981
advertisement

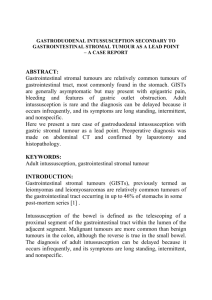
EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 Eissa & Moustafa THE ROLE OF SURGERY AND AIR REDUCTION IN THE TREATMENT OF INTUSSUSCEPTION IN YAMEN By Omar Eissa* and **Mostafa M Mostafa Departments of *General Surgery, El-Minia Faculty of Medicine and **Radiology, Assuit Faculty of Medicine ABSTRACT: Intussusception is the most common cause of bowel obstruction in children under two years of age. The proximal part of the bowel and its mesentery (the intussusceptum) enter within that part immediately beneath it (the intussuscipiens). Being pulled by peristalsis the mesenterial vessels get compressed which result in ishaemia of the bowel wall. Most intussusceptions are ileocolic. The diagnosis can be confirmed by a contrast enema or ultrasound. Therapeutic reduction can be attempted by a contrast enema (following diagnostic procedure) or by air, both under fluoroscopic monitoring, or by normal saline under sonographic guidance. When presentation is delayed, intussus-ceptions may be difficult to reduce using standard enema regimens. Our endeavour to minimize the need for surgery in an environment where failed reductions are common has led to the development of an aggressive, non-operative method of reducing intussusceptions. Thirty patients with intussusceptions were reviewed with the aim of evaluating a new method of reducing intussusceptions suited to our Third World environment. Delayed presentation was common, with 32% of patients presenting more than 48h after the onset of the intussusception. On clinical grounds alone, 41% of patients required a primary laparotomy. Standard barium and air reductions for intussusceptions were rarely successful under these conditions i.e.13% and 22%, respectively. By using an air enema under general anaesthesia in the operating theatre, the reduction rate has improved to 53%. Air enema under anesthesia is suggested as a last attempt at reducing an intussusception prior to laparotomy following failed standard enema reduction, and as the first line of management in the attempted reduction in the patient with delayed presentation without symptoms of peritonitis. KEYWORDS: Intussusception Air reductions INTRODUCTION: Nonsurgical reduction has paved the way for successful management of childhood intussusception. The success rates have varied between 63% and 95%1-24. Although the techniques of nonsurgical reduction differed in many earlier reports depending on the instit-utional site, recently, the reduction tech-nique most commonly used seems to be an air enema performed under fluoro-scopic guidance because the air is quick, less messy, Delayed presentation Surgical intervention General anaesthesia and safer than a liquid enema in bowel perforation1-3. To the best of our knowledge, there are only a few published reports dealing with the use of sonographic guidance in air enemas for nonsurgical reduction of childhood intussusceptions4. The concerns of missing bowel pathology, reduction of gangrenous bowel with consequent shock, perforation of bowel and causing peritonitis ___________________________________________________________________________________ 311 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 Eissa & Moustafa have been adequately addressed by adopting criteria for case selection and delineation of pressures of 80-130 mm Hg as effective and safe for reduction of intussusceptions25,26. It has been reported that successful hydrostatic reduction may be less likely in patients with symptoms for more than 48 hours, and consequently patients with prolonged symptoms are nowadays likely to under-go operative reduction as the first line treatment27-29. advanced disease, an awareness of the complications of Laparotomy32, and a lack of paediatric radiologists, have provided the impetus for an aggressive non-operative managment protocol. In a Third World environment, where delayed presentation of intussusceptions is common and enema reduce-tions are rarely successful, operative reductions frequently become the only option30,31. Local circumstances, such as frequently seen There were no exclusion criteria for this study. On admission, the diagn-osis of intussusception was made on clinical and radiological grounds figure (1) and was followed by an aggressive period of resuscitation. MATERIALS AND METHODS: All 30 patients treated for intussusception during a 2-year period (Jane 2007 to Jane 2009) at the Department of Surgery, Suady German hospital and Yamen International hosoital in Yamen. Figure 1. Ileocolic intussusception in a 2-year-old boy for which air enemas failed. A, Transverse sonogram of the right upper abdomen shows intramural gas (black arrowheads) peripherally located within the markedly swollen returning limb of the intussusceptum (arrows). When optimally resuscitated, usually within 1–2 h, the patient was transferred for either a reduction attempt or a laparotomy. The new method of reduction required the patient to be transferred to the operating theatre; a general anaesthetic was administered, followed by the set-up for an air reduction. This involved inserting a large Foley ___________________________________________________________________________________ 312 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 catheter (30 FG) into the rectum and partially inflating the balloon. The catheter was joined via a Y-connection to an inflation bulb and a pressure monitor. Using the inflation bulb, a steady pressure of air, not exceeding 120 mmHg for 3 min at a time, was passed into the colon. The movement of air was visualised using on-table imaging, and an attempt at reducing the intussusception was made. When the procedure failed to reduce the intussusceptions after three attempts, or when a complication occurred (e.g. a bowel perforation), the child’s abdomen was prepared, draped, and an immediate laparotomy was done. Intraoperative Details The abdomen and bowel are typically explored through a right lower quadrant transverse incision, although some advocate a right transverse supraumbilical or even an upper midline incision. After inspection for signs of perforation, the intussusception is identified and delivered into the wound. First, an attempt is made at manual reduction by retrograde milking of the intussusceptum. Although gentle pulling may aid in reduction, avoid vigorous pulling apart of the intussuscepted segment of bowel. Gentle finger pressure is necessary for reduction of intussusception. This subjective "gentleness" is dependant on experience of the surgeon and varies from person to person. Focal pressure on the intussuscipient and apex of the intussusceptum by the finger during reduction may be more damaging than the diffusely transmitted hydrostatic pressure even by a less-experienced surgeon. This will avoid the needless resection and Eissa & Moustafa anastomosis of the intestine on many occasions33. If manual reduction is unsuccessful, if a mass or pathologic lead point is present, or if perforation has occurred, segmental bowel resection is necessary. After resection, a primary anastomosis may be performed. Often after succe-ssful manual reduction, the involved segment of bowel appears edematous, hyperemic, or ischemic. These findings do not necessarily mandate resection. An incidental appendectomy is often performed, particularly if a right lower quadrant incision was made for access to the abdomen, as it may be presumed that the patient has had an appendectomy. Postoperative Details IV fluid resuscitation is continued and calculated, taking into consideration maintenance requirements and third-space losses. Upon resolution of ileus, diet is advanced at the discretion of the surgeon. RESULTS: Of the 30 patients diagnosed with an intussusception, 16(53.3%) presented within the first 48 h of developing features of this condition, and 10 (33.3%) presented later than 48 h (range 3–7 days). The remaining 4 (13.4%) patients were admitted with no indication of the duration of the intussusception, as shown in Table 1. Clinically, there was a palpable abdominal mass in 18 (60%) patients, of whom 8 (44.4%) had a left-sided or rectal mass. Fifteen (50%) patients were noted to have per-rectal bleeding. There was no correlation between leftsided masses and duration of the disease process. The classical type of ileo-colic intussusception was present in 24 ___________________________________________________________________________________ 313 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 Eissa & Moustafa (80%) patients, colo-colic intussusceptions was seen in 3(10%), and the remaining 3 (10%) patients had small bowel intussusception. An associated midgut malrotation was found in 6 patients with ileocolic intussusceptions and in one patient who had a small bowel intussus-ception. important primary treatment method, and many studies have reported it to be a widely available and highly successful technique with a low incidence of complications34-61. Initial diagnosis may be carried out by contrast enemas controlled by fluoroscopy or by ultra-sonography62-64 The patients’ abdominal presenting features determined their management. 12(40%) patients had a surgically acute abdomen at presentation, and no attempts were made to reduce their intussusceptions.One of these patients died during the resuscitation period. Although the intussusceptions seen in children of the Third World are similar to those in children in developed countries, there are some important differences: the frequent delays in presentation of patients30,32, the high incidence of colocolic intussusce-ptions66, and the frequently noted association between intussusception and midgut malrotation, called Waugh’s syndrome67. The reasons for these differences and their primary causes are unknown, but they do make the diag-nosis and simple reduction of intussus-ception more difficult. The remaining 11 (36.6%) patients went for laparotomy, at which 9 (75%) patients were found to have ischaemic bowel requiring resection. The 18 (60%) patients with no features of an acute abdomen at admission were all managed with an attempted enema reduction. Patients with intussusception and a nonacute abdomen had an attempted reduction in the operating theatre once they were optimally resuscitated and anaesthetised. This resulted in 10 (55.5%) successful and 8 (44.5%) failed reductions. The latter 8 patients were further managed with laparotomy, at which 4 (22.25%) patients had bowel necrosis and one (5.5%) patients were found to have bowel perforations. Three (10%) of the 30 patients died. The deaths were among the acute surgical group of patients and occurred either during resuscitation or subsequently from overwhelming sepsis. DISCUSSION: Nonsurgical reduction for pediatric intussusception has been an Regarding the delayed presentations in our study of 30 patients, at least 33% presented more than 48 h after the onset of the intussusception. The effects of this delay were manifest in the progression of the condition and the development of complications. In all, 10% of patients died. A further 40% of patients had a distended, peritonitic abdomen warranting a laparotomy, a decision that proved to be justified because 75% of this acute group required a bowel resection. In the 18 patients meaningful improvement was seen with the introduction of air enema reductions in theoperating theatre under a general anaes-thetic, achieving a success rate of 55.5%. Failed reduction of intussusceptions is seen in developed and underdeveloped nations alike65,68, but is a common feature and of particular ___________________________________________________________________________________ 314 Eissa & Moustafa EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 concern in our Third World environment. In such patients we perceive distinct advantages to attempting a reduction in the operating theatre on an anaesthetised child who is fully resuscitated. The child is totally relaxed and pain-free during the procedure, which thereby abolishes the unhelpful effects of a straining abdomen. This allows the intraluminal forces of the air in the bowel, at pressures not exceeding 120 mmHg for more than 3 min at a time, to act unopposed, giving this method a greater chance of success. ception in children under fluoroscopic guidance. The results of reduction with the device were equal to those by saline enema reduction under ultrasound guidance69. It was of note that the patient profile for age, as well as site and duration of the intussusception, was the same for both the successful and failed groups of the 18 patients in whom a reduction was attempted under anaesthesia. Bowel perforations are a major concern when attempting to reduce an intussusception. In two patients there was leakage of gas into the peritoneal cavity following perforation during failed air reduction. Reju and Syam have developed a portable device for insufflation of air reliably at pressures accepted as safe for effective reduction of intussus- The findings at laparotomy for the 8 failed reductions showed the presence of bowel pathology in 5 (62.5% of this group) patients as a possible cause. This finding is of particular significance, as the clinical features of compromised bowel were not present in these patients prior to the attempted reduction. It has been previously noted that although air reductions are more likely to perforate, air is safer than barium in the peritoneal cavity70. Table (1): Management versus duration (GA general anaesthetic) Duration Patients Primary surgery <48hrs 16 5 >48hrs 10 6 unknown 4 1 Total 30 12 Attempted Reduction air with GA 11 4 3 18 Conclusion: In a population group in which 33.3% of patients have a delayed presentation and in which a high incidence of ‘‘hidden’’ bowel ischaemia exists, we have improved the success rate of non-operative reduction of intussusceptions. This method is suggested as a last attempt at reducing intussusceptions prior to laparotomy and Failed Succeful reduction reduction 5 6 2 2 1 2 8 10 should be used in all patients following a failed standard enema reduction. It should also be used as the first line of management in the attempted reduction in the patient with delayed presentation without symptoms of an acute abdomen. REFERENCES: 1. Bisset GS III, Kirks DR. Intussusception in infants and children: ___________________________________________________________________________________ 315 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 diagnosis and therapy. Radiology 1988; 168:141–143. 2. Gu L, Alton DJ, Daneman A, et al. Intussusception reduction in children by rectal insufflation of air. AJR Am J Roentgenol 1988; 150:1345–1348. 3. Stein M, Alton DJ, Daneman A. Pneumatic reduction of intussusception: 5-year experience. Radiology 1992; 183: 681–684. 4. Yoon CH, Kim HJ, Goo HW. Intussusception in children: USguided pneumatic reduction—initial experience. Radiology 2001; 218:85– 88. 5. Guo JZ, Ma XY, Zhou QH. Results of air pressure enema reduction of intussusception: 6,396 cases in 13 years. J Pediatr Surg 1986; 21:1201– 1203. 6. Shiels WE II, Maves CK, Hedlung GL, Kirks DR. Air enema for diagnosis and reduction of intussusception: clinical experience and pressure correlates. Radiology 1991; 181: 169–172. 7. Tamanaha K, Wimbish K, Talwalkar YB, Ashimine K. Air reduction of intussusception in infants and children. J Pediatr 1987; 111:733–736 8. Zheng JY, Frush DP, Gui JZ. Review of pneumatic reduction of intussusception: evolution not revolution. J Pediatr Surg 1994; 29:93–97. 9 De Campo JF, Phelan E. Gas reduction of intussusception. Pediatr Radiol 1989; 19:297–298. 10. Kirks DR. Air intussusception reduction: "the winds of change." Pediatr Radiol 1995; 25:89–91. 11. Glover JM, Beasley SW, Phelan E. Intussusception: effectiveness of gas enema. Pediatr Surg Int 1991; 6:195–197. 12. Katz M, Phelan E, Carlin JB, Beasley SW. Gas enema for the reduction of intussusception: relationship between clinical signs and Eissa & Moustafa symptoms and outcome. AJR Am J Roentgenol 1993; 160:363–366. 13. Saxton V, Katz M, Phelan W, Beasley SW. Intussusception: a repeat delayed gas enema increases the nonoperative reduction rate. J Pediatr Surg 1994; 29:588–589. 14. Navarro OM, Daneman A, Chae A. Intussusception: the use of delayed, repeated reduction attempts and the management of intussusceptions due to pathologic lead points in pediatric patients. AJR Am J Roentgenol 2004; 182: 1169–1176. 15. del-Pozo G, Albillos JC, Tejedor D, et al. Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics 1999; 19:299–319. 16. Woo SK, Kim JS, Suh SJ, Paik TW, Choi SO. Childhood intussus-ception: US-guided hydrostatic reduction. Radiology 1992; 182:77–80. 17. Riebel TW, Nasir R, Weber K. US-guided hydrostatic reduction of intussusception in children. Radiology 1993; 188: 513–516. 18. Meyer JS, Dangman BC, Buonomo C, Berlin JA. Air and liquid contrast agents in the management of intussusception: a controlled, randomized trial. Radiology 1993; 188:507– 511. 19. Grasso SN, Katz ME, Presberg HJ, Croitoru DP. Transabdominal manually assisted reduction of pediatric intussusception: reappraisal of this histo-rical technique. Radiology 1994; 191: 777– 779. 20.Choi SO, Park WH, Woo SK. Ultrasound-guided water enema: an alternative method of nonoperative treatment for childhood intussusception. J Pediatr Surg 1994; 29: 498–500. 21. Rohrschneider WK, Tröger J. Hydrostatic reduction of ___________________________________________________________________________________ 316 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 intussusception under US guidance. Pediatr Radiol 1995; 25: 530–534. 22. Peh WCG, Khong PL, Chan KL, et al. Sonographically guided hydrostatic reduction of childhood intus-susception using Hartmann’s solution. AJR Am J Roentgenol 1996; 167:1237–1241. 23..Koumanidou C, Vakaki M, Pitsoulakis G, Kakavakis K, Mirilas P. Sonographic detection of lymph nodes in the intussusceptions of infants and young children: clinical evaluation and hydro-static reduction. AJR Am J Roentgenol 2002; 178:445–450. 24. Wang GD, Liu SJ. Enema reduction of intussusception by hydrostatic pressure under ultrasound guidance: a report of 377 cases. J Pediatr Surg 1988; 23:814–818. 25. .Ein SHMercer S, Humphry A, Macdonald P. Colon perforation during attempted barium enema reduction of intussusception. J Pediatr Surg 1981;16:313-5. 26. Wang GD, Liu SJ. Enema reduction of intussusception by hydrostatic pressure under ultrasound guidance: A report of 377 cases. J Pediatr Surg 1986;23:814-8. 27. West KW, Stephens B, Vane DW, et al. Intussusception: current management in infants and children. Surgery 1987; 102:704–10. 28. Davis CF, Mc Gabe AJ, Raine PAM. The ins and outs of intussus-ception: history and management over the past fifty years. J Pediatr Surg 2003; 38:60–4. 29. Reijnen JA, Festen C, van Roosmalen RP. Intussusception: factors related to treatment. Arch Dis Child 1990;65:871–3. 30. Postma MH, Hadley GP (1985) Intussusception in black children. S Afr Med J 68:405–406 31. Yang CM, Hsu HY, Tsao PN, et al. (2001) Recurrence of intussusception in childhood. Acta Paediatr Taiwan 42:158–161 Eissa & Moustafa 32.. Archibong AE, Usoro IN, Ikpi E, et al. (2001) Paediatric intussus-ception in Calabar, Nigeria. E Afr Med J 78:19–2 33.Uday Sankar Chatterjee, Ajoy Ghosh, Ashoke Kumar Basu, Partha Pratik Mukhopadhyay. Intraoperative hydrostatic reduction of intussusceptions. Journal of Indian Association of Pediatric Surgeons.2008:13:3:107108 34.Bisset GS III, Kirks DR. Intussusception in infants and children: diagnosis and therapy. Radiology 1988; 168:141–143 35. Gu L, Alton DJ, Daneman A, et al. Intussusception reduction in children by rectal insufflation of air. AJR Am J Roentgenol 1988; 150:1345–1348. 36. Stein M, Alton DJ, Daneman A. Pneumatic reduction of intussusception: 5-year experience. Radiology 1992; 183: 681–684. 37. Yoon CH, Kim HJ, Goo HW. Intussusception in children: US-guided pneumatic reduction—initial experience. Radiology 2001; 218:85– 88. 38. Guo JZ, Ma XY, Zhou QH. Results of air pressure enema reduction of intussusception: 6,396 cases in 13 years. J Pediatr Surg 1986; 21:1201– 1203. 39. Shiels WE II, Maves CK, Hedlung GL, Kirks DR. Air enema for diagnosis and reduction of intussusception: clinical experience and pressure correlates.Radiology 1991;181:169–172. 40. Tamanaha K, Wimbish K, Talwalkar YB, Ashimine K. Air reduction of intussusception in infants and children. J Pediatr 1987; 111:733–736. 41. Zheng JY, Frush DP, Gui JZ. Review of pneumatic reduction of intussusception: evolution not revolution. J Pediatr Surg 1994; 29:93–97. ___________________________________________________________________________________ 317 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 42. de Campo JF, Phelan E. Gas reduction of intussusception. Pediatr Radiol 1989; 19:297–298. 43. Kirks DR. Air intussusception reduction: "the winds of change." Pediatr Radiol 1995; 25:89–91. 44. Glover JM, Beasley SW, Phelan E. Intussusception: effectiveness of gas enema. Pediatr Surg Int 1991; 6:195–197. 45. Katz M, Phelan E, Carlin JB, Beasley SW. Gas enema for the reduction of intussusception: relationship between clinical signs and symptoms and outcome. AJR Am J Roentgenol 1993; 160:363–366. 46. Saxton V, Katz M, Phelan W, Beasley SW. Intussusception: a repeat delayed gas enema increases the nonoperative reduction rate. J Pediatr Surg 1994; 29:588–589. 47. Navarro OM, Daneman A, Chae A. Intussusception: the use of delayed, repeated reduction attempts and the management of intussusceptions due to pathologic lead points in pediatric patients. AJR Am J Roentgenol 2004; 182: 1169–1176. 48. del-Pozo G, Albillos JC, Tejedor D, et al. Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics 1999; 19:299–319. 49. Woo SK, Kim JS, Suh SJ, Paik TW, Choi SO. Childhood intussus-ception: US-guided hydrostatic reduction. Radiology 1992; 182:77–80. 50. Riebel TW, Nasir R, Weber K. US-guided hydrostatic reduction of intussusception in children. Radiology 1993; 188: 513–516. 51. Meyer JS, Dangman BC, Buonomo C, Berlin JA. Air and liquid contrast agents in the management of intussusception: a controlled, randomized trial. Radiology 1993; 188:507– 511. Eissa & Moustafa 52. Grasso SN, Katz ME, Presberg HJ, Croitoru DP. Transabdominal manually assisted reduction of pediatric intussusception: reappraisal of this historical technique. Radiology 1994; 191:777–779. 53. Choi SO, Park WH, Woo SK. Ultrasound-guided water enema: an alternative method of nonoperative treatment for childhood intussusception. J Pediatr Surg 1994; 29: 498–500. 54. Rohrschneider WK, Tröger J. Hydrostatic reduction of intussusception under US guidance. Pediatr Radiol 1995; 25: 530–534. 55. Peh WCG, Khong PL, Chan KL, et al. Sonographically guided hydrostatic reduction of childhood intussusception using Hartmann’s solution. AJR Am J Roentgenol 1996; 167:1237–1241. 56. Koumanidou C, Vakaki M, Pitsoulakis G, Kakavakis K, Mirilas P. Sonographic detection of lymph nodes in the intussusception of infants and young children: clinical evaluation and hydro-static reduction. AJR Am J Roentgenol 2002; 178:445–450. 57. Wang GD, Liu SJ. Enema reduction of intussusception by hydrostatic pressure under ultrasound guidance: a report of 377 cases. J Pediatr Surg 1988; 23:814–818. 58. Swischuk LE, Hayden CK, Boulden T. Intussusception: indications for ultrasonography and explanation of the doughnut and pseudokidney signs. Pediatr Radiol 1985; 15:388–391. 59. del-Pozo G, Albillos JC, Tejedor D. Intussusception: US findings with pathologic correlation— the cres-cent-in-doughnut sign. Radiology 1996; 199:688–692. 60. Zambuto D, Bramson RT, Blickman JG. Intracolonic pressure measurements during hydrostatic and air contrast barium enema studies in children. Radiology 1995; 196:55–58. ___________________________________________________________________________________ 318 EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 61. Miller SF, Landes AB, Dautenhahn LW, et al. Intussusception: ability of fluoroscopic images obtained during air enemas to depict lead points and other abnormalities. Radiology 1995; 197:493–496. 62.Meyer JS. The current radiological management of intussusception: A survey and review. Pediatr Radiol 1992;22:323-25. 63. Verschelden P, Filiatrault D, Garel l, Grignon A, Perreault G, Boisvert J, et al. Intussusception in children: reliability in diagnosis: A prospective study. Radiology 1992;185:741-4. 64. Zheng JY, Frush DP, Guo JZ. Review of pneumatic reduction of intussusception: Evolution not revolution. J Pediatr Surg 1994;29:93-7. 65. Pierro A, Donnell SC, Paraskevopoulou C, et al. (1993) Indication for laparotomy after hydrostatic reduction for intussusception. J Pediatr Surg 28:1154–1157 Eissa & Moustafa 66. Grant HW, Buccimazza I, Hadley GP (1996) A comparison of colo-colic and ileo-colic intussusception. J Pediatr Surg 31(12):1607–1610 67. Breckon V, Hadley GP (2000) Waugh’s syndrome: a report of six patients. Pediatr Surg Int 16:370– 373 68. Calder FR, Tan S, Kitteringham L, et al. (2001) Patterns of management of intussusception outside tertiary centers. J Pediatr Surg 36:312–315 69.Reju J Thomas,and Syam Rakhesh. An air insufflation device for reduction of intussusception in children. Journal of Indian Association of Pediatric Surgeons. 2008 : 13 : 3 : 9496 70. Maoate K, Beasely SW (1998) Perforation during gas reduction of intussusception. Pediatr Surg Int 14:168–170 ___________________________________________________________________________________ 319 Eissa & Moustafa EL-MINIA MED. BULL. VOL. 20, NO. 1, JAN., 2009 عالج االنسداد المعوى عند االطفال الناتج من تداخل االمعاء جراحيا او بحقن الهواء تحت مخدر عام عمر عيسى -مصطفى محمد مصطفى أقسام *الجراحة العامة .كلية طب المنيا و**االشعة .كلية طب اسيوط *اجرى البث فى اليمن فىى مستشىىى الىيمن الىى لى مستشىىى السىد ىى املمى فى فىى الىتىر مىن ي في 2007الى ي لي 2009 *شىىما الب ىىث 30طىىىا تتىىرا م اهم ى رشه مىىن شى ر الىىى ىىخث سىىف اش تىىه تش ي ى ه ب مشىىد الكشف امكليفيكى ب بت ه ب فسىاى مد ى ف تج هن تىا ا اممد ء بدض ببدض *أ ضىىر ش ى مء امطى ى ا بدض ى ه بدىىى 48س ى ه مىىن ىىى ث المىىرض ك ف اهشىىر اطى ى ا تىىه اسد ف ه يث ى ا مف ه 6الى الجرا مب شر بدى الت ضير الجيىى اجريىش الم لى بضى ط ال اء ت ش الم ىر الد ه فجح فى شذ الم ل لتين ال لتين ام ريين اجريىش ل مى همليى جرا ي *ام من أ ضىر للطى ارىء لبىا 48سى ه فكى ن هىىىشه 16مريضى أجىرى ا 5مىف ه همليى ش جرا ي ه جل لمف بم ل ض ط ال اء ت ش م ىر ه ه ا 11مريض فج ىش الم لى فىى 6مش لجأف للجرا فى اا 5مش ام رى *مجم ع مش الب ث 30اجريش م ل فى اممدى ء هىن طريىط ضى ط ال ى اء ت ىش م ىىر ه ه ا 18فج ش الم ل فى 10اجريش الجرا ا 8مىف ه بىذل يكى ن هىىالمرضىى التىى اجريىىش ل ىىه هملي ى ش جرا ي ى 20ت ى فى مىىف ه 3مرضىىى ا ىىىشه لبىىا الجرا ى ام ىىرين بدىىى الدملي فتيج التل ث الشىيى لبا بدى الدملي ___________________________________________________________________________________ 320