communities are able to play a key role in the process of developing and implementing CPCRA
protocols.
Each CPCRA unit is required to document a wide base of support from the community served. At the
cornerstone of the community-based research initiative is the goal of developing research questions relevant
to the community. The CPCRA achieves this goal by including the community, through partnership with the
CABs, in decisions made regarding the design and implementation of protocols. An active CAB with
committed membership enables each unit to function as an integrated participant in the community’s effort to
combat AIDS and provides an established mechanism through which units can solicit support and guidance
from the populations they are mandated to serve.
Purpose
The purpose of this document is twofold:
(1) To define the roles, responsibilities, and relationships of CABs and CPCRA clinicians;
(2) To provide guidelines and standards for developing CABs, planning CAB meetings, selecting
CAB membership, and assigning a CAB liaison.
These guidelines have been developed by the Recruitment, Outreach, Accrual and Retention Committee
(ROARC). They are derived from the experiences of units under the original CPCRA contract and are
designed to maximize CAB functioning. The members of ROARC recognize that there are vast differences
among the communities represented in the CPCRA. Therefore, the following guidelines have been
developed as recommendations rather than regulations.
The CAB Mission
CABs exist to ensure that the needs of the community are considered in all matters regarding the design and
implementation of research-related clinical care, program management, and the establishment of the scientific
agenda. The board members represent the HIV-impacted community as a whole, with particular emphasis on
people of color, women, and injecting drug users.
CAB Operating Guidelines
The total membership of the CAB should be approximately fourteen (14).
Membership is open to all members of the HIV-infected and -affected community who successfully complete a
CAB orientation as defined by each CPCRA unit.
At least 30 percent of the total CAB membership (approximately four members) should be individuals who
self-identify as persons living with HIV infection.
CAB membership excludes CPCRA paid staff.
A CAB should endeavor to have at least seven (7) individuals regularly participate in CAB activities in order to
be considered “active.”
60
A CAB member is considered non-active if he/she is absent from three consecutive CAB meetings or
conference calls without contact with the CAB liaison.
CABs should meet face-to-face or via conference call at least monthly to discuss CAB issues.
The CAB liaison or his/her designee should attend all CAB meetings and conference calls. The liaison may
designate a member of the professional staff (physician, nurse, social worker, etc.) to attend meetings and
conference calls in his/her absence.
Each unit should decide if decisions are made by general consensus or majority vote.
Qualifications and Roles of CAB Members
CAB members should be:
Culturally sensitive to the barriers encountered by populations traditionally underrepresented in AIDS clinical
trials - i.e., women, people of color, and injecting drug users.
Knowledgeable about the medical and social aspects of HIV illness and willing to participate in educational
endeavors to expand and maintain their knowledge base.
Self-motivated and committed to independently pursuing knowledge and information on HIV treatment trends.
Familiar with or eager to learn about CPCRA protocols and the types of research questions relevant to the
communities that the CPCRA targets.
Responsibilities of CAB members include:
Demonstrating interest and commitment to the community-based clinical research initiative.
Participating in the protocol development process and study implementation.
Assisting units in rating concepts, reviewing informed consents, and suggesting strategies to enhance
recruitment to studies.
Providing real-life experience and acting as a resource to the local unit and national CPCRA network.
Helping achieve accrual, recruitment, outreach, and retention goals through consultation on the unit’s
recruitment and outreach plan.
Helping recruit study participants by enhancing outreach strategies, disseminating protocol information to the
local community about CPCRA protocols open to enrollment, and helping resolve problems with enrollment.
Offering information on improving study patient compliance and quality of life through personal experience or
knowledge of community-wide needs.
Assisting in the recruitment of new CAB members.
CAB Liaison Roles and Responsibilities
Each CPCRA unit should designate a paid staff employee to serve as liaison to the CAB. At most units, the
CAB liaison is the social/outreach worker, although other professional research personnel may also serve in
this role. This individual serves as a linkage between the community, unit, and national CPCRA committees
such as the Unit Operations Committee and Science Planning Committee.
The CAB liaison is responsible for:
Coordinating all activities of the CAB.
Ensuring that information is shared between the CAB and unit personnel.
Planning and coordinating CAB meetings and conference calls.
Assembling educational materials and handling administrative duties- e.g., memos and minutes.
Coordinating regular educational opportunities for CAB members to supplement their independent study.
Education may focus on protocol review techniques, new treatments, trends in the illness, epidemiology,
special populations, or any other area of interest identified by CAB members.
Working with the current CAB to identify and recruit new CAB members.
Community Programs for Clinical Research on AIDS
61
CAB Member Orientation
CAB Member Orientation (suggested)
CAUTION - Don’t Overwhelm New CAB Members with Information
Send Orientation Materials Prior to Training
Material (Limited)
Mission
Clinical Trials
Buddy System (Formalized)
Follow-up Phone Call or Meeting
Update on Local CAB Activities
Using CCG Training Materials
Use Other CAB Members to Communicate with New CAB Members (Mentor)
Ongoing Training at All CAB Meetings
Use Physicians to Recruit/Educate
Use Statistical Center/Operations Center Material
Advise on Retention/Follow-up Issues
Be Vocal to Help Activate HIV Community
Select a CCG Representative and Alternate
Develop Process to Recruit/Retain CAB Members
Clinical Trials 101 - Part 1
CAB/Unit Interaction (suggested)
Unit Liaison Involvement
Non CAB Meeting Function (Social-Educational)
PI Involvement
Communication with Entire Staff
Attend Physician/Consortium Meeting
Distribute CAB Information (Minutes/Notices) to Staff Members
Use Unit Staff as a Resource
Administrative Support for CAB Meetings
Meeting Agenda Topics with Staff Input/Involvement
Information on General CPCRA Structure
Know CCG Representative and Alternate
Sit in on CCG Conference Calls
Invite New CAB Member to Unit
Concept/Protocol Process Education
Process for Protocol Evaluation
Suggested CAB Activities
Campaign to Educate Patients About Clinical Trials
Patient Education Programs (General Public)
Clinical Trials 101 - Part 2
Brochure on CPCRA/CAB
Update/Disseminate Clinical Trials Information
Patient Education Handbook
Outreach Advice
Develop Mission Statement/Bylaws
Produce High Quality Educational Materials
Communicate with the Unit
Review Protocols
Review Education Material
Recruitment Advice
Educate Members (CAB)
Inform Unit About What’s Happening in the HIV Community
62
Help Unit Understand HIV Community
Good Representation of Local HIV Community
Networking
Free-Flowing Dialogue
Trusting Environment
Sensitivity to Target Population (Women, People of Color, Injecting Drug Users)
Suggestions for a Successful CAB
Committed Unit Liaison
CAB Members Feel That They Do Have Input
PI Involvement
CAB Member Orientation
Clearly Stated Mission/Goals of the CAB
Who’s Responsible for What in the CAB?
Bylaws (Method of Governance)
Regular Meetings
Food!
Comfortable Meeting Space
Meeting Agenda Determined by the CAB
Organized Correspondence (Minutes and Notices)
Administrative Assistance
Education (Ongoing)
Transportation
Good Facilitation
Clear understanding of how decisions are made
Clear understanding of the feedback mechanism with regard to CAB suggestions about trials
Community Programs for Clinical Research on AIDS
63
CAB Action Plan
PURPOSE
To establish a well-defined quantifiable goal and specific, concrete objectives to produce an action plan
for your local CAB.
INSTRUCTIONS
1. Develop a well-defined goal.
2. List the specific objective (activity) to accomplish the goal.
3. List the timeframe when the objective will be completed.
4. List the individual/group responsible for completing the objective.
5. List the resources needed to accomplish the objective.
6. List the barriers to completing the objective.
EXAMPLE:
Goal:
Objective:
To diversify the membership of our local CAB.
To identify: gender, ethnicity, age, HIV status, service organization/affiliation of
members.
Timeframe:
January 2003
Responsible Party: CAB Membership Committee
Resources:
Unit clerical staff time needed to survey individuals and compile the data.
Barriers:
Inaccurate list of CAB members.
GOAL:
OBJECTIVE 1
Timeframe
Responsible Party
Resources
Barriers
OBJECTIVE 2
Timeframe
Responsible Party
Resources
Barriers
OBJECTIVE 3
Timeframe
Resources
Barriers
Responsible Party
64
Mechanisms for Volunteer Recruitment: Local CABS
(Compiled from the National CAB Survey)
Develop CAB brochure and CAB application forms
Recruit at community forums and speaking engagements - bring application forms and CAB brochures
Personal contact by other CAB members
Personal contact by unit staff, especially MDs, nurses, and social workers
Word-of-mouth, self referral
PWA coalitions and other community-based AIDS service organizations
Place flyers and application forms in community and in clinics
CAB newsletter
Outreach workers
Ask CAB members to bring a friend to CAB meetings
Ask affiliated AIDS service organizations to appoint members
CAB recruitment committee
Advertise in local papers, ASO newsletters
Outreach to support groups
Community Programs for Clinical Research on AIDS
65
Organizations & Contacts
CCG Membership Directory
List of Key CPCRA Contacts
Clinical Trial Contacts
National AIDS Organizations
AIDS Treatment Resources
AIDS Publications Contacts
66
Community Programs for Clinical Research on AIDS
67
CCG Membership Directory
68
Community Programs for Clinical Research on AIDS
69
70
Community Programs for Clinical Research on AIDS
71
72
Community Programs for Clinical Research on AIDS
73
74
Community Programs for Clinical Research on AIDS
75
76
Community Programs for Clinical Research on AIDS
77
78
Clinical Trial Contacts
DAIDS (Division of AIDS)
http://www.niaid.nih.gov/daids
The National Institute of Health Division of AIDS funds numerous research networks including:
AACTG (AIDS Clinical Trials Group)
http://aactg.s-3.com
8757 Georgia Avenue, Suite 1200
Silver Spring, Maryland 20910
(301) 628-3000
CPCRA (Community Programs for Clinical Research on AIDS)
http://www.cpcra.org
8757 Georgia Avenue, Suite 1200
Silver Spring, Maryland 20910
(301) 628-3000
FAX: (301) 628-3306
HPTN (HIV Prevention Trials Network)
http://www.hptn.org
Family Health International
PO Box 13950
Research Triangle Park, NC 27709
(919) 544-7040
HVTN (HIV Vaccine Trials Network)
http://www.hvtn.org
HIV Vaccine Trials Network – FHCRC
1100 Olive Way, MW500
Seattle, WA 98101
(206) 667-6350
PACTG (Pediatric AIDS Clinical Trials Group)
http://pactg.s-3.com
8757 Georgia Avenue, Suite 1200
Silver Spring, Maryland 20910
(301) 628-3000
AIDSinfo
http://AIDSinfo.nih.gov
P.O. Box 6303
Rockville, MD 20849-6303
1-800-HIV-0440 (1-800-448-0440)
Canadian HIV Trials Network
http://www.hivnet.ubc.ca/ctn.html
620 - 1081 Burrard Street
Vancouver, BC V6Z 1Y6
(604) 806-8327
Fax (604) 806-8210
Community Programs for Clinical Research on AIDS
79
National AIDS Organizations and Related Organizations
AIDS Action
http://www.aidsaction.org
1906 Sunderland Place NW
Washington, DC 20036
(202) 530-8030
Fax: (202) 530-8031
AIDS Alliance for Children, Youth & Families
http://www.aids-alliance.org
1600 K Street, NW Suite 300
Washington, DC 20006
(202) 785-3564
Fax: (202) 785-3579
AIDS Community Research Initiative
http://www.acria.org
230 W 38th Street, 17th Floor
New York NY 10018
(212) 924-3934
fax: (212) 924-3936
AmFAR (American Foundation for AIDS
Research)
http://www.amfar.org
1828 L Street, NW, #802
Washington, DC 20036-5104
(202) 331-8600
Fax: (202) 331-8606
Elizabeth Glaser Pediatric AIDS Foundation
http://www.pedaids.org
1730 Rhode Island Ave. NW, Suite 400,
Washington, D.C., 20036
(202) 296-9165
Fax: (202) 296-9185
Committee of Ten Thousand (COTT)
906 D Street, NE
Washington, DC 20002
(800) 488-2688
Gay Men's Health Crisis
http://www.gmhc.org
The Tisch Building
119 West 24 Street
New York, NY 10011
(212) 807-6655
National Association of People with AIDS
(NAPWA)
http://www.napwa.org
NAPWA, 1413 K Street, NW
Washington, DC 20005
(202) 898-0414
fax: (202) 898-0435
National Hemophilia Foundation
http://www.hemophilia.org
116 West 32nd Street, 11th Floor
New York, NY 10001
(212) 328-3700
fax: (212) 328-3777
National Minority AIDS Council (NMAC)
http://www.nmac.org
1931 13th St, NW
Washington, DC 20009
(202) 483-6622
fax (202) 483-1135
80
AIDS Publications Contacts
The Active Voice
http://www.napwa.org
National Association of People with AIDS
1413 K. Street N.W.
Washington, D.C. 20005
202-898-0114 or Fax 202-898-0435
AIDS Treatment News
http://www.aidsnews.org
P.O. Box 411256
San Francisco, CA 94141
800-treat-1-2 or Fax 415 255 4659
Being Alive
http://www.beingalivela.org
3626 Sunset Blvd.
Los Angeles, CA 90026
213-667-3262 or Fax 213-667-2735
Bulletin of Experimental Treatments for AIDS
http://sfaf.org/beta
Infocom Group
1250 45th Street, #200
Emeryville, CA 94608-2924
900-959-1059 or Fax 510-596-9342
Critical Path AIDS Project
http://www.critpath.org
2062 Lombard Street
Philadelphia, PA 19146
24 hour treatment hotline 215-545-2212
Gay Men's Health Crisis, Inc.
http://gmhc.org
129 West 20th Street
New York, NY 10011
1-800-AIDS-NYC in NYC or 212-807-6655
Medical Alert
National Association of People with AIDS
http://www.napwa.org
1413 K. Street
Washington, D.C. 20005
202-898-0141 or Fax 202-898-0435
NATAP Reports
http://www.natap.org
NATAP 580 Broadway Ste 403
NY, NY 10012
212 219-0106
NIAID "AIDS Agenda"
National Institues of Health
Building 31, 7A50
Bethesda, MD. 20892-2520
Community Programs for Clinical Research on AIDS
81
Positively Aware
http://www.thebody.com
1258 West Belmont Avenue
Chicago, IL 60657-3292
312-472-6397 or Fax 312-472-7505
Positively Living
http://www.apla.org/apla/ed/publications.html
AIDS Project Los Angeles
1313 N. Vine Street
Los Angeles, CA 90028
2130993-1362 or Fax 213-993-1592
POZ
http://www.poz.com
Box 1279 Old Chelsea Station
New York, NY 10113-1279
800-883-2163 or Fax 212 675-8505
Project Inform
http://www.projinf.org
1965 Market Street #220
San Francisco, CA 94103
800-822-7422 or Fax 415-558-0684
Searchlight
AIDS Research Alliance
http://www.aidsresearch.org
621-A N. San Vincent Blvd.
West Hollywood, CA 90069
310-358-2423 or Fax 310-358-2431
STEP
Seattle Treatment Education Project
http://www.thebody.com/step/stepix.html
1123 East John Street
Seattle, WA 98102
(206) 329-4857
(877) 597-7837 (toll-free, valid only in the Pacific Northwest)
TAG LINE
http://www.aidsinfonyc.org/tag
350 Seventh Avenue
Suite 1603
New York, NY 10001
212-971-0022 or Fax 212-971-9019
Women Alive
http://www.women-alive.org
1566 S. Burnside Avenue
Los Angeles, CA 90019
323-965-1564, FAX 323-965-9886
Hotline: 1-800-554-487
82
Community Programs for Clinical Research on AIDS
83
Resources
CPCRA Meetings: Helpful Hints for Attendees
CPCRA Talking Points for CCG/CAB Members
Getting Started: Being A Community Advocate
Sitting at the Table
How to Critically (and quickly) Read a Protocol
Additional CPCRA Resources
84
CPCRA Meetings: Helpful Hints for Attendees
This information has been prepared to help attendees to have a good and productive experience at CPCRA
meetings.
Remember:
All of us have had the experience of attending our first meeting. Yes, it was a bit
overwhelming at first, but with the help of people back home and other attendees, it
turned out just fine.
Remember:
This is your meeting. You are among friends. Make the most of it. Meet new
people. You are all here for the same reason. Ask Questions!
Remember:
Each of you is an important, productive asset to the CPCRA.
Pre-meeting Preparation
Once you have received the information on the conference:
Talk to your unit CAB liaison or other CAB or CCG members. They
can help you by telling you what to expect when you arrive: what to do at
registration, where to sit during a session, how best to mingle, what kinds of
questions to ask and when to ask them.
Read the agenda – for both the CCG meetings and the conference as a whole.
Ask someone to help you prepare some questions in advance.
Come prepared with information regarding your unit, such as the names of unit staff, CAB and CCG
members names, and other CPCRA contacts; the types of clinical studies conducted at your unit; and
how often your CAB(s) meet.
Bring ideas and achievements from your unit. Discuss them with the unit staff and CAB/CCG members.
Onsite Meeting Hints
Participate in the buddy or mentor system. If you’ve been to a
meeting before, help someone who hasn’t.
Don’t be shy: If you have a question—ask it. If you have a
comment—say it.
Take notes. Even though you’ll receive material to take home to
your unit, you may want to write down your thoughts to share with
your CAB and community back home.
Fill out the Conference Evaluation Form. Your opinions are valuable. They will help us plan the
next conference.
Community Programs for Clinical Research on AIDS
85
CPCRA Talking Points for CCG/CAB Members
CPCRA Background
Formed in 1989 to incorporate clinical research into primary care settings, where most people with HIV
receive care 17 CPCRA units in 17 US cities (over 160 individual physicians’ offices and clinics)
Objectives of the CPCRA
Conduct scientifically sound research relevant to the day-to-day management of HIV disease
Integrate research into the primary care of persons with HIV disease
Develop research questions relevant to community settings and to individual communities
Involve community-based primary care providers in scientifically sound HIV clinical research
Include in clinical research people previously under-represented: women, people of color, and
injecting drug users
Benefits of Community-Based Research
Access to a representative patient population = more generalizable results
Patients enrolled with minimal disruption of their daily lives
Research conducted in a “real world” setting
Excellent follow-up of trial participants over time, very low lost-to-follow-up rates
Accurate tracking of multiple clinical endpoints/events
Ability to address basic primary care issues
Speeds translation of scientific advances to primary medical practice
CPCRA Achievements
Over 20 studies completed, enrolling over 25,000 participants
Study results based on “real world” intent-to-treat analysis
Over 500 primary care practitioners involved in AIDS clinical research
Median follow-up of 22 months with lost-to-follow-up rates generally below 3%
Innovations in clinical trial methodology, simplifying and standardizing data collection, definition of
endpoints, randomization of participants, and co-enrollment in multiple studies
Cross-study database used for observational analyses and trial design
86
Getting Started: Being A Community Advocate
The following was originally collected by Julie Davids for Project TEACH, with help from Charles Nelson,
Kiyoshi Kuromiya, and Jane Shull.
1. It is important that you are doing this: Serving as a community representative is hard work. Other people
have more experience than you, and may know more about the topic or the unspoken rules of meetings and
power. But you are an expert about your life and your community, and you can learn everything else. It can be
scary to speak up, especially the first time you disagree with a powerful person. Remember that you are doing
the right thing and speaking the truth, and you need to be heard. No one was born knowing how to do this,
and it will get easier. It is a challenge and you will have to take risks, but it will also teach you about yourself
and help people have longer and better lives.
2. Pick an issue or an organization to focus on -- and follow it wherever it goes. No one can know
everything, or do everything. Whether you are interested in tuberculosis, or your local AIDS Organization, or
teenagers with HIV, read all you can or ask people who know the most about the issues. Then start going to
meetings where decisions are made that affect peoples' lives. You will become the expert and feel more
comfortable speaking up.
3. Don't get isolated: It is usually a good idea to avoid being the one person living with HIV (or vaccine
volunteer) on a committee or panel. Demand that there are at least two, and ask to help select the other
person or people -- then meet ahead of time and between meetings to plan strategy. Get a list of who else is
on the committee, before you go to a meeting, and ask around about the other people. If you hear good things
about someone, call up and introduce yourself and ask any questions you may have. Don't judge people by
their title or position, but by their reputation and your experiences with them. Some researchers or
bureaucrats will give you good information and explain things clearly. Some “community members” may not
be trustworthy or share your beliefs and goals.
An affinity group is a group of people who work together on a certain issue. You could form an affinity group
to support you on this committee -- even if the other people are not on this committee -- as they may have
access to information and could help you figure out what to do. A support person can be someone who will
really stick with you, help you keep track of the process and your role in it, and let you complain. It should be
someone you like and trust, and can be someone who has been in your position or a similar situation.
Make contacts, and use them. Once you have found good people on your committee, or in the outside world
who know about the issues, talk to them often. If you have a question about a term or idea that comes up in a
meeting or on a conference call, and you do not feel comfortable asking about it right away, write it down and
ask it later.
4. Do your homework: If you are sent information before a meeting, read it or find someone to help you go
through it. Write down any comments or questions or anything that seems strange. If you need more
background information on the topic, call an expert or ask someone who has been in your position before.
Sometimes you will be sent too much information, and your contacts can help you decide what is important.
Other homework includes thinking about what is likely to happen at the meetings. What might you have to
speak up about? What will you say? How will others respond? What are arguments against your position, and
how will you take them on? Discuss this with your contacts and others who are working on the issues, or who
have worked with the people on your committee before!
5. Don't try to do everything: You cannot be on every committee and board and do a good job. Share the
load with your peers - - if they are new to this, make sure they fight for training and support them as they learn
and grow. Know your limits, and do not spread yourself too thin!
6. Make sure to take care of yourself.
Community Programs for Clinical Research on AIDS
87
Sitting at the Table
The following was collected by Julie Davids for Project TEACH, with help from Charles Nelson, Kiyoshi
Kuromiya, and Jane Shull.
1. Remember the people who aren't in the room: You are there to represent your community, not to
impress the other people at the table. You must be clear about what your community needs and wants, and
report back information to people who are not there. If you are sitting on a scientific committee designing
research, you don't have to be a scientist -- you need to think about and talk about how their research will
affect your community. Don't be afraid to go back and ask your community what they think.
2. Set goals to focus your participation: Your homework is to know the issue, and figure out how it affects
you and your community. What can this group or committee do about this issue? Your goals must be clear,
wellthought out, and possible for this group of individuals to do at this time. You can have goals for each
meeting, and overall goals for the committee's work. What goals must be met, and what goals are you willing
to compromise in order to win the most important
things? Discuss these with your contacts and
supporters. If you learn more or situations change,
Focus on what you do understand,
look again at your goals and change them if
necessary.
not what you don’t yet understand. It
is easy to become discouraged, but
3. Be truly present: You need to be there
remember that you have support and
physically, mentally, and emotionally. The first key
can learn.
to this is showing up. Go to all the meetings. If they
____________________________________
do not meet at times you can attend, demand that
the times change, or find someone else to take your
place. If they communicate through conference calls, be on all the calls, or you may miss important
information.
Listen to everything. It is not helpful for you to demand an answer to a question that was already answered 10
minutes ago. Try your best to keep track of the conversation. If you ask a question, you must listen to the
answer -- do not assume you know what they are going to say. It is very easy to get distracted, especially on
conference calls. Try to notice when you are not listening, and learn to concentrate on what is going on. Bring
a tape recorder if you have trouble remembering the details or taking notes, and review it later.
Stay awake. If you find yourself getting sleepy, stand up or walk around if possible. Go to the bathroom and
splash cold water on your face. Don't load up on coffee and sweets -- it can just lead to a crash. Snacks like
nuts and fruit can give you a better energy boost.
Focus on what you do understand, not what you don't yet understand. It is easy to become discouraged, but
remember that you have support and can learn. Picture ideas in your head at first, rather than trying to write
down details, especially with scientific and treatment issues.
4. Make all your comments and get your questions answered, sooner or later: You always have the right
to ask questions. If you do not understand something, and no one is helping you, interrupt the meeting and
demand an explanation. If you have a comment to make, do not let the conversation or meeting end until that
comment is made.
If you ask a question, and feel that it was not answered all the way, point that out. If you still feel like you are
getting the run-around, you have to make a decision -- should you continue to interrupt the meeting, or will
you give up for now and get your answer later from one of your contacts? Either decision is the right one at
different times -- it will become easier to tell with experience.
If you are not sure of how to say something important or sensitive during a meeting, make yourself a note.
Then work with your contacts and supporters afterwards to write a letter to all the committee members, stating
your position, and email or fax it to them or bring it to the next meeting.
88
Don't be afraid of disagreements, even with your contacts and allies. A good working relationship can include
arguments, so people know where you stand and that they can't walk over you. Do stay open and honest
without making personal attacks.
Sometimes you may have to pick your battles, and let things go if you can get an answer outside the meeting,
or come back with a stronger suggestion or proposal next time. Remember, you are there to meet your goals,
in order to help your community. If you call someone a "murderer" the first time you have a minor
disagreement or because they say something dumb, they may never listen to anything you say again. Some
people will say ignorant or offensive things to distract you from the real issues -- don't fall for it.
Avoid making up facts and figures. You may get caught. If you are pretty sure, say "I think that..." or "I believe
that...", and hope that someone else in the room can back you up. Or write a note to a contact near-by, asking
if they know and can make the point. Sometimes you may need to bluff to bring out an important issue or
make a point. You can act like you know the details without saying any. Use words like "approximately,"
"about," or "roughly" to describe your best guess, as in "About half the people dropped out of the study
because of side effects. Obviously there is a problem here."
5. Get in on the details. Most of your goals may be for big issues and decisions. But smaller things can
make a large difference, too. Sometimes the people who write the
final wording of a policy or decision have the most power. Do not
give your okay for a general statement and go home -- help write
it, or demand to see a copy before it is made final or sent out!
Most of your goals may be for
For example: If you are a representative for clinical trials, it is very
important to look at the details of the study. Will people have to
come in every week for a blood collection? How will they get
there? Do they really need all that blood?
Community Programs for Clinical Research on AIDS
big
issues and decisions. But smaller
things can make a large difference,
too.
____________________________________
89
How to Critically (and Quickly) Read a Protocol
Prepared by Dr. Jeffrey Schouten for the Adult AIDS Clinical Trials Group.
One of the challenges of being a CCG member is learning how to critically review a protocol from a
community perspective. These suggestions will help you focus on the most critical areas of the protocols you
will be reading and save you time.
The cover sheet of the protocol tells which RAC (Research Agenda Committee) developed the protocol and
will supervise it. Next is a listing of all the members of the protocol team, which should always include the
CCG representative(s). Then there is a list of the sub-studies of the main study.
The first section to review to get a basic understanding of the protocol is the
"Schema".
There, the basic protocol is outlined, including any randomizations, the number of subjects, the treatment
arms, criteria for treatment response and/or failure,
and secondary steps, etc. Spend some time reviewing
the schema so you have a good idea of the general
design of the study, and the target subjects-- i.e.
Now that you have a good idea about
treatment naïve, single PI failure, heavily pretreated,
what the study is all about, does the
etc.
Next review the primary and secondary objectives of
the study. Focus mainly on the primary objectives and
ask if this is a reasonable question to answer-- is it
important, is it very feasible, etc?
informed consent explain it in simple,
clear language?
____________________________________
Next, the most important areas to review are the inclusion and exclusion criteria.
It is here where very critical decisions are made concerning who can get into the study and who cannot. Ask if
the criteria unreasonably exclude certain people-- i.e. those between 13 and 18 years old, people with only
minor liver function abnormalities, etc. Unless there is a good justification for it, most studies are open to all
people, 13 years of age or older. The more people who are excluded from a study, the less generally
applicable will be the results of the study. For example, many studies used to exclude people with a liver
function test three times above normal, which excluded many people co-infected with Hepatitis C. Now, many
protocols only exclude people with liver function tests five times above normal.
Look at the table of evaluations, which will tell you how often someone has to come
in for exams and blood tests.
Are too many blood tests being done, are not enough viral loads being done, etc.? Also, ask whether the
person in the study will get the result of the blood test in "real time", i.e. will it be done immediately, or will the
test be "batched" (that is, run at a much later time), often with the result never being provided to the person in
the study.
Lastly, review the informed consent.
Now that you have a good idea about what the study is all about, does the informed consent explain it in
simple, clear language? Is there too much "medical-ese" in the consent? Are all the major risks and benefits
explained? Keep in mind that the informed consent is only a "template,” in that each individual institution's
Institutional Review Board (IRB) has their own requirements for the content and format for informed consents.
Also, quickly review the number of sub-studies, and ask if it is feasible to try to do so many studies under one
main study?
90
Additional CPCRA Resources
Glossary
Various glossaries that concentrate on HIV/AIDS and clinical trials are available to the community. Please
consider obtaining one or more of these glossaries for use by your community.
Some suggested sources are listed below:
CPCRA Investigator’s Handbook
CPCRA CAB Training Conference (glossary prepared by the CPCRA Statistical Center and distributed to
attendees)
CPCRA Investigator’s Handbook.
(This handbook is distributed to each CPCRA unit.) “The CPCRA Investigator’s Handbook documents
guidelines and procedures of the Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA)
related to the development and implementation of research studies in community-based settings.”
Areas is interest to the community include:
The Ethics section, which describes the history of ethical considerations and human subject
protection, including information on the 1972 Tuskegee syphilis study and the Belmont report.
The Publications & Presentations (P&P) Policy & Procedures section, which describes the
CPCRA P&P policy and procedures for submitting CPCRA-related abstracts and papers for P&P
Committee review.
CPCRA Data Collection Handbook.
(This handbook is distributed to each CPCRA unit.)
“The purpose of the CPCRA Data Collection Handbook is to document standard operating procedures of the
CPCRA related to the implementation and data collection of CPCRA studies.”
CPCRA Clinical Events Handbook.
(This handbook is distributed to each CPCRA unit.)
“The purpose of the CPCRA Clinical Events Handbook is to document policies of the Community Programs
for Clinical Programs on AIDS (CPCRA) related to the standardized reporting of “progression of HIV disease”
study endpoints for CPCRA experimental protocols.”
Community Programs for Clinical Research on AIDS
91
Populations
HIV/AIDS Clinical Trials & Women
HIV/AIDS Clinical Trials and Youth
HIV/AIDS Clinical Trials and People of Color
HIV/AIDS Clinical Trials and the Transgender
Community
92
Community Programs for Clinical Research on AIDS
93
HIV/AIDS Clinical Trials & Women
What We Know
Women make up one quarter of the population estimated to be living with HIV OR AIDS in the United
States, or approximately 200,000 to 225,000 women. 1
Women comprise a growing share of new AIDS cases each year. The proportion of AIDS cases among
women has more than tripled since 1986 from 7% to 23%2
Women of color are disproportionately impacted. Although African American woman represent only 13%
of the US female population, they account for almost two-thirds of new AIDS cases report among woman
in 1999. Similarly, Latinas accounted for 18% of new cases among women in 1999, but only 11% of the
US Population3
Women and Clinical Trials
Before 1993, women were often excluded from clinical trials. Researchers often cited concerns about
pregnancy not wanting to cause harm to a fetus. In 1993, however, the Food and Drug Administration
said woman could no longer be kept out of trials.
Women are still underrepresented in HIV/AIDS clinical trials. One analysis of 49 antiretroviral therapy
trials conducted between 1990 and 2000 showed an average of 12.25% of women in trials.4
Eligibility criteria may make it more difficult for woman to enter into clinical trials. The Women’s
Independent Health Study is currently the largest database of women with HIV in the United States, with
over 2,600 HIV positive and HIV negative women. Over 80% of the WIHS trial participants, however,
would be ineligible to participate in a typical AACTG trial due to illness, concomitant medications, and
psychiatric conditions.5
Gender Differences with HIV and AIDS
Because there has not been as much research, there is a lot we don’t know about women and HIV.
Some areas that are of particular interest to woman include: hormone levels, lypodystrophy,
gynecological care, and bone loss. For more information, an excellent brochure ‘Treatment Issues for
Women’ is available from the AIDS Community Research Initiative (www.acria.org)
Some Facts about Pregnancy and Clinical Trials
In many studies, women must agree to use birth control if they have sex with men. Pregnant or nursing
women usually can’t join a trial of an untested drug because it is not known if the drug might harm the
baby.
Some women think they must have an abortion if they become pregnant while in a study; this is not true.
1
Centers for Disease Control and Prevention, Division of HIV/AIDS Prevention, July 2000; Centers for Disease Control
and Prevention, HIV/AIDS Surveillance Report, Year-End Edition, Vol. 11, No. 2, 1999
2 Centers for Disease Control and Prevention, HIV/AIDS Surveillance Report, Year-End Editions, 1986, 1999
3 Centers for Disease Control and Prevention, HIV/AIDS Surveillance Report, Year-End Edition, Vol 11, No 2, 1999;
Urban Institute estimates of the March 200 Current Population Survey, US Bureau of the Census for the Kaiser Family
Foundation.
4 MA Pardo, MT Ruiz, A Gimeno, L Navarro, A Garcia, MV Tarazona, MT AZNAR, Gender Bias in clinical trials of AIDS
Drugs, presented at the Fourteenth International AIDS Conference, July 2002.
5 R. Greenblatt, Natural History of HIV-1 Infection in Women - - Findings from the Women’s Interagency HIV Study,
presented at the 10th Conference on Retroviruses and Opporunistic Infections, Feb 2003.
94
Every clinical trial has requirements about who can join. If a woman meets these requirements, she can
join.
For more information on Women and HIV/AIDS
Woman Alive
1566 Burnside Ave, Los Angeles, CA 90019. (323) 965-1564
www.women-alive.org
Woman Alive is a national treatment-focused, non-profit organization by and for women living with
HIV/AIDS.
WORLD
414 13th Street, 2nd floor, Oakland CA 94612. (510) 986-0340
www.womenhiv.org
WORLD is a diverse community of women living with HIV/AIDS and their supporters
Babes Network
1001 Broadway, Suite 100, Seattle, WA 98122. (206) 720-5566 ext. 12
www.babesnetwork.org
Babes Network is a sisterhood of women facing HIV together. Babes Network produces a monthly
newsletter available online or by mail.
Community Programs for Clinical Research on AIDS
95
HIV/AIDS Clinical Trials and Youth
What We Know
One-quarter of all new HIV infections in the U.S. are estimated to occur in young people under the age of
21.6
Among males ages 13 to 19, 41 percent of AIDS cases and 52 percent of HIV cases reported to the
Centers for Disease Control and Prevention (CDC) in 1997 were among YMSM (Young Men who have
Sex with Men) and YMSM injecting drug users.7
The percentage of adolescent AIDS cases among female teens in the U.S. has risen from 14 percent in
1987 to 49 percent of all adolescent cases reported in 1997. 8
Through 1997, African American and Latina teens accounted for 82 percent of the cumulative AIDS cases
among young women ages 13 to 19 in the U.S. 6
HIV infection is the leading cause of death among all people in the U.S. ages 25 to 44 and the sixth
leading cause among all people ages 15 to 24. Among those ages 15 to 24, HIV infection is the seventh
leading cause of death among white males and females, sixth among Latino males and females, fifth
among African American males, and third among African American females. 9
HIV/AIDS seriously affects adolescents throughout the world. One-third of all currently infected individuals
are youth, ages 15 to 24, and half of all new infections occur in youth the same age.1 More than five
young people acquire HIV infection every minute; over 7,000, each day; and more than 2.6 million each
year.10
For more information on Young People and HIV/AIDS
Advocates for Youth
1025 Vermont Avenue NW, Suite 200, Washington DC 20005. (202) 347 5700
www.advocatesforyouth.org
Advocates for Youth is dedicated to creating programs and advocating for policies that help young
people make informed and responsible decisions about their reproductive and sexual health.
Advocates provides information, training, and strategic assistance to youth-serving organizations,
policy makers, youth activists, and the media in the United States and the developing world.
AIDS Alliance for Children, Youth, and Families
1600 K Street, NW Suite 300, Washington, DC 20006. (202) 785-3564
www.aids-alliance.org
AIDS Alliance for Children, Youth and Families is the only national organization focused solely on the
needs of children, youth, and families living with, affected by, or at risk for HIV and AIDS.
6
The White House. The National AIDS Strategy. Washington, DC: Office of the President, 1997.
Centers for Disease Control & Prevention. U.S. HIV and AIDS cases reported through June 1997. HIV AIDS
Surveillance Report 1997; 9(1):1-39.
8 Centers for Disease Control & Prevention. HIV/AIDS Surveillance Report 1997; 9(2):1-39.
9 Anderson RN, Kochanek KD, Murphy SL. Report of final mortality statistics, 1995. Monthly Vital Statistics Report 1997;
45(11, Suppl 2):1-80.
10 UNAIDS. Listen, Learn, Live! World AIDS Campaign with Children and Young People: Facts and Figures. Geneva:
UNAIDS, 1999.
7
96
Community Programs for Clinical Research on AIDS
97
HIV/AIDS Clinical Trials and People of Color
What we know
Racial and ethnic minority groups in the United States continue to experience disparities in health care,
with many lower health outcomes than the white population. HIV AIDS is no exception to this trend.
Racial and ethnic minority groups in the U.S. make up 24% of the U.S. population yet they represent 67%
of new AIDS cases.11
Racial and ethnic minorities are also less likely to participate in HIV/AIDS Clinical Trials. A recent review
of trial participation showed that while African Americans make up 33% of those receiving treatment for
HIV/AIDS in the United States,
Receiving Care
In Trials
they comprise 23% of trial
African American
33%
23%
participants. The shame study
showed that while Hispanic
Hispanic
15%
11%
individuals make up 15% of those
White
49%
62%
receiving care, they make up only
11% of trial participants.12 Unfortunately, this study did not provide information on Asian and Pacific
Islanders.
Common Barriers to Trial Participation
Common barriers to trial participation for people of color include mistrust, economic factors, and
communications issues13.
Mistrust: Particularly in the case of African Americans, trial participation must be viewed in a historical
context. A review of past medical trials on African Americans reveals a number of brutal and unethical
trials culminating in the infamous Tuskegee Study14. One way trial sites address the issue of mistrust is
by actively engaging community representatives to serve on local community advisory boards.
Economic Issues: Trial participation requires time and commitment for trial participants which is not
always easy for those who have to miss work or arrange daycare for their children to participate in a trial.
Local sites address this issue by providing vouchers or travel reimbursement to trial participation.
Communication Issues: Many communities of color do not have all the information they need to make
sounds decisions about trial participation. Local sites can address this by community outreach and
patient education, making sure that the information is culturally appropriate and translated into different
languages as appropriate.
The Role of the CPCRA
The National Institutes of Health initiated the CPCRA network to in 1989 specifically to expand research
opportunities to communities of color, women, and others infected with HIV such as injection drug users.
CPCRA sites are located in many of the areas hardest hit by the AIDS epidemic in the United States.
The CPCRA continues to serve an important role in addressing disparities in AIDS Research.
Historically, people of color have comprised about 60% of CPCRA trial participants.
11
Centers for Disease Control and Prevention HIV/AIDS Surveillance Report, Year-end edition, Vol. 10, No 2, December
1998
12 New England Journal of Medicine 2002;346;18:1373-1382
13 Journal of the National Medical Association 1996;88:630-634
14 Journal of the National Medical Association 1996;88:630-634
98
For more information on AIDS Research and Communities of Color
National Minority AIDS Council
1931 13th Street, NW, Washington, DC 20009, (202) 483-6622
www.nmac.org
The National Minority AIDS Council (NMAC), is a national organization dedicated to developing
leadership within communities of color to address the challenges of HIV/AIDS.
Community Programs for Clinical Research on AIDS
99
HIV/AIDS Clinical Trials and the Transgender Community
The following section is adapted from the document: ”HIV/AIDS and Transgender Persons” by the
Department of Health and Human Services Leadership Campaign on AIDS, a program of the Office of
HIV/AIDS Policy.
Defining Transgender
Transgender individuals are those whose gender identity, expression, or behavior is not traditionally
associated with their birth sex. Some transgender individuals experience gender identity as incongruent with
their anatomical sex and may seek some degree of sex reassignment surgery, take hormones, or undergo
other cosmetic procedures. Others may pursue gender expression (masculine or feminine) through external
self-presentation and behavior. There are no reliable data on the number of transgender individuals in the
U.S. 15
What We Know
Although limited information is available about HIV/AIDS among transgender persons, HIV infection may be
high among this population. Here are some facts we do know:
15
A Centers for Disease Control and Prevention (CDC) review of an outbreak of tuberculosis among a
group of 26 transgender persons in Baltimore found that 62% were HIV infected. 16
Estimated HIV infection rates among specific transgender populations range from 14%-69%
according to several transgender HIV/AIDS needs assessments and sexual risk behavior studies.
The highest prevalence may be among male-to-female (MTF) transgender sex workers.17
Risky behaviors may be high among transgender persons, according to multiple transgender
HIV/AIDS needs assessments. Risk factors include: multiple sexual partners, irregular condom use,
unsafe injection practices (drugs and other substances including hormone and silicone injections); as
well as lack of transgender-appropriate education and prevention activities. 2
Although HIV/AIDS risk behaviors may be reportedly high among transgender persons, many
transgender persons self-identify as having low risk (according to various local HIV/AIDS needs
assessments of non-infected individuals and those not previously tested for HIV). 2
Transgender people face stigma and discrimination, which exacerbates their HIV risk. The stigma of
transgender status is associated with lower self-esteem, increased likelihood for substance abuse
and survival sex work in MTF's, and lessened likelihood of safer sex practices. Social marginalization
can result in the denial of education, employment and housing opportunities 1218
There are few transgender-sensitive HIV/AIDS prevention activities. In addition, access to care for
HIV disease may be limited due to low socio-economic status, lack of insurance, fear of one's
transgender status being revealed, provider lack of knowledge about caring for transgender persons,
and provider discrimination (e.g., exclusion of services such as drug rehabilitation programs, verbal
harassment and mistreatment). 123
In a study of persons diagnosed with AIDS between 1990-2000, and reported to CDC from 3-4 states,
transgender persons were more likely to be Black, Hispanic, or Asian Americans/Pacific Islanders,
compared to other persons with AIDS.
Definition by representatives of TLCA forum, January 2001
HIV-Related Turberculosis in a Transgender Network: Baltimore, Maryland, and New York City Area, 1998-2000."
MMWR. April 20, 2000.
17 Needs assesments on transgender persons and HIV/AIDS have been conducted in multiple sites. Data cited above
refer to studies in Atlanta, Boston, Chicago, Los Angeles, Minnesota, New York City, Philadelphia, San Francisco, San
Juan, and Washington, DC, with variable methods used to assess HIV status (i.e., self reported through confidential
surveys/interviews as well as baseline HIV tests).
18 Bockting, Walter. Transgender HIV Prevention: A Minnesota Response to a Global Health Concern, 1998. Nemoto T,
Luke D, Mamo L, Ching A, Patria J. HIV risk behaviors among male-to-female transgenders in comparison with
homosexual or bisexual males and heterosexual females. AIDS Care 1999; 11:297-312. John Snow Research and
Training Institute, Inc. "Access to Health Care for Transgendered Persons in Greater Boston." July 2000.
16
100
What We Can Do
Data. Improve data collection on transgender persons and HIV infection, particularly, separation of
transgender people from the men-who-have-sex-with-men (MSM) category in data reporting. This can
take place in partnerships between CDC, other researchers, and transgender communities.
HIV/AIDS Prevention. HIV/AIDS is not always a priority issue in the transgender community because
so many other basic survival issues outweigh it. In order to effectively reach this community,
HIV/AIDS prevention and care programs might be incorporated into a broader outreach effort, such
as job training or general access to health care.
Education of Decision-Makers. Conduct outreach to educate policymakers, health providers, and
others about transgender people and their concerns.
Providers. Build provider competency to address transgender health and its relationship to HIV/AIDS
transmission and prevention.
For more information on the Transgender Community and HIV/AIDS
TransHealth and Education Development Program
132 Boylston Street, 3rd Floor, Boston, MA 02116, 617-457-8150 ext. 342
http://www.jri.org
Established and sponsored by the Mass. Department of Public Health (DPH) since 1997, TransHealth
and Education Development Program educates healthcare and service providers to reach and care for
transgender (TG) clients and patients, to reduce the risk of HIV/AIDS and to promote positive
healthcare.
Gender Education & Advocacy
P.O. Box 65, Kensington, MD 20895, 301-949-3822, voice mailbox #8
http://www.gender.org
Gender Education and Advocacy (GEA) is a national organization focused on the needs, issues and
concerns of gender variant people in human society.
Community Programs for Clinical Research on AIDS
101
HIV/AIDS Clinical Trials & and Seniors
What We Know
According to the CDC, Individuals over the age of 50 now account for over 11% of AIDS Cases in the
United States. Some estimate that between 11% and 15% of U.S. AIDS cases occur in people over
the age of 50.19 AIDS cases among individuals over the age of 50 have increased 22% since 1991.
Up to 1999, 9.5% of all women diagnosed with AIDS were over the age of 50. 20
More than half of older Americans living with HIV are either African-American or from Hispanic/Latino
descent. 21
Seniors and HIV/AIDS
Later Diagnosis: Seniors often are dealing with multiple health issues. This may make it more
difficult for a doctor to distinguish between symptoms of HIV/AIDS and other medical decisions,
delaying an HIV/AIDS diagnosis. In addition, some medical providers may be less likely to associate
HIV/AIDS with older populations. Both of these factors may contribute to the fact that older persons
are more likely to be diagnosed at a late stage of infection.
Immune Response: Regardless of HIV status, our immune system naturally weakens as we get
older. This provides an added challenge for HIV positive seniors.
Seniors and HIV/AIDS Clinical Trials
19
Age Criteria for Trials: HIV/AIDS trials may exclude trial participants over a certain age or may set
limits on the number of participants over a certain age. For example, a recent AIDS Vaccine trial
excludes participants over the age of 60 and requires that no more than 10% of trial participants be
over the age of 50. This is due, in part, to the fact that these Seniors may have a weaker immune
response.
Health Criteria for Trials: HIV/AIDS trials may also specify that patients be in reasonably good
health at the time of study entry. This measurement of over-all health is often measured using the
‘Karnofsky Performance Score’. For example, the CPCRA SMART Trial does not have an upper age
limit for participation, but does require a Karnofsky score greater than or equal to 60 (indicating the
person does not require considerable assistance or frequent medical care).
Research on Seniors: Due in part to a lack of awareness of HIV/AIDS among Seniors, there is little
research that specifically addresses this population both in treatment research and prevention
research.
The CDC numbers are based on data acquired between 1991 and 1996. See MMWR, January 23, 1998, 47(02);21-27.
Organizations such as AIDS Action and the National Association of HIV over Fifty estimate the current number to be
between 11% and 15%.
20 AIDS Action, ‘Older Americans and HIV’, Policy Facts, June 2001
21 AIDS Action, ‘Older Americans and HIV’, Policy Facts, June 2001
102
For more information on Seniors and HIV/AIDS
National Association of HIV over Fifty
Jim Campbell, 23 Miner Street, Boston, MA 02215-3318, 617.233.7107
http://www.hivoverfifty.org
The National Association of HIV over Fifty works to promote the availability of a full range of
educational, prevention, service and health care programs for persons over age fifty affected by HIV.
Lesbian and Gay Aging Issues Network, American Society on Aging
833 Market St., Suite 511, San Francisco, CA 94103
http://www.asaging.org/networks/lgain
The Lesbian and Gay Aging Issues Network (LGAIN) works to raise awareness about the concerns of
lesbian, gay, bisexual and transgender (LGBT) elders and about the unique barriers they encounter in
gaining access to housing, healthcare, long-term care and other needed services. LGAIN has an online
links directory of information about HIV/AIDS and Seniors.
Community Programs for Clinical Research on AIDS
103
Historical Perspectives
History of Medical Research
History of Clinical Trials
History of CABS
Highlights in the History of Informed Patient
Consent
104
Community Programs for Clinical Research on AIDS
105
History of Medical Research
C. Lynn Besch, M.D., Principal Investigator, Louisiana Community AIDS Research.
In early societies, before man decided to group into cities, there were no physicians. Everyone fended for
themselves and learned by trial and error (i.e., eating a root or washing the wound in water, etc.). Then, when
societies developed, cities evolved, things were developed for the community good, (marketplaces, armies).
There was no medicine, but there was religion. Word of mouth suggested treatments. There was voluntary
exchange of information. Once societies grew to include rulers, Western medicine began. Greeks
established schools (called schools of philosophy) for men to learn to read and to take care of their bodies.
Nutrition was important. Medicine was relegated to the school of speculative thought. For a long time, as
medicine evolved, they were searching (trial and error) for answers; it was not really considered research yet.
Hippocrates took the learning of medicine out of the school of philosophy and created a medical school in
order to get some utility out of the knowledge of setting bones, etc. He described many things, including how
to know if the patient was compliant. At the time, many thought that health, and especially disease, came
from supernatural causes. There were many good observers at this time. They saw that there were different
diseases in different geographical areas, different diseases at different times of the year and in different
climates. Treatment was very generic.
The history of medical research cannot be explored without looking at the history of medicine. And the history
of medicine is out of context without looking at politics, finances, the way people were moving, and religious
thinking of the day. One of the next major figures in medical history was Claudius Galen, an anatomist. He
was considered to be an excellent clinician. He could cure ankle injuries, removed a breast tumor from a
woman, and actually became the personal physician of Marcus Aurelius. But Galen’s first love was anatomy.
He described muscles, internal organs, etc. Even though this was really information for information’s sake,
the information was passed down. After Galen, for about the next 1,000 years during the Middle Ages, there
was no advance in medicine.
Coming out of the Dark Ages, in the 1500’s, there were advances in several areas of science. Mathematics
improved, people learned how to grind lenses to make magnifying glasses, then a microscope. Much more
observation, in a detailed way, was possible. There were some experimental and quantitative methods being
developed not for medicine, but for war. Those who had wealth had power and they funded research, most of
it in warfare.
William Harvey, who discovered that blood flows in veins, stands out during this period in time. Before this
time, people thought that blood was packed in the body. People thought that the heart heated the blood
because most of the time people had raised temperatures when they bled. Harvey did a lot of work to figure
out circulation and he stands out as a champion in advancing medicine. By this time, physicians stood out
from priests and there was a trend to move away from religion influencing science to a more secular
environment. States and state governments were being formed.
The 1600’s showed great advances in physiology (how the body works). Large cities were being formed:
Paris, Amsterdam, Berlin, Milan, Florence. Commercial powers moved to northern Europe and so did the
science. Physicians found paying patients. Fee for service began during the Renaissance and has
continued.
The 1700’s showed great technological advances due to the industrial revolution (electricity, machines,
motors, and a lot of science). One of the most famous early medical studies concerned treatment for scurvy.
British ships went out for many months and had so much food and ale that the sailors got scurvy (a disease
due to lack of Vitamin C). Someone told them that if you ate limes you didn’t get scurvy. One captain divided
his ship and one-half of the sailors got limes and the other one-half did not. The people who ate limes did not
get scurvy. From then on the British took limes on their ships and were called “limeys.”
Edward Jenner discovered the small pox vaccine. Small pox was the scourge of Europe. Only farmers with
cattle were immune to small pox because the cattle had a related illness called cow pox. It was noted first
that the milkmaids got cow pox in a very mild form and then the farmers took the pox from cow lesions and
put it on scratches in their families’ skin. Farmer’s families were spared from getting small pox. Dr. Jenner
saw this, started working on a vaccine and tried it on this family first, then friends, and it worked. They were
all spared. He took this to the scientific community and was laughed out of the room. He went home,
106
continued vaccinating for 7 years, built up a very large case series, and went back to the scientific community
who could not refute his theory. He had large community support.
When medical questions outstripped the ability of the technology of the time, then people reverted to again
believing in supernatural explanation.
During the 1800’s, medical science and research took off. French and Germans were well supported in
research communities. There was no research support in America whose doctors went to train in Europe.
The French had enough teaching hospitals with large patient populations that they started asking questions.
For instance, does blood letting cure pneumonia? They conducted a trial and found out that it does not cure
pneumonia. They got a reputation for being good thinkers, for doing epidemiologic research, and for
repudiating things that had been done for years. There were more physical exams done, hence there was
more specific disease identification. Pierre Louis developed clinical statistics (to think in numerical order).
There were very few research physicians. The prevailing thought was that research should be done by
researchers, practice by clinicians. This was not financially possible, so some doctors did both research and
practice. A philosopher said, “Leaving research to practitioners would be as unfortunate as leaving
astronomy to sea captains.”
In the United States, there was some money for research but most was for public health. The Tulane School
of Public Health is the oldest in the United States. It was founded specifically to fight the yellow fever
epidemic. Through the study of yellow fever, it was proven that insects could carry disease, rather than
disease being spread through the air.
During the latter half of the 1800’s—Pharmacology was more prevalent and there were great advances in
microbiology, aspirin was produced, followed quickly by digitalis. Ignatz Semmelweis demonstrated the
importance of hand-washing in prevention of infections. He noticed that the infection and death rate after
women delivered babies in the hospital was very high for the medical students (who did autopsies before
going to see patients) compared with the midwives (who
were not allowed to do autopsies). He supposed that the
students were bringing the infection with them, so he had
them wash their hands after autopsy lab. The
During the 1900’s, maldistribution of
infection/death rate significantly decreased. However, he
care was acknowledged. The poor or
was basically laughed out of medical practice for such a
those who lived outside of the city did
radical idea.
Between 1895-1940, the federal government and wealthy
people began giving money for research.
not get much care.
____________________________________
During the 1900’s, maldistribution of care was
acknowledged. The poor or those who lived outside of the city did not get much care. People started to
organize medical research in the United States. Antibiotics were developed and they affected mortality.
Infectious diseases were better controlled. The first virus was isolated in 1935. There was more
sophisticated technology and statistics.
After WWI, chemists who worked for the government got together and proposed that they should get private
funding just to support a research institution devoted to medical research. The U.S. Senate heard and
proposed that it should be federally funded. Louisiana Senator Randall named the institution The National
Institutes of Health (NIH) and it started during the Depression. The NIH began as a one-room bacteriology
laboratory called the “Hygiene Laboratory” in 1887. It was basically funded to evaluate the health of
immigrants in New York at one point, then moved to Maryland.
Post WWII trials included randomization, placebo-controlled, and perhaps double-blinded design of studies.
Community Programs for Clinical Research on AIDS
107
Community-Based Research—History of Clinical Trials
Presented by Lawrence R. Deyton, M.S.P.H., M.D., Chief, HIV Research Branch, DAIDS/NIAID.
There has not been a very organized role for community participation in biomedical research before HIV. The
only organized way that the community voice was ever heard before HIV was through the Institutional Review
Board (IRB) process, which is really very new. When protection of human subjects became a concept that we
worried about, those laws and regulations were set up, those boards attached to hospitals and universities
were required to have some community participation. That was preacher, rabbi, and/or local government. It
was very new, very unique.
History in HIV research: Community-based research in AIDS was born purely out of the need expressed by
people with HIV disease and their clinicians. Between 1986-1988, when AIDS research began to take off and
the government was providing funding for AIDS research, activists, patients and clinicians made it clear that
there was not enough access to AIDS research and they wanted to participate. A shift happened and there
was catalytic activity going on in the formation of community-based research programs done by either
physicians caring for patients with AIDS and by patients themselves wanting to gain access to research. It
was then recognized that the epidemiology of this
epidemic was different than our early projections. It was
clear that this disease disproportionately affects
minorities, people who use drugs, and that the research
Community-based research in AIDS
infrastructure being set up by the government was not
was born purely out of the need
being placed in centers where those communities were
expressed by people with HIV
comfortable receiving care or going for research. These
disease and their clinicians.
factors led NIH to realize that it was time to seriously
consider a new kind of research program.
____________________________________
In late 1988, Jack Killen (then Deputy Director of DAIDS)
began meeting with community representatives,
advocacy groups, as well as people with HIV and AIDS, and the physicians and nurses caring for people with
HIV. The question was what should the government do? What types of programs are needed? We held
eight meetings in cities around the country; 1,200-1,500 people attended. There was clear communication
from those with AIDS and their clinicians regarding what was needed. So, in 1989, NIAID launched a pilot
program to establish community-based AIDS research—the CPCRA (Community Programs for Clinical
Research on AIDS).
After the first set of contracts was awarded, there was so much interest in community research that AmFAR
set up a similar program. Pharmaceutical companies began to look at community settings and doctors offices
in which to consider doing drug research and testing. Another important element of the CPCRA is that, for
the first time in NIH history, a Community Advisory Board (CAB) was required.
Early meetings of CPCRA community made it very clear that meetings should be open to the public and open
to the scrutiny of people with HIV disease. Prior to this, patients were not allowed to participate in any formal
way in discussions with researchers or to ask questions about research strategies. Many doctors and
scientists refused to participate. They thought that work would not get done. But since then, many have
learned the value of the community voice.
As the CPCRA grew, community participation was integrated into every aspect of what was done, including
representation on protocol teams, design and implementation of a trial, and the development of educational
materials. Interest groups were formed to provide input. Through these activities and a lot of hard work,
community representatives in these different settings have proven the importance of their contributions even
to those who were skeptical when it started.
Over the last year or two, the CPCRA has been restructured and community representatives were involved in
the process. In the final analysis, the testament of the worth of the community representatives and voice is
that the principal investigators decided that two voting members should be on the Steering Committee (all
other committees and units have only one voting member).
What has been learned in the last 4-5 years? The community is involved in all aspects that makes for better
research. Scientific questions are more relevant, designs of protocols are more sensitive to patients needs,
compliance is better, outcomes of research are more reliable. We have learned how to better provide
community input into the process. We are still learning and continuing to grow; it is a continual process.
108
I hope that we have learned that community participation is neither mere political correctness nor is it seen as
a universal requirement. Community participants need to prove and continue to prove the worth of this
participation. It should not be taken for granted. A seat at the table is not enough. The community must
contribute to the process and see themselves as good and patient teachers and good and patient students.
It is far too easy for CABs and members to lose focus and to try to do too much at once. They need to
remember that the reason the CPCRA exists is to do biomedical research; to start and finish that research.
The community needs to decide its top priority(ies) and build a long-term plan on how to get there. Repetition
is required for the message to be heard. Use your experience, your issues. Your questions are your fuel, but
do the work for those that will follow. Leave a strong legacy of the work that has been done.
The CPCRA has fundamentally changed the way
clinical research is done. The role of community
participation is one of the most important and
strongest legacies that must be left. Tell the
The CPCRA has fundamentally
research world about this. It must come from the
changed the way clinical research is
community. Tell how and why to do it. Produce
done. The role of community
teaching materials. Become more productive. This
includes writing and organizing; publishing your
participation is one of the most
perspective on important AIDS research issues. It
important and strongest legacies that
is important for the community being served to
must be left.
make their voice heard on the fundamentals of AIDS
research today. For example, what is the community
______________________________
perspective on the role and use of surrogate
______
markers in clinical research? The use of surrogate
markers with doctors in individual care? Comment on AIDS research in this country today. What is the role
of the NIH? What do you expect from the pharmaceutical industry? What are your thoughts on new ideas
such as large simple trials, MAPS strategy? Would you participate? You have a lot of experience in
recruitment, retention and issues in your community. You can educate the biomedical community.
Be disciplined, more focused, stronger, more productive than in the past. The road is getting rougher and
your voice is the clearest voice that needs to be heard.
Community Programs for Clinical Research on AIDS
109
History of CABs
Presented by Donald I. Abrams, M.D.
It’s an interesting story. In 1985, the mayor of San Francisco approached the chairman of the AIDS program
at San Francisco General Hospital (SFGH) and said, “You need to relate better to the physicians in the
community who are now caring for people with AIDS.” In response, a group of physicians caring for AIDS
patients in the community was formed. This group was initially called the County Community Consortium
(CCC) because it was a coming together of doctors at the county hospital—the AIDS center, and the
community physicians. Our goals were information exchange and informing community physicians about
what research we were doing. The CCC met monthly to exchange educational information and to talk about
our studies. After a few months the community doctors said they could do research in their practices too.
In 1986, the Community Consortium (CC—we dropped the word “county”) developed the first so called
“community-based clinical trial.” This trial was designed to discern if patients should be given preventive
treatments after their first episode of Pneumocystis pneumonia—one of the first trials of PCP prophylaxis
since little was known and every doctor seemed to be doing it differently.
After visiting the CC, this interesting idea intrigued New Yorkers like Mathilde Krim, Ph.D., President of
AmFAR and Joseph Sonnabend, M.D., one of the major doctors in the Village, so much that they attempted
to form a similar AIDS doctors’ consortium in New York. Because it was difficult to engage many NY doctors
who cared for AIDS patients to do clinical trials, they, instead, organized a new group called the Community
Research Initiative (CRI) under an organization called the PWA (people living with AIDS) Coalition.
The San Francisco group was comprised of all doctors. The New York group was a mixed group with a few
doctors, but mainly people living with HIV/AIDS. Historically, this was when Admiral Watkins and his AIDS
Commission were touring the country to learn about the disease. While in San Francisco, I explained the
concept of community-based clinical trials to the Commission. When they visited New York, the CRI put on a
very well-orchestrated presentation on community-based clinical trials and suddenly, as a result of their public
relations expertise, the CRI became nationally known.
Meanwhile, the CC, which is now 200 doctors caring for PWAs, kept meeting. In 1987-1988, when a growing
AIDS activist community in San Francisco advocated hard for more community-based clinical trials, they had
become aware of the New York group and wanted to have a CRI in San Francisco. By this time, the CC had
finished an aerosolized pentamidine study thatwas leading to a publication in the New England Journal of
Medicine and the FDA had approved inhaled pentamidine as a prophylaxis for PCP. Activists in San
Francisco, however, wanted to participate in the research process and formed the Community Research
Alliance (CRA), modeled after the CRI in New York. The CRA eventually merged with Project Inform. So,
ironically, the New York CRI model, which basically developed out of the San Francisco CC model, then
flipped back to California as the Community Research Alliance.
Because of increasing confusion as to just who was “community” in community-based clinical trials, the CC
established an organizational task force which developed a policy statement and redefined the “Community
Consortium” as a group of licensed health care providers in good standing. Then an Executive Board, a
Scientific Advisory Committee, and a Community Advisory Forum were all established in 1988 (the year
before the CPCRA was started).
The first community advisory board of the CC was comprised of adversarial activists; however, later other
more supportive members and some of my own patients were added. Finally, the San Francisco CAB
became a formal established structure in 1988. Soon, not only the CC, but the ACTG (AIDS Clinical Trials
Group) and CFAR (Center for AIDS Research) programs all decided to have Community Advisory Boards.
So we’re sort of proud that that’s how the first CAB, that we’re aware of, was set up. Now, the concept of
CAB is something we need to look at; because there are a limited number of people who are willing, years
later, to volunteer and dedicate time and energy to participate on these boards.
110
Highlights in the History of Informed Patient Consent
Throughout the twentieth century there has been a general evolution of mechanisms designed to afford
protections to the human subjects of scientific research. The independent visionary researchers of the
nineteenth century have been replaced with institutionalized medical researchers in the twentieth century. As
research has increased, so has the need to protect the subjects of research.
In 1900, Walter Reed’s experimental triumph in yellow fever research was accomplished with fully
informed research subjects. Consent statements written in both English and Spanish were signed by
both researchers and subjects, something Reed himself believed crucial to the integrity of his work.
The first efforts to form an international code of ethics to protect the subjects of research came as a result
of the abuses revealed at the 1946 Nuremburg trial of 23 Nazi medical professionals. Out of hundreds of
thousands of victims, only a handful survived to testify against their torturers. The defendants were
charged with offenses ranging from subjecting test subjects to extremes of altitude and temperature to
using them as human cultures to test vaccines for typhus and malaria. The “Nuremburg Code” accepted
and codified ethical standards that the 23 defendants had grossly violated, and thus became the first
internationally recognized code of medical research ethics. Its stated goal was not merely to “prevent
experimental abominations in the future but to increase the protection of the rights and welfare of human
subjects everywhere by clarifying the standards of integrity that constrain the pursuit of knowledge.” The
first principle of the Nuremburg Code stressed the importance of obtaining “informed consent” from
research subjects. The code also emphasized that human studies should not be random or unnecessary,
that animal studies should be undertaken before human studies, and that surveys of the natural histories
of disease should be undertaken before subjecting human subjects to laboratory-induced disease.
In 1953, the National Institutes of Health opened its Clinical Center as a research hospital and adopted a
policy that placed much of the responsibility for safeguarding human subjects of biomedical research with
principal investigators. Research involving normal human volunteers was to be formally reviewed by
panels of scientists.
In the early 1960’s, the drug thalidomide never received regulatory approval in the U.S., as a result of the
work of FDA drug reviewer Dr. Frances Kelsey. Nonetheless, thousands of U.S. doctors distributed
“samples” of the drug to patients in the U.S. without telling them that the drug was an experimental drug,
making them the unwitting subjects of human drug experimentation. As a result of the worldwide
thalidomide disaster, the U.S. Congress enacted what came to be known as the Kefauver-Harris
Amendments to the 1938 Food, Drug, and Cosmetic Act. This amendment was the first federal or state
law to require investigators to inform potential subjects of the experimental status of a new drug and
obtain informed consent. The 1962 amendments empowered the FDA to prohibit testing of a drug in
humans until animal studies could predict that the drug could be given safely in man.
In 1963 it was revealed that researchers from Sloan-Kettering, working with patients at the Jewish
Chronic Disease Hospital, had injected feeble and seriously ill patients with live cancer cells to study their
immune system responses. The patients were only told that “their resistance was being tested” and not
that they were being injected with cancer cells. A non-physician on the hospital board questioned the
propriety of the study and took the hospital to court to obtain access to the records. The resulting lawsuit
drew public attention and criticism to the physicians’ failure to respect the rights of patients.
In 1964, NIH Director James Shannon appointed a committee to review, study, and design mechanisms
to ensure that patients would be systematically and uniformly protected in all biomedical and behavioral
research funded by PHS.
1964 - The U.S. signed the Helsinki Declaration - adopted a series of guidelines from the World Medical
Association with 4 basic tenets:
1. Clinical research should be based on animal and laboratory experiments;
2. Clinical research should be conducted and supervised only by qualified medical workers;
3. Clinical research should be preceded by a careful assessment of risks and benefits to the patient;
and
Community Programs for Clinical Research on AIDS
111
4. Human beings should be “fully informed and must freely consent” to the research.
In June of 1966, noted Harvard Medical School researcher Dr. Henry K. Beecher published an article in
the New England Journal of Medicine raising ethical questions about studies conducted on human
subjects. Basing his work on published research papers, he cited serious breaches in the protection of
human subjects. In some cases, the controls were denied treatment, in others, surgical procedures were
attempted. Beecher concluded, “questionable ethical procedures are not common.”
July 1, 1966 - Dr. James Shannon’s work at NIH was codified in a policy statement issued by the Surgeon
General of the United States and based on a memorandum entitled “Investigations Involving Human
Subjects, Including Clinical Research: Requirements for Review to Ensure the Rights and Welfare of
Individuals.” “All research, grants, and awards in support of research, training, or demonstration projects
that involve research on human subjects require prior review.” Institutions that receive these grants must
provide “an independent prior review of the rights and welfare of the human subjects involved, the
appropriateness of the means to secure informed consent, and the risks and benefits involved in the
study.”
In August 1966, FDA regulations specified for the first time specifically how consent is supposed to be
obtained and what exceptions would be allowed. Written consent is required except in certain
circumstances including: unconscious patients, a child in an emergency without a parent available,
mentally incompetent patients without a representative, or patients suffering from an incurable disease,
the knowledge of which would be harmful to their welfare in the opinion of the doctor. In March, 1967, the
regulations were modified based on comments from the American Medical Association, the
Pharmaceutical Manufacturers Association, the National Academy of Sciences and others. Written
consent was still required in phase I and II trials, but in phase III trials, written consent would not be
mandatory in cases where “investigators are using the drug on patients essentially as it would be used if
approved for medical use.” Still the patient must be informed of all pertinent information. Phase III trials
still required patient informed consent but it could be oral, rather than written. If oral, however, it must be
recorded in writing. These regulations were finalized on June 20, 1967.
In 1972, public attention and outrage focused on the so-called “Tuskegee Experiment” -- a Public Health
Service study that had been conducted in Alabama on 300 black men with congenital syphilis. The study
had originally been designed in 1932 to study the untreated course of the disease in the absence of
effective treatments, but the study had continued unabated for forty years, during which time the
development of penicillin made the disease treatable. The men in the study were not told that they had
syphilis, merely that they had “bad blood,” they did not know that they were in any kind of a study, and
they were not offered treatment even after penicillin was available to treat their disease. The case was
heard by the Senate Health Subcommittee that concluded that human subjects needed more protection.
In 1974, Congress passed the National Research Act of 1974 (Title II, PL 93-348). This act required
codification of DHEW policy in regulations and imposed a moratorium on federally funded fetal research.
It also required the establishment of Institutional Review Boards to review all Health and Human Services
funded research and created the National Commission for the Protection of Human Subjects of
Biomedical and Behavioral Research.
1974 - Department of Health and Human Services established regulations for the Protection of Human
Subjects of Biomedical and Behavioral Research (45 C.F.R. 46). In accordance with Title II, it
established IRB review procedures. Subsequent regulations that year provided additional protection for
pregnant women and fetuses.
1974-1978 The National Commission for the Protection of Human Subjects of Biomedical and Behavioral
Research, a diverse committee, representing both science and society, issued detailed reports exploring
the ethical considerations inherent in human experimentation. The Committee’s work was widely
respected as it gave voice to growing concerns that in spite of the great progress made by researchers,
research subjects were still being abused. The committee issued reports and recommendations on fetal
research, on research involving prisoners, psychosurgery, children and the mentally infirm, on Institutional
Review Boards and informed consent. It also detailed problems at the frontier of biological research
including genetic research, mind-altering drugs, artificial hearts, behavior modification techniques and
drugs, and organ transplants all of which the committee deemed to pose significant new ethical problems
112
in addition to the age-old problems of safeguarding the poor, the disadvantaged, the institutionalized, children,
prisoners, the unborn, and the mentally disabled from assuming disproportionate risks as research subjects.
The Committee’s most important statement, known as the Belmont Report, remains the touchstone for current
researchers as they seek to evaluate and implement research protocols involving human subjects. It
discussed criteria for distinguishing research from the practice of medicine and discussed ethical principles
presumed to govern all research involving human subjects:
1) Respect (for persons) - recognizes the autonomy
of humans and mandates a well-defined set of
principles governing informed consent;
2) Beneficence - research must be shown to be
beneficial and must reflect the Hippocratic dictum to
“do no harm”; and
3) Justice - those who receive the benefits of
research must be balanced against those who take
the risks of research.
The Committee’s most important
statement, known as the Belmont
Report, remains the touchstone for
current researchers as they seek to
evaluate and implement research
protocols involving human subjects.
____________________________________
1978 - Revised DHEW regulations governing protections for
pregnant women, fetuses, in vitro fertilization (subpart B of 45 C. F. R. 46), and prisoners (subpart C) were
published.
1980-1983 - President’s Commission for the Study of Ethical Problems in Medicine and Biomedical and
Behavioral Research - This Commission was charged with, among other responsibilities, reviewing federal
policies governing human subjects research and determining how well those policies were being carried out.
It recommended that all federal agencies adopt the DHHS (formerly DHEW) regulations for the protection of
human subjects.
1981 - DHHS, responding to the recommendations of the National Commission, published a revision of 45
C.F.R. 46, specifying more carefully IRB requirements and responsibilities and the procedures IRB’s were
required to follow.
27 July 1981 - FDA regulations at 21 C.F.R. 50 governing informed consent procedures and at 21 C.F.R. 56
governing IRB’s were revised, based on the authority of the Belmont Report, to correspond to DHHS
regulations to the extent allowed under the Federal Food, Drug, and Cosmetic Act and its amendments.
1982 - President’s Science Advisor, Office of Science and Technology Policy (OSTP), appointed an
interagency committee to develop a common federal policy for the protection of human research subjects.
1983 - DHHS regulation issued governing protections afforded children in research (subpart D of 45 C.F.R.
46).
1986 - Proposed common federal policy for the protection of human research subjects was published.
June 18, 1991 - “The Common Rule” was codified in the regulations of fifteen federal agencies and adopted
by the CIA under executive order. The Common rule is identical to the basic DHHS policy for the protection
of research subjects (45 C.F.R. 46, subpart A). Other sections of the DHHS regulation provide additional
protections for pregnant women, fetuses, in vitro fertilization (subpart B), prisoners (subpart C), and children
(subpart D), and these have been adopted as administrative guidelines by several agencies. The FDA made
conforming changes in its informed consent and IRB regulations. The Common Rule contains provisions
mandating informed consent.
Community Programs for Clinical Research on AIDS
113
January 15, 1994 - President Clinton created the Advisory Committee on Human Radiation Experiments
in response to a growing number of reports describing possibly unethical conduct of the U.S. government
and institutions funded by the government, in the use of, or exposure to, ionizing radiation in human
beings at the height of the Cold War. The Committee was charged with uncovering the history of human
radiation experiments and intentional environmental releases of radiation; identifying the ethical and
scientific standards for evaluating these events; and making recommendations ensuring that whatever
wrongdoing may have occurred in the past could not be repeated. The Committee’s Final Report, issued
in October 1995, concluded that people were used as research subjects without their consent during the
Cold War era and they were wronged even if they were not harmed. In examining the current status of
experimental research, the Committee concluded that the nation still had problems and required improved
means to “better ensure that those who conduct research involving human subjects act in a manner
consistent with the interests and rights of those who may be put at risk and consistent with the highest
ethical standards of the practice of medicine and the conduct of science.” In cases in which research
activities must occur in secret, the Committee recommended that “special care” be taken to prevent
abuses in human subject research.
FDA History Office
Suzanne White Junod, Ph.D.
114
Tools
Community Programs for Clinical Research on AIDS
Common Abbreviations and Acronyms
Medical Abbreviations
Standard Format for CPCRA Research Ideas
Denver CAB Research Training
115
Common Abbreviations and Acronyms
CPCRA Units
ARAC
ARCA
CC
CHI
DEN
FIGHT
HATG
HFH
LaCARP
NJCRI
PIRNM
RAC
REG
SNJACT
WRAP
WSU
AIDS Research Alliance - Chicago
AIDS Research Consortium of Atlanta
Community Consortium
AIDS Research Alliance - Chicago
Denver Community Program for Clinical Research on AIDS
Philadelphia FIGHT
Harlem AIDS Treatment Group
Henry Ford Hospital
Louisiana Community AIDS Research Program
North Jersey Community Research Program
Partners in Research New Mexico
Richmond AIDS Consortium
The Research & Education Group
Southern New Jersey AIDS Clinical Trials
Washington Regional AIDS Program
Wayne State University
CPCRA Standing Committees & Advocacy Groups
CCG
P&P
SAB
SPC
UOC
UPC
Community Constituency Group
Publications & Presentations Committee
Science Advisory Board
Science Planning Committee
Unit Operations Committee
Unit Performance Committee
Organizations
AACTG
ACDDC
ACT-UP
ACTIS
AmFAR
ATTC
BMRC
CDC
CPCRA
CRMB
CSMG
CSRC
CTN
DAIDS
DHHS
DOD
DSMB
FDA
GMHC
ICAAC
IDSA
IRP
NCI
NIAID
NICHD
Adult AIDS Clinical Trials Group
AIDS Clinical Drug Development Committee
AIDS Coalition to Unleash Power
AIDS Clinical Trials Information Service
American Foundation for AIDS Research
AIDS Therapeutic Society
British Medical Research Council
Centers for Disease Control and Prevention
The Terry Beirn Community Programs for Clinical Research on AIDS
Clinical Research Monitoring Branch of DAIDS
Clinical Site Monitoring Group
Clinical Science Review Committee (DAIDS)
Canadian HIV Trials Network
Division of AIDS
Department of Health and Human Services
Department of Defense
Data and Safety Monitoring Board
Food and Drug Administration
Gay Men’s Health Crisis
Interscience Conference on Antimicrobial Agents and Chemotherapy
Infectious Diseases Society of America
Intramural Research Program (NIH Clinical Center)
National Cancer Institutes (NIH)
National Institute of Allergy and Infectious Diseases
National Institute of Child Health and Human Development
116
NIH
OAR
OPRR
PACTG
PAHO
PAB
RAB
ROC
WHO
National Institutes of Health
Office of AIDS Research (NIH)
Office of Protection from Research Risks
Pediatric AIDS Clinical Trials Group
Pan American Health Organization
Pharmaceutical Affairs Branch (DAIDS)
Regulatory Affairs Branch (DAIDS)
Regulatory Operations Center
World Health Organization
Other Acronyms
ADL
ADR
AE
AER
AIDS
CAB
CE
CFR
CRF
CS
CTA
CTAAG
CTS
FOI
GCP
GLP
HIV
IND
IoR
IRB
LFU
LOU
MAPS
MIS
MM
MO
MOOP
MOPPS
MOU
NDA
NWCS
PC
PI
PID
PLWA
PSR
PWA
QA
QC
QOL
RFA
RFP
SAE
SID
SOCA
SOP
Activities of Daily Living
Adverse Drug Reaction
Adverse Event or Experience
Adverse Experience Report
Acquired Immunodeficiency Syndrome
Community Advisory Board
Clinical Event
Code of Federal Regulations
Case Report Form
Concept Sheet
Clinical Trials Agreement
Clinical Trials At A Glance Report
Clinical Trials Specialist
Freedom of Information Act
Good Clinical Practice
Good Laboratory Practice
Human Immunodeficiency Virus
Investigational New Drug
Investigator of Record
Institutional Review Board
Lost to Followup
Letter of Understanding
Master Antiretroviral Protocol Strategy
Management Information System
Medical Monitor
Medical Officer
Manual of Operations
Multiple Opportunistic Pathogens Prophylaxis
Memo of Understanding
New Drug Application
New Work Concept Sheet
Project Coordinator
Principal Investigator
Patient Identification Number
Person Living With AIDS
Protocol Status Report
Person With AIDS
Quality Assurance
Quality Control
Quality of Life
Request for Applications
Request for Proposals
Serious Adverse Event/Experience
Study Identification Number
Studies for the Ocular Complications of AIDS
Standard Operating Procedure
Community Programs for Clinical Research on AIDS
117
Medical Abbreviations
A
a
Ab
ABG
abs feb
a.c.
AD
ADC
ad hib
ad lib
adst feb
ad us. ext
before
Antibody
arterial blood gas
when fever is absent
before meals
right ear
AIDS Dementia Complex
to be administered
as desired
when fever is present
for external use
Ag
agit. ante us.
ALT
alt hor
A.M.A.
AR
ARC
AST
a.s.
AU
antigen
shake before using
Alanine aminotransferase: SGPT
every other hour
against medical advice
Anti-retroviral
AIDS Related Complex
Aspartate aminotransferase: SGOT
left ear
both ears
blood
barium
blood brain barrier
branched chain DNA
bismuth (i.e., pepto bismol)
bioelectrical impedance analysis
drink
twice a day
BIW
BMR
BP
BRP
BSA
BUN
Bx
Twice a week
basal metabolic rate
blood pressure
bathroom privileges
body surface area
blood urea nitrogen
biopsy
calorie; complicance; concentration
with
approximately
cardioarterial
cancer; carcinoma; cardiac arrest
computerized axial tomography
complete blood cell count
cubic centimer
chief complaint
critical care unit; coronary care unit
Helper T-cells
Suppressor T-cells
food
continuous intravenous infusion
chronic lyphocytic leukemia
centimeter
Certified Medical Assistant
CMI
CMT
CMV
cell mediatedimmunity
Certified Medical Transcriptionist
cytomegalovirus; controlled
mechanical ventilation
central nervous system
coenzyme A
center of gravity
let the medicinebe continued
cardiopulmonary resuscitation
conditioned reflex
chronic respiratory disease
cerebrospinal fluid
computed tomography
cardiovascular accident (stroke)
cardiovascular disease
central venous pressure
chest x-ray
right (as opposed to left)
give
Zalcitabine
swallow
give
Stavudine
every other day
dil
one-half
desquamative pneumonia
dispense
dL
DLT
dMAC
B
b
Ba
BBB
bDNA
Bi
BIA
bib./BIB.
b.i.d./BID
C
C
_c
ca
c-a
CA
CAT
CBC
c.c.
C.C.
CCU
CD4
CD8
CIB
CIV
CLL
cm
CMA
CNS
CoA
COG
cont. rem
CPR
CR
CRD
CSF
CT
CVA
CVD
CVP
CXR
D
D
d
DDC
Deglut
det
D4T
dieb alt
dil
dim.
DIP
disp
DNR
DOT
dr
DTH
dur dol
D/W
Dx
deciliter
dose-limiting toxicity
disseminated Mycobacterium avium
Complex
do not resuscitate
directly observed therapy
dram
delayed type hypersensitivity
while the pain lasts
dextrose in water
diagnosis
118
E
EB/EBV
ECG/EKG
ED
EEG
EFV
Epstein-Barr virus
electrocardiogram
effective dose
electroencephalogram
Efavirenz
EIA
ELISA
emp
enzyme immunoassay (test)
enzyme-linked immunoadsorbent
assay (test)
as directed
fever
fever of unknown origin
Fx
g
fracture
gram
general anesthesia
gargle
genotypic antiretroviral resistance
testing
gall bladder
gonorrhea
growth hormone
gastrointestinal
gm
gn
grad
GSH
gtt
GTT
GU
GYN
grams
grains
by degrees, gradually
reduced glutathione
drops
glucose tolerance test
genitourinary
gynecology
hour
hepatitis-associated antigen
highly active antiretroviral therapy
hepatitis-associated virus
hemoglobin
hepatitis B virus
hematocrit
HCV
hd/h.s.
HMO
HSV
Hx
HZV
hepatitis C virus
at bedtime
health maintenance organization
herpes simplex virus
history
Herpes ZosterVirus
F
febris
FUO
G
GA
garg
GART
GB
GC
GH
GI
H
h
HAA
HAART
HAV
Hb/Hgb
HBV
HCT
I
IADL
ICU
IDU
IDV
IFN
Ig
IH
IL
IL-2
instrumental activities of daily living
intensive care unit
injecting drug user
Indinavir
interferon
Immunoglobulin
infectious hepatitis
interleukin
interleukin-2
IM
IMB
int cib
IPV
ITP
IU
IUPM
IV
intramuscular
information-motivation-behavioral skills
between meals
inactivated polio vaccine
idiopathic thrombocytopenia purpura
International Unit
infectious units per million cells
intravenous
kilo
potassium
kilogram
KPS
KS
Karnofsky Performance Scale
Kaposi’s Sarcoma
liter
left
lethal dose
liver function tests
liquid
LMP
LP
LPN
LVN
last menstrual period
lumbar puncture
Licensed Practical Nurse
Licensed Visiting Nurse
K
k
K
kg
L
l
L
LD
LFT
liq
119
M
µ
µµ
M
MAC
MCH
MCV
MDI
MDR
MDRTB
m et n
mg
MI
micromicrometer
mix
Mycobacterium avium Complex
mean cell hemoglobin
mean cell volume
metered dose inhaler
multidrug resistant
multidrug Resistant Tuberculosis
morning and night
milligram
myuocardialinfarction
mL
mm
mor dict
mor sol
MOS
MPD
mrd
MRI
mRNA
MTD
MW
milliliter
millimeter
in the manner stated
as usual, customary
medical outcomes study
maximum permissible dose
minimal reacting dose
magnetic resonance imaging
messenger RNA
maximum tolerated dose
molecular weight
N
N
NF
NFV
NK
NMR
NNRTI
normal
National Formulary
Nelfinavir
natural killer cells
nuclear magnetic resonance imaging
Non-Nucleoside Analogue Reverse
Transcriptase Inhibitor
Nucleoside Analogue Reverse
Transcriptase Inhibitor
npo
nothing by mouth
noc maneq at night and in the morning
NSAID
nonsteroidal anti-inflammatory drug
NRTI
O
OB
od/oid
OD
ODB
OI
an eye; oxygen
obstetrics
once a day
Doctor of Optometry; right eye; overdose
observational data base
opportunistic infections
omn hor
OOB
OS
OT
OTC
OU
at every hour
out of bed
left eye
occupational therapy
over the counter
both eyes
Physician’s Assistant
equal parts (amounts)
In divided doses
peripheral blood mononuclear cells
after a meal
Pneumocystis carinii pneumonia
polymerase chain reaction
physical examination
pulmonary function test
persistent generalized lymphadenopathy
Doctor of Philosophy
protease inhibitor
pelvic inflammatory disease
PK
PML
PR
prn
PRTD
pt
PT
Px
pharmacokinetics
progressive multifocal
leukoencephalopathy
Per Os (taken orally)
parts per million
pain, pallor, pulse, loss, parathesia,
paralysis
progressive resistance (exercise)
as needed
proximal renal tubular dysfunction
patient
physical therapy
prognosis
volume of blood flow
quaque die (every day, each day)
every hour
qid
ql
qs
four times a day
as much as desired
quantity sufficient; as much as is enough
P
PA
part. aeq.
part. vic.
PBMCs
pc
PCP
PCR
PE
PFT
PGL
PhD
PI
PID
PO
ppm
PPPPP
Q
Q
qd
qh
120
R
R
rbc
RBF
rIL-2
take; respiration
red blood cell count
renal blood flow
recombinant interleukin-2
RNA
RT
RTV
Rx
ribonucleic acid
reverse transcriptase
Ritonavir
the first word on a prescription; therapy
subcutaneous
standard deviation
serum glutamic-oxaloacetic
transaminase (a liver enzyme)
serum glutamic-pyruvic transaminase (a
liver enzyme)
serum hepatitis
write;inscribe,often used in the writing of
prescriptions
SOB
sol
sos
sp gr
SQ
SQV
stat
STD
Sx
short of breath
solution
repeat if necessary
specific gravity
subcutaneous
Saquinavir
immediately
sexually transmitted disease
symptom
temperature
tuberculosis
total bloodvolume
transientischemic attack
three times aday
tincture
Bactrim (trimethoprim sulfamethoxazole)
TORCH
TPR
3TC
Tx
toxoplasmosis, other infections, rubella,
cytomegalovirus, and herpes simplex
titer
tempreature,pulse,respiration
Lamivudine
treatment
unit
upper limit of normal
upper repiratory infection
USP
ut dict
UTI
United States Phamacopeia
as directed
urinary tract infection
venous blood
visceral fat: subcutaneous fat
visceral fat: total fat
VD
VQA
VS
S
sc/SC
Sd
SGOT
SGPT
SH
sig
T
T
Tb
TBV
TIA
t.i.d.
tinct
TMP/SMX
U
U
ULN
URI
V
v
VAT:SAT
VAT:TAT
W
WBC
white blood cell count
Y
YO
year old
Z
ZDV
Zidovudine
Community Programs for Clinical Research on AIDS
venereal disease
virology quality assurance
vital signs
121
Format for Submitting CPCRA Research Ideas
CPCRA Research Idea
Submitted by: [author(s) name(s)]
CPCRA Unit: [lead author’s unit name & location]
TITLE
The title should describe some characteristics of the proposed study such as the study population,
treatment(s), and basic trial design (allocation, blinding, controls).
(Note: A short title will be assigned by the CPCRA Operations Center.)
PURPOSE
A concise statement of purpose should be included to specify the intended focus and expected yield of
the proposed investigation.
BACKGROUND/RATIONALE
Sufficient information should be summarized to provide primary care physician researchers with an
understanding of (a) the relevance of the clinical questions posed by the investigation, (b) the current
state of efficacy and safety data in support of the proposed study regimens, and © the applicability of the
proposed study to CPCRA and NIAID strategic research goals.
OBJECTIVES
Objectives should be specific and measurable; both primary and secondary objectives should be stated.
METHODOLOGY
Basic Study Design
Sample Size and Statistical Considerations
Rough estimates are acceptable; include if available.
Basic Eligibility Criteria
TREATMENT PLAN
Procedures
Describe only any unusual details related to baseline screening, study enrollment, concomitant meds,
monitoring and followup, toxicity grading, etc. Unless specified, it will be assumed that scheduled
data collection will occur only at 4-month intervals.
Study Medication
State the dose, method, and frequency of administration (if known) for all study agents.
EVALUATION
Outcome Measures
Identify the evaluations to be used in measuring patient outcomes (e.g., clinical, behavioral,
psychological, immunological, or virological response parameters).
Endpoints
Identify the primary and secondary endpoints that will be used in statistical analysis of the data (if known).
LOGISTICS
Provide estimates of anticipated enrollment duration and total study duration. Note any unusual or
exceptional expenses likely to be associated with performance of the proposed study.
122
If outside collaboration with other trial sites is desirable, please provide justification in terms of the
logistics of enrolling the estimated sample size, and/or compelling clinical or public health reasons.
REFERENCES
A concise list of salient references should be included.
Community Programs for Clinical Research on AIDS
123
How to Review a Research Concept/Protocol
1. What is the research question?
Look at Purpose and Objectives sections. Is this question important?
Is this a high priority issue in the community?
2. What is the primary endpoint?
Is it a surrogate marker (like viral load or CD4+ cell count) or is it a clinical endpoint (such as disease
progression, death, etc.)?
Is there a good reason not to use a clinical endpoint in this study?
3. What is the control group?
Is it a placebo (no treatment) or is it a “standard of care” control?
What is the “worst case” for someone getting randomized into one of the arms of the trial?
4. How about switchover?
What are the criteria for changing from one arm of the study to another? Are there any?
5. Inclusion/exclusion criteria: do they make sense?
Will they exclude people from the trial unnecessarily?
6. Clinic visits: how often do people have to come in for visits?
Are visits to frequent?
Are they too long (look at what tests have to happen each visit)?
7. Other logistics: What do participants have to do?
Pills to take?
Injections?
Diaries or other record keeping?
Is this reasonable?
8. Participation: are there any aspects of the study design that will make participation difficult or unlikely in
your community?
How could these be changed?
124
Sample Proposed Protocol Evaluation
NJCRI
393 Central Avenue, Suite 301
Newark, NJ 07103
(201) 483-3444
Fax: (201) 485-7080
Proposed Protocol Evaluation
Protocol:
Please review the enclosed _____________________________________concept. Your input is very
important in helping decide whether this proposed protocol will move forward to implementation and whether
NJCRI will participate. Please return your comments no later than _______.
Do you think the community will be interested in this protocol?
Anything you particularly like about the protocol?
Anything you particularly dislike and would want to see changed:
What about the entry criteria?
What about the participant’s responsibilities? Number of follow-up visits? Number of tests required? The
study drug(s)?
Should NJCRI participate in this protocol if it is implemented: If you answered “no,” what changes might
change your answer to “yes?”
Other comments?
Community Programs for Clinical Research on AIDS
125
AIDS Research Alliance Chicago, Community Advisory Board Concepts/Protocols Review Guide
PREFACE:
- explains what the Terry Beirn Community Programs for Clinical Research on AIDS
(CPCRA) is and its purpose.
SYNOPSIS:
- summary of the protocol
INTRODUCTION:
Background and Rationale:
what kind of study was done in past
what we know about the drug
why we think the drug will do what we expect
***Look for community interest,
non-medical provider interest,
importance to community,
attractive to a large portion of community, and
accessible to population
Look for positive and negative aspects of the drug and unanswered questions.
Are you convinced that the drug will do what we expect?
Do you feel comfortable relying on results of studies in past? (Look at study size, length, methods, etc.)
Study Agents:
- explains what the drug is and what it does
***Look for the drug toxicity/side effects as well as positive aspects.
How is its bioavailability?
[Bioavalability: the rate and extent to which a substance is absorbed and circulated in the body.]
Is it water soluble?
Is it excreted in the urine?
PURPOSE:
- determine the efficacy, safety, etc., of the drug
STUDY OBJECTIVES:
- scientific questions that need to be answered
STUDY ENDPOINT & OUTCOME MEASURES:
Clinical Endpoint:
not the end of the study
statistical marker/clinical progression of the disease
Outcome:
observation recorded for patients in the trial at one or more time points after enrollment
126
METHODOLOGY:
- how the study is done
Study Design:
- How the study is structured
***Are there barriers to recruitment, retention, and compliance?
Is it randomized (to assign patients to a treatment using a random process)?
Is a placebo used in the study? Is it acceptable?
Is it double blinded (both patients and MDs do not know which drug is given to patients)?
Can patients switchover? Is it acceptable?
[Switchover: leave one treatment arm and switch to another treatment arm.]
Is is open label?
[Open label: a MD or a patient decides on the treatment to be administered.]
Look for how patients can actively participate in the trial/what decision they can make.
Sample Size and Statistical Considerations:
- statistical information
[Control Arm: a trial system of observation and data collection that provides a basis for comparison,
as with a comparison group.]
***Does this study appeal to people in your community?
Patient Selection:
- Karnofsky score
[Karnofsky score: a subjective score between 0-100, assigned by a physician to describe a
patient’s ability to function and perform common tasks.]
- genders
***Are eligibility requirement acceptable?
If one gender is excluded from the study, look for the reason.
Are you convinced of the explanation?
What are the potential or real barriers to patient enrollment?
STUDY PLAN:
- explains specimen collection and analysis
- information pertaining to drug administration
- what patients need to do
Study Medication:
- how it is provided
- how it is administered (orally, cutaneously, etc.)
- form (liquid, pill, powder)
- requirements, special preparation (refrigeration, storage, mixing drugs)
- clinic visits
***Do the potential side effects outweigh the benefit?
How realistic is it for patients to follow all instructions?
What can be a problem for patients to comply with the study requirements?
Is the drug easy to self administer?
Any specific precautions?
Look for issues that may discourage people from enrolling in the study.
Concomitant Medications:
- list of medications that can and/or cannot be taken with the study drug
Community Programs for Clinical Research on AIDS
127
Screening and Enrollment:
what information is needed for screening and enrollment
Patient Follow-up:
how patients are seen for clinical evaluation
***Look for the frequency of visits.
Do they fit with the standard of care?
Are there diaries, questionnaires, etc., that make participation more difficult?
Is the duration of the study acceptable?
Are follow-up laboratory requirements acceptable?
CLINICAL MANAGEMENT ISSUES:
- reporting requirements for clinicians
EVALUATION:
- how data are analyzed
- how safety data are evaluated
- what is evaluated
- adverse experience
[Adverse experience (AE): a toxic reaction to a treatment under study. In the CPCRA, All Grade 4
life-threatening toxicities and deaths are adverse experiences.]
DATA MONITORING:
- what kind of information is monitored and how often
PROCEDURES:
- data collection requirements for clinicians
- IRB requirements
[ITB: Institutional Review Board: a committee of physicians, statisticians, community advocates, and
others which ensures that a clinical trial is ethical and that the rights of the study participants are
protected.]
128
Denver CAB Research Training
Denver Community Advisory Board
Research Training and Orientation
August 3, 1995, 5:30 to 7:30pm
Denver Public Health Second Floor Conference Room
I Introduction/Dinner
II CPCRA
A. How is the CPCRA funded?
B. History of the CPCRA
C. What is a clinical trial?
D. Risks and benefits of clinical trials
E. Patients’ responsibilities
F. Investigator’s responsibilities (Randall/David)
III Clinical Trials
A. Types of studies
B. Factors in selecting clinical trials
C. CPCRA Concept/Protocol Development Process
D. How are research questions formulated?
1.Types of questions
2.Types of treatments
3.Planning a study
IV Elements of sound clinical trials
A. Randomization
B. Blinding
C. Eligibility
1. Safety concerns
2. Who may benefit
3. Control of variability
4. Stratification
5. Generalizability
D. Endpoints
E. Comparison Groups
F. Placebos
G. Sample size
V Parts of clinical trials
A. During
1. Data collection
2. Patients lost to follow-up
3. Monitoring data
4.“Intent to treat” analysis
B. After
1. Common closure
2. Results must be sent to everyone
3. Results must be published
4. New questions may result from the study
Conclusion
Community Programs for Clinical Research on AIDS
129
What is a clinical trial?
A clinical trial is a method of testing different medication/treatments to determine which ones are safe and
effective. There is a difference between being treated by your health care team and clinical trials. The
primary goal of a health care team is to help the patient stay healthy. While study participant’s health is an
essential part of clinical trials, the primary goal is to find out which treatments work for the most people.
Clinical trials can be funded by pharmaceutical companies, the National Institutes of Health (NIH) and other
funding sources. They can be conducted at universities, doctor’s offices and clinics. The research services
and research medications received in most clinical trials should be free and in some clinical trials study
participants get paid to be involved.
On the long road to approval
Prior to the Food and Drug Administration (FDA) approving medications for sale by pharmaceutical
companies, experimental medications must go through phases of testing to determine their safety and
effectiveness.
Phase I Clinical Trials: determine safe dosage levels of the medication/treatment being studied. The
sample size is small ranging from 10-20.
Phase II Clinical Trials: determine safety and effectiveness of the medication/treatment being studied.
There are a greater number of participants with a sample size ranging from a few dozen to a few
hundred.
Phase III Clinical Trials: determine the long term benefit from the medication/treatment. There are a
large number of participants with a sample size ranging from a few hundred to a few thousand
participants.
The CPCRA is primarily involved in Phase III clinical trials.
Once the medication/treatment has gone through testing phases, the FDA licenses the ones that are safe and
effective. At this point the medication/treatment may be prescribed by your physician. PLEASE note that not
all drugs go through all phases of testing before they receive approval from the FDA and the ones that are
determined as unsafe or ineffective are not licensed.
Risks and Benefits of Clinical Trials
Risks:
1. The treatment may not have any benefit.
2. The treatment may be harmful.
3. The medications may have side effects.
Benefits:
1.
2.
3.
4.
Participating in clinical trials will gather information which will help others.
Participants will have access to high quality medical care as well as additional care.
Research visits and research medications are free.
Participants may be among the first to receive new medications5.
People who participate in clinical
trials are taking positive action for self care.
130
Patients’ Responsibilities
Participants’ responsibilities include:
1. Full participation in informed consent to make sure that they clearly know what is involved in a clinical
trial;
2. Taking medications/treatments as prescribed;
3. Promptly informing the research nurse of any hospitalizations or opportunistic infections;
4. Notifying your research nurse of changes in medication;
5. Keeping all appointments;
6. Providing input and criticism to the investigators to help improve clinical trials.
Investigator Responsibilities
Investigator’s responsibilities include:
1. Guaranteed adequate medical care regardless of clinical trial participation or discontinuation;
2. Awareness of informed consent:
- Possible advantages of the clinical trail,
- Possible toxicities and adverse experiences22
- Additional time/effort burden,
- Disclosure of the purpose of the scientific question to be answered by the
clinical trial,
- Ongoing updates;
3. Access to answer participants questions.
4. High quality of data collection and follow-up.
5. Prompt analysis and publication.
22
A toxic reaction to a treatment under study
Community Programs for Clinical Research on AIDS
131
Types of Studies
Case Series: A study that involves persons with a condition of interest (cases) and a suitable group without
the condition (controls).
Historically Controlled: A group of patients considered to have the same disease as the study group but
were diagnosed and treated in a period of time prior to that of the study group.
Concurrent Non-randomized Controlled: A clinical trial involving one or more test treatments, at least one
control treatment, and concurrent enrollment without randomization.
Randomized Controlled: A clinical trial involving one or more test treatments, at least one control treatment,
and concurrent enrollment with randomization.
Case Series
Advantages
Historically
Controlled
Very quick
Fairly quick
No protocol or
consent required
Prospective data
collection
Concurrent
Non-randomized
Controlled
Prospective data
collection
Concurrent control
group
Randomized
Controlled
Comparable groups
Sample size
appropriate
Prospective data
collection
Disadvantages
No control group
Controls may not
be comparable
Small sample
Patients not
representative
Some cases of
PCP likely
missed
Groups not comparable
Small sample
Inappropriate
control
Patients not
representative
PCP ascertainment
may be different
Time-consuming
132
Special Situations When Uncontrolled Study May Be Appropriate23
No other treatment to use as control
Untreated patients have very poor prognosis
Treatment not expected to have serious side effects
Potential benefit to patients large and unambiguous
Result of study likely to be widely accepted
Factors in Developing Clinical Trials
Is based on a mix of factors:
- scientific
- clinical
- financial
- sociological
- ethical
1.
Timely trials are ethical
Too early: Not enough known, control likely to be better
Too late: Redundant, unattractive
2.
Tests commonly held practices that have not been proven
CD4 as indicator of therapy
Early use of AZT
Aerosol Pentamidine (AP) the superior PCP prophylaxis
Combination antiretrovirals will always be better than monotherapy
3.
Community education (clinical and patient) essential
4.
Active control trials or placebo controlled: all arms should have chance of being winner
THEREFORE: ALL STAKEHOLDERS SHOULD PROVIDE INPUT
23
Ref. Byar D, et al, NEJM, Vol 323, 1990
Community Programs for Clinical Research on AIDS
133
How Are Research Questions Formulated?
A.
Types of Questions
Does this treatment delay or prevent condition X?
For treatment of OIs or other acute conditions, does this treatment resolve condition X, or
delay relapse?
Does this treatment delay something that predicts X?
“surrogate markers” 24
Examples: CD4 as predictor of AIDS death
Often there is confusion between a marker of progression with a marker for treatment
effect
B.
In what group does this treatment have these effects?
Why does this treatment have these effects?
How does this treatment interact with other factors?
Types of Treatments:
Drugs
Devices
Non-pharmacological
Nutritional
“Body work”
Attitudinal and other “non-traditional”
C.
24
Lifestyle Interventions
Management strategies involving one of more of above
Choosing a Treatment to Study
How common is the condition to be treated?
Are there other options?
Evidence for benefit or harm that might influence choice
- Pre-clinical: in-vitro, animal studies
- Toxicology and pharmacokinetics
- Use in other conditions
- Other evidence of efficacy- anecdotal evidence
- All of these concerns are effected by availability or lack of other treatments
A test, measurement, or score that is used in place of a clinical event in the design of a trial.
134
Steps in Planning a Study
Specify research question
Define target population
Assess feasibility - sample size estimation
Observations; Readings
Research question
Aims, goals, objectives
Hypothesis
EXAMPLE
Observation
Many patients infected with HIV develop PCP
Risk of PCP increases once CD4+ drops below 200
Risk of PCP is also higher among patients with a prior episode of PCP, with HIVrelated thrush, or with unexplained fevers
Research Question
Among available drugs which one works best at preventing PCP?
To compare TMP/SMX (Bactrim) with AP in the secondary prevention of PCP
HO : The recurrence of PCP among patients given TMP/SMX equals the recurrence
of PCP among patients given AP
HA: The recurrence of PCP among patients given TMP/SMX is different than the
recurrence for patients given AP (25% vs 15% at one year)
Objective
Hypothesis
Community Programs for Clinical Research on AIDS
135
Randomization
Definition: The process of assigning patients to treatment using a random process, such as the use of
table of random numbers, the roll of a dice or the flip of a coin.
Advantages of randomization:
1.
Protects against conscious and unconscious bias;
2.
Balances influential variables making groups comparable;
3.
Makes results credible and inferences possible.
Important Points:
1.
Randomized clinical trials are essential for determining how good or bad a treatment is.
2.
The principal advantage of randomization is that the groups are similar except for the
treatments used.
Conclusion:
The goal of clinical trials is to obtain correct answers to clinically relevant question. The randomized
clinical trial, if properly designed and carried out, is the best design to use.
136
ACTG 021 Study
Baseline Comparability of Treatment Groups
TMP/SMX
(N=154)
AP
(N=156)
36
36
Male (%)
94.8
93.6
Race (% White)
71.6
69.2
Intravenous Drug Use (%)
17.6
16.9
62
51
Age (years)
CD4+
Blinding
Blind:
A condition imposed on an individual/group for the purpose of keeping the
individual/group from knowing or learning of some fact, such as treatment
assignment.
Double-blind: Participants and investigators are both unaware of treatment assignment. (example:
NuCombo)
Single-blind:
Participants blinded to treatment assignment, but the investigators are not.
(example: Acupuncture)
Non-blind:
Both patients or investigators are aware of treatment assignment.
Bactrim)
Advantage
Reduces conscious and unconscious bias.
(example:
Eligibility: Who Should be Studied?
Safety concerns
- Predisposition to toxicity
- Strong enough to survive/not be harmed by trial
- Potential benefit has good chance of outweighing potential risk
Who might benefit?
- Who is at risk of the condition being prevented or treated?
- Is this treatment appropriate for that group?
Examples of possible problems: expense; inconvenience; availability; IV treatment for ambulatory
patients.
- What is their risk?
Determines sample size, risk/benefit analysis of doing study
Community Programs for Clinical Research on AIDS
137
Control of Variability25
- Characteristics that alter risk
e.g. Previous infections, CD4 count, demographics
- Use of interacting treatments
e.g. Treatments active against same condition, or that antagonize treatment under study
- Predictors of compliance
e.g. active substance abusers
- Control of variability more useful when attempting to deduce biological activity
- Restricting variability restricts generalizability and accrual
Who Are These Results Relevant To?
Stratification26
- Are there subgroups that may vary? Is this meaningful?
Generalizability & extrapolation27
- How much are the results applicable to persons outside the trial?
Endpoints28: What Information is Important?
Primary Endpoints
Survival
Intermediate outcomes and quality of life
Composite endpoints
Surrogates
Secondary Endpoints
Clinical
- Signs and symptoms
- Other conditions
e.g. Toxo in PCP prophylaxis trial
- Toxicities
Laboratory parameters
Comparison Group
Treatment works as compared to what?
On whom?
Choice of comparison group depends on:
25
- Current knowledge
- Clinical issues
The degree to which a set of quantities vary.
The process of classifying patients into strata (a series of distinct levels) as part of the randomization process or for
data analysis
27 To infer as unknown from something known
28 A primary or secondary outcome used to judge the effectiveness of a treatment. This term most often does not indicate
the end of a study.
26
138
Placebos
- Ethics
- Practical constraints: time & money
Protects against bias due to the participants knowing the treatment
A placebo arm usually isn’t just “no intervention”
Screening, clinical visits, other treatments
No therapy placebos can be ethical IF
“No therapy” is clinically relevant
As in many prophylaxis trials
CPCRA TOXO Trial
CPCRA CMV Trial
If the question is “no big deal” e.g.
Short-term relief of nasal congestion
Community Programs for Clinical Research on AIDS
139
EXAMPLE: Effect of Antihistamine on Colds Under One Day
Duration (Br. Med. J., 1950)
After 2nd day of treatment:
Cured
Cured or Improved
13.4%
68.2%
Cured
Cured or Improved
Antihistamine
13.4%
68.2%
Placebo
13.9%
64.7%
Antihistamine
Second Day of Treatment:
Sample Size
Definition: The number of patients required for a clinical trial. The sample size is calculated using variables
making sure that there can be statistically significant results in a given period of time.
Key points:
1.
Sample size should be calculated and specified in advance.
2.
Sample size for many studies are too small which may result in misleading answers
3.
Evaluate whether sample size estimates are correct as the clinical trial progresses.
Important Points During Clinical Trials
1.
Care of data29 collection is extremely important “garbage in...garbage out”. (footnote #??)
2.
Getting follow-up on each participant is critical. Participants that are “lost to follow-up” may
skew the results.
3.
Looking for good and bad results is important. The Data Safety Monitoring Board (DSMB) is
charged with making sure study participants are safe.
4.
The “intent to treat” analysis looks at real world benefits of research.
Important Points After Clinical Trials
29
1.
Common closing date for end of study (if not stopped early) to permit timely reporting of
results
2.
Results must be sent to all concerned
3.
Results must be published so everyone knows what happened
4.
New questions with uncertainty may come up as a result of the trial
5.
Longer follow-up may be important
Information collected on study participants
140
Community Programs for Clinical Research on AIDS
141
Samples & Local CAB Materials
(Samples and Local CAB Materials will be included in the version of the CCG Handbook that will be mailed
out to Units after the Group Meeting)
142
Community Programs for Clinical Research on AIDS