PUBLIC CHILD WELFARE
TRAINING ACADEMY
KEY TO SUCCESS
TRANSFER OF LEARNING
A TOOL FOR CHILD WELFARE SUPERVISORS
Anita Harbert, Ph.D.
Principal Investigator
Executive Director—Academy for Professional
Excellence
Professor Emeritus—SDSU School of Social
Work
Donald Dudley, MSW
Co-Principal Investigator
Director, Academy for Professional
Excellence
Prepared by:
Nancy Kail
March 2009
PCWTA is a program of the Academy for Professional Excellence at
San Diego State University School of Social Work and
California State University San Bernardino Department of Social Work.
6505 Alvarado Road, Suite 107 / San Diego, CA 92120
http://theacademy.sdsu.edu
KEY TO SUCCESS
TRANSFER OF LEARNING:
A TOOL FOR CHILD WELFARE
SUPERVISORS
CALIFORNIA’S
STANDARDIZED
SOCIAL WORKER
CORE CURRICULUM
March 2009
TABLE OF CONTENTS
TAB
TITLE
1
Introduction
2
Framework for Child Welfare Practice in California
3
Child and Youth Development in a CW Context
4
Child Maltreatment Identification 1: Neglect,
Physical Abuse and Emotional Abuse
5
Child Maltreatment Identification 2: Sexual Abuse
6
Critical Thinking in Child Welfare Assessment:
Safety, Risk and Protective Capacity
7
Family Engagement in Case Planning and Case
Management
8
Placement and Permanency
9
Common Handouts (used throughout the course)
10
Master Glossary and References
Introduction
The Public Child Welfare Training Academy (PCWTA) and your county
have collaborated in developing this transfer of learning tool for supervisors.
Its purpose is to introduce supervisors to the training that their new social
workers are receiving and to assist supervisors in supporting this training on
the job.
In response to the Federal Child and Family Services Review (CFSR),
California developed a Performance Improvement Plan (PIP) which includes
standardized training for all child welfare social workers in the State of
California. The PCWTA Southern Region is responsible for delivering this
training to Imperial, San Diego, Orange, Riverside and San Bernardino
Counties. Seven of the sixteen classes in the Social Worker CORE series
are standardized. They are:
1. Framework for Child Welfare Practice in California
2. Child and Youth Development in a CW Context
3. Child Maltreatment Identification 1: Neglect, Physical Abuse and
Emotional Abuse
4. Child Maltreatment Identification 2: Sexual Abuse
5. Critical Thinking in Child Welfare Assessment: Safety, Risk and
Protective Capacity
6. Family Engagement in Case Planning and Case Management
7. Placement and Permanency
Attached to this introduction is an example of a full SW CORE course
schedule so you can see how these standardized classes are incorporated into
the course.
Transfer of Learning (TOL) is the application of skills and knowledge
learned in one context (the classroom) and applied to another context (the
job). Research shows that successful TOL will result in a higher level of
performance and increased quality of services provided to clients. Also,
staff that performs better on the job is more motivated to stay on the job.
The supervisor’s role is critical in the TOL process. You have the
opportunity and responsibility for helping your staff practice and apply what
they have learned in the classroom to their particular job. The classroom is
an extension to the job environment. Yes, it means extra work for you at
first because it takes some planning, thought, follow-up and modeling on
your part. But the payoff is seen in staff better prepared to do their difficult
job, staff who have good communication with their supervisor and staff who
grow and develop into confident, capable employees who can eventually
become competent mentors to other new staff.
The following tool has been developed to assist supervisors in planning
activities for new child welfare workers that will apply classroom skills and
knowledge on the job. It is a guide and intended to supplement on the job
training. Included in each section of the standardized Core classes are:
competencies and learning objectives
suggested TOL activities for you to review and/or assign to new staff,
and
supporting handouts.
Suggestions for using this tool to its maximum capacity would be to not only
use it 1:1 with your new staff, but also as a learning tool for yourself and for
your work unit as a group. Before writing on the activity pages, you may
want to copy them for reuse.
We hope you find this a useful tool. If you need additional assistance or
have any questions you may contact either of the following two Academy
staff:
Nancy Kail, Training Site Director
Oceanside Training Site
(760) 757-1592
NKail@projects.sdsu.edu
Rachel Hamilton, Training Site Director
Riverside Training Site
(951) 682-2580
rhamilton@projects.sdsu.edu
PUBLIC CHILD WELFARE TRAINING ACADEMY
Core Practice Course
Oceanside Training Center
September 11, 2007 to October 18, 2007
Date
9/11
9/12
Time
9-4
9-4
9/13
9/14
9/18
9/19
9/19
9/20
9/25
9-4
9-4
9-4
9-12
1-4
9-4
9-4
9/26
9-4
9/27
9/28
10/2
10/3
10/4
10/9
10/10
10/11
10/16
10/17
9-4
9-4
9-4
9-4
9-4
9-4
9-4
9-4
9-4
9-4
10/18
9-4
CEU
Course Title
Framework for Child Welfare Practice in California
CW Practice in a Multi-Cultural Environment
Child and Youth Development in a CW Context
Child Maltreatment Identification 1: Neglect,
Physical Abuse & Emotional Abuse
Child Maltreatment Identification 2: Sexual Abuse
6
Instructor
Nancy Kail, BA
Kahalifa King, MS, MA
Donna Pence, BS
Renee Sievert, RN,
MA, MFT
Lilli Miles, MA
Amy Stephen, LCSW
*Investigation Skills in CWS/*Crisis Intervention
Strategies
Critical Thinking in Child Welfare Assessment:
Safety, Risk and Protective Capacity
Family Engagement in Case Planning and Case
Management
Basic Interviewing
Placement and Permanency
Jessica Newmyer, BA
Court Procedures 1: Juvenile Court
Documentation for Legal Reports
Court Procedures 2: Testimony
Substance Abuse
Domestic Violence
David Casey, JD
Judi Nodurft, BA
Donna Pence, BS
Scott Johnson, LAC
Raymond Cameron,
MFT
Suzann Backes, MSW
Personal Safety/Time Management & CWS
Michelle Runnels,
MSW
Lisa Walker, BA
Lilli Miles, MA
Mike Jones, LCSW
*Course meets qualifications for number of hours listed above for continuing education
credit for post LCSWs and/or MFTs as required by the Board of Behavioral Sciences.
CEU Provider Number: PCE 3776
To receive CEUs, participant must bring a $35.00 check, on the day of the training only,
made out to “SDSU Research Foundation.” Cash and/or credit cards will not be
accepted. CEUs are not issued retroactively.
FRAMEWORK FOR CHILD WELFARE PRACTICE
IN CALIFORNIA
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
The trainee will understand the federal, state and county emphasis on achieving positive
and measurable outcomes for families and children.
The trainee will understand how evidence-based research contributes to the improvement
of public child welfare practice and outcomes.
The trainee will recognize and value the need for fair and equitable treatment of children,
youth, and families that addresses their unique sociocultural context.
The trainee will understand and value the importance of engaging children, youth,
families, kin networks, care providers, and community resources in a collaborative,
strength-based process.
LEARNING OBJECTIVES
Knowledge:
K1.
The trainee will be able to identify the three goals of the Adoptions and Safe
Families Act (ASFA) of 1997.
K2.
The trainee will be able to recognize the related outcomes and performance
indicators that are part of California’s Child Welfare Outcomes and
Accountability System.
K3.
The trainee will be able to describe an example of an evidence-based practice
implemented in California and the rationale that supports it.
K4.
The trainee will be able to identify the concepts of fairness and equity in child
welfare, and decision points in the life of a case where such issues may arise.
K5.
The trainee will be able to identify key concepts of strength-based practice.
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
K6.
The trainee will be able to describe effective strategies for engaging families and
youth.
Skills:
S1.
Given a case scenario, the trainee will be able to identify the strengths of the
child(ren), youth, parents and extended family members.
Values:
V1.
The trainee values the role of evidence-based research in advancing the efficacy
of social work practice.
V2.
The trainee values the importance of addressing the issue of disproportionality in
child welfare practice.
V3.
The trainee values engaging the family and youth as experts in identifying their
strengths, needs, and resources.
V4.
The trainee values collaborative decision-making involving families, kin and
community representatives, while acknowledging the potential impacts of
authority and power in the engagement process.
RELATED TITLE IV-E COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student demonstrates sensitivity to clients’ differences in culture, ethnicity, and sexual
orientation. (1.1)
Student demonstrates the ability to collaborate with individuals, groups, communitybased organizations and government agencies to advocate for equitable access to
culturally sensitive resources and services. (1.5)
Student is aware of forms and mechanisms of oppression and discrimination pertaining to
low income and single parent families and uses this knowledge in providing appropriate
child welfare services. (2.5)
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Student understands the importance of working together with biological families, foster
families, and kin networks, involving them in assessment and planning and helping them
cope with special stresses and difficulties. (2.14)
Student understands and can appropriately utilize authority and power in professional
relationships. (2.16)
Student demonstrates the ability to assess his or her own emotional responses to clients,
co-workers, and situations in which the worker’s values are challenged. (2.17)
Student demonstrates the ability to engage and work with involuntary clients. (2.18)
Student is able to engage and assess families from a strengths-based “person in
environment” perspective and to develop and implement a case plan based on this
assessment. (2.19)
Student demonstrates understanding of the influence of culture on human behavior and
family dynamics. (3.4)
Student demonstrates understanding of how the strengths perspective and empowerment
approaches can influence growth, development, and behavior change. (3.5)
Student demonstrates knowledge of the philosophy, purpose, requirements, and
application of federal and state child welfare policy and legislation. (6.1)
Student works collaboratively with biological families, foster families, and kin networks,
involving them in assessment and planning and helping them cope with special stresses
and difficulties. (6.6)
Student is able to identify agency and legislative policies and procedures that create
barriers to the growth and development of children and families. (7.4)
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
FRAMEWORK FOR CHILD WELFARE
PRACTICE IN CALIFORNIA
1. Locate and review your County’s County SelfAssessment (CSA), System Improvement Plan (SIP)
and Peer Quality Case Review (PQCR). What are
identified strengths and areas needing improvement?
What are identified strategies for improvement? Have
a discussion on what you can do in your job to
improve outcomes for children and families.
2. Research the formal/informal procedures in your
county for family group conferencing that ensures
families are engaged in a respectful manner that draws
on their strengths. Together, identify a case where
family group conferencing may be beneficial.
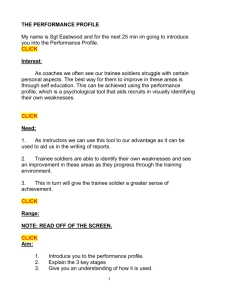
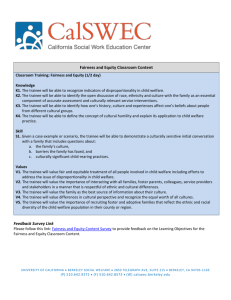
3. Review the graph in the trainee manual titled,
Ethnicity at Decision Points of the California Child
Welfare System - 2006. Have a discussion to ensure
understanding. Is there a disproportionality of
children of color in your county as compared to your
general population? If yes, what ethnicities are
overrepresented/underrepresented? Has your county
developed a strategy to minimize this? Have a
discussion on what you can do you in job to have a
positive impact on this disproportionality.
4. Using one of your cases, discuss family strengths that
were identified, of the parent, child, caretaker,
extended family members and community resources.
5. Using one of your cases, have a discussion on any
identified cultural issues of the family. Do you have
any personal biases that may affect decision making?
What can you do to minimize this?
6. Review the handout in the SW CORE training manual
titled, Evidenced-Based Practice. What are some
evidenced based and/ or promising practices currently
being used in your county? How might you utilize
these programs in your practice?
DATE
COMPLETED
Ethnicity at Decision Points of the
California Child Welfare System-2006
100%
3.30
9.8
0.5
3.9
0.9
4.0
1.1
3.1
80%
50.3
60%
51.6
48.6
Other
42.4
25.7
28.4
Population
(9,988,199)
Native
American
Hispanic
27.9
White
31.9
6.1
1.4
Asian/PI
29.6
0%
2.3
48.0
40%
20%
1.4
15.4
14.9
19.0
Referrals
(441,260)
Substantiations
(108,290)
Entries
(34,508)
28.3
Black
In Care
(77,232)
Chart taken from presentation by Barbara Needell, CSSR UC Berkeley,
California’s Child Welfare System: Using Data From CWS/CMS, February 2008
43
Evidence-Based Practice: Keeping up-to-date on the latest
and most effective practices
Research findings enhance our ability to build evidence about what works. Child welfare
professionals, like practitioners in the fields of science or technology, must consider
research and evidence as they practice. Just as a doctor uses a number of tests that have
demonstrated effectiveness in the detection and treatment of diseases, so will a social
worker use tools and practices that have been shown to be effective when working with
families.
Establishing an evidence-based practice system is one of the missions for child welfare
improvements in California at the state and county levels. This means that when there is
evidence indicating that a particular practice is effective, the worker will consider using
that practice, in conjunction with his/her critical thinking skills, for performing
assessments and other case planning activities.
Eileen Gambrill at the University of California, Berkeley, has written extensively on
evidence-based practice: “Evidence-based social work practice can be simply defined as
a set of tools and resources for finding and applying current best evidence from research
to service delivery with children and families. It also involves the integration of best
research evidence with clinical expertise and client values. Exhaustive, rigorous reviews
are not available regarding many practice questions. This does not negate the ethical
requirement to search carefully for research findings related to important practice
decisions, to critically appraise what is found, and to share what is found (including
nothing) with clients (Gambrill, 1999 in CWS Redesign, the Future of Child Welfare
Services).”1
A note on research and evidence-based practice
Much of the research in child welfare—particularly related to risk factors associated with
abuse and neglect—is deficit-based; it reviews family characteristics or behaviors and
measures whether these characteristics or behaviors (usually negative) are significantly
associated with the incidence of abuse or neglect. Since evidence-based practice involves
critical thinking about research and using it to inform practice, remember the following:
Even highly correlated behaviors or characteristics are not absolute. The worker
must evaluate the information specific to each family on a case-by-case basis.
Research does not dictate decisions in child welfare assessment -- it structures
thinking and informs practice. Research is applied within a context of clinical
expertise and client values.
1
Gambrill, E. (1999) in California Department of Social Services, CWS Stakeholders Group. (2003). CWS
Redesign: The Future of Child Welfare Services, Final Report. Sacramento, CA. Retrieved
October 6, 2003, from http://www.cwsredesign.ca.gov/res/pdf/CWSExecutiveSummary.pdf
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Keeping up with the latest practices through training
As practitioners, it is critical that we use methods that have been demonstrated to be
effective for working with children and families by continually updating our knowledge
and skills. For this reason, every practitioner needs ongoing and advanced training to
ensure state-of-the art and ethical practice.
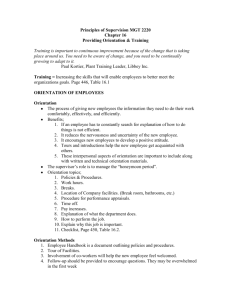
Cycle of evidence-based child welfare practice development
As envisioned, child welfare practice will continue to be informed by the Cycle of
Evidence Based Practice. Please see the diagram below.
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
CHILD & YOUTH DEVELOPMENT
IN A CHILD WELFARE CONTEXT
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
The trainee understands how child/adolescent development is affected by multiple
factors, including socioeconomic stressors and poverty in particular, ethnocultural
background, parent-child interactions, child abuse and neglect, and delays and disorders
common to children in the child welfare population.
The trainee understands children’s developmental needs and how developmental level
affects a child’s perception of events, coping strategies, and physical and psychological
responses to stress and trauma.
LEARNING OBJECTIVES
Knowledge:
K1.
The trainee will be able to recognize key concepts of three developmental theories
and describe their relevance to child welfare practice.
K2.
The trainee will be able to explain and give examples of the processes and
milestones of normal development of infants, toddlers, pre-schoolers, school-age
children, and adolescents across the physical, cognitive, social, emotional, and
sexual domains.
K3.
The trainee will be able to provide examples of how cultural variations, such as
parenting practices, can influence the manifestation and timing of developmental
skills and stages.
K4.
The trainee will be able to explain how parent-child interactions affect early brain
development, and provide examples of parenting behaviors that stimulate optimal
brain development.
K5.
The trainee will be able to provide examples of how parent-child interactions
affect the development of attachment and bonding.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
K6.
The trainee will be able to explain how physical and emotional trauma and
neglect affect brain function and development.
K7.
The trainee will be able to recognize the symptoms of PTSD in children and
adolescents, and be able to articulate when a mental health referral is useful or
necessary.
K8.
The trainee will be able to recognize possible adverse consequences of in utero
drug and alcohol abuse on infant and child development, including fetal alcohol
syndrome, mental retardation and developmental delays.
K9.
The trainee will be able to identify symptoms associated with failure to thrive and
be able to articulate when a medical assessment is useful or necessary.
K10. The trainee will be able to recognize the principal characteristics of Attention
Deficit Hyperactivity Disorder and the basic concepts underlying current methods
of assessment and treatment.
K11. The trainee will be able to identify the social, communication, and behavioral
indicators associated with autism and other pervasive developmental disorders
and explain why early intervention is important.
Skills:
S1.
Given a case example, the trainee will be able to distinguish between normal and
delayed developmental milestones.
S2.
Given a case example, the trainee will be able to articulate, in terms a parent can
understand, strength-based parenting strategies for children at different stages of
development.
S3.
Given a case example, the trainee will be able to analyze symptoms and possible
causes of developmental delays and disorders and recommend appropriate
referrals and interventions.
Values:
V1.
The trainee will value an understanding of how poverty, lack of education,
community distress and environmental stressors can impair a parent’s ability to
provide for a child’s developmental needs.
V2.
The trainee will value the importance of utilizing a strength-based perspective
with families/caregivers when gathering information and assessing the child’s
developmental history.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
V3.
The trainee will value and respect cultural variations in child-rearing practices and
beliefs when working with families from diverse ethnic, racial, and socioeconomic backgrounds.
V4.
The trainee will value the importance of keeping abreast of emerging research
evidence regarding attachment, child development, and disorders of childhood,
and applying current knowledge to child welfare practice.
V5.
The trainee will develop an awareness of the challenges that affect a parent’s
ability to provide care and nurturance to a child with a developmental delay,
medical challenge, and/or mental or emotional concern.
V6.
The trainee will value advocacy for early and appropriate interventions to assist
children with disorders, delays and other challenges associated with prenatal
exposure to alcohol and drugs, or resulting from other causes.
RELATED TITLE IV-E COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
The trainee demonstrates his/her understanding of the various stages, processes, and
milestones of physical, cognitive, social, emotional, and sexual child development.
The trainee understands the dynamics of teen sexuality.
The trainee understands how the strengths perspective and empowerment approaches can
influence growth, development, and behavior change.
The trainee understands the influence and value of traditional, culturally based
childrearing practices and uses this knowledge in working with families.
The trainee understands how attachment, separation, and placement affect a child and
family and how these experiences may influence a child’s physical, cognitive, social, and
emotional development.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
CHILD AND YOUTH DEVELOPMENT IN A
CW CONTEXT
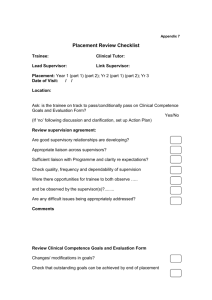
1. Review the booklet from the trainee manual titled
Child Development Milestones. Be able to articulate,
in language that the parent can understand, strength
based parenting strategies for children at different
stages of development. How may you use this
information in one of your cases?
2. Review the handout in the trainee manual titled The
Role of Culture in Development. We know that child
development cannot be assessed without a basic
understanding of the cultural environment that
surrounds and shapes a child’s experiences. Using one
of your cases, identify questions you would like to ask
about the family’s culture that would help you better
assess the child’s/children’s development.
3. Review the handout in the trainee manual titled The
Impact of Parental Substance Abuse on Children:
Specific Substances. Discuss one of your cases, where
parental substance abuse is an issue. How has the
child/children been affected? Depending on the age of
the child/children what interventions would be
appropriate? What resources are available, in your
county, for consultation and/or services for children
whose development may be affected by their parent’s
substance abuse?
4. Review the handout in the trainee manual titled Failure
to Thrive. Failure to thrive is decelerated or arrested
physical growth associated with poor development and
emotional functioning. It can be organic or nonorganic. Have a discussion about the signs, symptoms
and prevention. What resources are available, in your
county, for consultation in identify these children and
for services available once they are identified. How
can you access these services?
5. Review the handout in the trainee manual titled
ADHD and Depression. Many children have mental
health problems that interfere with normal
development. Discuss signs of and treatments for
ADHD. How may it affect school and social life?
Discuss signs, symptoms, risks and treatments of
depression. What resources are available, in your
county, for consultation and services for these
children? How can you access these services.
DATE
COMPLETED
Normal physical development: Approximately birth to 3
months
Birth to 3 months: Gains about 1 oz. per day after initial
weight loss in first week
Developed by the Northern California Training
Academy
and reprinted by CalSWEC with permission.
Child Developmental
Milestones
Birth
Reflexes (e.g., sucking, grasping, hands fisted, random
movement, etc.)
Vision at 8-12 inches and can lift head
1 month
Can lift head to 45-degree angle
Vocalizes and gurgles
2 months
Alert to people
3 months
Chuckles
Smiles
Whines and vocalizes
Rolls over
1
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Activities that promote healthy growth: Approximately
birth to 3 months
Developmental Concerns: By the end of 3-4 months
Offer me a finger to hold. Listen to me and learn my
responses. Smile and touch me when you talk to me. Tell
me I am wonderful.
Help me to develop trust. Gently hold me while talking in
sweet encouraging tones. Call me by name and make eye
contact.
Pick me up when I cry and reassure me. Don’t leave me
alone crying and give me the impression that no one cares
for me.
Learn how to soothe me and meet my needs before I cry.
Gently rub my back, sing to me, play music for me or
bounce me gently to music. I am sensitive to sound so
keep music low.
Hold me securely in new places and protect me.
Keep me clean, well fed and clothed appropriately for the
temperature.
Give me colorful toys that make interesting sounds.
Sucking calms me so let me suck my fingers or a pacifier.
Be gentle and don’t interrupt my sucking by pulling or
jiggling something I’m sucking on.
Alert your child’s doctor or nurse if your child displays any
of the following signs of possible developmental delay for
this age range:
Does not seem to respond to loud noises
Does not notice hands by 2 months
Does not follow moving objects with eyes by 2 to 3
months
Does not grasp and hold objects by 3 months
Does not smile at people by 3 months
Cannot support head well by 3 months
Does not reach for and grasp toys by 3 to 4 months
Does not babble by 3 to 4 months
Does not bring objects to mouth by 4 months
Begins babbling, but does not try to imitate any of your
sounds by 4 months
Does not push down with legs when feet are placed on a
firm surface by 4 months
Has trouble moving one or both eyes in all directions
Crosses eyes most of the time (occasional crossing of the
eyes is normal in these first months)
Does not pay attention to new faces or seems very
frightened by new faces or surroundings
Experiences a dramatic loss of skills he or she once had
2
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
3
Activities that promote healthy growth: Approximately 4-6
months
Normal physical development: Approximately 4-6 months
4-6 months: Gains 5-6 oz. per week
During bath time, try washing me in a sitting position. I
may also want to sit up and play. Help me sit up for 5-10
minutes and help me keep my back straight.
Give me safe healthy finger foods at 5-6 months. (e.g.,
crackers)
Lay me on a blanket on the floor and let me roll and
reach.
Spend time with me - play, smile, nod, talk and laugh
with me. Give me toys or attention when I need a
distraction.
Respond to my fears and cries by holding, talking to and
reassuring me. Talk to me about what I’m feeling and tell
me that it’s OK.
Talk to me, sing to me or give me my favorite toy at
diaper changing time. Don’t scold, make loud noises or
frowning faces.
Keep me in my car seat even if I complain. Distract me
with songs or toys and reassure me. Put my seat where I
can see outside.
Avoid separating me from you for days. I need consistent,
reliable relationships so if you leave me for long periods
expect me to be more clingy for awhile and need more
reassurance.
4 months
Grasps rattle
Pulls to sit up
Can bear some weight on legs
Laughs and smiles
5 months
Birth weight doubles
Sits without support
Feeds self cracker
Turns toward voice
6 months
Adds 2-3 inches to height
Sits up
Holds 2 cubes and works to reach for desired toy
Imitates speech sounds
4
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
5
Developmental Concerns: By the end of 7 months
Normal physical development: Approximately 7-11 months
Alert your child’s doctor or nurse if your child displays any of the
following signs of possible developmental delay for this age range:
7-11 months: Gains 2-3 oz. per week
Seems very stiff, with tight muscles
Seems very floppy, like a rag doll
Head still flops back when body is pulled to a sitting position
Reaches with one hand only
Refuses to cuddle
Shows no affection for the person who cares for him or her
Doesn’t seem to enjoy being around people
One or both eyes consistently turn in or out
Persistent tearing, eye drainage, or sensitivity to light
Does not respond to sounds around him or her
Has difficulty getting objects to mouth
Does not turn head to locate sounds by 4 months
Does not roll over in either direction (front to back or back to front)
by 5 months
Seems impossible to comfort at night after 5 months
Does not smile on his or her own by 5 months
Cannot sit with help by 6 months
Does not laugh or make squealing sounds by 6 months
Does not actively reach for objects by 6 to 7 months
Does not follow objects with both eyes at near (1 foot) and far (6 feet)
ranges by 7 months
Does not bear weight on legs by 7 months
Does not try to attract attention through actions by 7 months
Does not babble by 8 months
Shows no interest in games of peek-a-boo by 8 months
Experiences a dramatic loss of skills he or she once had.
7 months
Plays peek-a-boo, pulls to stand, gets to sitting position
Nonspecific “dada” or “mama”
8 months
Thumb-finger grasp is weak
Shakes head “no” and shouts for attention
9 months
Walks holding onto furniture and plays pat-a-cake
Shy with strangers
10 months
Stands momentarily
Specific “dada” or “mama” and can put 2 words together
11 months
Stands alone well
Plays ball with strangers
May recognize words as symbols
6
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
7
Activities that promote healthy growth: Approximately 7-11
months
Play peek-a-boo, puppets, wave bye-bye, and teach me
words and colors even if I can’t repeat the words right
now.
Have a regular bedtime routine. Slow my activity an hour
before bedtime, rock me, pat my back and bring my
favorite blanket. Once dry, fed and well prepared for bed,
leave me with a kiss. Ignore my cries for a few minutes
until I am asleep.
Encourage physical exploration within your eyesight.
Keep dangerous objects away from me and baby-proof
my environment. Be there to comfort me when I get hurt.
Help me stand by holding my hands. Make sure my heels
are flat.
I may purposefully drop and throw things as an
experiment. Give me safe things to drop and throw.
Open a cupboard in the kitchen kept safe for my
exploration. Keep only non-breakable objects that are
baby-friendly.
Give me something interesting on my tray to explore at
mealtime. (e.g., cooked spaghetti, spoons)
Do not force me to eat and understand that I am learning
and will be messy with my food.
Development Concerns: By the end of one year
Alert your child’s doctor or nurse if your child displays any
of the following signs of possible developmental delay for
this age range.
Does not crawl
Drags on side of body while crawling (for over one
month)
Cannot stand when supported
Does not search for objects that are hidden while he or
she watches
Says no single words (“mama” or “dada”)
Does not learn to use gestures, such as waving or shaking
head
Does not point to objects or pictures
Experiences a dramatic loss of skills he or she once had
8
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
9
Normal physical development: Approximately 12-23 months
1 year
Birth weight triples
Stoops and recovers, learning to drink from cup, pulls up
to a standing position, walks holding on to furniture
Knows 3 words other than “mama” or “dada”
13–14 months
Scribbles, 6+ word vocabulary, tries to sing, points
Walks backwards. Better cup control, spilling less
Towers 2 cubes and begins using a spoon
15–16 months
Begins using double syllable words and asks “What’s
that?” Learns names of body parts, objects, colors
Removes clothes, pulls adult hand to show something
17-19 months
Walks up steps, towers 4 cubes, asks for “more,” 20 word
vocabulary, hands toy to adult if unable to operate
Throws ball, follows directions, helps in simple tasks
20-23 months
Kicks ball forward, jumps in place, puts on clothes
Plays with 2 toys, pedals tricycle, towers 8 cubes, washes
and dries hands
10
Activities that promote healthy growth: Approximately
12-23 months
Learning to walk takes time. Hold my hand and encourage
me to take steps when I’m ready, don’t rush me.
If I grab, hit or bite when I’m mad, don’t scold me or hit me.
Teach me words to use instead of hurting others.
It will take time before I’m able to do many things. Set
limits, but I will break rules many times before I learn.
“No!” is not enough, please explain why. (e.g., “The stove is
too HOT!” Move me and show me a safe place to play.)
Give me choices whenever possible. Don’t say “no” too
often and distract me if I am refusing something. Reward
me for good behavior. Ignore my “no” if I do not get a
choice.
Let me scribble with thick washable crayons or felt markers,
tape a paper to the table so it doesn’t slip.
Compare colors and sizes with me (big spoon, red balloon).
Tell me about the story, let me pat the pages and make
noises, help me learn to turn pages by half lifting one.
Building blocks, sandboxes, ride and pull toys, jack-in-thebox, music toys and balls are very important learning tools.
Understand that me and mine are important before I can
learn about you and yours. Set up a box that is mine.
Teach me about not hurting others and sharing, but don’t
shame me. Be patient and encourage my empathy for
others.
11
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Developmental Concerns: By the end of 2 years
Normal physical development: Approximately 2-4 years
Alert your child’s doctor or nurse if your child displays any
of the following signs of possible developmental delay for
this age range:
Cannot walk by 18 months
Fails to develop a mature heel-toe walking pattern after
several months of walking, or walks only on his toes
Does not speak at least 15 words
Does not use two-word sentences by age 2
By 15 months, does not seem to know the function of
common household objects (brush, telephone, bell, fork,
spoon)
Does not imitate actions or words by the end of this period
Does not follow simple instructions by age 2
Cannot push a wheeled toy by age 2
Experiences a dramatic loss of skills he or she once had
2 years
Average height: 32-36”, weight: 22-31 lbs
Uses short sentences and adds “ing” and plurals
2 ½ years
Average height: 33-38”, weight: 24-34 lbs
Gains muscle control for toilet training
Asks “what, where, who” questions
Shows interest in peers, has difficulty sharing
Displays some self-control
3 years
Average height: 33-42”, weight: 24-42 lbs
Buttons clothes, walks downstairs and uses the toilet
Increased vocabulary and uses past tense, asks “why”
Has difficulty sharing and develops a basic sense of time
Identifies preferences and increased sense of self
Loses swayed back and large abdomen of the toddler at 3
½ years old
Can balance on one foot briefly and walks heel to toe
4 years
Catches a ball 2 out of 3 times and cuts with scissors
Talks to self and can share better
12
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
13
Strategies for potty training and tantrums: Approximately
2-4 years
Activities that promote healthy growth: Approximately
2-4 years
Let me do it myself when possible. Let me feed myself even if I’m
messy. Give me 2 choices when you can.
Let me make choices about the food I eat and let me refuse food.
Reduce in-between snacks so I will be hungry at mealtimes. Don’t
use food as a reward or punishment.
Teach me about dangerous things (matches, knives, strangers,
stray animals, cars, etc.). Significant consequences should be given
for dangerous behavior after giving warnings.
Naps are still important to reduce cranky and moody behavior.
Give me a warning that it will soon be time to move along.
Don’t hurry me too much, I need patience and time to learn.
Read to me, color with me, teach me games.
If there is a new baby, remember I will be jealous. Assure me of
your love, give me special time and let me help with the baby.
Talk to me about what I’m feeling - comfort me and don’t scold
me.
Offer a hand when I’m in a new situation as a substitute for
picking me up. Don’t insist I have to grow up.
Blow bubbles for me. Teach me to catch and throw a ball.
Respect my fears and do not force me into fearful situations.
Comfort me and encourage me that there is nothing to fear.
Potty training tips
No age is exact for toilet training. Watch for me to grimace at dirty
diapers, show you my wet pants and stay dry for up to 2 hours. I
need to be verbal enough to understand toilet training.
Change me as soon as possible, tell me it’s nice to be clean
Let me have a toy to keep me happy and busy on the potty-chair. Put
me on the potty briefly at first (up to 5 minutes).
Praise my efforts and encourage me to let you know when I need to
go potty. Teach me the family words for toilet training.
Dress me in easy to remove clothing, be patient, never scold me, visit
the potty before going somewhere, help me wipe, teach me to wash
my hands and show me how to flush.
Tantrums
Make sure I get enough sleep, eat healthy and keep a regular routine.
I need physical activity during the day. Teach me to ride a tricycle,
encourage running, dancing and jumping.
Learn warning signs and distract me. Don’t expect too much.
Since tantrums are a release of frustrated feelings and a way to get
attention, ignore me if I’m in a safe place. Don’t reward tantrums.
Stay calm and leave me reassuring me you will be back when I’m
quiet. When I stop, talk to me, tell me what I’m feeling. Help me
express my frustration in words.
14
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
15
Development Concerns: By the end of 4 years
Development Concerns: By the end of 3 years
Alert your child’s doctor or nurse if your child displays any
of the following signs of possible developmental delay for
this age range:
Alert your child’s doctor or nurse if your child displays any
of the following signs of possible developmental delay for
this age range:
Frequent falling and difficulty with stairs
Persistent drooling or very unclear speech
Cannot build a tower of more than four blocks
Difficulty manipulating small objects
Cannot copy a circle by age 3
Cannot communicate in short phrases
No involvement in “pretend” play
Does not understand simple instructions
Little interest in other children
Extreme difficulty separating from mother or primary
caregiver
Poor eye contact
Limited interest in toys
Experiences a dramatic loss of skills he or she once had
Cannot throw a ball overhand
Cannot jump in place
Cannot ride a tricycle
Cannot grasp a crayon between thumb and fingers
Has difficulty scribbling
Cannot stack four blocks
Still clings or cries whenever parents leave
Shows no interest in interactive games
Ignores other children
Doesn’t respond to people outside the family
Doesn’t engage in fantasy play
Resists dressing, sleeping, using the toilet
Lashes out without any self-control when angry or upset
Cannot copy a circle
Doesn’t use sentences of more than three words
Doesn’t use “me” and “you” correctly
Experiences a dramatic loss of skills he or she once had
17
16
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Normal physical development: Approximately 5-7 years
Activities that promote healthy growth: Approximately
5–7 years
Average height: 40-50”, weight: 34-55 lbs.
4-5 years
Paints and colors, draws figures in 6 parts, learning shapes
and colors
Climbs, runs, bike or trike riding
Broad vocabulary, listens carefully, asks questions
Learning letters, numbers and written name
Recognizes differences and similarities
Short and long term memory improves
Develops friendships with peers, recognizes gender
Believes rules can change to suit their own needs
6-7 years
Body proportions are similar to that of an adult
Imagination is an important part of development
Enjoys achieving in sports, rides a bike without training
wheels and learns to skate
Can learn to swim, swing, climb on jungle gyms and other
more complex physical tasks
Learning to read and do simple math
Understands concepts of first, next, last, large, larger, etc.
Understands time concepts of yesterday, today, tomorrow
Looks forward to holidays, birthdays and annual events
Discuss physical gender differences with me. Teach me the
proper names for body parts without shame. If I am old enough
to ask the question, I am old enough to understand the answer.
Don’t give me more information than I ask for.
Create a home library with interesting books about heroines and
heroes, fables and fun stories. Read to me every day and let me
read a part of each book, discuss the ideas in the book.
Remember rewards works better than punishment. Have a
sticker chart, give balloons, pennies for the bank, etc.
Play children’s music, sing, clap and dance with me.
Encourage physical involvement and imaginative expression.
(e.g., “Itsy-Bitsy Spider” and “I’m a Little Teapot”)
Teach me to count, sing my ABC’s and write my name with lots
of patience. This will take time and repetition.
I need a bike or trike, balls, clay and play space with toys.
Plant a garden or a pot from seed. Help me water it and watch it
grow. Pick flowers for my table and let me eat the vegetables.
Follow a routine at bedtime. Show me the clock and tell me it’s
time for bed. Let me pick out my bath toys, choose my pajamas,
read me a story, etc. Spend time with me. Sing me a song, rub my
back. Kiss me, say goodnight, I love you.
Give me permission to say no to adults that make me feel
uncomfortable. Talk with me and get to know how I’m feeling.
18
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
19
Developmental Concerns: By the end of 5 years
Normal physical development: Approximately 8-12 years
Alert your child’s doctor or nurse if your child displays any of the
following signs of possible developmental delay for this age range:
Average height: 45-58”, weight: 45-85 lbs.
Acts extremely fearful or timid
Acts extremely aggressively
Is unable to separate from parents without major protest
Is easily distracted and unable to concentrate on any single activity for
more than five minutes
Shows little interest in playing with other children
Refuses to respond to people in general, or responds only superficially
Rarely uses fantasy or imitation in play
Seems unhappy or sad much of the time
Doesn’t engage in a variety of activities
Avoids or seems aloof with other children and adults
Doesn’t express a wide range of emotions
Has trouble eating, sleeping or using the toilet
Can’t tell the difference between fantasy and reality
Seems unusually passive
Cannot understand two-part commands using prepositions (“Put the
doll on the bed, and get the ball under the couch.”)
Can’t correctly give her first and last name
Doesn’t use plurals or past tense properly when speaking
Doesn’t talk about her daily activities and experiences
Cannot build a tower of six to eight blocks
Seems uncomfortable holding a crayon
Has trouble taking off clothing
Cannot brush her teeth efficiently
Cannot wash and dry her hands
Experiences a dramatic loss of skills he or she once had
8-9 years
Play and imagination are still important developmental
tools
May enter puberty early
Very verbal and asks factual questions, may request
instruction
Social roles are better understood
School and neighborhood are important arenas for
growth
10-11 years
Girls may experience a growth spurt
Tolerates frustration better, good with time concepts, can
plan and understands cause and effect, more rational and
logical
Needs affection and affirmation from adults
Concrete thinking with a strong sense of fairness
Begin to see conflicts between peers and parent values
20
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
21
Activities that promote healthy growth: Approximately 8-12
years
Turn off the TV and play a game with me or talk things
over. Don’t let me watch PG-13 or R-rated movies.
Bake cookies with me. We can wear aprons and don’t get
too upset about how messy the kitchen becomes.
Teach me cards and board games I can play with my
friends.
Encourage outside play. (e.g., jump rope, skates, balls, etc.)
Draw a hopscotch grid on the sidewalk with chalk.
Teach me about nurturing by giving me responsibility for a
family pet. Understand I may forget and remind me.
I need to know how to swim to stay safe in water.
Teach me about nature through camping, hiking and going
to the zoo.
Let me organize a water fight with the hose and balloons.
Establish family traditions. Remind me about what we did
last year. Tell me why it is important.
Strategies for child safety: Approximately 8-12 years
22
Know where I am at all times. Teach me to check in and
give me timelines. Provide clear instructions to me about
what you believe is safe and supervise my activities.
Make my house safe, friendly and child centered. Children
can visit under your watchful eye.
Get to know the parents in my neighborhood and my
friend’s parents. Teach me to keep away from places that
are unsafe.
Give me permission to say “my mom or dad wants me
home” or “my mom won’t let me” if they need to make an
excuse to get out of an uncomfortable or pressure
situation.
Teach me about drugs, alcohol, smoking and teen
pregnancy. Let me tell you how I feel about these things.
Value me and teach me how to value and care for myself.
Teach me to be cautious of overly friendly adults or
strangers.
Ask me how I’m feeling. Listen and keep communication
open.
Be reliable and predictable and create a safe place for me
to put my trust. Forgive me when I fail and apologize
when you have let me down. Teach me about respect by
modeling it.
Teach me about my bright future and celebrate each
accomplishment along the way. Give me vision.
23
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Normal physical development: Approximately 13-18 years
Activities that promote healthy growth: Approximately 13-18
years
13-14 years
Challenges limit setting and parent’s judgment
Wants to be with peers more often
Puberty has begun or been achieved
Awkwardness and self-doubt may occur with new
growth
15-16 years
Girls full stature is achieved, boys may continue some
growth until age 18
Skills are developed and refined
Introspection and intense self-analysis
Conflict between parents grows, will push you away as
he or she attempts to take on more autonomy
Peers values become more important
Experimentation with social roles is expected
Boys may experience a growth spurt.
17-18 years
Hormonal and brain development continues
Interest in school increases or decreases
Youth relies more on peers for affection and approval
Individual identity forms, seeks independence
Parents and family are still important and necessary
Vision for the future and belief in self is essential
Be clear about what you expect of me. Set curfews and
know where I am at all times. Make sure I check in
frequently.
Start with small freedoms, assuring me that larger
freedoms will be allowed once I’ve proven myself capable
of the smaller ones.
Allow me to have my own music in my room.
Encourage me to express my feelings in writing and
verbally. It’s OK to be angry, not mean.
When I speak, listen to the feeling underneath along with
the words. Am I scared? Or hurting?
Peers are very important for me. Allow me to talk on the
phone and have friends over.
As much as you can, let me wear what I like as part of selfexpression.
Encourage volunteer or paid work. Instill responsibility
and polite public behaviors.
Support and encourage me to gain a special talent early in
my teen years (dance, music, drama, sports, art, etc.).
24
25
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Strategies for dealing with conflict: Approximately 13-18
years
Understand my need for developing a separate self and
do not take my struggles to gain independence
personally.
Understand that I still need supervision, guidance and
protection even if I push you away or am critical of you.
Troubled children often report a parent doesn’t “love
them enough” to wonder where they are or what they do.
Acknowledge my feelings and maintain consistent
consequences for my disobedience of clear limits you set.
Consequences should always be related to my
disobedience. (e.g., If an hour late, set the next curfew
time an hour earlier.)
Don’t give up - when I make mistakes, disobey or lose my
temper when you set limits, know that this is normal.
Reassure me that you still care and won’t give up on me.
Give me another chance. I want your love and approval
and will keep trying. Reassure me that you are still proud
of me.
Give me a vision for who I can become. Give me a reason
why I should make healthy positive choices.
Maintain communication and physical affection.
At Risk Adolescents
Typical adolescent behavior taken to the extreme -- more
moody, more hostile.
Defiance. Ignoring the rules. Violating curfew.
Totally uncommunicative to you or teachers. Only talks to
peers.
Sense of complete aimlessness or alienation.
Destructive eating habits. Eating disorders can be lifethreatening.
Missing money or greater expenditures.
Greater secrecy.
Drinking or other substance abuse
Factors that can increase risk
Undiagnosed learning disability. This child is subject to
constant personal frustration and criticism from others.
Discouragement and disaffection soon follow. It's never too
late for educational/psychological testing.
Unhappy family life
Family size
Traumatic illness in the family
Severe moodiness or depression
Isolated family
Friends that have destructive characters and behaviors
26
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
27
Northern California Training Academy
UC Davis Extension
University of California
1632 Da Vinci Court
Davis, CA 95616
Symptoms of PTSD (Post Traumatic Stress Disorder)
Play
Children begin to play out, draw, dramatize or tell their stories of
trauma.
Post-traumatic play is often grim, monotonous, and, at times,
dangerous. Connection between the play and the trauma is usually not
obvious.
For this reason, it often goes unnoticed as a symptom by caretakers.
The power to play is so strong that it impels the child to play.
Even adolescents, well beyond the age-range of the usual “pretend”
player, may play post-traumatically with art or music.
For this reason, some “acting out” behavior in adolescents is actually
post-traumatic play.
Symptoms in very young children
Ego-centric
Time Skew – Mis-sequencing trauma
Omen Formation – should have seen it coming
Bids for control
Symptoms in elementary school-aged children
Generalized fear – stranger or separation anxiety, avoidance of
situations or people associated with trauma
Sleep disturbance
Preoccupation with words
Post-traumatic play
Lost developmental skills
PTSD in Adolescents
May begin to look like adults
Traumatic reenactment
Telephone (530) 757-8643
Fax (530) 752-6910
e-mail academy@unexmail.ucdavis.edu
Web site http://www.humanservices.ucdavis.edu/academy/index.asp
From CARING FOR YOUR BABY AND YOUNG CHILD: BIRTH TO
AGE 5 by Steven Shelov, Robert E. Hannermann, © 1991, 1993, 1998,
2004 by the American Academy of Pediatrics. Used by permission of
Bantam Books, a division of Random House, Inc
28
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Trainee Content for Day 1, Segment 6A
The Role of Culture in Development
Culture can be viewed as a total system that regulates life within a particular group of
people. It consists of values, beliefs, attitudes, traditions, and standards of behavior. The
interplay and expression of these facets of culture exert a powerful influence on every
domain of development. Consequently, child development cannot be assessed without a
basic understanding of the cultural environment that surrounds and shapes a child’s
experiences.
In general:
Culture may set parameters or limitations on aspects of an individual’s development.
Culture creates context and expectations for human development.
Cultural preferences often result in some behaviors/traits being rewarded while others
are ignored. Those behaviors that are rewarded flourish; those that are ignored often
disappear.
Cultural expectations for developmental milestones may create situations that compel
the individual to meet the expectation, or restrain certain aspects of the individual’s
development.
The benefit of identifying cultural influences is to help determine when a child’s
developmental progress is considered normal or abnormal within the context of the
family’s culture. According to specific goals envisioned for children, different cultures
provide a variety of child rearing environments and obtain different behavioral outcomes.
Because cultures have different socialization practices, the behavior of infants, young
children and adolescents varies across cultures. In addition, what is viewed in one culture
as normal development, as well as the methods needed to achieve such development, may
be seen by another culture as strange, deficient or even pathological.
For example, the age at which a child learns to walk may depend on the parent’s cultural
beliefs about holding a child. If a child is constantly held or carried and not allowed to
explore before the age of 2, the child may not learn to walk by the typical age of 12-13
months. Given the cultural context, this would not be considered as “abnormal”
development.
Cultures typically have strong beliefs about male and female roles that significantly affect
the social and emotional development of children. Girls that are taught to speak only
when spoken to may learn not to initiate conversations with adults and consequently
develop a shy personality style. On the other hand, boys that are taught at a young age to
be independent, and afforded more opportunities to explore and interact with their
environment, may develop greater ease in social interactions.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Implications for Child Welfare Practice—Key Points
The purpose for understanding cultural influences is to help determine when different
developmental outcomes constitute delays or abnormal patterns of development,
thereby warranting casework intervention, and when cultural variations do not require
intervention.
When working with parents, it is important to consider:
In almost all cultures, the primary parental responsibilities are considered to be
protection of the young and transmission of the culture to the offspring.
Parents learn to parent as they were parented.
Cultural mores set the standards and expectations of a “good” parent and shape
parent-child interactions.
How to Learn More About a Family’s Culture
Consider the following questions that would be appropriate to include in an ethnographic
interview, and with each, consider the following:
1) How can this information help you understand the parent?
2) How can this information help you understand the child?
What is (are) the primary cultural group(s) with which the family identifies?
Does the family have strong social connections with other members of their culture?
What specific cultural values are important to the family?
Are there any cultural norms that may affect the children’s development?
What characteristics of individual family members influence the family’s
functioning?
For how many generations has this family lived in the United States?
Are there generational conflicts between parents and children resulting from a clash
between a family’s traditional culture and contemporary U.S. culture?
How much do prejudice, stigma, or immigration laws play a role in how well the
family is able to function?
How might services be tailored for this family to address their unique cultural needs?
Responses to these and other questions will help determine casework interventions and
whether they are needed at all.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Trainee Content for Day 2, Segment 19B
The Impact of Parental Substance Abuse on Children:
Specific Substances
Caution re: the use of substances by nursing mothers
Although the incidence of breastfeeding by substance-abusing mothers is generally low,
it is important to counsel nursing mothers that drugs of abuse are hazardous to them and
their infants. Overall, studies demonstrate the need for close follow-up and early
intervention for children born to substance-abusing women.
Opiates
Symptoms of neonatal opiate withdrawal are often present at birth but may not reach a
peak until 3 to 4 days or as late as 10 to 14 days after birth. Evidence of withdrawal from
opiates can persist in a sub-acute form for 4 to 6 months after birth. Common features of
the neonatal abstinence Syndrome mimic those of an adult's withdrawal from opiates. For
example, the opiate-exposed fetus may experience withdrawal in utero when drugs are
withdrawn from a dependent mother or after delivery when the mother’s use no longer
directly affects her newborn.
Cocaine
A major problem confronting pediatricians today arises from the consequences of
maternal cocaine use during pregnancy. As in other substance-abusing populations,
cocaine-dependent pregnant women have a high incidence of infectious diseases,
especially hepatitis B, acquired immunodeficiency syndrome, and other sexually
transmitted diseases. Although women who use cocaine may be at increased risk of
abruptio placentae, preterm labor and intrauterine growth retardation, they usually
experience an uncomplicated labor and delivery.
Cocaine-exposed infants have an increased incidence of premature birth, impaired fetal
growth and neonatal seizures, and Sudden Infant Death Syndrome (SIDS).Although a
specific cocaine withdrawal syndrome in neonates has not been defined, some show signs
of irritability and tremulousness, lethargy, inability to respond appropriately to
stimulation and abnormal cry patterns. Perinatal cerebral infarctions have occurred in
infants whose mothers have used cocaine a few days before delivery. These perinatal
cerebral infarctions exemplify the severe morbidity that may be associated with
intrauterine exposure to cocaine.
Marijuana
Withdrawal from other substances such as marijuana does not seem to be as severe.
Increased research is needed to define the degree of permanent residual effects in these
infants. In addition, interpretation of clinical studies is complicated by the fact that abuse
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
of multiple drugs often occurs.
However, several long-term studies have demonstrated that substance-exposed infants are
at risk for developmental and learning problems. In a group of 3- and 4-year-old children
exposed prenatally to marijuana, Fried and Watkinson found that, when controlling for
alcohol and tobacco exposure, by 4 years of age marijuana exposure was associated with
lower scores in the verbal and memory domains. The overall cognitive abilities of the
children were normal.
Effects of substance abuse on mother/baby/child
Effects on the mother
Poor judgment
Poor eating
Tolerance
Intoxication
CNS depression
Alcohol
Effects on the baby
Too small at birth
Brain damage
Heart problems
Kidney problems
Malformations
Changes in the face
Effects on children
Mental retardation
Behavior problems
Learning problems
Alcohol Related
Neurological Disorder
(ARND)
Fetal Alcohol
Syndrome (FAS)
Effects on the mother
Shortness of breath
Heart problems
Poor weight gain
Stroke or heart attack
Cigarettes
Effects on the baby
Too small at birth
Heart problems
Premature
Breathing problems
Crib death
Effects on children
Hyperactivity
Asthma and breathing
problems
Cocaine, Crack Cocaine
Effects on the mother
Effects on the baby Effects on children
Poor judgment
Too small at birth
Slow development
Poor eating
Brain damage
Behavior problems
Accidents
Premature
Learning problems
HIV/AIDS risk
Seizures
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Heart attack or stroke
Hepatitis
Drug withdrawal
Heart attack or stroke
inside the womb
Kidney problems
Malformations
Crib death
Amphetamines, Stimulants
Effects on the mother
Effects on the baby
Poor judgment
Too small at birth
Poor eating
Brain damage
Accidents
Premature
HIV/AIDS risk
Seizures
Heart attack or stroke
Heart attack or stroke
inside the womb
Hepatitis
Kidney problems
Malformations
Crib death
Effects on the mother
Poor judgment
Poor eating
Accidents
HIV/AIDS risk
Effects on the mother
Poor judgment
Poor eating
Accidents
Heroin, Opiates
Effects on the baby
Too small at birth
Small brain
Premature
Seizures
Drug withdrawal
Crib death
Oxycontin
Effects on the baby
Too small at birth
Small brain
Premature
Effects on children
Slow development
Behavior problems
Learning problems
Effects on children
Slow development
Behavior problems
Learning problems
Effects on children
Slow development
Behavior problems
Learning problems
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
HIV/AIDS risk
Effects on the mother
Poor judgment
Poor eating
Accidents
Disorientation
Seizures
Drug withdrawal
PCP, Angel Dust
Effects on the baby
Too small at birth
Brain damage
Premature
Seizures
Effects on children
Slow development
Behavior problems
Learning problems
Nervous system
problems
Shaky
Effects on the mother
Poor judgment
Accidents
Poor eating
Increased heart rate
Toxic to respiratory
system and immune
system
Marijuana
Effects on the baby
Too small at birth
Unknown risks to fetus
Effects on children
Learning problems
Behavior problems
Signs and symptoms of withdrawal in adults
Alcohol
Early symptoms of alcohol withdrawal generally appear 6 to 48 hours after drinking has
stopped but can occur up to 10 days after the last drink. Withdrawal symptoms may
include:
restlessness
tachycardia
irritability
hypertension
anorexia
insomnia
nausea
vomiting
impaired concentration
sweating
impaired memory
tremors
elevated vital signs
nightmares
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
More severe symptoms of alcohol withdrawal may include:
increased tremulousness
increased agitation
increased sweating
delusions (usually paranoid)
grand mal seizures
Hallucinations-auditory, visual, tactile
delirium (with confusion, disorientation, impaired memory& judgment)
Note: Withdrawal symptoms do not necessarily progress from mild to severe. In some individuals,
a grand mal seizure may be the first sign of withdrawal. Seizures usually occur 12 to 24 hours
after cessation or reduction of drinking. One-third of all patients who have seizures develop
delirium tremens.
Cocaine
Withdrawal from cocaine dependence is characterized by depression, anxiety and
lethargy, which begin to resolve after approximately one week. Less common are signs
of a paranoid psychosis during withdrawal from chronic use of high doses of cocaine. In
cocaine withdrawal, medication is rarely needed for the serious sequelae that are
associated with alcohol, barbiturate and opioid withdrawal.
Opioids
Mild withdrawal signs and symptoms include:
generalized anxiety
restlessness
opioid craving
lower back pain
slight aching of muscles, joints, and bones
Mild to moderate withdrawal signs and symptoms include:
tension
lethargy
yen sleep (mild insomnia) mydriasis (pupils dilated)
diaphoresis (usually perspiration)
Moderate withdrawal signs and symptoms include:
anorexia
rhinorrhea (runny nose)
rhinorrhea (runny nose)
nausea and/or stomach cramps
lower back pain
elevated pulse and blood pressure
lacrimation (tearing)
aching of muscles, joints, bones
goose flesh (earlier if client is in a cold, drafty room)
chills alternating with flushing and diaphoresis (sweating)
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Moderate to severe withdrawal signs and symptoms include:
diarrhea
vomiting
tremors
tachycardia (pulse over 100BPM)
increased respiratory rate & depth
Severe withdrawal signs and symptoms include:
kicking movements
doubling over w/stomach cramps
elevated temperature (usually low grade, less than 100 degrees F)
Note: Withdrawal signs and symptoms differ in their order of appearance from one individual to
another. Some individuals may not exhibit certain withdrawal signs and symptoms. Signs may
also include uterine irritability, increased fetal activity, or rarely, hypotension.
Barbiturates
Abstinence syndrome
The barbiturate abstinence syndrome begins 6 to 24 hours after the last dose, and
symptoms are generally more severe with short-acting barbiturates. Signs and symptoms
of barbiturate abstinence include:
tremulousness
diaphoresis
anxiety
postural hypotension
insomnia
agitation
anorexia
nausea and vomiting
delirium
tendon hyperreflexia
grand mal convulsions (between days 3 and 7)
Note: If untreated, withdrawal symptoms can progress to hyperpyrexia, electrolyte abnormalities,
cardiovascular collapse and death.
Early interventions for infants
Follow-up interventions include but are not limited to
nutrition
psychomotor assessment/monitoring of development
vision and hearing screening
speech and language assessment/therapy
emotional development assessments/therapy
play therapy
Intervention strategies for drug-exposed infants should promote:
self-regulation: the ability to regulate activity, attention, affect
secure relationships with mother and significant caregivers:
developmentally appropriate progress in motor skills, cognitive skills, speech and
language skills
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Early interventions for toddlers
Follow-up interventions include but are not limited to
Early childhood education program
Individual therapy
Strategies to support self-regulation
An orderly, consistent, child-appropriate environment
Predictable routines and consistent schedules
Clear expectations and rules
Clear patterns for transitions
Offering simple choices to children
Praising a child's efforts, not just successes
Using anticipatory guidance to avoid difficult situations
Operate from their strengths
Strategies to support secure relationships with caregivers
Individual attention, celebration of each person
Activities fostering positive self-esteem
Labeling feelings to assist the child with identifying feelings
Clear adult/child boundaries
Transition to the preschool period
Needed therapeutic services should be provided
speech and language
physical therapy
occupational therapy
play therapy
Teacher training
understand general addiction issues
understand women's addiction issues and family systems
understand cultural/ethnic factors
recognize behavioral cues to promote self-regulation
provide consistency, predictability, structure
plan for transitions
address issues relating to addiction, abuse and violence
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Trainee Content for Day 2, Segment 21A
Failure to Thrive
Failure to thrive (non-organic, NOFTT; also called psychosocial failure to thrive) is
defined as decelerated or arrested physical growth (height and weight measurements fall
below the fifth percentile, or a downward change in growth across two major growth
percentiles) associated with poor developmental and emotional functioning. Organic
failure to thrive is caused by medical complications of premature birth or other medical
illnesses that interfere with feeding and normal bonding activities between parents and
infants. Non-organic (psychosocial) failure to thrive occurs in a child who is usually
younger than age 2 and has no known medical condition that causes poor growth.
What causes non-organic failure to thrive?
Infants born into families with psychological, social, or economic problems are more at
risk of developing non-organic failure to thrive. NOFTT occurs when maladaptive
behaviors develop in both the infant and the primary caregiver. Maladaptive behaviors
may develop around problems establishing regular, calm feeding routines, problems of
attachment between the mother and the infant, and/or problems of separation. Other risk
factors that put a child at risk for developing non-organic failure to thrive include mother
or primary caregiver with any, or several, of the following conditions present:
depression
alcohol or drug abuse
psychosocial stress
lack of affection or warmth shown toward infant
lack of knowledge about proper feeding
lack of understanding of the infant's needs
Signs and symptoms
The following are the most common symptoms of failure to thrive. However, each child
may experience symptoms differently. Symptoms may include:
lack of appropriate weight gain
irritability
easily fatigued
excessive sleepiness
lack of age-appropriate social response (i.e., smile)
avoids eye contact
lack of molding to the mother's body
does not make vocal sounds
delayed motor development
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
The symptoms of failure to thrive may resemble other conditions or medical problems. A
doctor should always be consulted for a diagnosis. The individual issues involved in
causing NOFTT are almost always complex. Treatment planning usually requires the
involvement of a pediatrician, nutritionist, social worker, physical or occupational
therapist, and a psychiatrist or other qualified mental health provider.
The first year of life is an important time for brain growth. Children with NOFTT that are
not treated for an extended period of time may have difficulty “catching up”
developmentally and socially. About 50% of children who experienced failure to thrive
as an infant or young child continue to have social and emotional problems or eating
problems later in life.
Prevention of failure to thrive
NOFTT occurs because of social, emotional, economic, and interpersonal problems.
Community efforts to educate and encourage people to seek help for their problems may
help to reduce the incidence of NOFTT. Encouraging parenting education courses in high
school and educational and community programs may help new parents enter parenthood
with an increased knowledge of an infant's needs. Early detection and intervention can
reduce the severity of symptoms, enhance the process of normal growth and
development, and improve the quality of life experienced by infants and children.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Trainee Content for Day 2, Segment 20B
ADHD & Depression
Introduction
Many children have mental health problems that interfere with normal development and
functioning. In the U.S., 1 in 10 children and adolescents suffer from mental illness
severe enough to cause some level of impairment. However, in any given year, it is
estimated that less than 1 in 5 of these children receives needed treatment. Recent
evidence compiled by the World Health Organization indicates that by the year 2020,
childhood neuropsychiatric disorders will rise proportionately by over 50%
internationally, to become one of the five most common causes of morbidity, mortality,
and disability among children.
Attention Deficit Hyperactivity Disorder (ADHD)
Attention Deficit Hyperactivity Disorder (ADHD) is a condition that becomes apparent in
some children in the preschool and early school years. It is hard for these children to
control their behavior and/or pay attention. It is estimated that between 3 and 5% of
children have ADHD, or approximately 2 million children in the United States. This
means that in a classroom of 25 to 30 children, it is likely that at least one will have
ADHD.
Symptoms and types
The principal characteristics of ADHD are inattention, hyperactivity, and impulsivity.
These symptoms appear early in a child’s life. Because many normal children may have
these symptoms, but at a low level, or the symptoms may be caused by another disorder,
it is important that the child receive a thorough examination and appropriate diagnosis by
a well-qualified professional. There are three main types of ADHD. One type is
characterized by inattentiveness; one type is characterized by hyperactive or impulsive
behavior. The third type is combined, when children exhibit signs of both inattentiveness
and hyperactivity.
Some signs of hyperactivity-impulsivity are:
Fidgeting excessively
Difficulty staying seated
Running or climbing inappropriately
Talking excessively
Difficulty playing quietly
Always seeming to be “on the go”
Blurting out answers or frequently interrupting
Having trouble waiting his or her turn
Interrupting or intruding on others
Some signs of inattentive behavior are:
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Difficulty following instructions
Difficulty focusing on tasks
Losing things at school and at home
Forgetting things often
Becoming easily distracted or having difficulty listening
Lacking attention to detail, making careless mistakes or being disorganized
Failing to complete homework or tasks
The presence of some symptoms, however, does not confirm a diagnosis of ADHD. Just
because a child has a lot of energy or difficulty paying attention in school does not mean
the child has ADHD. An accurate diagnosis relies on the presence of a range of
symptoms and difficulties that prevent the child from performing at an appropriate level
for his or her age and intelligence level. Symptoms may go unnoticed until a child enters
school. Teachers are often first to observe these issues, and their input should be
considered seriously.
Is it really ADHD?
The child’s pattern of behavior is compared against a set of criteria and characteristics of
the disorder as listed in the DSM-IV-R. To be diagnosed with ADHD, a child must show
symptoms in at least two settings, such as home and school, and the symptoms must
interfere with the child’s ability to function at home or school for at least six months.
Critical questions include: Are these behaviors excessive, long-term, and pervasive? That
is, do they occur more often than in other children the same age? Are they a continuous
problem, not just a response to a temporary situation? Specialists have agreed that at least
six symptoms from the previous lists must be present for an accurate diagnosis, and
symptoms must begin by age 7.
Seeking help
Parents and other caregivers play a crucial role in ensuring that children receive the care
that they need. Children with symptoms of ADHD should be referred to and evaluated
by a mental health professional that specializes in treating children, or a primary care
doctor who has experience in treating this disorder. The diagnostic evaluation should
include behavioral observation in the classroom and at home. A comprehensive
treatment plan should be developed with the family, and, whenever possible, the child
should be involved in making treatment decisions. Educational testing should be
performed when learning disabilities are present.
A variety of professionals may be helpful:
Specialty
Can diagnose
ADHD
Can prescribe
medication, if needed
Can provide
counseling or training
Psychiatrists
Yes
Yes
Yes
Psychologists
Yes
No
Yes
Pediatricians or
Family Physicians
Yes
Yes
No
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Neurologists
Yes
Yes
No
Clinical Social
Workers
Yes
No
Yes
Licensed Marriage
and Family
Therapists
Yes
No
Yes
What causes ADHD?
ADHD is nobody’s fault. Researchers believe that biology plays a large role in the
development of ADHD. 30 to 40% of children diagnosed with ADHD have relatives with
the same disorder, suggesting that genes are at least partly responsible. Brain scans reveal
that the brains of children with ADHD differ from those of children without the
disorder. Children with ADHD are thought to have problems with the part of the brain
that controls the organization and direction of thought and behavior.
How does ADHD affect school and social life?
Symptoms of ADHD such as trouble sitting still, paying attention to details, and listening
can make school difficult for a child with ADHD. Although most children with ADHD
have normal or above-normal intelligence, 40 to 60% have serious learning difficulties.
Many others have specific problems with schoolwork or maintaining good grades, and
face particular challenges with assignments and tests that require focused attention,
lengthy writing, or have time limits. On a social level, children with ADHD often have
trouble developing meaningful relationships with peers and family members. Other
children may find it frustrating to play with a child who has ADHD, because of classic
symptoms such as difficulty following rules, waiting one’s turn, or excessive talking.
Disorders that sometimes accompany ADHD
Children and adolescents with ADHD are more likely than children without the disorder
to suffer from other mental disorders. About one-half of all young people with ADHD
have oppositional defiant disorder; about one-quarter have an anxiety disorder; and as
many as one-third have depression and one-fifth have bipolar disorder. Adolescents with
untreated ADHD are at risk for substance abuse disorders. Research shows that young
people treated for ADHD have lower rates of substance abuse than children who go
untreated.
Learning disabilities
Many children with ADHD, approximately 20 to 30%, also have a specific learning
disability. In preschool years, these disabilities include difficulty in understanding
certain sounds or words and/or difficulty in expressing oneself in words. In school age
children, reading or spelling disabilities, writing disorders, and arithmetic disorders may
appear. Dyslexia, a reading disorder, is quite widespread. Reading disabilities affect up to
5% of elementary school children.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Tourette’s syndrome
A very small proportion of people with ADHD have a neurological disorder called
Tourette’s syndrome. People with Tourette’s syndrome have various nervous tics and
repetitive mannerisms, such as eye blinks, facial twitches, or grimacing. Others may clear
their throats frequently, snort, sniff, or bark out words. These behaviors can be controlled
with medication. While very few children have this syndrome, many cases of Tourette’s
syndrome have been associated ADHD.
Oppositional defiant disorder
As many as one-third to one-half of all children with ADHD, mostly boys, have another
condition, known as oppositional defiant disorder (ODD). These children are often
defiant, stubborn, and non-compliant. They are likely to have outbursts of temper, or
become belligerent. They argue with adults and refuse to obey.
Conduct disorder
About 20 to 40% of ADHD children may eventually develop a more serious pattern of
antisocial behavior known as a conduct disorder (CD). These children frequently lie or
steal, fight with or bully others. They are at risk of getting into trouble at school or with
the police. They are aggressive toward people and/or animals, destroy property, commit
thefts, carry or use weapons, or engage in vandalism. These children or teens are at
greater risk for substance use experimentation, and later dependence and abuse. They
need immediate help.
Anxiety and depression
Some children with ADHD have co-occurring anxiety or depression. If the anxiety or
depression is recognized and treated, the child will be better able to handle the problems
that accompany ADHD. Conversely, effective treatment of ADHD can have a positive
impact on anxiety as the child is better able to master academic tasks.
Bipolar disorder
There are no accurate statistics on how many children with ADHD also have bipolar
disorder. Differentiating between ADHD and bipolar disorder in childhood can be
difficult. In its classic form, bipolar disorder is characterized by mood cycling between
periods of intense highs and lows. But in children, bipolar disorder often seems to be a
rather chronic mood dysregulation with a mixture of elation, depression, and irritability.
There are some symptoms that can be present both in ADHD and bipolar disorder, such
as a high level of energy and a reduced need for sleep. For differentiating children with
ADHD from those with bipolar disorder, elated mood and grandiosity are distinguishing
characteristics for bipolar disorder.
The treatment of ADHD
Early identification, diagnosis and treatment help children reach their full potential. The
most effective treatments for ADHD include a combination of medication, behavioral
therapy, and parental support and education. Nine out of ten children respond to
medication, and 50% of children who do not respond to an initial medication will respond
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
to a second. When ADHD co-occurs with another disorder, such as depression or anxiety,
a combination of medication and psychotherapy is shown to be particularly effective.
Medications
For decades, medications have been used to treat the symptoms of ADHD. The
medications that seem to be the most effective are a class of drugs known as stimulants.
Following is a list of the stimulants indicating their generic names, their trade (or brand)
names, and approved age. “Approved age” means that the drug has been tested and found
safe and effective in children of that age.
Generic name
Trade name
Approved age
Amphetamine
Adderall
3 and older
Dextroamphetamine
Dextrostat, Dexedrine
3 and older
Dexmethylphenidate
Focalin
6 and older
Methylphenidate
Ritalin
6 and older
methylphenidate
(extended release)
Metadate ER, Metadate CD,
Ritalin SR
6 and older
methylphenidate
(long acting)
Ritalin LA, Concerta
6 and older
Pemoline
Cylert*
6 and older
*Because of its potential for serious side effects affecting the liver, Cylert should not ordinarily
be considered as first-line drug therapy for ADHD.
The U.S. Food and Drug Administration (FDA) recently approved a medication for
ADHD that is not a stimulant. The medication, Strattera®, or atomoxetine, works on the
neurotransmitter norepinephrine, whereas the stimulants primarily work on dopamine.
Both of theses neurotransmitters are believed to play a role in ADHD. More studies will
need to be done to contrast Strattera with the medications already available, but the
evidence to date indicates that over 70% of ADHD children given Strattera manifest
significant improvement in their symptoms.
The stimulant drugs come in long- and short-term forms. The newer sustained-release
stimulants can be taken before school and are long-lasting so that the child does not need
to go to the school nurse every day for a pill. Doctors can discuss with parents the child's
needs, decide which preparation to use, and whether the child needs to take the medicine
during school hours only or in the evening and on weekends too.
Side effects of the medications
Most side effects of the stimulant medications are minor and are usually related to the
dosage of the medication being taken. Higher doses produce more side effects. The most
common side effects are decreased appetite, insomnia, increased anxiety, and/or
irritability. Some children report mild stomachaches or headaches.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
The stimulant drugs, when used with medical supervision, are usually considered quite
safe. Stimulants do not make the child feel “high,” although some children say they feel
different or funny. Such changes are usually minor. Although some parents worry that
their child may become addicted to the medication, to date there is no convincing
evidence that stimulant medications used for treatment of ADHD cause drug abuse or
dependence. A review of all long-term studies on stimulant medication and substance
abuse, conducted by researchers at Massachusetts General Hospital and Harvard Medical
School, found that teenagers with ADHD who remained on their medication during the
teen years had a lower likelihood of substance use or abuse than did ADHD adolescents
who were not taking medications.
Facts to remember about medication for ADHD
Medications for ADHD help many children focus and be more successful at school,
home, and play. Avoiding negative experiences now may actually help prevent
addictions and other emotional problems later.
About 80% of children who need medication for ADHD still need it as teenagers.
Over 50% need medication as adults.
As with other mental health issues, it is important that practitioners keep abreast of
current research on ADHD.
Depression
No one thing causes depression. Children who develop depression may have a family
history of the disorder. Family history, stressful life events such as losing a parent,
divorce, or discrimination, and other physical or psychological problems are all factors
that contribute to the onset of the disorder. Children who experience abuse, neglect, or
other trauma or who have a chronic illness are at a higher risk for depression. Depression
in children often occurs along with other mental health problems such as anxiety, bipolar,
or disruptive behavior disorders.
Depression can lead to academic underachievement, social isolation, and create difficult
relationships with family and friends. Depression in children is also associated with an
increased risk for suicide. In fact, the U.S. Surgeon General estimates that more than
90% of children and adolescents who take their lives have a mental health disorder such
as depression. The rate of suicide among young people has nearly tripled since 1960.
Adolescents who become clinically depressed are also at a higher risk for substance
abuse problems. They will use alcohol and drugs as a way to numb or manage their pain.
Any child or adolescent who abuses substances should be evaluated for depression. If an
addiction develops, it is essential to treat both the mental health disorder and the
substance abuse problem at the same time.
Once a young person has experienced an episode of depression, he or she is at an
increased risk for having another episode of depression within the next five years.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
Children who experience a depressive episode are five times more likely to have
depression as an adult.
What are the signs and symptoms?
The list below outlines possible signs of depression. If a child is struggling with any
combination of these symptoms for more than two weeks, a doctor or mental health
professional should be consulted.
Frequent sadness, tearfulness, or crying
Feelings of hopelessness
Withdrawal from friends and activities
Lack of enthusiasm or motivation
Decreased energy level
Major changes in eating or sleeping habits
Increased irritability, agitation, anger or hostility
Frequent physical complaints such as headaches and stomachaches
Indecision or inability to concentrate
Feelings of worthlessness or excessive guilt
Extreme sensitivity to rejection or failure
Pattern of dark images in drawings or paintings
Play that involves excessive aggression directed toward oneself or others, or involves
persistently sad themes
Recurring thoughts or talk of death, suicide, or self-destructive behavior
Risk factors
In childhood, boys and girls appear to be at equal risk for depressive disorders, but during
adolescence, girls are twice as likely as boys to develop depression. Children who
develop major depression are more likely than patients with adolescent- or adult-onset
depression to have a family history of the disorder, often a parent who experienced
depression at an early age. Adolescents with depression are also likely to have a family
history of depression though the correlation is not as high as it is for children.
Other risk factors include
Stress
Cigarette smoking
A loss of a parent or loved one
Break-up of a romantic relationship
Attention, conduct or learning disorders
Chronic illnesses, such as diabetes
Abuse or neglect
Other trauma including natural disasters
The depressed child
The first step in helping the depressed child is to recognize the depression. This can be
challenging. It is difficult for adults to accept that young children, even infants, can suffer
from depression. Childhood is supposed to be a happy, carefree time of life. Only in
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
recent years has scientific evidence convinced most mental health specialists that
childhood depression exists.
Recognizing the symptoms of childhood depression can also be difficult. While some
children display the classic symptoms (sadness, anxiety, restlessness, eating and sleeping
problems), others express their depression through physical problems (various aches and
pains) that do not respond to treatment. Still others hide their feelings of hopelessness
and worthlessness under a cover of irritability, aggression, hyperactivity, and
misbehavior.
Complicating the recognition of depression are the developmental stages that children
pass through on the way to adulthood. Negativism, clinginess or rebellion may be normal
and temporary expressions of a particular stage. In addition, children go through
temporary depressed moods just as adults do. Careful observation of a child for several
weeks may be required to determine if there is a problem. When symptoms of possible
depression seem severe or continue for more than a few weeks, an evaluation by the
child's pediatrician to rule out a physical illness would be a good first step. A next step,
if deemed necessary, would be consultation with a mental health professional that
specializes in treating children. While parents typically assume prime responsibility for
getting treatment for their depressed child, other people such as relatives, teachers, and
friends can play a role.
Treatment
An evaluation for depression may include consultation with a child psychiatrist,
psychological testing, and medical tests to rule out an underlying physical condition that
might explain the child’s symptoms. A comprehensive treatment plan should include
psychotherapy and, in some cases, medication. Selective Serotonin Reuptake Inhibitors
(SSRIs) such as Prozac, Paxil, and Zoloft have been shown to be more effective with
children. Studies do not support the use of tricyclic antidepressants (Elavil, Imipramine,
etc.) in youth. However, Imipramine is sometimes used to treat enuresis (bed-wetting)
because it improves the functioning of the smooth muscle of the bladder. A plan to treat
depression should be developed with the family, and, whenever possible, the child should
be involved in making treatment decisions.
Common Core | Child & Youth Development | Trainee’s Guide | Version 1.0, June 2007
CHILD MALTREATMENT IDENTIFICATION
PART 1: NEGLECT, EMOTIONAL ABUSE, & PHYSICAL ABUSE
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
The trainee will accurately identify factors that constitute abuse and/or neglect as defined
by the Welfare & Institutions Code Section 300 (a) - (j) and recognize parenting
behaviors that promote child safety and family well-being outcomes.
The trainee will distinguish scenarios of child maltreatment from those that are not child
maltreatment based on a constellation of factors such as physical injuries and behavioral
indicators, within a cultural context.
The trainee will value the importance of diversity as it relates to child maltreatment.
LEARNING OBJECTIVES
Knowledge:
K1. The trainee will be able to identify indicators of physical abuse.
K2.
The trainee will be able to identify indicators of neglect.
K3.
The trainee will be able to identify indicators of emotional abuse.
K4.
The trainee will understand the legal basis of identifying abuse and neglect in
California, and understands the associated sections of the Welfare & Institutions
Code Section 300 (a) - (j).
K5.
The trainee will be able to identify strength-based information gathering strategies
(that include exploration of family strengths, resources, and risk and safety
factors) necessary for working with children, families, and others in the context of
making a child maltreatment determination.
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
K6.
The trainee will be able to identify physical, emotional, and behavioral
characteristics of children who have been maltreated, while attending to the
cultural and ethnic context of the children.
K7.
The trainee will be able to identify three cultural practices that may be mistaken
for child maltreatment.
Skills:
S1.
Given a case scenario, the trainee can identify child maltreatment.
S2.
Given a case scenario, the trainee will be able to distinguish child maltreatment
from benign cultural factors.
Values:
V1.
The trainee will be aware of their personal values related to abuse and neglect as
they relate to the legal definitions described in the Penal Code and the Welfare &
Institutions Code Section 300 (a) - (j).
V2.
The trainee will make decisions consistent with the legal definition as described in
the Penal Code and Welfare & Institutions Code Section 300 (a) - (j).
V3.
The trainee will value the benefit of acquiring and utilizing up-to-date information
about cultural differences to identify child maltreatment.
V4.
The trainee will value the importance of working with families and communities
utilizing a strength-based model of practice.
RELATED TITLE IV-E CURRICULUM COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student understands the influence and value of traditional, culturally based childrearing
practices and uses this knowledge in working with families. (1.4)
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Student is able to identify the multiple family and social forces contributing to child
abuse and neglect. (2.1)
Student recognizes and accurately identifies physical, emotional, and behavioral
indicators of child abuse, child neglect, and child sexual abuse in children and their
families. (2.3)
Student is aware of forms and mechanisms of oppression and discrimination pertaining to
low-income and single-parent families and uses this knowledge in providing appropriate
child welfare services. (2.5)
Student understands the policy issues and child welfare legal requirements and
demonstrates the capacity to fulfill these requirements in practice. (2.10)
Student demonstrates the ability to assess his or her own emotional responses to clients,
co-workers, and situations in which the worker’s values are challenged. (2.17)
Student demonstrates understanding of the potential effects of poverty, racism, sexism,
homophobia, violence, and other forms of oppression on human behavior. (3.3)
Student demonstrates understanding of the influence of culture on human behavior and
family dynamics. (3.4)
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
CHILD MALTREATMENT I NEGLECT,
DATE
PHYSICAL ABUSE AND EMOTIONAL ABUSE COMPLETED
1. Locate the W&I Code book in your office. What does
it say about a parent’s right to spank their child? What
does your County’s manual of policies and procedures
say regarding the parent’s right to spank their child?
Have a discussion about your personal value on
spanking. How do you think your value may impact
the decisions you make on the job?
2. Attend a multi-disciplinary case consultation on a
physical abuse case. Have a discussion about what
you learned and how you will use this knowledge on
the job and/or specific to one of your cases.
3. Locate and have a discussion about your Agency’s
policy on SW’s doing body checks of children, taking
pictures of children and the use of medical experts.
4. Review your Agency’s protocols on doing physical
abuse investigations and neglect investigations.
5. Review the handout in the SW CORE binder titled
Partners in Identifying and Assessing Child
Maltreatment. Using one of your cases, identify which
of these partners have or will be consulted. What
valuable information did/may you get from them?
6. Locate and review your Agency’s policy on children
born with a positive toxicology. Have a discussion on
whether you agree or disagree and how your opinion
may influence the work you do on the job.
7. Either using some of your own cases, or cases known
by your supervisor, have a discussion about 3 known
cultural practices that may be mistaken for child
maltreatment.
8. Review the handout in the SW CORE binder titled
Possible Indicators of Child Neglect. Using one of
your cases, where neglect is the issue, identify which
of these indicators were/are present.
9. Review the handout in the SW CORE binder titled
Elements to Consider in Identifying Physical Abuse.
Using one of your own cases, where physical abuse is
the issue, identify which of these elements were/are
present.
10. Review the handout in the SW CORE manual titled
Indicators of Emotional Abuse. Using one of your
cases, where emotional abuse is an issue, identify
which of these elements were/are present.
Trainee Content for Day 1, Segment 3, Activity 3A
Partners in Identifying and Assessing Child Maltreatment
The Family
In a child abuse investigation, family members will be interviewed as part of the
investigation. For example, depending on your county policy, the family may be brought
in early as part of a Team Decision-Making meeting. Note to trainees: The family does
not participate in the decision as to whether or not the allegation under investigation
is substantiated, indicated, or unfounded.
In the past, families (including fictive kin, extended family members, close family
friends) involved in the Child Welfare System were often excluded from the decisionmaking process that affected the care and custody of their children. More and more, in
California and beyond, families are being included in collaborative efforts to reach
decisions. It has been recognized that by doing so, more effective outcomes occur and
families “own” decisions when they have been a part of making them.
The Community
The society in which we live sets the moral tone, culture, and standards of the
community. Communities support children being cared for properly. Children are best
raised in families. Communities have resources and supports to help families better care
for their children.
Child Welfare Workers/Child Welfare System
Child welfare workers make the home calls and act as “eyes and ears for the court.”
They interpret the W&I Code and offer crisis intervention, counseling, and resources to
families in which maltreatment has occurred or who have been reported as having
possibly been at risk for the occurrence of maltreatment. They utilize a professional body
of ethics, knowledge of family dynamics, human and child development, social work,
risk assessment, child maltreatment, assessment and case planning skills, and case
management to protect children, strengthen families, and provide a child welfare related
spectrum of services.
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Medical System
The medical system offers the scientific explanation for abuse versus accidents, but
cannot do it in isolation. An accurate history and assessment of family functioning and
interaction is vital to the process of accurate diagnosis of child abuse and child welfare
workers can assist in obtaining that information. Medical assessment and evidence is
critical in making accurate determinations if maltreatment has occurred, which the child
welfare system cannot accomplish without the involvement of child abuse experts and the
medical profession.
Mental Health System/Victim Witness Advocates:
Depending on the facts of the case, these individuals can also add their expertise or
knowledge to the collaborative process.
Law Enforcement
Law enforcement is charged with enforcing the laws which have been passed by Federal,
State, and local governing bodies, such as the California Penal Code. Law enforcement is
responsible for investigating all allegations of child abuse and severe neglect, to
determine, through investigation, if a violation of criminal law has occurred, to collect
evidence, interview victims and potential witnesses, apprehend the offender/s, and file
appropriate criminal charges. In child maltreatment cases, the preferred method for
accomplishing these tasks is through coordination with multidisciplinary child abuse
investigation teams.
Legislative/Legal/Judicial System
Legislators make the laws; they interpret the changing societal/cultural norms and mores.
Laws give child welfare workers and law enforcement the legal basis for their authority
to intervene in the lives of children and their families. Law enforcement prosecutes
crimes, versus the child welfare system that protects children, but the two systems work
together. Law enforcement investigates child maltreatment. Child welfare assesses if
children need protection and if families need services to better care for their children.
Courts oversee and carry out the protective and prosecution aspects of child welfare cases
and ensure the rights of both children and parents are protected.
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Possible Indicators of Child Neglect
Children unattended, left alone, lack of supervision, playing with matches, house fires
Child sleepy, dirty, hungry, poorly clothed for weather (often question of degree,
chronicity)
Lice, scabies, chronic poor hygiene
Child depressed/withdrawn/fearful
Child rocks, self-comforts, clingy
Child antisocial, destructive, acts out (may also indicate physical abuse)
Child uses drugs, gang membership
Child is frequently injured (can also be abuse)
Child hit by car, found wandering in street
Child left in car, especially risky in hot weather
Filthy home
Unsafe home, hazards
No/Insufficient food in home
Failure to obtain medical/psychological treatment which results in pain/detriment
Chronic truancy/tardiness
“Bottle rot”, dental neglect
Flat back of head
Child thin, begging for food, dehydrated, malnourished
Non-organic failure to thrive
Child drowning (or near-drowning) in pool, tub, pond, etc.
Child tests positive for drugs, legal or illegal
- Positive toxicology screen at birth
- Older child ingests drugs left out
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Trainee Content for Day 1, Segment 8, Activity 8A
Elements to Consider in Identifying Physical Abuse
(Short Version)
In order to carry out effective child abuse assessments and investigations, the following
framework will assist child welfare workers. By carefully considering each element,
child welfare workers will be much more capable of reaching the determination of
whether child maltreatment has occurred. The elements to consider in evaluating
physical abuse are:
Location/Scene of Incident
Location of Injury on the Body
Type(s) of Injury
Severity/Extent of Current Injury/Injuries
Frequency of Injuries over Time
Explanation of Injury
Child’s Overall Appearance
Chronological Age of Child
Developmental Abilities of Child
History of Unreported Maltreatment of these children by any caregivers, or history of
unreported maltreatment by these caregivers toward any children
History of CWS Involvement – with these children or with these caregivers
Parent’s/Caregiver’s Own History of Maltreatment
Parent/Caregiver Substance Abuse
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Trainee Content for Day 1, Segment 6, Activity 6A
Indicators of Emotional Abuse
This destructive behavior includes, but is not limited to:
Assaults (Verbal)
The adult engages in (including, but is not limited to):
Name calling of the child
Profanity about the child
Threatens the child
Belittles the child
Cinderella Syndrome or Scapegoat
The adult singles out one child to criticize, punish, and/or do work.
Confusion
The adult confuses the child’s sexual identity by dressing the child as the opposite gender
and not allowing normal gender identity to develop.
Corruption
The adult “mis-socializes” the child by:
Stimulating the child to engage in destructive antisocial behavior,
Reinforcing that deviance, and
Making the child unfit for constructive social experience.
Domestic Violence (Exposure to)
Children exposed to violence are likely to suffer emotional damage (National
Clearinghouse on Child Abuse and Neglect, 2000).
“Double Binds”
The adult puts the child in a “no win” situation: whatever the child does or chooses is
going to be “wrong.”
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
Humiliation
The adult performs acts that result in extreme embarrassment and feelings of humiliation
for the child.
Ignoring and/or Depriving
The adult deprives the child of essential stimulation and responsiveness, stifling
emotional growth and intellectual development. This may include depriving the child of
books or toys, which also impacts emotional and intellectual growth, and results in
psychic pain.
Isolation
The adult:
Cuts the child off from constructive experiences
Prevents the child from forming friendships
Makes the child believe he or she is alone in the world
Rejection
The adult:
Refuses to acknowledge the child’s worth
Refuses to acknowledge the legitimacy of the child’s needs
Shows overt rejection (pushes the child away)
Dismisses the child’s comments, ideas, or needs.
Terrorizing
The adult:
Verbally assaults the child
Creates a climate of fear for the child
Bullies or frightens the child
Makes the child believe that the world is capricious and hostile.
Unpredictability (Parental)
Most situations, even when unjust and painful, are easier to deal with if their occurrence
is logical and predictable. However, when emotional or physical trauma is capricious and
unpredictable, a constant and extreme degree of anxiety and apprehension can exist.
Unrealistic Expectations
The adult is scolding, yelling, and demeaning when the child displays developmentally
appropriate behavior. Alternatively, the adult scolds, yells, or demeans the child, based
on behavior the child is not yet capable of.
Common Core | Child Maltreatment Identification, Part 1: Trainee’s Guide | Version 1.25, January 2009
CHILD MALTREATMENT IDENTIFICATION
PART 2: SEXUAL ABUSE AND EXPLOITATION
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
Knowledge
The trainee will accurately identify conduct that may constitute sexual abuse and
exploitation, as defined by the Penal Code and referenced in the Welfare and Institutions
Code.
Skills
The trainee will distinguish scenarios of sexual abuse from those that are not sexual
abuse, taking into account the physical, emotional, and behavioral indicators of child
sexual abuse in child victims and their families.
Values
The trainee will incorporate a sensitivity to the cultural landscape when engaged in
identifying and assessing sexual abuse and exploitation.
LEARNING OBJECTIVES
Knowledge
K1.
The trainee will know the physical, behavioral and emotional indicators and
effects of child sexual abuse.
K2.
The trainee will understand that in some cases there are no identifiable physical,
behavioral, and emotional indicators of child sexual abuse.
K3.
The trainee will understand the legal basis of identifying sexual abuse and
exploitation under California law, specifically as defined by the Penal Code and
as referenced in the Welfare and Institutions Code.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
K4.
The trainee will understand the family dynamics vis-à-vis a child victim, a nonoffending parent, the offender, and the significance of these dynamics in
identifying sexual abuse and exploitation.
K5.
In an assessment, the trainee will recognize effective engagement strategies that
elicit family strengths and protective capacities, as well as risk and safety factors.
K6.
The trainee will recognize the difference between therapeutic/supportive
interviewing techniques and legally acceptable forensic interviewing techniques.
K7.
The trainee will recognize the factors that may mitigate the short- and long-term
effects of child sexual abuse.
Skills
S1.
Given a case scenario, the trainee will recognize and accurately identify physical,
emotional, and behavioral indicators of child sexual abuse and exploitation in
child victims and their families.
S2.
Given a case example, the trainee will recognize cultural and familial factors that
may impact assessment and intervention in child sexual abuse.
Values
V1.
The trainee will be aware of their personal values and biases related to sexuality,
and how they may or may not affect the assessment.
V2.
The trainee will be aware of their personal values and biases related to child
sexual abuse and exploitation, and how they may or may not affect the
assessment.
V3.
The trainee will value the benefit of acquiring and utilizing up-to-date information
in assessing sexual abuse and exploitation.
V4.
The trainee will value the importance of working with culturally diverse families
and communities utilizing a strength-based model of practice in assessing sexual
abuse and exploitation.
V5.
The trainee will value the difference between therapeutic/supportive interviewing
techniques and legally acceptable forensic interviewing techniques.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
TITLE IV-E CURRICULUM COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student understands the influence and value of traditional, culturally based child rearing
practices and uses this knowledge in working with families. (1.4)
Student demonstrates the ability to assess the interaction of factors underlying abuse and
neglect and capacity to identify strengths that act to preserve the family and protect the
child. (2.2)
Student recognizes and accurately identifies physical, emotional, and behavioral
indicators of child abuse, child neglect, and child sexual abuse in children and their
families. (2.3)
Student understands the policy issues and child welfare legal requirements and
demonstrates the capacity to fulfill these requirements in practice. (2.10)
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
CHILD MALTREATMENT IDENTIFICATION
DATE COMPLETED
PART 2: SEXUAL ABUSE AND EXPLOITATION
1. Review the handout in the trainee binder titled
Indicators of Sexual Abuse: Elements used to Identify
Child Sexual Abuse and Exploitation. Note the
physical, emotional and behavioral indicators of child
victims and their families. Using one of your cases, if
possible, what current or past indicators are/were
present?
2. Review the handout in the trainee binder titled Child
Rearing Standards and child Sexual Abuse in a
Cultural Context. Using one of your cases, if possible,
have a discussion about the cultural factors that may
impact assessment and intervention strategies.
3. Review the handout in the trainee binder titled
Personal Difficulties in Dealing with Sexuality and
Victimization. Have a discussion about your personal
values and bias related to child sexual abuse and
exploitation and how they may or may not affect
assessment and case planning.
4. Have a discussion about how cases of sexual abuse are
handled in your county. What special measures are
taken during the sexual abuse investigation, such as
forensic interviewing, special sex unit, etc?
5. Review the 3 handouts in the trainee binder titled,
Child Disclosures, Reluctance to Disclose, The NonOffending Parent/Caregiver and Myths & Research
about Sexual Offenders. Have a discussion about the
family dynamics in one of your sexual abuse cases, if
possible. Are/were the dynamics in your case
significant in identifying sexual abuse or exploitation?
6. Review the handout in the trainee binder titled
Treatment Issues. While there is no available
“formula” to determine whether and how long children
should be in treatment, every child and teenager who
is a victim of sexual abuse should be assessed by a
qualified professional to determine their mental health
status and needs. Using one of your sexual abuse
cases, if possible, have a discussion about the
assessment for treatment, treatment provided and
outcome of treatment. In general, what services are
available, in your county, for sexual abuse victims and
their families?
Trainee Content for Day 1, Segment 6
Indicators of Sexual Abuse:
Elements Used to Identify Child Sexual Abuse and Exploitation
This section of the curriculum outlines the elements that are examined to determine
whether sexual abuse has occurred. Many of these elements are often referred to as
indicators of child sexual abuse. The elements are divided into four broad categories:
Reporting (including aspects of the allegation and disclosure);
Physical (including medical indicators);
Behavioral (including emotional indicators for the victim); and
Familial (including family and caretaker dynamics).
Reporting Elements
Several elements must be considered that relate to the reporting of the allegation,
including the circumstances of the disclosure of the sexual abuse by the child or another
person.
1. Credibility of the report (and the reporter)
This element includes looking at a report and who reported it, and determining whether
the report is credible.
Social workers should consider the clarity of the report, including whether the
reporter had direct knowledge of the incident, or whether they are able to provide
specific information as to time, place, etc.
When evaluating a report of sexual abuse, the social worker should consider if there
is some advantage to an involved party related to the sexual abuse allegation. This is
most common in cases when sexual abuse allegations arise in the context of a divorce
and custody dispute.
Consider the reporter’s motive for reporting. For example, a school social worker or
teacher might be perceived as credible while a parent engaged in a custody battle
might be much less so. More credible reporters may include medical personnel,
school staff, and mental health professionals.
The alleged perpetrator or the non-offending parent may, individually or together,
attempt to undermine the credibility of the reporter or the credibility of the child’s
report. For example, they may attack the reporter and say the reporter has a vendetta
against the perpetrator.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
2. Type and credibility of the child’s disclosure
The circumstances and type of the disclosure must be considered when attempting to
determine if sexual abuse occurred.
A direct, unprompted verbal disclosure by the child is most highly correlated with
sexual abuse. Such disclosures may happen inadvertently or intentionally.
The specificity of the disclosure is important. Disclosures with specific details about
where they were, what they were wearing, and what exactly the alleged perpetrator
did may be more reliable than vague disclosures that lack detail.
Children will sometimes recant a disclosure of sexual abuse once they have made it,
depending on the response of their family or the person to whom they made the
disclosure.
Often, children’s disclosures are tentative. They “hint” at what is going on (“I don’t
want to go home…”; “I don’t like my Dad anymore”; or “I know someone who….”)
to test the waters of how non-offending parents and other adults might respond.
Disclosures made to a trained interviewer in a forensic setting (such as a multidisciplinary interviewing center) are more reliable, since the interviewer is
specifically trained to ask questions that do not influence the disclosure.
It is also possible for children’s statements to be misunderstood because of
bizarre, fantasy-like, or implausible aspects of the disclosure. 2 Any disclosure of
sexual abuse, no matter how tentative or bizarre, should be evaluated seriously by
CPS and law enforcement.
More information on child disclosures will be covered in Segment 8.
CSA and custody dispute: CPS workers are frequently called upon to evaluate CSA
allegations in the context of custody and visitation disputes. Many investigators in CPS
and law enforcement question the credibility of allegations made under these
circumstances.
Reports of sexual abuse do increase during those times, for any number of reasons—
including the fact that the discovery of the abuse itself may have prompted the divorce.
Social workers should evaluate the validity of sexual abuse allegations that occur during
child custody disputes—by examining the particular information related to the case.
It is much more likely that children will deny true abuse than make false
accusations. 3
3. Corroboration of disclosure/report
Corroboration is defined as the confirmation that some fact or statement is true through
the use of some kind of observable evidence. Since there is often no direct evidence of
sexual abuse, corroborating evidence often helps to confirm whether sexual abuse
occurred. Corroborating evidence should be observable.
2
For more information, see Everson, Mark (1997). Understanding bizarre, improbable, and fantastic
elements in children’s accounts of abuse, Child Maltreatment, Vol. 2, No. 2.
3
For more information, see Faller, 1991.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Since sexual abuse is often shrouded in secrecy and coercion, the only two witnesses to
the event are generally the perpetrator and the victim. In some cases, however, someone
witnesses sexual abuse, and this should be considered.
The statements and observations of other parties about the allegation may be
considered. This might include the statement of teachers, non-custodial parents, and
others who are able to verify some of the facts related to the report.
The statement of the alleged perpetrator may be considered. If law enforcement has
obtained a confession or some other incriminating (or vindicating) statement from the
alleged perpetrator, this should be considered. Remember that interviews with
alleged perpetrators should be coordinated with law enforcement whenever possible.
Other corroborating evidence, such as copies of letters/emails/text messages, pictures,
or videotapes should be considered.
Corroborating evidence may support details about the case. For example, if the child
talks about it happening in a bed with Superman sheets, and those sheets are indeed,
in the closet, then that would be considered corroborating evidence. Other examples
of corroborating evidence include witness statements, medical exams, pictures of
bruises, and witness statements (e.g., a neighbor provides a statement that the stepdad
babysat the girls every Saturday morning).
Corroboration could include verification/observation of injuries to the body (aside
from the genitalia) that were sustained during the sexual abuse. These might include
bruises or injuries sustained trying to restrain the child, for example (e.g., finger tip
bruises on arms). Injuries to the genitals are covered in Elements 6 and 7.
Corroboration of other facts related to the report should also be considered, such as
whether the alleged perpetrator and victim were together at the time of the alleged
incident.
4. Statements about prior unreported sexual abuse
Of these children by any caregivers, or
By these caregivers toward any children
For families that both are and are not involved with CWS, there may be a history of
unreported sexual abuse of the children or a history of unreported maltreatment by the
parents/caregivers of any children (in or out of the household). CWS social workers
should assess for possible unreported maltreatment history, not only to complete a
comprehensive picture in the identification process of child maltreatment, but also
because:
these are important factors in the assessment of safety, risk, and protective capacity,
these are important pieces of information to consider in the development of case
planning services for children, youth, and families involved with CWS, and
these factors may affect the eventual placement of the child(ren) with extended
family, friends, or non-relative foster caregivers.
Prior suspicions or allegations of sexual abuse may be more likely to go unreported, since
allegations of sexual abuse are considered taboo to discuss. This is also culturally
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
mediated, in that a family may have handled the prior report of sexual abuse without
involving the child welfare system (such as having the perpetrator attend church services,
sending the child or perpetrator away for a period of time, etc.).
Note: For this element, consider statements about sexual abuse that are not related to the
current report. The current report or allegation could be a longstanding abusive situation,
and this would not be prior abuse. Examples of prior unreported abuse would include
sexual abuse of the same child by another perpetrator, or sexual abuse of another child
under the care of the caregivers.
5. History of CWS Involvement
With these children, and/or
With these caregivers
Because of the family dynamics involved in sexual abuse, there may be sexual abuse in
the family that involves another family member or a member of the extended family who
has access to the children. In addition, prior reports of abuse and neglect in the family
may indicate lack of supervision, which would create an opportunity for a sexual
perpetrator to befriend or coerce a child victim.
Prior CWS involvement indicates there is a higher risk of maltreatment. Review prior
records carefully to see if there is a pattern and to gain a thorough understanding of
the case history. In some cases, multiple allegations of sexual abuse have been made
on a family, or against a particular member of the family. A family with significant
resources to pay for legal services may be able to successfully have the cases closed
by the Juvenile Court, but multiple prior allegations may indicate that the alleged
perpetrator or non-offending parent are able to successfully cover up allegations of
abuse. CWS social workers should make sure to obtain as much information as
possible about prior allegations of sexual abuse, either in their county or another
jurisdiction.
Prior Juvenile Court involvement indicates increased risk of maltreatment. This
indicates there were family issues and problems that required a high level of
intervention. It indicates a history of maltreatment to the child or a sibling of the
child.
Children freed for adoption/never reunified indicates high risk. These include
children who were made dependents of the court for some type of maltreatment; the
parents were offered services for their return and did not substantially comply with
their reunification plan. Based on the history, this indicates a risk for other children
living with those parents.
If parents have other children who are not living with them, this may be a risk factor.
Make sure to inquire if parents have had any other children who do not live with them
now.
If parents have deceased children, make sure to include this information as well.
Inquire about and note the date, cause, and location of death. This can also be a risk
indicator.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Physical Elements
When a child has been physically involved in sexual activity, there may be physical
indicators or injuries that can be validated through a medical examination by medical
personnel trained in the identification of the signs of child sexual abuse. This is not true
in all cases, however; some children who have been sexually abused will have no
physical indicators of the abuse, even when a comprehensive forensic examination is
conducted within 72 hours of the alleged abuse.
6. Presence of illness or injury(ies)
This element refers to current illness or injury as a result of sexual abuse that can be
documented. These might include (adapted from Rycus & Hughes, 1998, p. 163):
Physical injury to the genitals or another part of the body related to the circumstances
of the abuse (for example, marks or indicators of restraint)
The presence of sexually transmitted diseases
Suspicious stains, blood, or semen on the child’s underwear, clothing, or body
Vaginal discharge, bleeding
Genital pruritis (itching)
Presence of a vaginal foreign body
Recurrent bladder or urinary tract infections
Early, unexplained pregnancy, particularly in a child whose history and behaviors
would not suggest sexual activity with peers
Encopresis, constipation secondary to anal discomfort
These illnesses may or may not be discovered as part of a forensic medical examination
completed as part of the investigation and assessment of the allegations.
Note: Children who have been sexually abused often come to the attention of medical
professionals with general medical symptoms or somatic complaints, such as stomach
aches, insomnia, etc. These are considered under Element 15.
7. Report of past illness or injury (ies)
This element refers to past injuries or illnesses, as above, which were not reported or
recorded as sexual abuse at the time of occurrence. Examples of this might be a report by
a parent or other caregiver that they had noticed soreness or redness in the vaginal area
after previous contact with the alleged perpetrator, but had assumed that it was due to a
problem with hygiene. Conversely, a caregiver might report that the child has a chronic
rash in the genital area, and that they have been working with the pediatrician to address
the problem.
Whenever possible, the social worker should have the parent sign a release of information
form so that they can verify the information provided with the child’s medical provider.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
8. Explanation of illness or injury (ies)
This element refers to the explanation given to the injury or illness. It is highly unlikely
that a young child would develop an STD accidentally, and injuries to the genital area are
fairly rare. Medical or nursing personnel with experience in evaluating sexual abuse
should be consulted when evaluating this element.
When attempting to determine whether sexual abuse has occurred, it is vital to verify all
the claims and explanations for illnesses and injuries. The information that you receive
from the parent may differ from the physician’s assessment, and this should be noted.
Information from a doctor or other health professional should also be assessed critically,
particularly if the health professional is not specially trained in sexual abuse.
Some family physicians may not consider that sexual abuse is a possible cause of a
given medical condition, especially if they have a longstanding relationship with the
family.
Conversely, some medical professionals may become convinced that sexual abuse has
occurred, when an alternative hypothesis appears more likely.
9. Developmental abilities of the alleged victim
The developmental ability of the victim may make them more vulnerable to coercion by
the alleged perpetrator, or make them more easily manipulated or threatened by the
perpetrator. Developmental abilities can refer to a child’s growth, motor skills (gross and
fine), cognitive development, verbal skills, and social/emotional development.
Vulnerability of the child should be considered. Of course, younger children have less
developmental abilities. Children who have impaired or reduced developmental abilities,
particularly in comparison to their peers, may have more vulnerability to abuse. This is
particularly relevant for children with delayed language skills. They may also be more
dependent upon their caregivers, thus increasing the power differential.
Children with impaired or reduced developmental ability have an increased risk of being
maltreated. Child maltreatment may affect development which in turn can precipitate
further abuse (American Academy of Pediatrics, 2001).
10. Developmental abilities of alleged perpetrator
Note: This element only applies when the alleged perpetrator is also a child.
Sexual behavior should be considered in light of the developmental level, rather than just
the age. In cases of sibling abuse, or sexual activity between an older child and a
younger child, the developmental abilities of the alleged perpetrator should be
considered. The impact on the victim should be the overriding concern when identifying
sexual abuse.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
11. Medical assessment findings
Medical Evaluation of Sexual Abuse
An important part of the sexual abuse investigation is the forensic medical exam. In
California, law enforcement officers often authorize sexual abuse examinations as part of
their investigation. However, CPS workers may also authorize4 the exam and may
choose to do so even if law enforcement has declined, because the medical exam has both
physical and psychological benefits (see below). CPS workers should be familiar with
what the usual protocol is in their county for obtaining an exam. Many counties have
specialized, child-friendly pediatric sexual assault clinics as part of their county’s
Multidisciplinary Interview Center/Child Advocacy Center. Other counties perform both
acute and non-acute (see below) exams at hospital emergency rooms.
Types of Medical Evaluations
There are two types of sexual abuse examinations: acute evidentiary (immediate, sameday) and non-acute (as soon as possible after disclosure).
Acute examinations include:
Collection and preservation evidence (semen, saliva, hair, fibers on clothes, etc.)
following a recent sexual abuse/assault episode (usually within past 72 hours,
sometimes longer);
Evaluation, documentation, and treatment of any injuries;
Evaluation for and prophylactic treatment for STDs and pregnancy; and
Provision of crisis intervention services.
Most child abuse forensic examinations are of a non-acute nature (over 72 hours since
last incident of abuse/assault) because of the dynamics of delayed disclosure (discussed
above).
Non-acute forensic examinations include:
Evaluation, documentation and treatment of any injuries;
Evaluation and documentation of old or healing injuries/trauma;
Provision of (post-disclosure) crisis intervention;
Assurance of the physical and psychological well-being of the child.
When Should Children Be Referred for a Forensic Medical Examination?
There is a distinction between “authorization” and “consent.” Authorization refers to
the legal authority that requests that the exam be completed at public expense. Consent
refers to permission to perform the exam and release the results to those with legal
authority to obtain the results. Children over 12 must consent to the exam themselves,
but the exam should not be performed by force even on younger children. Refer to
Family Code 6927 and 6928 for further information on consent issues with minors.
4
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
In all cases in which the most recent episode of abuse/assault occurred within the
last 72 hours (these children should be taken to an emergency room or 24-hour
evidentiary clinic). Note: Due to advances in forensics/evidence gathering
techniques, some jurisdictions perform forensic medical examinations after longer
intervals. When an assault has been disclosed, check with the forensic medical
practitioner to see if an immediate examination is warranted.
When there is a disclosure of penetration, regardless of time elapsed.
When there is evidence by history of pain, trauma, or infection, regardless of time
elapsed.
When the child has physical complaints related to the abuse.
If the disclosure is incomplete or the details are unclear and this might be clarified by
an examination.
When the child or family has questions that would best be answered by an expert
medical practitioner.
When the child would benefit from reassurance that he/she is “okay.”
In summary, the medical evaluation is a very useful tool for CPS workers. Children
benefit both physically and psychologically from the opportunity to meet with a medical
specialist to talk about their bodies. Medical examinations can also yield forensic
evidence that is admissible in both dependency and criminal courts, or medical examiners
can explain why the absence of findings may be consistent with a child’s statements. CPS
workers are encouraged to develop relationships with the medical evaluators in their
counties and to ask for explanations of the findings and the forms/documentation
associated with the sexual abuse medical exam.
Behavioral Elements
12. History of sexually abusive behavior by someone in the home or with access to
the child
This is perhaps the most important indicator of possible sexual abuse, aside from a clear
verbal disclosure by the child. Adults with a history of sexual interest in children are
very likely to re-offend, particularly without intensive treatment. The CWS social worker
should ascertain whether anyone who had access to the children has a history of sexual
behavior with children, either reported or unreported. The non-offending parent may or
may not have knowledge of the history of the perpetrator, and may or may not believe the
allegation (see Familial Elements).
Note: For this element, consider behaviors that are not related to the current report. The
current report or allegation could be a longstanding abusive situation, and this element
would not be relevant. This element would apply to sexually abusive behavior toward
other children, either within or outside the home.
13. Developmentally or socially inappropriate sexual knowledge and/or sexual
behavior
Non-abused children and sexually abused children may exhibit common sexual behaviors
(see the Toni Cavanagh Johnson charts earlier in this curriculum). This may make it
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
difficult to distinguish between sexual behaviors that appear to be the result of sexual
abuse and those that are not.
Sexual behaviors that are common for non-abused children include self-stimulating
behaviors, exhibitionism, and behaviors related to personal boundaries. Less frequently
seen behaviors in non-abused children are more intrusive, such as putting the mouth on
sex parts or putting objects into the vagina or rectum. Behavior that suggests a child’s
explicit or inappropriate knowledge of adult sexual behavior and compulsive
masturbation warrant further investigation.
The CWS social worker should pay special attention to the onset of a shift in behavior(s)
away from the child’s baseline, and whether this coincides with the onset of the abuse
that was alleged, or with the alleged perpetrator’s access to the child. An example of
such a shift in behavior is when a child’s clothing or style of dress changes from one style
to another (either more provocative style of dress or very covered up).
14. Self-protective behavior by the alleged victim
This element includes physical and behavioral methods that the victim uses to protect
themselves from the sexual abuse. The child may attempt to prevent the abuse from
happening long before the abuse is disclosed.
Examples of protective behavior might include:
Attempts to make themselves as unappealing as possible sexually (e.g.,weight gain,
poor hygiene, etc.)
Wearing layers of clothing to make body contact more difficult
Refusal to visit the alleged perpetrator after the onset of the abuse, or attempts to
avoid unsupervised contact with the alleged perpetrator
Temper tantrums when returning to the care of the alleged perpetrator
15. Indicators of emotional distress by alleged victim
Children who have been sexually abused may display a variety of indicators of emotional
distress. The presence of these indicators of distress does not in and of itself indicate that
a child has experienced sexual abuse, however. All of them are also signs of trauma or
distress that could be caused by other forms of abuse, or other sources of stress. The
indicators below are broadly grouped in terms of trauma-related indicators, depressionrelated indicators, anxiety-related indicators, and other indicators.
When evaluating these indicators, the CWS social worker should pay special attention to
the onset of the behaviors, and whether this coincides with the onset of the abuse that was
alleged, or with the alleged perpetrator’s access to the child.
Trauma-related indicators:
Physiological reactivity/hyperarousal (hypervigilance, panic, and startle responses,
etc.)
Retelling and replaying of trauma and post-traumatic play
Intrusive, unwanted images and thoughts and activities intended to reduce or dispel
them
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Sleeping disorders with fear of the dark and nightmares
Dissociative behaviors (forgetting the abuse, placing self in dangerous situations
related to the abuse, inability to concentrate, etc.)
Cutting behaviors
Anxiety-related indicators
Obsessive cleanliness
Self-mutilating or self-stimulating behaviors
Changed eating habits (anorexia, overeating, avoiding certain foods)
Depression-related indicators
Lack of interest in participating in normal physical activities, loss of pleasure in
enjoyable activities
Social withdrawal and the inability to form or to maintain meaningful peer relations
Profound grief in response to losses of innocence, childhood, and trust in oneself,
trust in adults
Suicide attempts
Low self-esteem, poor body image, negative self-perception, distorted sense of one’s
own body
Other indicators
Personality changes
Temper tantrums
Running away from home
Premature participation in sexual relationships
Prostitution
Aggressive behaviors or irritability
Regressive behaviors in young children (thumb sucking or bedwetting)
Poor school attendance and performance
Somatic complaints
Accident proneness and recklessness
Excessive piercings
Dressing down, dressing in thick layers, padding or taping down genitals
Perfect child/extremely high achiever/overly controlled/rigid
Heightened sexualized behavior
Indiscriminate sex
16. Coaching or grooming behaviors
The CWS social worker should try to determine if the perpetrator groomed or prepared
the child for the abuse, by providing special attention to the child, or by escalating the
type and intensity of sexual contact.
Gathering and assessing this information can be difficult, since grooming or coaching
behaviors are often subtle, and difficult to distinguish from normal expressions of care
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
and affection by adults. Sexual perpetrators often provide the same kind of attention that
is appropriate for a parent or grandparent to provide to children.
Sexually abusive adults often groom or initiate children by disguising their motives
through the use of games, secrets, toileting/bathing, and tickling and/or wrestling.
Offenders often “teach,” “help,” and “mentor” older children. They may treat children to
special gifts, special time, and special favors. They may use kid games (videogames,
Gameboy) and interests (sports, motorcycle riding) to connect with them and/or to use for
coercive purposes. They may also expose children to sexual talk and pornographic
movies to desensitize them to sexuality and have frequent physical contact (tickling,
wrestling, hugging, touching) to desensitize children to touch.
Familial Elements
17. Isolation of the child
The more isolated a child is socially and emotionally, the fewer opportunities they will
have to disclose abuse. Moreover, if they feel emotionally isolated, they may be less
compelled to disclose. A child who is socially or emotionally withdrawn may also
present a “safe target” for a perpetrator. But this isolation may also be a reaction to the
abuse.
This element also includes active attempts by the alleged perpetrator to keep the child
isolated from outside social contacts or influences that might cause them to disclose the
abuse. This might include physically isolating the child from outside contacts such as
social groups, school, church, etc. The child may also be isolated in the home, or even
self-isolating from his or her normal activities. The perpetrator might also engage in
isolating behaviors and have, for example, little contact with adult peers. Isolation
encompasses both the physical aspect of isolation as well as emotional separateness.
18. Coercion/threats made to the child to prevent disclosure
The perpetrator will sometimes threaten harm to the child if they disclose the abuse to
their parent or another adult. Threats might include, but are not limited to:
Threats of physical harm to the child or the child’s family
Threats to a treasured object of the child, such as a family pet
Threats that the family will dissolve, or that the child will never see the alleged
perpetrator again (especially in cases of incest)
Threats that appear fantastical to an adult, but may be believable by the child, such as
threats that the child will “go to hell” or that the perpetrator will use some sort of
supernatural powers to harm the child
Threats regarding the safety of the family
Promises of gifts
Other coercive behaviors may also be present, such as bribes or special prizes given to
the child by the perpetrator in exchange for keeping the “secret” of the abuse.
A non-offending parent who does not believe that the abuse occurred may threaten the
child as well.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
The CWS social worker should pay special attention to coercion and threats when
children appear extremely anxious and fearful about the disclosure, or make frantic
attempts to recant their previous disclosure. A forensic interview may be able to sort out
whether threats or coercion were evident.
19. Current caregiver’s substance abuse
A significant number of children in this country are being raised by parents with
addictions. With more than 1 million children confirmed each year as victims of child
abuse and neglect by state Child Protective Service agencies, state welfare records have
indicated that substance abuse is one of the top two problems exhibited by families in
81% of the reported cases5. Cases of sexual abuse may also involve substance abuse by
the parent or guardian.
Children may be poorly supervised by parents who are under the influence, out
looking for drugs, passed out, and coming down off of drugs, or who leave children
unattended when under the influence. The inebriated or high parent may leave
children in the care of inappropriate caregivers who may subject them to physical
abuse, sexual abuse, or neglect. Parents who are under the influence have
compromised judgment and compromised ability to provide appropriate nurturing,
care, and supervision to children.
Loss of impulse control by parents/caregivers under the influence can lead to violence
and abuse, including sexual abuse. There may be an overlap with domestic violence
and substance abuse.
People may lie/minimize while under the influence of drugs or alcohol.
20. Opportunity for the abuse to occur
When identifying whether sexual abuse occurred, the CWS social worker must consider
the opportunity that the alleged perpetrator had to abuse the child. This includes the
home environment, and the capacity of the non-offending parent to perceive that the
abuse may be occurring and protect the child if they suspect that it is.
The non-offending parent may have a great deal of difficulty recognizing the possibility
of sexual abuse, even when it seems obvious to an outsider. The alleged perpetrator may
hold great emotional power over the caregiver, with the result that the caregiver might
not be able to see sexual abuse as a possibility. Examples of this might include when the
alleged perpetrator has very high status in family’s community, such as a church elder or
a community leader.
There may be lack of boundaries in the home, such as no set sleeping locations or the
child/ren not having their own bed/space or privacy.
5
National Association for Children of Alcoholics. (1998). Children of alcoholics: Important facts.
Rockville, MD.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
The non-offending caregiver may also have to work long hours, and may not have the
resources to provide licensed child care for supervision of the child.
Note: This element is often more important in determining that sexual abuse did NOT
occur, i.e., in cases where there was no possibility of contact between the alleged
perpetrator and the alleged victim. This is because most children are alone with other
children or adults at least part of the time. This does not mean that sexual abuse may
occur, unless there are other circumstances that make the opportunity particularly
striking. These might include, for example, a parent who refuses to supervise a child or
children even in a situation that might be sexualized.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5
Child Rearing Standards and Child Sexual Abuse in a Cultural Context
Sexual Behaviors in a Cultural Context
Before the worker can identify any behavior as abnormal, it is important to become
familiar with the normal sexual development, related behaviors, interactions, and feelings
of the growing child. It is important to remember that no child will follow these
developmental stages exactly. Deviations in behavior do not necessarily indicate a serious
problem or sexual abuse in particular, but they should be assessed in the context of the
history, physical findings, and the child’s family environment (Hillman & Solek-Tefft,
1988).
Child Rearing Standards in a Cultural Context (refer back to CMI-1)
The definition of child abuse has changed over time and varies according to the values
and beliefs of the majority culture. Thus child maltreatment can be viewed in a cultural
context as a reflection of the time and area in which we live. Child rearing standards in
general also may be viewed in a cultural context. What defines good parenting today
differs significantly from times past. What is considered optimal parenting also varies by
the culture, time, and place in which one lives.
Child Sexual Abuse in a Cultural Context
In non-clinical studies, Caucasian and African-American women have similar rates of
abuse with Asian rates slightly lower. Latinas are at increased risk for incest. The reasons
for these cultural differences are not clear (Fontes, 2005).
Cultural Aspects of Shame in Child Sexual Abuse:
Responsibility for the abuse
The assignment of responsibility for the abuse can vary widely across cultures. In
many traditional cultures, sexual relations are viewed as a fundamental struggle:
something females should try to avoid and males of all ages should try to obtain.
Where sexual acts have occurred outside marriage, the girl or woman is assumed to
have made herself accessible and is often held responsible, even when there is a
difference in age or power between the people involved. A Peruvian woman
described how her brother had been found to be having sexual relations with his 9year-old stepdaughter, and how the girl was banished to a convent. “It wasn’t his
fault!” she insisted. “The girl was right there with him and was very pretty. She wore
short dresses. She sat on his lap. She asked him to tuck her in at night. Her mother
was away for a month. He couldn’t help himself!” (Hillman & Solek-Tefft, 1988).
It is important for workers to understand cultural norms around the assignment of
blame and responsibility. At the same time, professionals need to help their clients
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
place responsibility for past incidents on the shoulders of the perpetrator, and ensure
that different family members take responsibility for future protection of the child.
Failure to protect
Nonoffending family members are often ashamed of having failed to protect a child
from sexual abuse-thereby having proved themselves inadequate in a key task of their
cultural roles as mothers, fathers, older brothers, etc. A man whose child has been
victimized may feel like a failure as a man; his sense of failure could drive him to
physically attack the perpetrator to recover his feelings of dignity and self-worth.
Professionals need to show fathers and other concerned adults ways in which they can
actively and positively participate in the child victim’s recovery and protect other
children (Pearce & Pezzot-Pearce, 1997).
Fate
People with a culturally fatalistic view, believing that forces outside or beyond an
individual determine the life course, will often respond quite passively to the
discovery of sexual abuse. This world view is unlikely to be changed.
The worker can ask each person involved, “How do you explain why the abuse
happened?” in an effort to determine if they see fate as the reason for the abuse. A
worker can then follow up with a statement such as:
o “Thank you for letting me know how you explain what happened. I’d like to
suggest a couple of other ideas, so you can know how I think about it. I expect
that both perspectives contain some truth. ____________ chose to abuse your
child because______________ has sexual feelings toward children, and found a
way to be alone with your child and act on those feelings. We can work together
to help your child and family recover from this, and to make sure nothing like this
happens again. I encourage you to continue to do all the things you are doing to
help you to cope [e.g. praying]. I have ideas about other things that could be
helpful to you and your child too, and have been helpful to other people in your
situation” (Fontes, 2005, pp.143-145).
Damaged goods
There is a sense of being “soiled” or “spoiled” and the child may come to believe they
are “dirty” as a result of the abuse. If the knowledge of the sexual abuse were to
become known in their community, the family and child might be ostracized and
considered unworthy. The girl victim might also lose her potential value as a future
wife and daughter-in-law, an important part of a grown woman’s identity in many
cultures around the world.
Virginity
Many cultures control women’s sexuality by expecting girls to maintain their
virginity until marriage. This expectation includes traditional families from many
parts of Asia, Africa, Europe, the Middle East, and the Americas. In some traditional
cultures, a girl who has engaged in any kind of sexual activity, even forced, may well
be perceived as losing her virginity, and thereby be considered either not suitable for
marriage or of lesser value as a bride.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
“In many places the absence of virginity may mean that a young girl loses her chance
for marriage. If the situation is known, she loses her prestige within the family [just]
as the family loses it in their close neighborhood…Sexual abusers seem to pay
attention to this issue, and some girls are threatened with “losing their hymen” which
explains [the elevated presence of] nonpenetrating sexual abuse. On the other hand,
the first reaction of the nonoffending parent and other relatives is to take the child or
young girl for an examination of her virginity, when they find out about the abuse. If
the hymen is left intact, the sexual abuse cannot be proved, and this makes the denial
easier for the family. Professionals, therefore, emphasize that fact that the presence of
the hymen does not preclude sexual abuse” (Yuksel, 2000).
Predictions of a shameful future- promiscuity, homosexuality, and sexual offending
People from many cultures believe that girls who have suffered sexual abuse are
likely to become promiscuous and boys who have been sexually abused by men are
likely to become either homosexuals or sexual offenders. There is no indication that
sexual abuse will influence a boy’s later sexual orientation (Arey, 1995). Boys who
have been sexually abused appear to engage in more sexual behaviors, such as
masturbation, sexual play, and sexual aggression with younger children, than boys
who have not been sexually abused (Friedrich, Grambsch, Damon, Koverola, Hewitt,
Lang, & Wolfe, 1992).
Re-victimization
In some cultures, when a girl is known to have been sexually abused, she has lost the
special protective aura of virginity and is considered to be “fair game” for other men
to try to seduce or assault. Russell (1986) suggests that knowledge of prior
victimization may disinhibit some perpetrator’s abusive tendencies toward these girls.
Grauerholz (2000) describes a variety of reasons why girls and women may be more
likely to suffer further experiences of sexual assault following sexual abuse in
childhood: continued exposure to the factors that put her at risk in the first place,
lessened ability to detect danger, and the use of substances that inhibit her ability to
avoid dangerous situations or to escape from them.
Layers of shame
There are factors which the individual might already feel a sense of shame about
because they are not congruent with what is valued by the majority culture, such as
skin color, hair texture, eye shape, or social status. The sexual abuse and its
consequences magnify these factors (Fontes, 2005).
Gender and Role Differentiation Issues Influencing Child Sexual Abuse
Double Standard between Male and Female Children:
In almost every society, expectations of and for male and female children are different.
This difference is frequently reflected in the expression of sexual behaviors. When we
talk about the sexual victimization of children, if you have a 12 year old girl who is
molested by a 25 year old male, no one has a problem in seeing the girl as a victim of
sexual abuse or exploitation. In general, child protection and law enforcement systems
will move to protect the child and hold the perpetrator accountable for the violation of
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
criminal laws. If the child is a 12 year old boy and the perpetrator is a 25 year old
woman, there is much more ambivalence in viewing the boy as a victim, and in fact,
many may see him as “lucky”. Within some cultures this may be seen as a desired part of
his development as a man. The protection and enforcement systems may be slower to act
to protect, the family may be less supportive of such intervention, and the child not seen
in need of therapeutic services.
However, if the 12 year old boy has been molested by a 25 year old male, the paradigm
shifts and the child is now without question, the victim, and the adult responsible, an
offender. The protective systems come in rapidly and act to protect, the family feels a bad
thing has happened to their son, and the belief is that without therapeutic intervention the
child may suffer long term, potentially severe, consequences. There is also the additional
concern he will become either a perpetrator himself, or, within some cultures, a
homosexual (Fontes, 2005). The scenario of the 12 year old female being molested by a
25 year old female is rarely considered.
The double standard also is reflected in the behaviors considered “normal” or appropriate
for a child or adolescent within that culture. As noted in earlier classes, culture is
evolving, and the norms, including sexual norms, change over time. In general, males
have more freedom and are allowed a wider expression of sexual behaviors than females,
with fewer repercussions or sanctions when they violate cultural or community norms.
The value of a boy or man’s masculinity may hinge on the number of his conquests, and
the value of a girl or woman’s femininity may hinge on her chastity (Fontes, 2005). It
may be difficult for families to assign responsibility appropriately in cases of brothersister incest, particularly in cultures that value boys more highly than girls. Parents
frequently minimize or deny the significance of brother-sister incest, or they blame the
girl (Fontes, 2005).
Sexual Orientation – Gay, Lesbian, Bisexual, Transgendered & Questioning Youth
What is allowed in terms of expression or exploration of sexual identity also varies
between cultures, ages, and genders. “Expectations for gender roles and heterosexual
activity are communicated overtly and covertly and are the ways and means through
which girls and boys learn the values, beliefs, and customs of conventional masculinity
and femininity” (Ungar, 2005, p. 266). Same sex experimentation may be more expected
and/or excused among younger children or one gender. Because homophobia and
heterosexism continue to be largely unchallenged in contemporary society, lesbian, gay,
bisexual, transgendered, and questioning (LGBTQ) youth frequently face overt
discrimination without intervention from others. The Gay, Lesbian, and Straight
Education Network’s survey of LGBTQ students across the United States reported that
83% had been verbally harassed and 42% had been physically harassed in school, with
84% of high school students hearing the words faggot or dyke in the classroom frequently
or often (Ungar, 2005). This peer isolation, added to family lack of acceptance may
increase the child’s search for love and acceptance in unsafe ways with individuals more
predisposed to abuse or exploiting them.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 2
Personal Difficulties in Dealing with Sexuality & Victimization
Emotional reactions to child sexual abuse is normal and to be expected. However, it is
important to recognize our emotional reactions to prevent them from impairing our
professional judgment or performance of our duties as child welfare workers. Despite
education and training, which specifies how to perform our professional roles, it is
normal for each of us to have personal reactions to our work. Child sexual abuse probably
arouses more personal reactions than many of the problems we encounter. Although these
may become less intense over time, they do not disappear. Initially, the enormity of
sexual abuse is likely to engender one of two opposing responses—disbelief or belief
accompanied by an intense desire for retribution.
Gender
The gender of the professional is likely to influence reactions to cases of child sexual
abuse. Both male and female professionals have empathy for victims. However, it is
possible that gender identification causes each to be more sensitive when the victim is of
his or her own gender. Professional reactions to sexual abuse may differ by gender
because men and women experience living in society differently.
Life Experiences
Many life experiences can intrude upon professional practice, and working in sexual
abuse can intrude upon a professional’s personal life. Three personal issues that seem
particularly salient are: having been sexually victimized, being a parent, and sexuality.
Sexual Victimization
A professional who has been sexually abused her/himself or who is part of a family in
which there has been sexual abuse must cope with this personal issue as well as with the
other stresses of work associated with working with sexual abuse survivors. Persons who
have sexual victimization in their background bring special sensitivity and experience
that can be of great value in their work. Nevertheless, professionals who have personal
experiences of sexual abuse need to have addressed these in therapy, be especially aware
of countertransference issues, and be alert to the importance of protecting their own
mental health.
Warning signs that the professional’s own victimization is impeding performance can
include:
□ Feeling so overwhelmed by fear, anxiety, disgust, or anger that the victimization
interferes with sound decision making or intervention or evokes the strong desire for
retribution;
□ Experiencing intrusive thoughts or having flashbacks at work;
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
□
□
□
Recalling previously repressed memories of victimization when involved in cases of
sexual abuse;
Displaying overly punitive responses to the non-offending parent or offender; and/or
Minimizing or not seeing the safety issues involved in a case, or the severity of the
effects on a child.
Being A Parent
The experience of parenthood can affect one’s reaction to a case of sexual abuse, and
working with sexual abuse can influence parenting. Parenthood can make the
professional more appreciative of the risks as well as more appalled at the transgressions
of the parenting role. Parents are confronted with many situations in which the child’s
behavior (e.g. wanting to sleep in bed between the parents) and parenting responsibilities
(the need to assist the child in bathing, toileting, and understanding the differences
between male and female anatomy) can present risks for sexual activity.
Sometimes, professionals who are parents are less willing to label client behaviors as
sexually inappropriate because of their over-identification with the client as a parent. For
example, a professional who is a father may minimize genital contact between an alleged
offender father and his daughter, accepting the explanation that the daughter was being
helped to learn about “wiping herself.”
Conversely, certain biological drives and normative proscriptions inhibit sexual activity
with children for parents. Because of these personal experiences, parents may be more
censorious than non-parents when these boundaries are crossed. Individual families will
have differing norms for what are acceptable personal boundaries or privacy, male and
female roles in parenting behaviors, and acceptable discussions around perceived or real
sexual matters.
In terms of work influencing parenting, a common effect of professional involvement
with sexual abuse cases is for the parent to become quite concerned about the risk of
his/her own children being sexually abused or exploited. Parents may be hypervigilant to
behavioral or physical indicators exhibited by their own children, such as urinary tract
infections, masturbation, enuresis, and sleep disturbances.
Comfort and History with Sexuality
Being familiar and comfortable with all aspects of sexuality is essential in working in the
field of child sexual abuse. For the professional, this means being able to talk freely about
all types of sexual issues.
Professional involvement with cases of sexual abuse very frequently has an impact on
personal sexuality.
Coping with Personal Issues
The best way to prevent personal reactions from undermining the quality of professional
work is to be aware of their existence. Once these reactions are identified, several
methods can be used to help to mitigate them, including:
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
□
□
□
□
□
Self-talk, in which the professional reminds him/herself of personal biases and
reactions.
Talking about, acknowledging and processing personal reactions and feelings about
cases with a supervisor, mentor, or trusted colleague. (Note: Remember that all case
information is confidential; child welfare workers need to request time with someone
within the agency, such as your supervisor, to discuss any detailed information.)
Using established guidelines and research to guide decision-making.
When possible, using collaborative decision-making with colleagues involved in the
case.
When the above suggestions are not sufficient, talking about, acknowledging and
processing personal reactions and feelings about cases with a counselor or therapist.
Avoiding Burnout
There is no denying that work in the field of sexual abuse is extremely stressful and may
lead to burnout. There are several characteristics of cases that make the work potentially
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 8
Child Disclosures, Reluctance to Disclose
Child disclosure of sexual abuse has generated controversy, with great debate in the press
and the academic community about the validity of children’s disclosures. Many studies
have methodological problems, and/or small sample sizes, exacerbating the controversy.
Only recently has a body of research emerged and analyzed that provides some guidance
for child welfare practitioners. Olafson and Lederman (2006) provide perhaps the most
comprehensive analysis and summary of the available research in their article, The State
of Debate About Children’s Disclosure Patterns in Child Sexual Abuse Cases. Their
summary of research findings are excerpted below, with some clarifying definitions
inserted.
Summary of Research Findings on Disclosure of Children Regarding Their Sexual
Abuse
1. Experts agree that a majority of child sexual abuse victims do not disclose their abuse
during childhood.
2. Experts agree that when children do disclose sexual abuse during childhood, it is
often after long delays.
3. Prior disclosure predicts disclosure during formal interviews. Children who have told
someone about the abuse prior to the formal interview are more likely to disclose
during the interview than children who have not. Children who have not previously
disclosed and who have come to the attention of the authorities because of medical
evidence, videotapes, and other external evidence, are less likely to disclose during
medical or investigative interviews than are previously disclosing children.
4. Gradual or incremental disclosure (where a child may disclose only aspects of an
abusive event during the initial interview) of child sexual abuse occurs in many cases,
so that more than one interview may become necessary.
5. Experts disagree about whether children will disclose sexual abuse when they are
interviewed. However, when both suspicion bias (cases which come to the attention
of the authorities because a child disclosed to someone prior to the formal interview)
and substantiation bias (substantiation was completely independent of the child’s
statements) are factored out of studies, studies with external corroborating evidence
of child sexual abuse show that 42% to 50% of children do not disclose sexual abuse
when asked during formal interviews.
6. School-age children who do disclose are most likely to first tell a caregiver about
what happened to them.
7. Children first abused as adolescents are most likely to disclose than are younger
children, and they are more likely to confide first in another adolescent than to a
caregiver.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
8. When children are asked why they did not tell about the sexual abuse, the most
common answer is fear. (We need to ask children in the child interview what they
are afraid will happen if they talk about what happened when…)
9. Further research is needed about recantation rates, which range in various studies
from 4% to 22%.
10. Lack of maternal or paternal support is a strong predictor of children’s denial of
abuse during formal questioning. Abuse by a family member may inhibit
disclosure. Dissociative and post-traumatic symptoms may contribute to nondisclosure. Modesty, embarrassment, and stigmatization may contribute to nondisclosure. Gender, race, and ethnicity affect children’s disclosure patterns.
11. Many unanswered questions about children’s disclosure patterns remain, and further
multivariate research is warranted.
Intentional and Accidental Disclosure
Sgroi (1982) suggested two types of disclosures are encountered—the purposeful and
the accidental. In the former, the child makes the conscious decision to tell of the abuse.
In accidental disclosures, the child has made no overt statement to anyone with the
intention of seeking intervention. The accidental class of disclosure includes such
allegations as those involving sexually explicit play on the part of a preschooler, a
pregnancy in a very young adolescent, a child presenting with a sexually transmitted
disease, the purposeful disclosure of a child victim who names other child victims, or the
observation of the perpetrator-child sexual activity, including the interception of child
pornography.
Where the child has made a purposeful (deliberate) disclosure to an adult, the initial CWS
interview with the child is more likely to yield a more detailed description of the sexually
abusive activity. Even when there is independent evidence or information for the sexual
abuse or exploitation, the child interview might not yield a disclosure if the child has not
cognitively made the decision to tell. Research indicates that multiple interviews are
frequently necessary for a number of children to feel safe or comfortable enough to
disclose.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 8
The Non-Offending Parent/Caregiver
Much research has demonstrated that the non-offending parents’ ability to provide
support following a disclosure of sexual abuse is the most critical factor influencing the
child’s post-disclosure adjustment. Non-offending parents may be viewed on a
continuum. They range from those who, prior to disclosure, have knowledge of the abuse
and do nothing, to those who “sense” something is not right but do nothing, to those who
recognize potentially abusive actions and are proactive in protecting the child. Postdisclosure responses range from those who align with the perpetrator and do not believe
the child to those who immediately believe and take protective action upon hearing a
disclosure.
In her book, The Mother’s Book: How to Survive the Molestation of Your Child (1992),
Carolyn Byerly lists these diverse reactions of non-offending parents after a disclosure of
child sexual abuse:
Numbness
Jealousy
Distance
Sexual inadequacy or rejection
Anger
Religious concerns
Disbelief
Minimizing the seriousness
Denial
Revenge
Shame
Financial and other fears
Invisibility
Hatred
Guilt and self-blame
Repulsion
Hurt and betrayal
A desire to protect him (the alleged
Confusion and doubt
offender)
It is difficult to predict how a particular parent will react. Responses may also reflect
cultural components as well as the non-offending parent’s role in the relationship. Crosscultural marriages and dependency issues may also color both immediate and long-term
responses. Although not all parents experience significant distress following a disclosure
of sexual abuse, many do. Some parents may experience emotional distress and
depression which can be related to loss of income and financial support, changes in
relationships with family and friends, and disruptions in employment and living
situations.
There is growing evidence that when mothers are incapacitated in some way, children are
more vulnerable to abuse. That incapacitation may take a variety of forms. When a
mother is absent from a family due to divorce, death, or sickness, children appear to
suffer more abuse. Mothers may also be psychologically absent because they are
alienated from their children or husband or are suffering from other emotional
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
disturbances, with similar consequences. Mothers may be unable to protect children
because they themselves are abused and intimidated. Even large power imbalances that
may stem from differences in education may undercut a woman’s ability to be an ally for
her children (Finkelhor, 1984).
When non-offending caregivers first learn about the abuse, their reactions vary
considerably. The majority of mothers believe their child’s allegations, either totally or in
part, and most take some protective action. However, a substantial number did not
believe their children’s allegations and did not take protective action. Some were in the
middle; although ambivalent about the allegations, they took protective action anyway.
Elliot & Carne’s (2001) study examined a history of abuse on non-offending parent
reaction post-disclosure. The study examined four factors to see if parental belief,
support, and protection can be predicted. These factors include: mother’s relationship
with the perpetrator; mother’s own history of childhood abuse; victim’s age; and victim’s
gender. Anecdotal experience suggests that sometimes a parental history of sexual abuse
or victimization may influence whether her ”radar” responds to warning signs that abuse
may be happening. Some mothers who never disclose their own abuse or did not receive
treatment may deny abuse because, by acknowledging it in their children, they must
acknowledge their own history. Most of the above factors yielded inconsistent results,
though some studies indicate that young children are believed more often than older
children and adolescents.
A parent who has introduced the perpetrator to the child or family, such as the single
mother who is dating, may experience denial, guilt, or depression upon hearing the
child’s disclosure of sexual abuse. A mother may go through stages analogous to those
experienced by individuals who are dying, before she comes to believe the child. Denial,
guilt, anxiety, fear of repercussions, or depression may decrease the mother’s ability to
help the child cope with the traumatic experience.
Denial. Denial is a defense mechanism used to avoid psychic trauma or painful
reality. Denial can cause reactions such as: “No, not me, not my child, not my
husband, etc., etc. There must a mistake. My child must be making this up for some
reason.” Instead of immediately being labeled as non-cooperative, it is important for
child welfare workers to distinguish between a normal, initial reaction of disbelief,
which indicates a need for support and service, and chronic denial. As the literature
above notes, even parents who are non-believing or in denial can take protective
measures.
Anger. In the grief cycle, people need to blame someone outside themselves for their
painful situation. Anger may be directed at themselves for not seeing the abuse, at
the child for participating, at CWS and law enforcement for their involvement, at the
“situation,” and, appropriately, at the perpetrator. (Note: Anger may be due to lack
of understanding about the dynamics of sexual abuse. Anger at the child that persists
despite the passage of time or following education and support may be an indicator of
inability to provide support or protection, requiring CWS intervention).
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Bargaining. During this phase, the parent tries to regain some emotional stability.
Feelings may alternate between “positive” actions such as reporting, seeking therapy,
kicking out the perpetrator, etc., and “negative” actions such as continuing to seek
alternative explanations, believing the child while allowing the perpetrator to retain
access, thinking they can handle it within the family, etc., and making inconsistent
statements to the child, e.g., “I believe you, but I also can’t believe your uncle is
lying.”
Note: It is very important that child welfare workers make efforts to explore and
understand the motivations behind seemingly negative actions. Sometimes, parents
are doing what they think is best for the child, as in families who would otherwise be
homeless or without any means of financial support or families with domestic
violence and the mother fears that the father may injure or kill her or the children.
Families may also respond in a particular way because of deeply held cultural or
religious beliefs or out of fear of the system response. (See section on cultural
issues.) Understanding these motivations provides windows into important points of
service intervention.
Depression. This is a very painful and uncertain period as the full magnitude of what
has happened sinks in. Depression can be debilitating as the parent feels that her
whole life is defined by the abuse, and is unable to see a future where this will not be
the case. It may be difficult for her to be emotionally supportive of her child because
of her own pain. For non-offending parents with their own history of abuse, this
phase can include a recapitulation of their own abuse experience. (Note: This stage
can be a powerful point of intervention if the parent receives support.)
Resolution. In this final stage, the parent begins to put the pieces of her life back
together, can envision and begin to create a future. It does not mean that she forgets
what has happened, but she can place it in perspective and not have it dominate her
whole life. She can also help the child and siblings with their own healing and
resolution.
In summary, by being aware of the range of responses in terms of belief and
protectiveness, child welfare workers can contribute to better outcomes for children.
While the research on maternal responsiveness is inconclusive, one thing is clear: a
supportive parent is associated with a better outcome for children. For this reason, a
nonjudgmental and empathic approach during the early stages of investigation and
intervention may be more effective than confrontation. Normalizing a parent’s denial or
shock and helping her to understand her response, rather than labeling her as “nonprotective” or “uncooperative,” can be an effective engagement strategy.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Trainee Content for Day 1, Segment 9
Myths & Research about Sexual Offenders6
There are commonly held beliefs about sexual offenders that are actually myths. Since
the 1970s, empirical data from various sources (research through the National Institutes
of Mental Health, records from Great Britain’s prisons and studies in outpatient clinics in
Great Britain and the USA) has improved our knowledge about sexual offending and
undermines these myths (Abel, Mittleman, Cunningham-Rather, Rouleau, & Murphy,
1987; Abel & Harlow, 2001).
1. Molesters usually have a particular type of victim they look for and are probably
not dangerous to children who don’t fit the profile (e.g., only molest boys, only
young girls, etc.).
In the 1970s, Gene Abel, MD and colleagues collected extensive data on 533 convicted
sex offenders in their Atlanta and New York clinics. These men received immunity from
prosecution and their names and information were sealed. Even with these protections,
the belief is that they underreported their offenses. Nonetheless, the findings from this
landmark study were astonishing:
62.5% of men who had molested a male had also molested a female.
23% of men who molested a female had also molested a male.
Of men who were convicted for molesting adolescents, 100% admitted to molesting
adolescents, 68% admitted to also molesting children, and 45% had also raped adults.
Of men who were convicted for raping adults, 100% admitted to raping adults, 49%
admitted to also molesting children, and 39% had also molested adolescents.
Of men who were convicted for molesting children, 100% admitted to molesting
children, 43% admitted to also molesting adolescents, and 34% had also raped adults
(Abel, et al., 1987).
A study from the British Penal System also found a very high degree of crossover in both
gender and age. For example, when the initial victim was a male child, 1 out of 3 men
6
The material on sexual offenders has been in part provided Miriam Wolf (Child Sexual
Abuse) and Niki Delson (www.delko.net).
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
who were subsequently rearrested victimized a female; when the initial victim was a
female, one-fifth was rearrested for a molest of a male child (Thornton, 2000).
Abel & Harlow (2001) later conducted a larger study with a sample of 3,952 admitted
child molesters and found:
Of the pedophiles who molest girls, 21% also molest boys. Of the pedophiles who
molest boys, 53% also molest girls.
Male molesters whose preference is for adolescent males (14-17 years old),
“ephebophiles”, frequently become involved with other children. A study of over 600
male ephebophiles found that slightly over 50% also had a history of molesting boys
under age 14. In addition, over 28% had molested girls under age 14, and 20% had
molested girls 14 to 17 years of age.
2. There is a typical “offender profile.”
The Abel & Harlow Child Molestation Prevention Study (2001) highlights the fact there
is no typical offender profile and that child molesters look the same as everyone else.
(Note: Due to small sample size, all females’ data was removed from survey as was the
data for those who molested adolescents above the age of 13. See supplemental handouts
for more information on female perpetrators)
Comparison with Men in the U.S. Population:
Demographics (Admitted child molesters N = 3,952, Ages: 18 to 95, average age 38.5)
U. S. Males
Admitted Child
Molesters
Married or formerly
married
Some college or higher
education
High school graduate
73%
77%
49%
46%
32%
30%
Working
64%
65%
Religious
93%
93%
Ethnicity (2% of the study sample reported they were from none of the represented ethnicities)
U. S. Males
Admitted Child
Molesters
Caucasian
72%
79%
Hispanic/Latin American
11%
9%
African-American
12%
6%
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Asian
4%
1%
American Indian
1%
3%
3. Because it is a family problem, incest offenders do not present much danger
outside their families.
From the Abel, et al (1987) study:
65.8% of men who committed sex offenses inside of their families had also
committed sex offenses outside of their families.
From the Abel & Harlow (2001) study:
68% reported they had molested a child in their family. (The 68% is based on
individual men, while each individual man may have molested one child or several
children who were in different family relationships with them.)
o 19% reported molesting a biological child
o 30% reported molesting a stepchild, adopted child (3.3%), or foster child (1.3%)
o 18% reported molesting nieces or nephews
o 5% reported molesting grandchildren
o 12% of perpetrators as teenagers, molested a much younger brother or sister
40% reported molesting the children of their friends or neighbors.
o Nearly 24% of the men who were molesting children in their own family were
also molesting the children of friends and neighbors
o 5% said they had molested “a child left in my care by an organization”
4. Most sexual offenders perpetrate sexual abuse and rape because they were
victims of sexual abuse and are acting out what was done to them.
For many years, there has been an idea of a “victim-to-victimizer” cycle; that sexual
abuse as a child is a powerful risk factor for becoming a sexual offender. However, this
conclusion is not supported by research. Although not entirely without foundation
(somewhere between 20-30% of adult, male offenders do have a sexual abuse history),
most sexual offenders do not have sexual abuse histories. The “victim-to-victimizer”
theory was initially borrowed from physical abuse, where there is a stronger cycle
connection between childhood experiences and adult perpetrator behavior. The notion
was also supported by early retrospective self-report data from incarcerated, adult sex
offenders. This population has some motivation to exaggerate or lie about their abuse
histories, as people may look at their offenses more “kindly” if they are also “victims”.
Studies which attempted to verify these self-reports using polygraphs have demonstrated
that self-reports of victimization are exaggerated.
The rate does appear to be higher for children with sexual behavior problems. However,
most children who were sexually victimized never perpetrate against others. So,
while a sexual abuse history is a factor in individual cases, it does not seem to be
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
sufficient as a general explanation about why people sexually offend. The causes are
more complex. Research does point to links with childhood histories of physical abuse or
neglect and witnessing domestic violence, as well as other pathways that are similar to
other kinds of violent offending, such as early behavior/conduct problems, delinquency,
alcohol/drug use (Chaffin, Letourneau, & Silovsky, 2002).
Conclusions
There have been many classifications proposed to help categorize and understand the
motivations of offenders and predict recidivism (Cohen, Groth, & Siegel, 1978; Lanning,
2001). Typologies such as “fixated/regressed” and “situational/preferential” were
proposed. While important contributions to the literature, it has become clear that child
molesters are a very heterogeneous group, with different motivations for offending and a
need for varied treatment methodologies. The conclusions we can make are:
There is no single “child molester personality profile.”
Child molestation is usually not an isolated incident; by the time it is discovered, the
pattern is often chronic.
Most offenders are reluctant to admit offenses/deviances other than that for which
they have been caught, but when given immunity, many molesters report victims into
the dozens or hundreds.
Offenders commonly use tactics of manipulation, deception, and denial to seduce
children and to convince others of their innocence.
We cannot assume that children who do not fit the molester’s “victim profile” are not
at risk; there is significant crossover among age, gender, and intra- and extra-familial
victims.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Trainee Content for Day 2, Segment 13
Treatment Issues
Treatment of the Child Victim7
It is not known if all children need treatment following sexual abuse. As discussed above
in the section on child victims, a significant number of children may not display
symptoms at the time of abuse. When children do display symptoms, the literature is
conflicting about whether and how quickly symptoms subside, with or without therapy.
There is great diversity in individual victim characteristics (see above section on
mediating factors). Some children will show improvement without therapy, some after
short-term (10–16 sessions), some only after longer-term therapy, and some may benefit
from “crisis-intervention” that consists of anticipatory guidance about recognizing and
responding to problems in the future.
While there is no available “formula” to determine whether and how long children
should be in treatment, every child and teenager who is a victim of sexual abuse
should be assessed by a qualified professional to determine their mental health
status and needs. Such evaluation should consider the possibility that some children
engage in maladaptive avoidant behaviors as well as the fact that few children or
teenagers will self-refer for treatment. (Note: In California, minors age 12 and older are
legally allowed to self-refer for the purposes of treatment for sexual assault. —Cal. Fam.
Code § 6924.)
The Mental Health Care for Child Crime Victims: Standards of Care Task Force
Guidelines published by the California Victims of Crime Program notes that an
appropriate child treatment plan should do the following:
Take into account a child’s developmental status;
Specify treatment goals that are achievable and that address the presenting
problems;
Employ methods that have empirical support or the support of extensive expert
opinion in peer review publications;
Include parents or caregivers in the treatment plan in a meaningful way;
Include consultation with other adults who may have a significant role in the
child’s well being, e.g., teachers or healthcare providers;
7
Parts of this section were adapted by Miriam Wolf, LCSW, from Winterstein, M., &
Scribner, S. (Eds.) (2001). Mental health care for child crime victims: Standards of Care
Task Force guidelines. Sacramento, CA: Victims of Crime Program, California Victim
Compensation and Government Claims Board. Used with permission of, and thanks to,
Michele Winterstein, Ph.D.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Assume that if any gains made in the therapy hour are to survive and generalize,
the child must be living in a safe environment, free from abuse.
While there are different modalities of providing therapy (individual, group, play therapy,
etc.), many child victims can benefit from trauma-focused, or abuse-specific, treatment.
The treatment goal is successful emotional and cognitive processing of the event.
Education is provided to the child and family by the therapist. If disturbing events can be
described, and the responses to them understood, then out-of-proportion attributions for
the event and the abuse-related coping responses can be contained, avoiding the
development of more serious consequences over time.
Frequently cited goals of therapy with sexually abused children include:
Providing a safe release of feelings, both positive and negative, about the abuse
experience;
Providing relief from symptoms and behaviors that are interfering with the child’s
functioning and making connections between the behaviors and the abuse
experience;
Helping to correct cognitive distortions (how thinking has been affected by the
abuse, misunderstandings, misattributions of blame, etc.);
Addressing any developmental interruptions (assisting the child or adolescent in
redoing missed or distorted tasks and encouraging growth)
Rebuilding trust in oneself and in others;
Developing a sense of perspective and distance regarding the trauma, and hopes
for the future;
Education and support about age-appropriate aspects of sexuality.
Longer-term therapy may also address the longer-term effects of abuse and associated
behaviors (discussed above in the section on victim dynamics, effects, and mitigating
factors). Because intrafamilial abuse occurs within the context of a family, all of the
family relationships are affected, first by the abuse itself and then by changes in the
family system that occur with intervention. The relationships between the victim and the
offender, non-offending parent and sibling(s) are usually complex and affects children in
multiple aspects of their emotional and social lives. While there are emotional impacts
such as guilt, ambivalence, fear, and anger toward the offender, or feelings that the nonoffending parent failed to protect them, there may also be issues associated with losses
such as removal from the family home, loss of relationships with family and friends, and
the challenge of adjusting to life with relatives, foster parents, or residential placement.
Treatment may also address these areas.
The child’s therapist may also coordinate and monitor the timing and advent of visitation,
dyadic and family therapy, and reunification, if planned (see section on visitation and
reunification, above). It is recommended that each family member (child victims,
siblings, and non-offending parents) have access to their own individual or group therapy.
Dyadic and family therapy, often concurrent with individual or group therapy, can
accelerate progress for many children and families. Managing the intense feelings that
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
can be generated by that therapy and visitation are key areas for the child’s therapist in
cases of intrafamilial sexual abuse. Reunification therapy is quite complicated and
requires specialized training. CPS workers should be sure that the child’s therapist has
expertise in this area.
Treatment of Adolescents
A note about treatment needs of adolescents: Like younger victims, not all adolescents
will need psychological treatment. Developmental issues, however, often get in the way
of an accurate assessment of treatment needs. The impact of abuse can vary depending
on onset and duration of abuse—whether it began in childhood and continued, worsened
in adolescence, or began in adolescence. Some adolescents view treatment as intrusive
and a challenge to their emerging autonomy. Many work very hard at avoiding dealing
with the experience only to have symptoms/effects emerge at a later time. Still others
view treatment as a “punishment” and express anger that no one else (non-offending
parent or offender) “has” to go. Additionally, some adolescents view the relationship in
question as consensual and are angry at others’ perception of it as abusive. It is safe to
say that many adolescents will be reluctant to enter therapy for these and other reasons.
Just as in other areas of providing guidance and limit-setting to teens, this may be an area
where their reluctance to do something should not always be accepted at face value.
Developing a cadre of therapists with demonstrated success in engaging and working
with adolescents to refer to is important for CPS workers.
Treatment of Siblings
Just as victims should be assessed for treatment needs and goals, so should siblings.
Siblings may have their own as-yet-undisclosed victimization/trauma history as well as
emotional responses to what has transpired in the family. Complex feelings may include
anger/blame (at the victim, other family members, the situation), guilt, fear, jealousy as a
result of observing the favored status of the victim, helplessness and powerlessness in the
face of a perceived inability to protect the victim. These issues should be addressed in the
therapy of the sibling in order to develop or restore a healthy, mutually respectful and
protective relationship between the victim and his or her siblings.
Treatment of the Non-Offending Parent
As discussed above, the literature demonstrates that non-offending parents frequently
experience significant distress following a disclosure of sexual abuse. The literature also
confirms that support/protection from non-offending parents is associated with improved
emotional and behavioral adjustment and healing in the child victim. For these reasons,
non-offending parents should also be referred for a mental health assessment. Because
their symptoms and coping abilities will vary during this tumultuous period, assessments
may need to be conducted at different points in the life of a case.
Foci of treatment often include:
Support/empathy for distress symptoms;
Psycho-education about sexuality and dynamics/effects of sexual abuse;
The offending cycle/how abuse happens;
Reducing denial and minimization;
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Addressing feelings of betrayal and violation by the offender;
Addressing effects of prior victimization, if any;
Increasing capacity for safety and protection;
General parenting education and support.
Offender Treatment
Most offender treatment programs use a combination of cognitive-behavioral treatment
and relapse prevention techniques. Modalities include both individual and group therapy
and may include victimization awareness and empathy training, cognitive restructuring,
learning about the sexual abuse cycle, relapse prevention planning, anger management
and assertiveness training, social and interpersonal skills development, substance abuse
treatment, and changing deviant sexual arousal patterns. Pharmacological interventions
may also be used.
CPS workers should ensure that any treatment provider is experienced working with a
sex offender population. Treatment providers should be able to mention the instruments
they use in evaluation and treatment and the professional organizations they belong to
(ATSA—Association for the Treatment of Sexual Offenders and CCOSO
http://www.ccoso.org —California Coalition on Sexual Offending, etc.).
Treatment in Los Angeles County
In Los Angeles County, the Department of Children and Family Services has what seems
to be a unique approach to intrafamilial child sexual abuse. The agency has two units that
are staffed by line staff who are licensed, that provide counseling to families impacted by
intrafamilial child sexual abuse.
The mission of these two counseling programs is to specifically work with these families
who present high levels of risk related to the perpetrator's continued access (intent to
silence or minimize the disclosure) and the non-offending parent’s ambivalent response
to the child victim. These two crises limit the family members from benefiting from
treatment that is short term and growing in availability in the community.
This is especially evident now due to the emergence of Trauma-Focused Cognitive
Behavioral Treatment (TFCBT), which is strongly recommended as a treatment approach
that is highly effective in mediating child trauma. The two crises noted above limit
individual family members from benefiting from TFCBT.
The Los Angeles County Department of Children and Family Services supports the
Sexual Abuse Treatment Program so long as the program prepares clients to benefit from
TFCBT by reducing the impact of these crises. The agency benefits by keeping children
in the home of the parent more often than without the service, by returning children who
are placed in out-of-home care faster, and by stopping the cycle of abuse referrals. These
represent Title IV-E Waiver cost savings.
The point is that in treatment, the crises of intra-familial child sexual abuse regarding
perpetrator access, and non-offending parent support must be addressed prior to referring
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
the client family to TFCBT. In the video clip “Johnny’s Story,” the use of TFCBT could
have helped Johnny and his family resolve the trauma after short-term treatment. It is the
time spent resolving the crises of intrafamilial child sexual abuse that CSWs often must
focus on in case management. CSWs also work with specially trained therapists as part
of this process.
Workers should check with their counties and supervisors about treatment in their locale.
Summary of Treatment Issues
Guiding principles for treating intrafamilial sexual abuse should include the use of
consultation, collaboration with adjunct services and external systems, and coordination
among treatment providers. If these guidelines are incorporated into the therapy process
and the family is motivated to pursue treatment, the prognosis for a successful outcome is
good.
The California Victims of Crime Program’s Standards of Care Task Force identified
several general principles in the treatment of intrafamilial abuse. These are as follows:
The safety of the child requires a thorough initial assessment and continuing
vigilance regarding risk. The child’s safety is paramount.
Treatment is best carried out with multiple therapists. This requires coordination,
collaboration, and consultation among several treatment providers.
All family members should have access to therapy, including child victims,
siblings, non-offending parents, and offenders.
The therapist must be able to navigate through multiple systems, including law
enforcement, the courts, and child welfare services.
Children and families often need advocacy as they interact with other agencies
and systems.
Family therapy is an essential component of a successful treatment plan for
intrafamilial abuse, although who to include in sessions and the timing of sessions
requires considerable clinical judgment.
Group therapy is often beneficial in intrafamilial abuse cases to help reduce
isolation, decrease denial, normalize traumatic events, and to encourage peer
group empathy and emotional support.
When parenting ability is impaired (for example, by substance abuse or mental
illness), treatment must include the use of adjunct and consultation services and
referral of the client to appropriate resources.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
Treatment plans may require strategies for contact between the victim and
offender, such as conjoint therapy or monitored visitation.
Common Core | Child Maltreatment Identification, Part 2 | Trainee's Guide
Version 1.15, January 2009
Trainee Content for Day 1, Segment 5, Activity 5B
CRITICAL THINKING IN CHILD WELFARE
ASSESSMENT: SAFETY, RISK AND PROTECTIVE
CAPACITY
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
The trainee applies knowledge of factors associated with child maltreatment in assessing
safety, risk and protective capacity.
The trainee accurately gathers and evaluates relevant information about children and
families to assess safety, risk and protective capacity.
The trainee performs assessments of safety, risk and protective capacity that are informed
by child welfare research and best practice, and that consider issues of personal values,
fairness and equity.
Learning Objectives
Knowledge:
K1.
The trainee will be able to describe the definition of safety as it applies to child
protective services.
K2.
The trainee will be able to describe the definition of risk as it applies to child
protective services.
K3.
The trainee will be able to describe the definition of protective capacity as it
applies to child protective services.
K4.
The trainee will be able to recognize factors correlated with child maltreatment,
including child development, substance abuse and domestic violence.
K5.
The trainee will be able to identify the elements of an effective safety plan.
K6.
The trainee will be able to identify the stages in CWS cases where assessments of
safety, risk, and protective capacity must occur.
Common Core | Critical Thinking in Child Welfare Assessment: Trainee's Guide
Version 1.1, November 2006
Trainee Content for Day 1, Segment 5, Activity 5B
K7.
The trainee will be able to describe the definition of Minimum Sufficient Level of
Care.
K8.
The trainee will be able to identify the factors to consider in assessing for
Minimum Sufficient Level of Care.
Skills:
S1.
Given a case scenario, the trainee will be able to analyze factors relevant to an
assessment of safety, risk, and protective capacity which includes information
from the reporting party, extended family members, case records, and other
collateral sources.
S2.
Given a case scenario, the trainee will be able to articulate his/her assessment of
significant factors - including factors related to culture - and behavioral indicators
related to safety, risk and protective capacity.
S3.
Given a case scenario, the trainee will be able to determine when a safety plan is
needed for a child, and will be able to formulate an effective and viable safety
plan with the family’s involvement.
S4.
Given a case scenario, the trainee will be able to determine when consultation is
necessary to conduct an effective assessment.
Values:
V1.
The trainee will understand how important it is to consider and document the
family’s basic needs, cultural identity, values, strengths and protective capacity
when assessing safety and risk.
V2.
The trainee will value the concept of “minimum sufficient level of care” in
assessing safety and risk, as well as in developing safety plans.
V3.
The trainee will value the role of the community and the family’s social support
network in enhancing safety, decreasing risk and increasing protective capacity.
V4.
The trainee will be aware of how personal values, bias, and countertransference
issues may affect an assessment, and seek appropriate consultation as necessary.
V5.
The trainee will understand how important effective assessments are in
determining appropriate levels of intervention and producing more positive
outcomes for children and families.
V6.
The trainee will value effective methods of engaging culturally and linguistically
diverse families during the assessment process, including basic strategies for
Common Core | Critical Thinking in Child Welfare Assessment: Trainee's Guide
Version 1.1, November 2006
Trainee Content for Day 1, Segment 5, Activity 5B
interviewing that are related to conducting an assessment of safety, risk and
protective capacity.
V7.
The trainee will be able to recognize that children of different ethnicities are
disproportionately represented at the point of entry into the child welfare system
when compared with their percentage in the population at large.
RELATED TITLE IV-E COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student demonstrates the ability to conduct an ethnically and culturally sensitive
assessment of a child and family and to develop an appropriate intervention plan. (1.1)
Student understands the importance of a client’s primary language and supports its use in providing child welfare
assessment and intervention services. (1.2)
Student is able to identify the multiple family and social forces contributing to child
abuse and neglect. (2.1)
Student demonstrates the ability to assess the interaction of factors underlying abuse and
neglect and the capacity to identify strengths that act to preserve the family and protect
the child. (2.2)
Student recognizes and accurately identifies physical, emotional, and behavioral
indicators of child abuse, child neglect and child sexual abuse in children and their
families. (2.3)
Student is able to gather, assess and present pertinent information from interviews, case
records, and other collateral sources required to evaluate an abuse or neglect allegation.
(2.4)
While incorporating knowledge of individual, family, and cultural dynamics, the student
recognizes signs and symptoms of substance abuse in children and adults and is able to
assess its impact. (2.7)
Student recognizes the need to monitor the safety of the child by initial and ongoing
assessment of risk. (2.9)
Common Core | Critical Thinking in Child Welfare Assessment: Trainee's Guide
Version 1.1, November 2006
Trainee Content for Day 1, Segment 5, Activity 5B
Student understands the importance of working together with biological families, foster
families, and kin networks, involving them in assessment and planning and helping them
cope with special stresses and difficulties. (2.14)
Student demonstrates the ability to assess his or her own emotional responses to clients,
co-workers and situations in which the worker’s values are challenged. (2.17)
Student demonstrates skill in interviewing children and adolescents for assessments,
interventions and forensic purposes. (6.4)
Student works collaboratively with biological families, foster families, and kin networks,
involving them in assessment and planning and helping them cope with special stresses
and difficulties. (6.6)
Student demonstrates the ability to recognize potential for violence, suicide, and other
potentially harmful behaviors. (7.2)
Common Core | Critical Thinking in Child Welfare Assessment: Trainee's Guide
Version 1.1, November 2006
CRITICAL THINKING IN CHILD WELFARE
ASSESSEMENT: SAFETY, RISK AND
PROTECTIVE CAPACITY
1. Review the definitions, in the Master Glossary of this
TOL Tool, for risk assessment, safety assessment and
protective capacity. Using one of your cases, have a
discussion on identified risk, identified safety issues
and the protective capacity of the family.
2. Locate and review your Agency’s risk assessment
method or tool. Have a discussion on its strengths
and/or any concerns you have about this method.
3. Use the aforementioned tool to do an assessment on
one of your cases.
4. What does the W&I code say about neglect? Review
the Minimum Sufficient Level of Care handout in your
SW CORE training binder. Have a discussion about
your Agency’s, your community’s and your
supervisor’s standard for neglect of children.
5. Do a ride-a-long on an immediate response referral
that may require a removal decision. Have a
discussion on the risk and safety factors that were
weighed. What cultural factors were considered?
How do you feel, whether you agree with the decision
or not?
6. Locate and review your Agency’s policy on when a
case consultation is mandatory or recommended in the
process of conducting an effective risk and safety
assessment. Using one of your cases, identify who
should be at the table.
7. Personal biases can impact a social worker’s decisionmaking, as well as what information they gather about
a child and family, and what information they pay
attention to and document. Review the handout in the
SW CORE training manual titled, Role of Bias in
Assessment. Using one of your cases, have a
discussion about any personal biases you have that
could affect your decision making in assessing risk
and safety.
8. Using one of your cases, identify the role of
community support and family support in enhancing
safety, reducing risk and increasing protective capacity
DATE
COMPLETED
Trainee Content for Day 1, Segment 5, Activity 5B
Minimum Sufficient Level of Care
Definition of MSLC
The minimum sufficient level of care is the social standard for the minimum of parent
behavior below which a home is inadequate for the care of a child.
Important Considerations in MSLC
MSLC is meant as a minimum, not an ideal. The terms “minimum” and
“sufficient” are crucial to this concept; the standard is related to the objective of
keeping children safe and protected. The terms “minimum” and “sufficient” are
used to explicitly differentiate from higher standards.
MSLC is case specific. A variety of factors must be considered for each child, and
there are no fixed criteria for assessing when a home falls below this minimum
standard. This decision must be made by informed judgment that evaluates each
case individually.
The MSLC must remain consistent for the duration of the case. Once the MSLC
is developed for a given child, it does not change throughout the life of the
family’s case unless the needs of the child change (e.g., child develops a high risk
health condition). When a child is in placement, the decision about reunification
must be based on the same MSLC baselines as when the child was removed.
Factors to consider in assessing MSLC
Although the MSLC is unique for each child, there are commonalities in nearly all
situations. The factors to consider in establishing what the MSLC is for a particular child
include those that relate to:
1.
The child’s needs in the areas of:
Physical care (e.g., safety, protection, food, clothing , shelter, medical and
dental care)
Emotional wellbeing (e.g., attachment between child and caregivers, sense of
security)
Development (e.g., education, special help for children with disabilities)
The key question is, “Are the caregivers providing consistent care at a basic level that
keeps the child safe and protected in the areas of physical, emotional and
developmental needs”?
Common Core | Critical Thinking in Child Welfare Assessment: Trainee's Guide
Version 1.1, November 2006
2.
Contemporary Social Standards
Many social standards now are codified in law, e.g., definitions of child
maltreatment, compulsory school attendance, and child labor. Others are mainly
normative, e.g., expectations for how much work/chores children do in order to
contribute to the family’s well being. Social standards have greatly changed over
the last 100 and even 25-50 years so there is a wide range of accepted social
standards.
The key question is “Are the caregivers’ behaviors within or outside the
commonly accepted child-rearing practices in our society?”
3.
Community Standards
The United States is a highly pluralistic country and many communities have
standards that vary from the “Contemporary Social Standards.” For instance, the
age at which children can have any of the following responsibilities varies:
Caring for younger siblings
Being left alone
Responsibilities for various chores
Working outside the home
Quitting school
There are also wide variations about what is considered appropriate punishment,
e.g., with regard to:
Hitting
Verbally chastising
Length and place for “time outs”
Deprivation, e.g., of
o (favorite) foods,
o social interaction with family and friends
o toys
The importance of “community standards” is explicitly identified in the Indian
Child Welfare Act (ICWA) which mandates that the standards applied to a given
Native American child reflect his tribe’s standards.
The key question is “Are the caregivers’ behaviors within or outside the
commonly accepted child-rearing practices in their community?
The Rationale for using MSLC
The [Rationale] for using Minimum Sufficient Level of Care as a standard includes:8
It maintains the child’s right to safety and permanence while not ignoring the
parents’ right to their children.
It is required by law (as a practical way to interpret the “reasonable efforts”
provision of PL 96-272).
It is possible for parents to reach.
It provides a reference point for decision-makers.
It protects (to some degree) from individual biases and value judgments.
It discourages unnecessary removal from the family home.
It discourages unnecessarily long placements in foster care.
It keeps decision-makers focused on what is the least detrimental alternative
for the child.
It is sensitive across cultures.
Challenges in Applying MSLC
There are challenges in applying MSLC. Often the standard for removal differs from the
standards applied to return a child to the parent’s custody. Sometimes the values and
attitudes of the social worker about what constitutes MSLC can also color the way they
think about a family. Different cultures have different interpretations of what constitutes
the MSLC. Some steps to ensure fairness and equity might include:
Discussing the MSLC during case consultations with a supervisor or a multidisciplinary team.
Taking additional training on how to apply MSLC to cases.
Working in community partnerships to learn more about how different cultures
view MSLC.
Systematically considering what the standard was for removal and what the
expectations are for return of the child, to assure that the standard is not raising
over the life of the case.
8
National CASA © 2002 Chapter 1: Unit 3 Principles & Concepts That Guide CASA/GAL Volunteer Work 1–26
The Role of Bias in Assessment
When conducting assessments, personal biases can impact a social worker’s decisionmaking, as well as what information they gather about a child and family, and what
information they pay attention to and document.
Some examples of bias include:
Bias about kin or community (“the apple doesn’t fall from the tree”).
How children would have a “better life” elsewhere, even though the safety issues
have been addressed by the family.
Bias based on the personal experiences or history of the worker, such as bias
against parents who abuse alcohol by a worker with an alcoholic spouse or parent
(this is often called counter-transference).
Gathering information to “fit” a preconceived assessment or plan for the family or
caregiver.
Remember, bias is often hidden. We are not always aware of our biases, and actions that
a worker may find impartial may be interpreted as biased by someone from a different
community or culture.
FAMILY ENGAGEMENT IN CASE PLANNING
AND CASE MANAGEMENT
- TRAINER’S AND TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
The trainee will understand the dynamics of engaging families in a mutual family
assessment, and comprehensive case planning that includes an assessment of risk/safety
factors, underlying contributing factors to maltreatment, and extensive exploration of
family strengths and resources.
The trainee will develop with the family appropriate, time limited case goals and
objectives, and formulate observable, behavioral measures of these goals and objectives,
and outline all parties’ agreed upon roles, responsibilities, and activities within required
time frames.
The trainee will value the importance of engaging and collaborating with the family and
their resources in strength-based, culturally competent ways towards developing a
comprehensive, family-specific assessment and case plan.
LEARNING OBJECTIVES
Knowledge:
K1. The trainee will be able to identify effective strategies for engaging the family in
the development of the case plan.
K2.
The trainee will be able to identify socioeconomic, cultural and ethnic differences
that may impact the case planning process and the actual plan.
K3.
The trainee will be able to recognize relevant laws and policies that need to be
considered during the case plan process:
a. ICWA (Federal): Indian Child Welfare Act of 1978
b. AB 408 (State): Assembly Bill 408, re: Quality of Life for Foster Children
c. AB 490 (State): Education for children and youth in foster care
d. AB 636 (State): Child Welfare System Improvement and Accountability Act of
2001
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
e. Division 31 regulations (State): CDSS Manual of Policies & Procedures, Sec.
31
f. Concurrent planning
g. Reasonable efforts (reunification)
K4.
The trainee will be able to identify the legal timeframes for case planning
activities.
K5.
The trainee will be able to identify the multiple sources of information necessary
to both develop a comprehensive case plan and monitor a family’s progress
toward case plan goals.
K6.
The trainee will be able to recognize that purposeful and frequent visitation is
highly correlated with successful reunification.
K7.
The trainee will be able to identify the factors necessary in proceeding with CWS
case closures that promote child safety, well-being, and permanency, and also
decrease recurrence of maltreatment and recidivism in CWS.
Skills:
S1.
Given a case scenario, the trainee will be able to articulate the specific
engagement skills the trainee would use to identify and address the strengths,
needs, and cultural considerations of families, and describe the reasons why these
skills are effective in developing the case plan.
S2.
Given a case scenario, the trainee will be able to formulate case plan objectives
that are specific, measurable, achievable, relevant, and time-limited.
S3.
Given a case scenario, the trainee will be able to articulate and present the
reassessment process, which includes updating case plan objectives and amending
case plans with family participation and endorsement.
S4.
Given a case scenario, the trainee will be able to apply “minimum sufficient level
of care” standards to sample case goals and objectives.
S5.
Given a case scenario, the trainee will be able to incorporate socioeconomic and
cultural considerations into the case plan.
S6.
Given a case scenario, the trainee will be able to develop case plans that provide
opportunities for family members to learn and practice new behaviors (case plan
objectives) that provide for the safety, permanency, and well-being of children.
S7.
Given a case scenario, the trainee will be able to successfully complete a written
case plan. (Optional: Trainee will also be able to complete a child welfare
services case plan and case plan family assessment document in CWS/CMS.)
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
S8.
Given a case scenario, the trainee will be able to develop an aftercare plan.
Values:
V1.
The trainee values the importance of jointly developing case plans with children,
youth, and families.
V2.
The trainee understands the importance of an empathetic and non-judgmental
approach when working with families.
RELATED TITLE IV-E COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student demonstrates sensitivity to clients’ differences in culture, ethnicity, and sexual
orientation. (1.1)
Student demonstrates the ability to conduct an ethnically and culturally sensitive
assessment of a child and family and to develop an appropriate intervention plan. (1.2)
Student understands the dual responsibility of the child welfare caseworker to protect
children and to provide services that support families as caregivers. (2.6)
Student understands policy issues and child welfare legal requirements and demonstrates
the capacity to fulfill these requirements in practice. (2.10)
Student understands the principles of concurrent and permanency planning. (2.13)
Student demonstrates the ability to assess his or her own emotional responses to clients,
co-workers, and situations in which the worker’s values are challenged. (2.17)
Student demonstrates the ability to engage and work with involuntary clients. (2.18)
Student is able to engage and assess families from a strengths-based “person in
environment” perspective and to develop and implement a case plan based on this
assessment. (2.19)
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Student understands and utilizes the case manager’s role to create and sustain a helping
system for clients, a system that includes collaborative child welfare work with members
of other disciplines. (2.20)
Student demonstrates knowledge and understanding of the termination process, with
clients and with systems. (2.22)
Student demonstrates understanding of the influence of culture on human behavior and
family dynamics. (3.4)
Student demonstrates understanding of how the strengths perspective and empowerment
approaches can influence growth, development, and behavior change. (3.5)
Student is able to critically evaluate the relevance of intervention models to be applied
with diverse ethnic and cultural populations. (5.2)
Student demonstrates knowledge of the requirements of the Indian Child Welfare Act and
is able to apply its provisions in working with tribal representatives. (5.3)
Student demonstrates knowledge of and the ability to apply the Multi-ethnic Placement
Act. (5.4)
Student demonstrates knowledge of the philosophy, purpose, requirements, and
application of federal and state child welfare policy and legislation. (6.1)
Student demonstrates skill in interviewing children and adolescents for assessments,
interventions, and forensic purposes. (6.4)
Student works collaboratively with biological families, foster families, and kin networks,
involving them in assessment and planning and helping them cope with special stresses
and difficulties. (6.6)
Student understands how to use information, research, and technology to evaluate
practice and program effectiveness, to measure outcomes, and to determine
accountability of services. (8.4)
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
FAMILY ENGAGEMENT IN CASE
PLANNING AND CASE MANAGEMENT
1. Review and discuss the NASW Code of Ethics on
conflict of interest, power and use of authority. (See
booklet in side pocket.) Have a discussion on a case
where there is/was any known or potential conflict of
interest.
2. Review the handout in the trainee binder titled Keys to
Engaging Families. Using one of your cases, have a
discussion on what family engagement
strategies/techniques/words were used or can be used
to engage the family.
3. Identify the methods of formal/informal family group
conferencing used in your county. Attend one and
discuss. Identify one of your cases where family
decision making would be appropriate. Have a
discussion on who should be at the table.
4. Review the handout in the trainee binder titled Quality
of Life Issues AB408 Summary. Locate and review
your Agency’s policies and procedures regarding
Independent Living Skills programs and extra
curricular programs for youth. How are service
needs for youth identified and delivered?
5. Review the handout in the trainee binder titled The
Rationale and Purposes for Case Planning. Using one
of your case plans, if possible, review for S.M.A.R.T.
6. Review the handout in the trainee binder titled
Activity: Fairness and Equity in Case Planning: A
Revealing Child Welfare Exercise. Identify one of
your cases with a family of a different race or culture
than you. Have a discussion around bias and
stereotyping. How might your bias or knowledge of
stereotyping family engagement and case planning?
7. Review the handouts in the SW CORE training binder
titled, California Definition of Concurrent Planning.
Locate and review your agency’s policies and
procedures regarding concurrent planning. Have a
discussion on how to discuss concurrent planning with
the family and with the substitute care provider.
8. Review the handout in the trainee binder titled: ICWA
& You” Locate and review your county’s policies and
procedures on managing ICWA (Indian Child
Welfare) cases? Are there differences from non
ICWA cases?
DATE
COMPLETED
NASW WebEd
Code of Ethics
of the National Association of Social Workers
Approved by the 1996 NASW Delegate Assembly and revised
by the 2008 NASW Delegate Assembly
Order from NASW Press
Preamble
The primary mission of the social work profession is to enhance human wellbeing and help meet the
basic human needs of all people, with particular attention to the needs and empowerment of people who
are vulnerable, oppressed, and living in poverty. A historic and defining feature of social work is the
profession’s focus on individual wellbeing in a social context and the wellbeing of society. Fundamental to
social work is attention to the environmental forces that create, contribute to, and address problems in
living.
Social workers promote social justice and social change with and on behalf of clients. “Clients” is used
inclusively to refer to individuals, families, groups, organizations, and communities. Social workers are
sensitive to cultural and ethnic diversity and strive to end discrimination, oppression, poverty, and other
forms of social injustice. These activities may be in the form of direct practice, community organizing,
supervision, consultation administration, advocacy, social and political action, policy development and
implementation, education, and research and evaluation. Social workers seek to enhance the capacity of
people to address their own needs. Social workers also seek to promote the responsiveness of
organizations, communities, and other social institutions to individuals’ needs and social problems.
The mission of the social work profession is rooted in a set of core values. These core values, embraced
by social workers throughout the profession’s history, are the foundation of social work’s unique purpose
and perspective:
service
social justice
dignity and worth of the person
importance of human relationships
integrity
competence.
This constellation of core values reflects what is unique to the social work profession. Core values, and
the principles that flow from them, must be balanced within the context and complexity of the human
experience.
Purpose of the NASW Code of Ethics
Professional ethics are at the core of social work. The profession has an obligation to articulate its basic
values, ethical principles, and ethical standards. The NASW Code of Ethics sets forth these values,
principles, and standards to guide social workers’ conduct. The Code is relevant to all social workers and
social work students, regardless of their professional functions, the settings in which they work, or the
populations they serve.
The NASW Code of Ethics serves six purposes:
1.
2.
The Code identifies core values on which social work’s mission is based.
The Code summarizes broad ethical principles that reflect the profession’s core values and
establishes a set of specific ethical standards that should be used to guide social work practice.
You can order bulk orders of
the NASW Code of Ethics
from NASW Press.
Code of Ethics, Spanish
language version Codigo de
Etica from NASW Press.
3.
4.
5.
6.
The Code is designed to help social workers identify relevant considerations when professional
obligations conflict or ethical uncertainties arise.
The Code provides ethical standards to which the general public can hold the social work
profession accountable.
The Code socializes practitioners new to the field to social work’s mission, values, ethical
principles, and ethical standards.
The Code articulates standards that the social work profession itself can use to assess whether
social workers have engaged in unethical conduct. NASW has formal procedures to adjudicate
ethics complaints filed against its members.* In subscribing to this Cod, social workers are
required to cooperate in its implementation, participate in NASW adjudication proceedings, and
abide by any NASW disciplinary rulings or sanctions based on it.
The Code offers a set of values, principles, and standards to guide decision making and conduct when
ethical issues arise. It does not provide a set of rules that prescribe how social workers should act in all
situations. Specific applications of the Code must take into account the context in which it is being
considered and the possibility of conflicts among the Code‘s values, principles, and standards. Ethical
responsibilities flow from all human relationships, from the personal and familial to the social and
professional.
Further, the NASW Code of Ethics does not specify which values, principles, and standards are most
important and ought to outweigh others in instances when they conflict. Reasonable differences of
opinion can and do exist among social workers with respect to the ways in which values, ethical
principles, and ethical standards should be rank ordered when they conflict. Ethical decision making in a
given situation must apply the informed judgment of the individual social worker and should also consider
how the issues would be judged in a peer review process where the ethical standards of the profession
would be applied.
Ethical decision making is a process. There are many instances in social work where simple answers are
not available to resolve complex ethical issues. Social workers should take into consideration all the
values, principles, and standards in this Code that are relevant to any situation in which ethical judgment
is warranted. Social workers’ decisions and actions should be consistent with the spirit as well as the
letter of this Code.
In addition to this Code, there are many other sources of information about ethical thinking that may be
useful. Social workers should consider ethical theory and principles generally, social work theory and
research, laws, regulations, agency policies, and other relevant codes of ethics, recognizing that among
codes of ethics social workers should consider the NASW Code of Ethics as their primary source. Social
workers also should be aware of the impact on ethical decision making of their clients’ and their own
personal values and cultural and religious beliefs and practices. They should be aware of any conflicts
between personal and professional values and deal with them responsibly. For additional guidance social
workers should consult the relevant literature on professional ethics and ethical decision making and seek
appropriate consultation when faced with ethical dilemmas. This may involve consultation with an agencybased or social work organization’s ethics committee, a regulatory body, knowledgeable colleagues,
supervisors, or legal counsel.
Instances may arise when social workers’ ethical obligations conflict with agency policies or relevant laws
or regulations. When such conflicts occur, social workers must make a responsible effort to resolve the
conflict in a manner that is consistent with the values, principles, and standards expressed in this Code. If
a reasonable resolution of the conflict does not appear possible, social workers should seek proper
consultation before making a decision.
The NASW Code of Ethics is to be used by NASW and by individuals, agencies, organizations, and
bodies (such as licensing and regulatory boards, professional liability insurance providers, courts of law,
agency boards of directors, government agencies, and other professional groups) that choose to adopt it
or use it as a frame of reference. Violation of standards in this Code does not automatically imply legal
liability or violation of the law. Such determination can only be made in the context of legal and judicial
proceedings. Alleged violations of the Code would be subject to a peer review process. Such processes
are generally separate from legal or administrative procedures and insulated from legal review or
proceedings to allow the profession to counsel and discipline its own members.
A code of ethics cannot guarantee ethical behavior. Moreover, a code of ethics cannot resolve all ethical
issues or disputes or capture the richness and complexity involved in striving to make responsible choices
within a moral community. Rather, a code of ethics sets forth values, ethical principles, and ethical
standards to which professionals aspire and by which their actions can be judged. Social workers’ ethical
behavior should result from their personal commitment to engage in ethical practice. The NASW Code of
Ethics reflects the commitment of all social workers to uphold the profession’s values and to act ethically.
Principles and standards must be applied by individuals of good character who discern moral questions
and, in good faith, seek to make reliable ethical judgments.
Ethical Principles
The following broad ethical principles are based on social work’s core values of service, social justice,
dignity and worth of the person, importance of human relationships, integrity, and competence. These
principles set forth ideals to which all social workers should aspire.
Value: Service
Ethical Principle: Social workers’ primary goal is to help people in need and to address social problems.
Social workers elevate service to others above selfinterest. Social workers draw on their knowledge,
values, and skills to help people in need and to address social problems. Social workers are encouraged
to volunteer some portion of their professional skills with no expectation of significant financial return (pro
bono service).
Value: Social Justice
Ethical Principle: Social workers challenge social injustice.
Social workers pursue social change, particularly with and on behalf of vulnerable and oppressed
individuals and groups of people. Social workers’ social change efforts are focused primarily on issues of
poverty, unemployment, discrimination, and other forms of social injustice. These activities seek to
promote sensitivity to and knowledge about oppression and cultural and ethnic diversity. Social workers
strive to ensure access to needed information, services, and resources; equality of opportunity; and
meaningful participation in decision making for all people.
Value: Dignity and Worth of the Person
Ethical Principle: Social workers respect the inherent dignity and worth of the person.
Social workers treat each person in a caring and respectful fashion, mindful of individual differences and
cultural and ethnic diversity. Social workers promote clients’ socially responsible selfdetermination. Social
workers seek to enhance clients’ capacity and opportunity to change and to address their own needs.
Social workers are cognizant of their dual responsibility to clients and to the broader society. They seek to
resolve conflicts between clients’ interests and the broader society’s interests in a socially responsible
manner consistent with the values, ethical principles, and ethical standards of the profession.
Value: Importance of Human Relationships
Ethical Principle: Social workers recognize the central importance of human relationships.
Social workers understand that relationships between and among people are an important vehicle for
change. Social workers engage people as partners in the helping process. Social workers seek to
strengthen relationships among people in a purposeful effort to promote, restore, maintain, and enhance
the wellbeing of individuals, families, social groups, organizations, and communities.
Value: Integrity
Ethical Principle: Social workers behave in a trustworthy manner.
Social workers are continually aware of the profession’s mission, values, ethical principles, and ethical
standards and practice in a manner consistent with them. Social workers act honestly and responsibly
and promote ethical practices on the part of the organizations with which they are affiliated.
Value: Competence
Ethical Principle: Social workers practice within their areas of competence and develop and enhance
their professional expertise.
Social workers continually strive to increase their professional knowledge and skills and to apply them in
practice. Social workers should aspire to contribute to the knowledge base of the profession.
Ethical Standards
The following ethical standards are relevant to the professional activities of all social workers. These
standards concern (1) social workers’ ethical responsibilities to clients, (2) social workers’ ethical
responsibilities to colleagues, (3) social workers’ ethical responsibilities in practice settings, (4) social
workers’ ethical responsibilities as professionals, (5) social workers’ ethical responsibilities to the social
work profession, and (6) social workers’ ethical responsibilities to the broader society.
Some of the standards that follow are enforceable guidelines for professional conduct, and some are
aspirational. The extent to which each standard is enforceable is a matter of professional judgment to be
exercised by those responsible for reviewing alleged violations of ethical standards.
1. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES TO CLIENTS
1.01 Commitment to Clients
Social workers’ primary responsibility is to promote the wellbeing of clients. In general, clients’ interests
are primary. However, social workers’ responsibility to the larger society or specific legal obligations may
on limited occasions supersede the loyalty owed clients, and clients should be so advised. (Examples
include when a social worker is required by law to report that a client has abused a child or has
threatened to harm self or others.)
1.02 SelfDetermination
Social workers respect and promote the right of clients to selfdetermination and assist clients in their
efforts to identify and clarify their goals. Social workers may limit clients’ right to selfdetermination when,
in the social workers’ professional judgment, clients’ actions or potential actions pose a serious,
foreseeable, and imminent risk to themselves or others.
1.03 Informed Consent
(a) Social workers should provide services to clients only in the context of a professional relationship
based, when appropriate, on valid informed consent. Social workers should use clear and understandable
language to inform clients of the purpose of the services, risks related to the services, limits to services
because of the requirements of a thirdparty payer, relevant costs, reasonable alternatives, clients’ right to
refuse or withdraw consent, and the time frame covered by the consent. Social workers should provide
clients with an opportunity to ask questions.
(b) In instances when clients are not literate or have difficulty understanding the primary language used in
the practice setting, social workers should take steps to ensure clients’ comprehension. This may include
providing clients with a detailed verbal explanation or arranging for a qualified interpreter or translator
whenever possible.
(c) In instances when clients lack the capacity to provide informed consent, social workers should protect
clients’ interests by seeking permission from an appropriate third party, informing clients consistent with
the clients’ level of understanding. In such instances social workers should seek to ensure that the third
party acts in a manner consistent with clients’ wishes and interests. Social workers should take
reasonable steps to enhance such clients’ ability to give informed consent.
(d) In instances when clients are receiving services involuntarily, social workers should provide
information about the nature and extent of services and about the extent of clients’ right to refuse service.
(e) Social workers who provide services via electronic media (such as computer, telephone, radio, and
television) should inform recipients of the limitations and risks associated with such services.
(f) Social workers should obtain clients’ informed consent before audiotaping or videotaping clients or
permitting observation of services to clients by a third party.
1.04 Competence
(a) Social workers should provide services and represent themselves as competent only within the
boundaries of their education, training, license, certification, consultation received, supervised
experience, or other relevant professional experience.
(b) Social workers should provide services in substantive areas or use intervention techniques or
approaches that are new to them only after engaging in appropriate study, training, consultation, and
supervision from people who are competent in those interventions or techniques.
(c) When generally recognized standards do not exist with respect to an emerging area of practice, social
workers should exercise careful judgment and take responsible steps (including appropriate education,
research, training, consultation, and supervision) to ensure the competence of their work and to protect
clients from harm.
1.05 Cultural Competence and Social Diversity
(a) Social workers should understand culture and its function in human behavior and society, recognizing
the strengths that exist in all cultures.
(b) Social workers should have a knowledge base of their clients’ cultures and be able to demonstrate
competence in the provision of services that are sensitive to clients’ cultures and to differences among
people and cultural groups.
(c) Social workers should obtain education about and seek to understand the nature of social diversity
and oppression with respect to race, ethnicity, national origin, color, sex, sexual orientation, gender
identity or expression, age, marital status, political belief, religion, immigration status, and mental or
physical disability.
1.06 Conflicts of Interest
(a) Social workers should be alert to and avoid conflicts of interest that interfere with the exercise of
professional discretion and impartial judgment. Social workers should inform clients when a real or
potential conflict of interest arises and take reasonable steps to resolve the issue in a manner that makes
the clients’ interests primary and protects clients’ interests to the greatest extent possible. In some cases,
protecting clients’ interests may require termination of the professional relationship with proper referral of
the client.
(b) Social workers should not take unfair advantage of any professional relationship or exploit others to
further their personal, religious, political, or business interests.
(c) Social workers should not engage in dual or multiple relationships with clients or former clients in
which there is a risk of exploitation or potential harm to the client. In instances when dual or multiple
relationships are unavoidable, social workers should take steps to protect clients and are responsible for
setting clear, appropriate, and culturally sensitive boundaries. (Dual or multiple relationships occur when
social workers relate to clients in more than one relationship, whether professional, social, or business.
Dual or multiple relationships can occur simultaneously or consecutively.)
(d) When social workers provide services to two or more people who have a relationship with each other
(for example, couples, family members), social workers should clarify with all parties which individuals will
be considered clients and the nature of social workers’ professional obligations to the various individuals
who are receiving services. Social workers who anticipate a conflict of interest among the individuals
receiving services or who anticipate having to perform in potentially conflicting roles (for example, when a
social worker is asked to testify in a child custody dispute or divorce proceedings involving clients) should
clarify their role with the parties involved and take appropriate action to minimize any conflict of interest.
1.07 Privacy and Confidentiality
(a) Social workers should respect clients’ right to privacy. Social workers should not solicit private
information from clients unless it is essential to providing services or conducting social work evaluation or
research. Once private information is shared, standards of confidentiality apply.
(b) Social workers may disclose confidential information when appropriate with valid consent from a client
or a person legally authorized to consent on behalf of a client.
(c) Social workers should protect the confidentiality of all information obtained in the course of
professional service, except for compelling professional reasons. The general expectation that social
workers will keep information confidential does not apply when disclosure is necessary to prevent serious,
foreseeable, and imminent harm to a client or other identifiable person. In all instances, social workers
should disclose the least amount of confidential information necessary to achieve the desired purpose;
only information that is directly relevant to the purpose for which the disclosure is made should be
revealed.
(d) Social workers should inform clients, to the extent possible, about the disclosure of confidential
information and the potential consequences, when feasible before the disclosure is made. This applies
whether social workers disclose confidential information on the basis of a legal requirement or client
consent.
(e) Social workers should discuss with clients and other interested parties the nature of confidentiality and
limitations of clients’ right to confidentiality. Social workers should review with clients circumstances
where confidential information may be requested and where disclosure of confidential information may be
legally required. This discussion should occur as soon as possible in the social workerclient relationship
and as needed throughout the course of the relationship.
(f) When social workers provide counseling services to families, couples, or groups, social workers should
seek agreement among the parties involved concerning each individual’s right to confidentiality and
obligation to preserve the confidentiality of information shared by others. Social workers should inform
participants in family, couples, or group counseling that social workers cannot guarantee that all
participants will honor such agreements.
(g) Social workers should inform clients involved in family, couples, marital, or group counseling of the
social worker’s, employer’s, and agency’s policy concerning the social worker’s disclosure of confidential
information among the parties involved in the counseling.
(h) Social workers should not disclose confidential information to thirdparty payers unless clients have
authorized such disclosure.
(i) Social workers should not discuss confidential information in any setting unless privacy can be
ensured. Social workers should not discuss confidential information in public or semipublic areas such as
hallways, waiting rooms, elevators, and restaurants.
(j) Social workers should protect the confidentiality of clients during legal proceedings to the extent
permitted by law. When a court of law or other legally authorized body orders social workers to disclose
confidential or privileged information without a client’s consent and such disclosure could cause harm to
the client, social workers should request that the court withdraw the order or limit the order as narrowly as
possible or maintain the records under seal, unavailable for public inspection.
(k) Social workers should protect the confidentiality of clients when responding to requests from members
of the media.
(l) Social workers should protect the confidentiality of clients’ written and electronic records and other
sensitive information. Social workers should take reasonable steps to ensure that clients’ records are
stored in a secure location and that clients’ records are not available to others who are not authorized to
have access.
(m) Social workers should take precautions to ensure and maintain the confidentiality of information
transmitted to other parties through the use of computers, electronic mail, facsimile machines, telephones
and telephone answering machines, and other electronic or computer technology. Disclosure of
identifying information should be avoided whenever possible.
(n) Social workers should transfer or dispose of clients’ records in a manner that protects clients’
confidentiality and is consistent with state statutes governing records and social work licensure.
(o) Social workers should take reasonable precautions to protect client confidentiality in the event of the
social worker’s termination of practice, incapacitation, or death.
(p) Social workers should not disclose identifying information when discussing clients for teaching or
training purposes unless the client has consented to disclosure of confidential information.
(q) Social workers should not disclose identifying information when discussing clients with consultants
unless the client has consented to disclosure of confidential information or there is a compelling need for
such disclosure.
(r) Social workers should protect the confidentiality of deceased clients consistent with the preceding
standards.
1.08 Access to Records
(a) Social workers should provide clients with reasonable access to records concerning the clients. Social
workers who are concerned that clients’ access to their records could cause serious misunderstanding or
harm to the client should provide assistance in interpreting the records and consultation with the client
regarding the records. Social workers should limit clients’ access to their records, or portions of their
records, only in exceptional circumstances when there is compelling evidence that such access would
cause serious harm to the client. Both clients’ requests and the rationale for withholding some or all of the
record should be documented in clients’ files.
(b) When providing clients with access to their records, social workers should take steps to protect the
confidentiality of other individuals identified or discussed in such records.
1.09 Sexual Relationships
(a) Social workers should under no circumstances engage in sexual activities or sexual contact with
current clients, whether such contact is consensual or forced.
(b) Social workers should not engage in sexual activities or sexual contact with clients’ relatives or other
individuals with whom clients maintain a close personal relationship when there is a risk of exploitation or
potential harm to the client. Sexual activity or sexual contact with clients’ relatives or other individuals with
whom clients maintain a personal relationship has the potential to be harmful to the client and may make
it difficult for the social worker and client to maintain appropriate professional boundaries. Social
workers—not their clients, their clients’ relatives, or other individuals with whom the client maintains a
personal relationship—assume the full burden for setting clear, appropriate, and culturally sensitive
boundaries.
(c) Social workers should not engage in sexual activities or sexual contact with former clients because of
the potential for harm to the client. If social workers engage in conduct contrary to this prohibition or claim
that an exception to this prohibition is warranted because of extraordinary circumstances, it is social
workers—not their clients—who assume the full burden of demonstrating that the former client has not
been exploited, coerced, or manipulated, intentionally or unintentionally.
(d) Social workers should not provide clinical services to individuals with whom they have had a prior
sexual relationship. Providing clinical services to a former sexual partner has the potential to be harmful
to the individual and is likely to make it difficult for the social worker and individual to maintain appropriate
professional boundaries.
1.10 Physical Contact
Social workers should not engage in physical contact with clients when there is a possibility of
psychological harm to the client as a result of the contact (such as cradling or caressing clients). Social
workers who engage in appropriate physical contact with clients are responsible for setting clear,
appropriate, and culturally sensitive boundaries that govern such physical contact.
1.11 Sexual Harassment
Social workers should not sexually harass clients. Sexual harassment includes sexual advances, sexual
solicitation, requests for sexual favors, and other verbal or physical conduct of a sexual nature.
1.12 Derogatory Language
Social workers should not use derogatory language in their written or verbal communications to or about
clients. Social workers should use accurate and respectful language in all communications to and about
clients.
1.13 Payment for Services
(a) When setting fees, social workers should ensure that the fees are fair, reasonable, and commensurate
with the services performed. Consideration should be given to clients’ ability to pay.
(b) Social workers should avoid accepting goods or services from clients as payment for professional
services. Bartering arrangements, particularly involving services, create the potential for conflicts of
interest, exploitation, and inappropriate boundaries in social workers’ relationships with clients. Social
workers should explore and may participate in bartering only in very limited circumstances when it can be
demonstrated that such arrangements are an accepted practice among professionals in the local
community, considered to be essential for the provision of services, negotiated without coercion, and
entered into at the client’s initiative and with the client’s informed consent. Social workers who accept
goods or services from clients as payment for professional services assume the full burden of
demonstrating that this arrangement will not be detrimental to the client or the professional relationship.
(c) Social workers should not solicit a private fee or other remuneration for providing services to clients
who are entitled to such available services through the social workers’ employer or agency.
1.14 Clients Who Lack DecisionMaking Capacity
When social workers act on behalf of clients who lack the capacity to make informed decisions, social
workers should take reasonable steps to safeguard the interests and rights of those clients.
1.15 Interruption of Services
Social workers should make reasonable efforts to ensure continuity of services in the event that services
are interrupted by factors such as unavailability, relocation, illness, disability, or death.
1.16 Termination of Services
(a) Social workers should terminate services to clients and professional relationships with them when
such services and
relationships are no longer required or no longer serve the clients’ needs or interests.
(b) Social workers should take reasonable steps to avoid abandoning clients who are still in need of
services. Social workers should withdraw services precipitously only under unusual circumstances, giving
careful consideration to all factors in the situation and taking care to minimize possible adverse effects.
Social workers should assist in making appropriate arrangements for continuation of services when
necessary.
(c) Social workers in feeforservice settings may terminate services to clients who are not paying an
overdue balance if the financial contractual arrangements have been made clear to the client, if the client
does not pose an imminent danger to self or others, and if the clinical and other consequences of the
current nonpayment have been addressed and discussed with the client.
(d) Social workers should not terminate services to pursue a social, financial, or sexual relationship with a
client.
(e) Social workers who anticipate the termination or interruption of services to clients should notify clients
promptly and seek the transfer, referral, or continuation of services in relation to the clients’ needs and
preferences.
(f) Social workers who are leaving an employment setting should inform clients of appropriate options for
the continuation of services and of the benefits and risks of the options.
2. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES TO
COLLEAGUES
2.01 Respect
(a) Social workers should treat colleagues with respect and should represent accurately and fairly the
qualifications, views, and obligations of colleagues.
(b) Social workers should avoid unwarranted negative criticism of colleagues in communications with
clients or with other professionals. Unwarranted negative criticism may include demeaning comments that
refer to colleagues’ level of competence or to individuals’ attributes such as race, ethnicity, national origin,
color, sex, sexual orientation, gender identity or expression, age, marital status, political belief, religion,
immigration status, and mental or physical disability.
(c) Social workers should cooperate with social work colleagues and with colleagues of other professions
when such cooperation serves the wellbeing of clients.
2.02 Confidentiality
Social workers should respect confidential information shared by colleagues in the course of their
professional relationships and transactions. Social workers should ensure that such colleagues
understand social workers’ obligation to respect confidentiality and any exceptions related to it.
2.03 Interdisciplinary Collaboration
(a) Social workers who are members of an interdisciplinary team should participate in and contribute to
decisions that affect the wellbeing of clients by drawing on the perspectives, values, and experiences of
the social work profession. Professional and ethical obligations of the interdisciplinary team as a whole
and of its individual members should be clearly established.
(b) Social workers for whom a team decision raises ethical concerns should attempt to resolve the
disagreement through appropriate channels. If the disagreement cannot be resolved, social workers
should pursue other avenues to address their concerns consistent with client wellbeing.
2.04 Disputes Involving Colleagues
(a) Social workers should not take advantage of a dispute between a colleague and an employer to obtain
a position or otherwise advance the social workers’ own interests.
(b) Social workers should not exploit clients in disputes with colleagues or engage clients in any
inappropriate discussion of conflicts between social workers and their colleagues.
2.05 Consultation
(a) Social workers should seek the advice and counsel of colleagues whenever such consultation is in the
best interests of clients.
(b) Social workers should keep themselves informed about colleagues’ areas of expertise and
competencies. Social workers should seek consultation only from colleagues who have demonstrated
knowledge, expertise, and competence related to the subject of the consultation.
(c) When consulting with colleagues about clients, social workers should disclose the least amount of
information necessary to achieve the purposes of the consultation.
2.06 Referral for Services
(a) Social workers should refer clients to other professionals when the other professionals’ specialized
knowledge or expertise is needed to serve clients fully or when social workers believe that they are not
being effective or making reasonable progress with clients and that additional service is required.
(b) Social workers who refer clients to other professionals should take appropriate steps to facilitate an
orderly transfer of responsibility. Social workers who refer clients to other professionals should disclose,
with clients’ consent, all pertinent information to the new service providers.
(c) Social workers are prohibited from giving or receiving payment for a referral when no professional
service is provided by the referring social worker.
2.07 Sexual Relationships
(a) Social workers who function as supervisors or educators should not engage in sexual activities or
contact with supervisees, students, trainees, or other colleagues over whom they exercise professional
authority.
(b) Social workers should avoid engaging in sexual relationships with colleagues when there is potential
for a conflict of interest. Social workers who become involved in, or anticipate becoming involved in, a
sexual relationship with a colleague have a duty to transfer professional responsibilities, when necessary,
to avoid a conflict of interest.
2.08 Sexual Harassment
Social workers should not sexually harass supervisees, students, trainees, or colleagues. Sexual
harassment includes sexual advances, sexual solicitation, requests for sexual favors, and other verbal or
physical conduct of a sexual nature.
2.09 Impairment of Colleagues
(a) Social workers who have direct knowledge of a social work colleague’s impairment that is due to
personal problems, psychosocial distress, substance abuse, or mental health difficulties and that
interferes
with practice effectiveness should consult with that colleague when feasible and assist the colleague in
taking remedial action.
(b) Social workers who believe that a social work colleague’s impairment interferes with practice
effectiveness and that the colleague has not taken adequate steps to address the impairment should take
action through appropriate channels established by employers, agencies, NASW, licensing and regulatory
bodies, and other professional organizations.
2.10 Incompetence of Colleagues
(a) Social workers who have direct knowledge of a social work colleague’s incompetence should consult
with that colleague when feasible and assist the colleague in taking remedial action.
(b) Social workers who believe that a social work colleague is incompetent and has not taken adequate
steps to address the incompetence should take action through appropriate channels established by
employers, agencies, NASW, licensing and regulatory bodies, and other professional organizations.
2.11 Unethical Conduct of Colleagues
(a) Social workers should take adequate measures to discourage, prevent, expose, and correct the
unethical conduct of colleagues.
(b) Social workers should be knowledgeable about established policies and procedures for handling
concerns about colleagues’ unethical behavior. Social workers should be familiar with national, state, and
local procedures for handling ethics complaints. These include policies and procedures created by
NASW, licensing and regulatory bodies, employers, agencies, and other professional organizations.
(c) Social workers who believe that a colleague has acted unethically should seek resolution by
discussing their concerns with the colleague when feasible and when such discussion is likely to be
productive.
(d) When necessary, social workers who believe that a colleague has acted unethically should take action
through appropriate formal channels (such as contacting a state licensing board or regulatory body, an
NASW committee on inquiry, or other professional ethics committees).
(e) Social workers should defend and assist colleagues who are unjustly charged with unethical conduct.
3. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES IN
PRACTICE SETTINGS
3.01 Supervision and Consultation
(a) Social workers who provide supervision or consultation should have the necessary knowledge and
skill to supervise or consult appropriately and should do so only within their areas of knowledge and
competence.
(b) Social workers who provide supervision or consultation are responsible for setting clear, appropriate,
and culturally sensitive boundaries.
(c) Social workers should not engage in any dual or multiple relationships with supervisees in which there
is a risk of exploitation of or potential harm to the supervisee.
(d) Social workers who provide supervision should evaluate supervisees’ performance in a manner that is
fair and respectful.
3.02 Education and Training
(a) Social workers who function as educators, field instructors for students, or trainers should provide
instruction only within their areas of knowledge and competence and should provide instruction based on
the most current information and knowledge available in the profession.
(b) Social workers who function as educators or field instructors for students should evaluate students’
performance in a manner that is fair and respectful.
(c) Social workers who function as educators or field instructors for students should take reasonable
steps to ensure that clients are routinely informed when services are being provided by students.
(d) Social workers who function as educators or field instructors for students should not engage in any
dual or multiple relationships with students in which there is a risk of exploitation or potential harm to the
student. Social work educators and field instructors are responsible for setting clear, appropriate, and
culturally sensitive boundaries.
3.03 Performance Evaluation
Social workers who have responsibility for evaluating the performance of others should fulfill such
responsibility in a fair and considerate manner and on the basis of clearly stated criteria.
3.04 Client Records
(a) Social workers should take reasonable steps to ensure that documentation in records is accurate and
reflects the services provided.
(b) Social workers should include sufficient and timely documentation in records to facilitate the delivery
of services and to ensure continuity of services provided to clients in the future.
(c) Social workers’ documentation should protect clients’ privacy to the extent that is possible and
appropriate and should include only information that is directly relevant to the delivery of services.
(d) Social workers should store records following the termination of services to ensure reasonable future
access. Records should be maintained for the number of years required by state statutes or relevant
contracts.
3.05 Billing
Social workers should establish and maintain billing practices that accurately reflect the nature and extent
of services provided and that identify who provided the service in the practice setting.
3.06 Client Transfer
(a) When an individual who is receiving services from another agency or colleague contacts a social
worker for services, the social worker should carefully consider the client’s needs before agreeing to
provide services. To minimize possible confusion and conflict, social workers should discuss with
potential clients the nature of the clients’ current relationship with other service providers and the
implications, including possible benefits or risks, of entering into a relationship with a new service
provider.
(b) If a new client has been served by another agency or colleague, social workers should discuss with
the client whether consultation with the previous service provider is in the client’s best interest.
3.07 Administration
(a) Social work administrators should advocate within and outside their agencies for adequate resources
to meet clients’ needs.
(b) Social workers should advocate for resource allocation procedures that are open and fair. When not
all clients’ needs can be met, an
allocation procedure should be developed that is nondiscriminatory and based on appropriate and
consistently applied principles.
(c) Social workers who are administrators should take reasonable steps to ensure that adequate agency
or organizational resources are available to provide appropriate staff supervision.
(d) Social work administrators should take reasonable steps to ensure that the working environment for
which they are responsible is consistent with and encourages compliance with the NASW Code of Ethics.
Social work administrators should take reasonable steps to eliminate any conditions in their organizations
that violate, interfere with, or discourage compliance with the Code.
3.08 Continuing Education and Staff Development
Social work administrators and supervisors should take reasonable steps to provide or arrange for
continuing education and staff development for all staff for whom they are responsible. Continuing
education and staff development should address current knowledge and emerging developments related
to social work practice and ethics.
3.09 Commitments to Employers
(a) Social workers generally should adhere to commitments made to employers and employing
organizations.
(b) Social workers should work to improve employing agencies’ policies and procedures and the
efficiency and effectiveness of their services.
(c) Social workers should take reasonable steps to ensure that employers are aware of social workers’
ethical obligations as set forth in the NASW Code of Ethics and of the implications of those obligations for
social work practice.
(d) Social workers should not allow an employing organization’s policies, procedures, regulations, or
administrative orders to interfere with their ethical practice of social work. Social workers should take
reasonable steps to ensure that their employing organizations’ practices are consistent with the NASW
Code of Ethics.
(e) Social workers should act to prevent and eliminate discrimination in the employing organization’s work
assignments and in its employment policies and practices.
(f) Social workers should accept employment or arrange student field placements only in organizations
that exercise fair personnel practices.
(g) Social workers should be diligent stewards of the resources of their employing organizations, wisely
conserving funds where appropriate and never misappropriating funds or using them for unintended
purposes.
3.10 LaborManagement Disputes
(a) Social workers may engage in organized action, including the formation of and participation in labor
unions, to improve services to clients and working conditions.
(b) The actions of social workers who are involved in labormanagement disputes, job actions, or labor
strikes should be guided by the profession’s values, ethical principles, and ethical standards. Reasonable
differences of opinion exist among social workers concerning their primary obligation as professionals
during an actual or threatened labor strike or job action. Social workers should carefully examine relevant
issues and their possible impact on clients before deciding on a course of action.
4. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES AS
PROFESSIONALS
4.01 Competence
(a) Social workers should accept responsibility or employment only on the basis of existing competence
or the intention to acquire the necessary competence.
(b) Social workers should strive to become and remain proficient in professional practice and the
performance of professional functions. Social workers should critically examine and keep current with
emerging knowledge relevant to social work. Social workers should routinely review the professional
literature and participate in continuing education relevant to social work practice and social work ethics.
(c) Social workers should base practice on recognized knowledge, including empirically based
knowledge, relevant to social work and social work ethics.
4.02 Discrimination
Social workers should not practice, condone, facilitate, or collaborate with any form of discrimination on
the basis of race, ethnicity, national
origin, color, sex, sexual orientation, gender identity or expression, age, marital status, political belief,
religion, immigration status, or mental or physical disability.
4.03 Private Conduct
Social workers should not permit their private conduct to interfere with their ability to fulfill their
professional responsibilities.
4.04 Dishonesty, Fraud, and Deception
Social workers should not participate in, condone, or be associated with dishonesty, fraud, or deception.
4.05 Impairment
(a) Social workers should not allow their own personal problems, psychosocial distress, legal problems,
substance abuse, or mental health difficulties to interfere with their professional judgment and
performance or to jeopardize the best interests of people for whom they have a professional
responsibility.
(b) Social workers whose personal problems, psychosocial distress, legal problems, substance abuse, or
mental health difficulties interfere with their professional judgment and performance should immediately
seek consultation and take appropriate remedial action by seeking professional help, making adjustments
in workload, terminating practice, or taking any other steps necessary to protect clients and others.
4.06 Misrepresentation
(a) Social workers should make clear distinctions between statements made and actions engaged in as a
private individual and as a representative of the social work profession, a professional social work
organization, or the social worker’s employing agency.
(b) Social workers who speak on behalf of professional social work organizations should accurately
represent the official and authorized positions of the organizations.
(c) Social workers should ensure that their representations to clients, agencies, and the public of
professional qualifications, credentials, education, competence, affiliations, services provided, or results
to be achieved are accurate. Social workers should claim only those relevant professional credentials
they actually possess and take steps to correct any inaccuracies or misrepresentations of their
credentials by others.
4.07 Solicitations
(a) Social workers should not engage in uninvited solicitation of potential clients who, because of their
circumstances, are vulnerable to undue influence, manipulation, or coercion.
(b) Social workers should not engage in solicitation of testimonial endorsements (including solicitation of
consent to use a client’s prior statement as a testimonial endorsement) from current clients or from other
people who, because of their particular circumstances, are vulnerable to undue influence.
4.08 Acknowledging Credit
(a) Social workers should take responsibility and credit, including authorship credit, only for work they
have actually performed and to which they have contributed.
(b) Social workers should honestly acknowledge the work of and the contributions made by others.
5. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES TO THE
SOCIAL WORK PROFESSION
5.01 Integrity of the Profession
(a) Social workers should work toward the maintenance and promotion of high standards of practice.
(b) Social workers should uphold and advance the values, ethics, knowledge, and mission of the
profession. Social workers should protect, enhance, and improve the integrity of the profession through
appropriate study and research, active discussion, and responsible criticism of the profession.
(c) Social workers should contribute time and professional expertise to activities that promote respect for
the value, integrity, and competence of the social work profession. These activities may include teaching,
research, consultation, service, legislative testimony, presentations in the community, and participation in
their professional organizations.
(d) Social workers should contribute to the knowledge base of social work and share with colleagues their
knowledge related to practice, research, and ethics. Social workers should seek to contribute to the
profession’s literature and to share their knowledge at professional meetings and conferences.
(e) Social workers should act to prevent the unauthorized and unqualified practice of social work.
5.02 Evaluation and Research
(a) Social workers should monitor and evaluate policies, the implementation of programs, and practice
interventions.
(b) Social workers should promote and facilitate evaluation and research to contribute to the development
of knowledge.
(c) Social workers should critically examine and keep current with emerging knowledge relevant to social
work and fully use evaluation and research evidence in their professional practice.
(d) Social workers engaged in evaluation or research should carefully consider possible consequences
and should follow guidelines developed for the protection of evaluation and research participants.
Appropriate institutional review boards should be consulted.
(e) Social workers engaged in evaluation or research should obtain voluntary and written informed
consent from participants, when appropriate, without any implied or actual deprivation or penalty for
refusal to participate; without undue inducement to participate; and with due regard for participants’ wellbeing, privacy, and dignity. Informed consent should include information about the nature, extent, and
duration of the participation requested and disclosure of the risks and benefits of participation in the
research.
(f) When evaluation or research participants are incapable of giving informed consent, social workers
should provide an appropriate explanation to the participants, obtain the participants’ assent to the extent
they are able, and obtain written consent from an appropriate proxy.
(g) Social workers should never design or conduct evaluation or research that does not use consent
procedures, such as certain forms of naturalistic observation and archival research, unless rigorous and
responsible review of the research has found it to be justified because of its prospective scientific,
educational, or applied value and unless equally effective alternative procedures that do not involve
waiver of consent are not feasible.
(h) Social workers should inform participants of their right to withdraw from evaluation and research at
any time without penalty.
(i) Social workers should take appropriate steps to ensure that participants in evaluation and research
have access to appropriate supportive services.
(j) Social workers engaged in evaluation or research should protect participants from unwarranted
physical or mental distress, harm, danger, or deprivation.
(k) Social workers engaged in the evaluation of services should discuss collected information only for
professional purposes and only with people professionally concerned with this information.
(l) Social workers engaged in evaluation or research should ensure the anonymity or confidentiality of
participants and of the data obtained from them. Social workers should inform participants of any limits of
confidentiality, the measures that will be taken to ensure confidentiality, and when any records containing
research data will be destroyed.
(m) Social workers who report evaluation and research results should protect participants’ confidentiality
by omitting identifying information unless proper consent has been obtained authorizing disclosure.
(n) Social workers should report evaluation and research findings accurately. They should not fabricate or
falsify results and should take steps to correct any errors later found in published data using standard
publication methods.
(o) Social workers engaged in evaluation or research should be alert to and avoid conflicts of interest and
dual relationships with participants, should inform participants when a real or potential conflict of interest
arises, and should take steps to resolve the issue in a manner that makes participants’ interests primary.
(p) Social workers should educate themselves, their students, and their colleagues about responsible
research practices.
6. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES TO THE
BROADER SOCIETY
6.01 Social Welfare
Social workers should promote the general welfare of society, from local to global levels, and the
development of people, their communities, and their environments. Social workers should advocate for
living conditions conducive to the fulfillment of basic human needs and should promote social, economic,
political, and cultural values and institutions that are compatible with the realization of social justice.
6.02 Public Participation
Social workers should facilitate informed participation by the public in shaping social policies and
institutions.
6.03 Public Emergencies
Social workers should provide appropriate professional services in public emergencies to the greatest
extent possible.
6.04 Social and Political Action
(a) Social workers should engage in social and political action that seeks to ensure that all people have
equal access to the resources, employment, services, and opportunities they require to meet their basic
human needs and to develop fully. Social workers should be aware of the impact of the political arena on
practice and should advocate for changes in policy and legislation to improve social conditions in order to
meet basic human needs and promote social justice.
(b) Social workers should act to expand choice and opportunity for all people, with special regard for
vulnerable, disadvantaged, oppressed, and exploited people and groups.
(c) Social workers should promote conditions that encourage respect for cultural and social diversity
within the United States and globally. Social workers should promote policies and practices that
demonstrate respect for difference, support the expansion of cultural knowledge and resources, advocate
for programs and institutions that demonstrate cultural competence, and promote policies that safeguard
the rights of and confirm equity and social justice for all people.
(d) Social workers should act to prevent and eliminate domination of, exploitation of, and discrimination
against any person, group, or class on the basis of race, ethnicity, national origin, color, sex, sexual
orientation, gender identity or expression, age, marital status, political belief, religion, immigration status,
or mental or physical disability.
Top of Page | Print This Page | Contact Us | Privacy Statement
National Association of Social Workers
750 First Street, NE • Suite 700 • Washington, DC 20002-4241
©2008 National Association of Social Workers. All Rights Reserved.
Trainee Content for Day 1, Segment 9, Activity 9A
Keys to Engaging Families
Keys to Engaging
Families
KEYS TO ENGAGING FAMILIES:
KEYS TO ENGAGING
FAMILIES:
Listen for needs,
interests, and
concerns
Define terms of
working
together with
the family using
full disclosure
Assist family
members in
identifying
connections and
strengths
Engagemen
t Skills:
Manage the
use of power
and authority
Demonstrate
warmth, empathy,
and genuineness
as a foundation for
engaging family
members around
concern for child
safety and building
parental capacity
Use active listening
Provide
concrete and
clear
information to
support the
change
process
Motivate and
support
participation
skills
Tune into self and
others (empathy)
Assist families in
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
making their
own case for
change
EMPATHY
Empathy is tuning in to the
way the other person sees
and feels about her
experience and
communicating to her both
your attempt to understand
and your compassion.
Example(s):
Worker: Megi has been in
foster care nearly six
months and she needs
to be someplace
where she can grow
up.
Mother: I know she needs a
home for good. I am
trying! You try kicking
this habit. It is, like, so
hard!
Worker: I know it’s been
tough for you.
Mother : Do you? Do you?
Worker: (pause) You have
always told me that,
even during the worst
of times, you keep
Megi in your heart and
she is your reason to
keep trying to kick
your habit.
PARTIALIZING
Partialzing is helping clients
deal with one problem at a
time or breaking down
complex problems.
Example(s):
Mother: I can’t believe you
guys want me to do
all this stuff right
away!
Worker: Well, let’s go over it
to see the different
parts—it’s probably
not as much as you
might be thinking.
First, we need to be
sure that Leroy is
never left alone. So,
let’s go over the
plan for that again.
What are your
plans?
Mother: I’ll take him over to
this new day care
on my way to work
everyday.
Worker: OK. And how
about if your car
breaks down like last
week?
PAST SUCCESS QUESTIONS
Past success questions are
intended to help the
client to describe specific
times when s/he has had
success in a situation that
could be applicable to a
current concern.
Example(s):
It’s not easy to raise three
children on your own.
How did you do it?
After
having
been
through
what
you’ve
been through, how did
you find enough strength
to keep pushing on?
What do you need to do
so that you’ll feel good
about yourself and in
control again?
What would it take for
you to bring back the
confidence you had
when you were in high
school?
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
REFRAMING
Reframing helps clients
change their way of looking
at problems so that the
positive aspects can be more
clearly seen.
Example(s):
Parent: So, there you have it. I
guess what I am telling
you is yes, I hit Andy
with that strap and yes,
that is how he got the
bruises on his back.
So, I guess you think I
am worse than the
wicked witch of Oz.
Worker: No. I think from what
you told me that you
are trying to find a
way to keep Andy
from touching his sister
in a sexual way. I think
you are concerned
about both of your
kids. I want to help
you find a way to help
them—and punishing
Andy in this way will
likely not stop him from
doing it again. He
needs a different kind
of help.
RECOGNIZING STRENGTHS
Recognizing strengths
involves identifying and
emphasizing what the
client can do to control
safety concerns and
reduce risks.
Example(s):
Father: Well, yes, I do have
some other ways
that I discipline Rory.
I send him to his
room and I use that
chair over there—I
face it to the wall.
Worker : Tell me about a
time you used one
of these ways.
Father: I tried sending him
to his room just
before I had to
spank him—but he
tore up some books
and that’s when I
had to spank him.
Worker: I can see that you
have tried a
different method
and that is a real
strength.
SCALING QUESTIONS
Scaling questions are a
clever way to make
complex features of a
client’s life more concrete
and accessible. Scaling
questions can be used to
assess self-esteem, selfconfidence, investment in
change, perception of
hopefulness, etc. They
usually take the form of
asking the client to give a
number from 0-10 that
best represents where the
client is at some specified
point. Ten (10) is the
positive end of the scale,
one is lower.
Example(s):
Let me ask you, on a
scale of 1 to 10, with 10
standing for ‘as
determined as anybody
can be in your
circumstances to get your
daughter back,’ how
close would you say you
are to 10?
Okay, now this time10
stands for ‘as confident as
anyone can be that you
will get your child to
come back to live with
you.’ Where would you
put yourself on the same
1 to 10 scale?
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
OPEN-ENDED QUESTIONS
When you ask questions that
are an open invitation to say
whatever is on the person’s
mind, it is sometimes amazing
what people will share.
Solutions often begin to
emerge from this type of
processing out loud. This
applies to any question for
which “yes” or “no” or “I don’t
know” are not likely responses.
Example(s):
What else can you tell me
about that?
Tell me about your family
when you were young.
“WHEN…” RATHER THAN
“IF…” QUESTIONS
“When” implies trust that
the person is going to do
something. “If” implies that
they may or may not.
“When” presumes a desire
for, and the possibility of, a
positive outcome. (Revisit
your strength-based
language list.)
Example(s):
When… (you’re not
drinking), how do you feel
in the mornings when it’s
time to get the children off
to school?
When you are in control of
your temper…
When you go to your drug
treatment program…
QUESTIONS THAT BEGIN
WITH “HOW”
These questions tend to
be more solutionoriented, and less likely to
call for blame or
defensive responses than
“why” questions.
Example(s):
How can you tell? How
do you know this?
How did you do it before?
How would that be
helpful to you/ your
family?
How long have you felt
this way?
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
QUESTIONS THAT BEGIN WITH
“WH…”
These questions are solutionoriented and imply the
person’s ability to solve
problems.
Example(s):
Where is the best place for this
to happen?
What would your
children/mother/friend say to
you about this?
Who helped you when…?
What difference would this
make to you?
What would it take…?
What are your thoughts about
this?
What part of this do you agree
with, and disagree with?
Who can you call when you
are feeling that way?
Where can you go when you
decide you want to get help
for that?
STRENGTHS CHAT
This is a normal, informal
conversation seeking
information about the
family’s “Positive Family
Processes.” Responses to
these questions can reveal
strengths the family can rely
on when times get tough or
when there is a crisis.
Example(s):
What do you do for fun?
What does your family do
together?
What is one of your
comforting family
traditions?
What are some things you
like best about your
children?
How do you blow off
steam?
How did you meet your
spouse/significant other?
What is one thing each
week that you really look
forward to doing?
How do you picture yourself
and your family five years
from now?
What is something that
makes you smile when you
think about your family?
EXCEPTION-FINDING
QUESTIONS
Elicit information that
addresses how a
problematic situation
might have been
different. These questions
allow the receiver to talk
about their successes
(strengths). Exceptions
are the building blocks of
success. They shrink the
problem. Exceptions
focus on the possibilities.
Example(s):
Tell me about the times, in
recent days, when you
could have hit Tommy
(screamed at him, called
him names, etc.), but
somehow managed to
handle it differently?
When you are… (not
drinking…), what is
different at home?
Let’s talk about the days
when you do feel safe
and hopeful. What is it
you are doing differently
on those days?
Tell me about the most
recent time when you
could have gotten
stoned, but you didn’t.
How did you manage not
to?
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
COPING QUESTIONS
When dealing with difficult
behaviors or situations, ask
questions in a way that
demonstrates empathy and
compassion. This
acknowledges your
understanding of the pain,
fear or frustration they may be
experiencing.
Example(s):
I imagine these children are a
real handful. I’m sure they
keep you on your toes all day.
What seems to help? That’s
very clever!
How do you do it? Who do
you turn to when you feel you
need help?
How did you manage to stay
sober for a whole week?
Considering how tough this
week has been for you, it must
have been hard to do.
MIRACLE QUESTIONS
These questions ask for
families to disregard their
current troubles and for a
moment imagine what their
lives would be like in a
successful future. It creates
a vivid image or vision of
what life will be like when
the problem is solved and
hope that life can be
different. These questions
are inspirational because
they help to remove
hopelessness.
Example(s):
Suppose one night there is
a miracle while you were
sleeping and your problem
is solved. You don’t know
the miracle has happened.
What will you notice that is
different the next morning
that will tell you that the
problem is solved?
ETHNOGRAPHIC
INTERFVIEWING
Interviewing people
about their cultures helps
us to understand a
significant part of what
influences their goals,
values, problem-solving
approaches, and childrearing behaviors. This
means focusing on their
view of their culture first
and only secondly on
their view about how they
are similar or different
than their culture.
Example(s):
Tell me about how your
______ view physical
punishment of children?
Most groups of people
have ideas about what
children ought to be
doing at various ages. Tell
me what people in your
group think about how
children ought to act by
age 10?
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1, Segment 5, Activity 5A
Quality of Life Issues
AB 408 Summary
Brief overview summary of WIC 362.05 (AB 408)
States that every child adjudged a dependent child of the juvenile court shall be
entitled to participate in age-appropriate extracurricular, enrichment, and social
activities.
This legislation denotes a commitment to having dependent children in out of home
care live as normal a life as possible.
It promotes ability for dependent children to participate in age-appropriate
extracurricular, enrichment and social activities.
WIC 362.05 specificity and expectations
No state or local regulation or policy may prevent or create barriers to participation in
extracurricular, enrichment or social activities.
State and local agencies shall ensure that private agencies that provide foster care
services to dependent children have policies consistent with the provisions of WIC
362.05.
Private agencies must promote and protect the ability of dependent children to
participate in age-appropriate extracurricular, enrichment and social activities.
The caregiver shall take reasonable steps to determine the appropriateness of the
activity in consideration of the dependent child’s care, maturity and developmental
level
Practice implications
Caregivers like parents are now authorized to determine whether to give permission (i.e.,
signing permission slips) for a dependent child to participate in extracurricular,
enrichment, and social activities, including but not limited to:
Attending slumber parties
Participating in sports activities
Going to the mall
Participating in school related extracurricular events
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1, Segment 5, Activity 5A
Ensuring Educational Rights and Stability for Foster Youth—AB 490
Summary
(Youth Law Center/Children’s Law Center of Los Angeles, December 2003)
Effective January 1, 2004, AB 490 (Steinberg), Chapter 862, imposes new duties and
rights related to the education of dependents and wards in foster care. The Act’s key
provisions are as follows:
Establishes legislative intent that foster youth are ensured access to the same
opportunities to meet academic achievement standards to which all students are
held, maintain stable school placements, be placed in the least restrictive
educational placement and, have access to the same academic resources, services
and extracurricular and enrichment activities as all other children. Makes clear
that education and school placement decisions are to be dictated by the best
interest of the child.
Creates school stability for foster children by allowing them to remain in their
school of origin for the duration of the school year when their placement changes
and remaining in the same school are in the child’s best interests.
Requires county placing agencies to promote educational stability by considering
in placement decisions the child’s school attendance area.
Requires Local Educational Agencies (LEAs) to designate a staff person as a
foster care education liaison to ensure proper placement, transfer and enrollment
in school for foster youth.
Makes LEAs and county child welfare workers or probation officers jointly
responsible for the timely transfer of students and their records when a change
of schools occurs.
Requires that a comprehensive public school be considered as the first school
placement option for foster youth.
Provides that a foster child has the right to remain enrolled in and attend his/her
school of origin pending resolution of school placement disputes.
Allows a foster child to be immediately enrolled in school even if all typically
required school records, immunizations, or school uniforms are not available.
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Requires an LEA to deliver the pupil’s education information and records to
the next educational placement within 2 days of receiving a transfer request from
a county placing agency.
Requires school districts to calculate and accept credit for full or partial
coursework satisfactorily completed by the student and earned while attending a
public school, juvenile court school or nonpublic, nonsectarian school.
Authorizes the release of educational records of foster youth to the county
placing agency, for purpose of compliance with WIC 16010, case management
responsibilities required by the Juvenile Court or law, or to assist with transfer or
enrollment of a pupil.
Ensures that foster youth will not be penalized for absences due to placement
changes, court appearances, or related court ordered activities.
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1, Segment 4, Activity 4A
The Rationale and Purposes for Case Planning
1. ROADMAP FOR PERMANENCY
Provide a roadmap for what needs to be done in order to achieve the permanency goal
for the child or youth. The order of preference of permanency goals is:
Remain safely in own home
Return home (reunification)
Adoption with siblings
Adoption
Legal Guardianship with Relatives
Legal Guardianship
Long-Term Foster Care with Relative
Long-Term Foster Care with non-Relative
Stable foster care with emancipation (older youth)
2. TAILOR THE INTERVENTIONS
Ensure that the “intervention reasons” and the “contributing factors” (i.e., why the
child or youth is in the child welfare system) are addressed adequately. The safety
concerns, the risks, and the related needs of the family must be the basis for the
objectives, interventions, and actions described in the plan. The need for a case plan
indicates that the parents’ ability to provide the minimum sufficient level of care
(MSLC) is a concern.
3. S.M.A.R.T.
Ensure that the interventions and actions are prioritized and SMART:
a. Specific (meet the needs of this family given their concerns, strengths, and
culture; includes who is responsible for what)
b. Measurable (vis à vis the objectives)
c. Attainable (reasonable for family to accomplish; doable)
d. Results-oriented (success of interventions and actions is a pathway to the
permanency goal)
e. Time-limited (within the legal deadlines)
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
The Rationale and Purposes for Case Planning (continued)
4. FAMILY INVOLVEMENT
Ensure that the family and the family’s team have opportunity and support for being
involved in developing and implementing the plan, evaluating progress, and revising
the plan as needed.
5. SPECIAL PLAN COMPONENTS
Ensure that special aspects of planning are completed:
a. In the case of removal and placement of children or youth, a placement plan
(including visitation) and a concurrent plan (an alternate permanency goal and a
plan for achieving it, usually involving placement of the child in the home of the
family who is identified in the concurrent plan) can be created.
b. In the case of youth 16 and older who reside in out-of-home care, a Transitional
Independent Living Plan (TILP) can be created.
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1, Segment 7, Activity 7A
Activity: Fairness and Equity in Case Planning: A Revealing Child
Welfare Exercise
(Williams in Anderson, Ryan, & Leashore, 1997)
Carol Williams, DSW, is a former Associate Commissioner for the Children’s
Bureau, Administration on Children, Youth and Families, USDHHS
“In a personal experience at the National Child Welfare Leadership Center, Child
Protective Services administrators went through a decision-making exercise. They were
given brief vignettes in which examples of child maltreatment were presented and the
managers were asked to rank vignettes in terms of the seriousness of the problem that the
families encountered and what could be done to intervene. Did they think it was a minor
problem or a very severe problem? Would they open a case, leave the child in the home,
or place the youngster in out-of-home care?
The vignettes were varied by race and the scores compared. There was no consistency in
decision-making. For example, in one vignette a 3-year-old was left unsupervised and
ingested some cocaine. In the Caucasian vignette, the child was more likely to remain at
home under supervision. In the African American vignette, the child was more likely to
enter out-of-home care. The facts were the same; the race valued and influenced the
choice made. One could not, however, predict the way in which race influenced
decisions. Sometimes race leads to more intrusive interventions. Other times it seems to
normalize unacceptable behavior.
Race is a complex factor in decision-making at every point in the child welfare service
delivery continuum. Attention needs to be paid to decision-making and the impact of
race in regard to the existence of maltreatment, whether children stay at home, what level
and kind of effort is necessary to help families, and what level of effort is called for to
achieve permanence for children. Families and children are served in a system in which
race is a powerful variable in decision-making but is rarely talked about.”
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1 Segment 11, Activity 11A
California Definition of Concurrent Planning
(Adapted from a handout developed by Rose Wentz for this training)
Concurrent planning refers to the process of immediate, simultaneous and continuous
assessment and case plan development that provides for reunification services, with the
concurrent development of an alternative permanent plan for a child in the event that
reunification is not achieved. Concurrent planning includes a continuum of options to
promote early reunification for every child removed from his or her family. Service
planning for concurrent plans is a court/agency/family collaboration which must include
the probability of reunification with the child’s family of origin, availability of extended
family resources, and identification of an alternate family who will commit to providing a
permanent home for the child.
(CDSS, 1997)
State
WIC 16501.1(f)(9)
When goal is reunification, case plan must address both how services will
restore family capacity AND how legal permanency will be achieved,
should reunification fail.
WIC 358.1(b), 366.21(e) & .22(a)
Efforts to achieve legal permanency must be addressed at Disposition
Hearing & in subsequent court reports.
WIC 361.3
All relative caregivers must be assessed on their ability to provide
permanency for a child.
CDSS Division 31-201 Regulations
Order of service priority when determining the case plan goal: FM FR
PP
Permanency priority: Reunification Adoption Legal Guardianship
Prior to termination of reunification services, determine potential for
adoption
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
Trainee Content for Day 1, Segment 6, Activity 6A
“ICWA & You”
(Digest for IndigenousNewsNetwork@topica.com, Issue 494)
What is ICWA?
The Indian Child Welfare Act or ICWA is a law that applies to state, county, and private
child welfare agencies. It covers tribal children from all American Indian and Alaska Native
tribes listed in the Federal Register. ICWA supports Indian tribes’ authority over their
members and the well-being of Indian children and families.
Who is an Indian child?
Under ICWA, a child is Indian if he or she has a mother or father who is a member of an
Indian tribe. The child must also be a member of a tribe or be eligible for membership.
Why is the law only for an Indian child?
History tells us why: Indian tribes are sovereign nations. The federal government has a
unique political relationship with Indian nations through treaties that it does not have with
any other people in the United States.
Why was the law passed?
Countless Indian children have been removed from their families and tribes. Boarding
schools run by the government and other groups kept school-age children away from their
homes. Many Indian children lost their traditions and culture and experienced serious
problems later in life. Often, child welfare agency workers used their own cultural beliefs to
decide if Indian children were being raised properly. Also, many did not understand the
importance of the extended family—relatives other than the mother or father—in bringing up
children in Native cultures. This often resulted in Indian children being improperly removed
from their families and tribes.
Does the law apply to people living away from Indian reservations?
Many people believe that the Indian Child Welfare Act only applies to Indian children living
on reservations. The law applies to ALL Indian children, wherever they live. Therefore, it is
important that child welfare workers assess ancestry of ALL children referred for neglect or
abuse. If known, the child’s tribe must always be notified by certified mail of any court
proceedings involving placing Indian children in foster care, termination of parental rights, or
adoption. Where ancestry is not clear, the Bureau of Indian Affairs should be notified.
Common Core | Case Planning & Case Management | Trainee’s Guide
Version 1.2, March 2007
PLACEMENT & PERMANENCY
- TRAINER'S & TRAINEE’S GUIDES -
CORE COMPETENCIES AND LEARNING OBJECTIVES
CORE COMPETENCIES
Placement of Children and Youth:
The trainee will understand the trainee’s role and responsibilities when placing children
and youth in out-of-home care, as well as the impact of placement on children, youth, and
families.
Working Effectively with Caregivers:
The trainee will understand the benefits to children, youth, and families of forming and
maintaining strength-based partnerships with caregivers and service providers.
Legal Mandates Regarding Placement:
The trainee will understand the legal intent and key elements of public policy, federal
laws, California laws, and regulations specific to placement of children and youth in outof-home care.
Permanency:
The trainee will understand the federally mandated priorities and rationale for
permanency, and how permanency addresses the cultural, developmental, and emotional
needs of children and youth.
The trainee will understand the necessity for cultural understanding and awareness in all
aspects of placement planning and services to support permanency and well-being.
LEARNING OBJECTIVES
Knowledge:
K1.
The trainee will be able to identify the key elements of public policy, federal laws,
California laws, and regulations specific to children and youth placed in out-ofhome care:
a. ASFA (Federal): Adoption and Safe Families Act of 1997
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
b.
c.
d.
e.
f.
g.
h.
i.
j.
k.
MEPA (Federal): Multi-Ethnic Placement Act of 1994
ICWA (Federal): Indian Child Welfare Act of 1978
Relative placement (State: CDSS)
NREFM (CDSS): Non-Relative Extended Family Member placement
Sibling placement (State: W&I Code)
ICPC (State): Interstate Compact on the Placement of Children
SIJS (Federal): Special Immigrant Juvenile Status
AB408 (State): Assembly Bill 408, re: Quality of Life for Foster Children
Foster Children’s Bill of Rights (State: CA Code of Regulations)
Least restrictive environment (Federal): Adoption Assistance and Child
Welfare Act of 1980
l. Institutional abuse (CDSS Manual of Policies & Procedures, Sec. 31)
m. AB490 (State): Education for children and youth in foster care
K2.
The trainee will be able to identify a wide range of behaviors that relate to
separation, including expressions of grief and loss, in children of different
developmental stages and of different cultural backgrounds.
K3.
The trainee will be able to identify cultural factors that influence family
dynamics, parenting, and behavior, as they relate to facilitating adjustment
between the home of the child’s family of origin and out-of-home caregivers.
K4.
The trainee will be able to identify the principles of concurrent planning and
permanency, and their impact on placement decisions for children and youth.
K5.
The trainee will be able to understand the distinction between legal permanency
and emotional permanency.
K6.
The trainee will be able to identify the factors that affect the ability of care
providers to support the well-being of children and youth in all areas of culture,
health, education, visitation, and mental health needs.
K7.
The trainee will be able to understand that purposeful and frequent visitation is
highly correlated with successful reunification.
Skills:
S1.
Given a case scenario, the trainee will be able to demonstrate culturally
appropriate prevention and intervention strategies that will minimize trauma and
long-term negative consequences for children and youth placed in out-of-home
care.
S2.
Given a case scenario, the trainee will be able to apply concurrent planning
guidelines when making placement decisions throughout the life of a case.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
S3.
Given a case scenario, the trainee will know how to engage children, youth, and
families in the process of identification and assessment of permanent
relationships.
S4.
Given a vignette, the trainee will be able to apply at least two interventions that
meet the needs of children and youth placed into families of a different race,
ethnicity, or culture.
Values:
V1.
The trainee values the importance of placing children and youth in the least
restrictive environments that will meet their needs.
V2.
The trainee values the importance of utilizing all available resources and
strategies to engage parents, extended family members, and caregivers to the
fullest extent possible.
V3.
The trainee values the importance of maintaining connections to family, culture,
and support systems to lessen the consequences of grief and loss for children and
youth placed in out-of-home care.
V4.
The trainee values well-being (providing health, education, visitation, and mental
health services within a cultural context) as a critical aspect of placement and
permanence.
V5.
The trainee values adoption/permanency as achievable for all children and youth,
regardless of age or disability.
V6.
The trainee values the importance of recognizing personal biases that may affect
placement and permanency decisions.
RELATED TITLE IV-E CURRICULUM COMPETENCIES
The Title IV-E MSW competencies were developed for the M.S.W. specialization in public
child welfare in California, a two-year full time graduate program. The MSW
competencies may overlap with the common core competencies, but are primarily
designed for a full MSW program. Learning objectives and competencies in the common
core support the MSW Title IV-E competencies, but not all of the IV-E material can be
delivered during an in-service training session. MSW Title IV-E competencies may
therefore be linked to multiple topic areas of the common core.
Student understands the influence and value of traditional, culturally based childrearing
practices and uses this knowledge in working with families. (1.4)
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Student demonstrates the ability to collaborate with individuals, groups, communitybased organizations, and government agencies to advocate for equitable access to
culturally sensitive resources and services. (1.5)
Student is aware of forms and mechanisms of oppression and discrimination pertaining to
low-income and single-parent families and uses this knowledge in providing appropriate
child welfare services. (2.5)
Student understands policy issues and child welfare legal requirements and demonstrates
the capacity to fulfill these requirements in practice. (2.10)
Student understands how attachment, separation, and placement affect a child and family
and how these experiences may influence a child’s physical, cognitive, social and
emotional development. (2.12)
Student understands the principles of concurrent and permanency planning. (2.13)
Student demonstrates the ability to assess his or her own emotional responses to clients,
co-workers and situations in which the worker’s values are challenged. (2.17)
Student demonstrates knowledge of the requirements of the Indian Child Welfare Act and
is able to apply its provisions in working with tribal representatives. (5.3)
Student demonstrates knowledge of and the ability to apply the Multi-ethnic Placement
Act. (5.4)
Student demonstrates knowledge of the philosophy, purpose, requirements, and
application of federal and state child welfare policy and legislation. (6.1)
Student demonstrates the ability to recognize abuse occurring in out-of-home placements
and to take appropriate action to protect children from abuse. (6.2)
Student understands the requirements for effectively serving and making decisions
regarding children with special needs and the balancing of parental and child rights. (6.3)
Student works collaboratively with biological families, foster families, and kin networks,
involving them in assessment and planning and helping them cope with special stresses
and difficulties. (6.6)
Student demonstrates the ability to assess the effects of family transitions and the impact
of becoming a client of the child welfare system. (7.1)
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
PLACEMENT AND PERMANENCY
1. Review the handout in the SW CORE training manual
titled Summary of Laws and Procedures. Locate and
review your Agency’s policies and procedures that
support these.
2. Review the handout in the trainee binder titled
Visitation. Study findings show that visitation is the
biggest factor in determining reunification. Locate
and review your county’s policies and procedures
regarding visitation. What services are available to
families to support visitation?
3. Review the handout in the SW CORE training manual
titled Developmentally Appropriate Visitation
Activities. Supervise a visit on one of your own cases,
if possible. Use the form titled Visitation Plans for the
Cassel Children to plan the visit. Use the form titled
Visitation Observation to document your observations.
4. Review the handout in the trainee binder titled
Relettive/Non-Reletive Extended Family Member
(R/NFEFM). Review the policies, procedures and
resources, in your county, available for out-of-home
care providers. Discuss ways that you can support the
care providers in your cases.
5. Review the handout in the SW CORE training manual
titled Children and Families of Color in the Child
Welfare System. How do your county’s statistics
compare? What policies, procedures and/or best
practices are in place to minimize this disparity of
children of color in placement?
6. Well-Being (providing health, education, visitation,
and mental health services within a cultural context) is
a critical aspect of placement and permanency. Have a
discussion about what you can do to ensure well-being
of the children you work with.
7. Review the handout in the SW CORE training manual
titled Developmental Considerations for Placing
Children and Youth: Using one of your cases, identify
and discuss which key factors of that child’s
Age/Stage are present and/or need assessment.
8. Discuss the need for permanency in a child’s life and
the effects of multiple placements on the child’s
development. What interventions are available in your
county to reduce multiple placements?
DATE
COMPLETED
Trainee Content Day 1, Segment 4, Activity 4A
Summary of Laws and Procedures
Federal
Adoption Assistance and Child Welfare Act of 1980 (PL 96-272)
Reasonable efforts must be made to keep children in their own homes by providing their
families with services. If removal is necessary, children should be placed where their
needs could best be met. The “least restrictive” environment that could meet the child’s
needs should be used (e.g., foster care instead of institutional care). Visitation with
parents should be encouraged.
Indian Child Welfare Act of 1978
Tribes have a significant role in determining where Native American children should be
placed when their parents cannot provide a safe home for them. When a child is removed,
his or her tribe must be contacted.
Family Preservation and Support Act of 1993
Provides funds to prevent placement by enhancing services that promote family strengths
and parenting skills.
Multiethnic Placement Act of 1994
Mandates that race/ethnicity should not be a reason to delay or deny the placement of
children into foster or adoptive care. Thus, if trying to make same-race selection of
caregivers would delay or deny a child a foster or adoptive placement, the child must be
placed where there is a ready home.
Adoption and Safe Families Act of 1997
Addresses the concerns of the permanency planning movement. It reduces the amount of
time that children can be in foster care. Permanency hearings must be held within 12
months of removal.
Special Immigrant Juvenile Status (SIJS):
8 U.S.C. § 1101 (a)(279J), INA § 101(a)(27)(J)
Federal law permits immigrant children who are in the Child Welfare system to apply for
lawful permanent residence (a “green card”) under two conditions: 1) they are in the
custody of the county department due to maltreatment or 2) they have been maltreated by
a U.S. citizen or permanent resident parent or spouse (the latter is a provision of the
Violence Against Women Act). This allows the child/youth to work legally, qualify for
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content Day 1, Segment 4, Activity 4A
Summary of Laws and Procedures (continued)
in-state tuition at college, and avoid deportation. The County can qualify for federal
foster care matching funds. For more information about SIJS, go to:
1. http://www.ilrc.org/sijs.html, and
2. Fact Sheets:
http://www.ilrc.org/resources/sijs/Fact%20sheets%20immigrant%20children.pdf
California
Welfare and Institutions Code, Section 300
This large section of California law pertains to child welfare practice. California has
addressed all federal law by passing similar state laws. Additionally, California has
passed state-specific laws. As child welfare laws are passed in California (Assembly
Bills - AB and Senate Bills - SB), they are codified in Section 300.
Newer California law is often referred to by its AB or SB number, e.g.:
AB 408 (W&I Code Sect. 362.05) seeks to improve quality of life for children and youth
in foster care by insuring access to age-appropriate extracurricular, enrichment, and
social activities. This affects licensing of providers. The intentions of AB408 need to be
part of the case plan for children and youth in care.
AB 490 seeks to insure that children and youth in foster care have opportunities for a
high quality education. After placement, the child/youth has a right to remain in his
school of origin for the duration of the school year. Children and youth in foster care
should attend a mainstream public school program unless they have individualized
educational programs (IEPs) requiring that they attend school elsewhere. See Trainee
Content “Ensuring Educational Rights and Stability for Foster Youth—AB 490
SUMMARY”.
AB 636 focuses on accountability first by fleshing out the mandated federal outcomes of
safety, permanency and well-being. Each county CWS must write an improvement plan,
which in turn must be approved by the Board of Supervisors and a designated community
committee. Collaboration between CWS and community partners must be a central
feature of both the planning process and the improvement plan.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content Day 1, Segment 4, Activity 4A
Summary of Laws and Procedures (continued)
California Department of Social Services Manual of Policies and Procedures,
Section 31 This manual contains the policies and procedures that direct the work of Child
Welfare Services with and on behalf of families.
California Interstate Compact on Placement of Children (CA Family Code Section
7900) All states are part of an interstate compact that is designed to ensure that children
who are placed in another state are in safe and suitable environments. The ICPC defines,
supports, and monitors the processes for sending a child to another state and receiving a
child from another state.
Relative/Non-Relative Extended Family Members Evaluation (California CDSS
Manual Procedural Guide 0100-520.10)
To shorten time to permanency, and to reduce the likelihood of recidivism by assessing
the homes of a child’s relatives and non-relative extended family members as placement
options and placing children in them whenever possible.
Foster Children’s Bill of Rights
Children and youth in out of home care have a set of rights, as well as the right to know
about them and ask questions. The social worker must talk with children/youth at least
once every six months about these rights in ways that they can understand.
http://www.youthlaw.org/Californiafostercareyouthrights
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content for Day 2, Segment 19, Activity 19A
Visitation
The primary purpose of visiting, in most cases, is to allow children to maintain
relationships with their parents, siblings, and others who were close to them prior
to placement. The younger the child, the more frequent the contact must be in
order to maintain relationships. Especially for young children, frequency is much
more important than length. Frequent visitation is linked with reunification.
Visitation is usually important for maintaining family connections even when
reunification is not the permanency goal. Birth family connections allow children
the opportunity to develop permanent positive attachments, preserve these ties,
and learn to maintain long-term relationships. Many youth return to their family
of origin when they age out of the system. Many children are adopted by relatives
and see their birth parents anyway. Some children whose relationships with birth
parents are severed seek them out in adulthood.
Visiting should never be used as a reward or punishment. Changes in visiting
arrangements should reflect assessment of risk to the child and progress toward
achieving the permanency goal, not attempts to reward or punish either the child
or the parents’ behavior.
Visiting should occur in settings that encourage the most natural interaction
between family members, while minimizing any risk to the child that may exist.
It can, and should, include parental and family participation in normally occurring
events in the child’s life (e.g., school conferences, medical appointments, church
programs, and athletic activities).
Supervised visitation is an opportunity for CWS to assess a parent’s progress with
respect to caring for his/her child and also to assist/teach the parent and to observe
how the parent responds. This is critical because the best measure of how well a
parent is doing in being able to provide a safe and nurturing home is the quality of
the parent’s actual interaction with the child.
When parental rights are terminated, and there will not be continuing face-to-face
contact between the parents and the child, consideration should be given to a
goodbye visit between the parents and the child, and a determination must be
made concerning continuing visits between the child and siblings placed
elsewhere.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content for Day 2, Segment 20, Activity 20A
Developmentally Appropriate Visitation Activities*
Stage
Infancy
Developmental Tasks
Toddler
(2-4)
Pre school
(5-7)
Developmentally Related Visitation
Activities
develop primary
attachment
develop object
permanence
basic motor development
word recognition
beginning exploration and
mastery of environment
meet basic needs (cuddling, feeding,
changing)
peek-a-boo games
help with standing, walking; “come to
me” games
name objects, repeat name games;
reading books
taking walks; encourage exploration;
playing together with noisy, colorful,
moving items
develop impulse control
language development
imitation, fantasy play
large motor development
(run, climb, dance, hop)
small motor
coordination
develop sense of time
asserting preferences
making and consistently enforcing
rules
reading simple stories; playing word
games
“let’s pretend” games; encourage
imitative play by doing things
together
playing together at the park; assist in
learning to ride a bike; dance together
to music
draw together; string beads
discuss events in terms of “after
breakfast,” “after lunch,” “before
supper”
allow choices in foods, activities,
clothes worn
gender identification
begin development of
conscience
develop ability to problem
solve
begin concrete perations
(time, space, hierarchy)
be open to discuss boy/girl
differences; be open to discussions of
sex roles; read books about heroes
and heroines together
make and enforce consistent rules;
discuss consequences of behavior
encourage choices in everything
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
School age
(8-12)
Early
adolescence
(13-17)
Late
adolescence
(18-22)
task completion
understanding concept
of rules
school entry
point out cause/effect
plan activities that have a beginning,
middle, and end
play simple games such as
Candyland, Old Maid
shop for school clothes together;
provide records needed for school
entry; visit school together;
accompany child on first day of
school
skill development (in
school, sports, special
interests)
peer group development
team play
develop self awareness
preparation for puberty
help with homework; practice
sports together; show support of
special interests; attend school
conferences/activities
involve peers in visitation activity
attend team activities with child
be able to provide feedback
discuss physical changes expected;
answer questions openly
cope with physical
changes
begin abstract thinking
become independent of
parents
changes in peer group
associations
separation from family
help with attention to personal
appearance (shaving, buying
cosmetics); provide information
plan and discuss future; talk about
politics, religious ideas
help learn to drive; delegate
responsibility
transport to peer activities; include
peers in visitation
encourage independence by action
(help move to apartment, help apply
for a job)
develop life goals
rework own identity and
gender identity
develop capacity for
intimacy
be aware of and tolerate
independence/ dependence conflict
be open to discuss adolescent’s
options, “think through” together
share own experiences as young
adult
* Note: Adapted from Peg Hess, 1981, Working With Birth and Foster Parents: Trainer’s and Trainee’s
Manual. University of Tennessee School of Social Work.
This section was adapted from the Placement and Reunification Curriculum developed by the Institute
for Human Services (IHS).
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Visitation Plans for Cassel Children
Child:___________________
Time frame for this Visitation Plan (number of weeks or months):
People to be included in the visits (parents, siblings, others):
Frequency of visits:
Visit locations:
Visit lengths and times:
Visit activities:
Conditions of visits:
Visits supervised by:
Transportation arrangements:
Other contact (not face-to-face):
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Visitation Observation
Supervisors of visitation should observe and record the following:
Date, time, length, and location of visit
Who participated?
Who supervised? Was supervision observational only or active participation?
Goals of visit
Activities during visit
Assessment of interaction of adult and children
Adult’s recognition of child’s needs
Adult’s ability to meet child’s needs
Adult used help from supervisor as needed
Relevant issues for case plan implementation
Follow-up needed?
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content for Day 2, Segment 14, Activity 14A
Relative/Non-Relative Extended Family Member (R/NREFM)
Relatives are the preferred caregivers for children and shall be considered first for all
children. However, safety and best interest of the child are the criteria for selecting a
placement.
After a child is taken into temporary custody, the worker should ask the parent/legal
guardian and child (if appropriate) to identify relatives and non-relative extended
family members. These people should be contacted and asked if they are interested in
providing a home for the child or helping support the child in another way. If they
are interested in providing a home, they must be willing to be checked for criminal
and child abuse history through two databases: California Law Enforcement
Telecommunication System (CLETS) and Live-Scan. Youth in the home who are
over age 14 must have a Juvenile Automated Index (JAI) records check if there is
reason to believe they have a criminal record. Additionally, all adults who would
have significant contact with the child in this home must make a Criminal Record
Statement (DCFS 5603 form).
Both first degree (grandparents, uncles, aunts, and adult siblings of the child) and
other relatives who request placement will be assessed. First degree relatives have
priority.
The relatives’ ability and interest to take sibling groups should be assessed since this
is the preference for placement of sibling groups.
Despite a relative’s interest, their home does not have to be considered (and thus
assessed) if any prospective caregiver is subject to denial based on criminal
convictions or Child Abuse Central Index information.
Assessments are done by the CWS Permanency Resource Division staff, but the
decision about where to place is made by the case-carrying CWW and/or the
Dependency Investigator (for Pre-Release Investigations).
The approval process has the same standards used to license foster family homes.
Corrective Action Plans (Caps) can be put in place to help the family correct
deficiencies.
Homes must be approved prior to placement, except under certain limited conditions
such as when the decision not to place in the home of a willing relative must be made
with the ARA. The court must be informed.
Counties are required by legislation to help the relative families succeed in providing the
placement.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content for Day 1, Segment 3, Activity 3A
Children and Families of Color in the Child Welfare System
In almost all states, African American children are placed in foster care at twice the
rate of White children.
African American children have significantly longer stays in care than White or
Latino children (accounting for kinship care).
Although Native American children represent .75% of California’s population, they
represent 1.2% of children in care. This disproportionality indicates that more Native
American children would be in care if they represented a greater proportion of the
population.
Children of color are more likely to be placed in foster care than receive in-home
services, even when they have the similar problems and characteristics as White
children.
Children of color and their families receive fewer services overall than White
families.
Children of color have fewer contacts with their biological families than White
children.
Children of color are more likely to enter foster care at a younger age.
African-American children are reunified at half the rate of White children.
White children are four times more likely to be adopted than African-American
children, and twice as likely to be adopted as Latino children.
African American children have the highest rate of re-entry into foster care.
A 2004 study of CASA services showed that the average amount of time a CASA
volunteer spent with a child was 3.2 hours per month but that “the amount of time
spent per child dropped by more than an hour per volunteer” with African-American
children. (from Youth Today)
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Trainee Content Day 1, Segment 9, Activity 9A
Developmental Considerations for Placing Children and Youth: How
the Trauma of Separation Can Affect Children’s Development9
Understanding Separation and Loss—General
Separating children from their parents can have harmful effects upon their development.
The more traumatic the separation, the more likely there will be significant negative
developmental consequences.
Repeated separations interfere with the development of healthy attachments and a child's
ability and willingness to enter into intimate relationships in the future. Children who
have suffered traumatic separations from their parents may also display low self-esteem,
a general distrust of others, mood disorders (including depression and anxiety),
immaturity, and inadequate social skills. Generalized cognitive and language delays are
also highly correlated with early traumatic separation.
When children are removed from their families, the normal attachment of the children to
their parents is disrupted. For this reason, child welfare policies stress the importance of
maintaining children in their own homes whenever possible. When children must be
removed, their relationship with their parents must be maintained through regular and
frequent visitation until they can return home. If reunification is not possible, the child’s
concurrent plan for permanence is used so that the child can form healthy attachments as
soon as possible.
We have all experienced separations and know that they have the potential to be very
painful. Key factors that can contribute to the trauma associated with a separation are:
The degree of significance of the person lost:
The stronger the relationship with the lost person, the greater the likelihood of
trauma. Hence, the loss of a parent is the most traumatic separation a child can
experience.
Whether the separation is temporary or permanent:
Temporary separations, while distressing, are rarely as painful as the permanent
loss of a loved one. Many people are able to survive even lengthy separations if
they are certain that it is not permanent.
9
Adapted from curriculum developed by The Institute for Human Services (IHS)
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Am I the cause of the separation? Guilt:
If a child perceives the self to be the cause of a separation, either through
negligence, an act of commission or inadequacy, normal feelings of loss are
complicated by feelings of guilt and self-blame. This creates additional emotional
distress.
The availability of other meaningful attachments to provide support:
Support from other meaningful relationships helps one cope during the period of
grieving and prevents a feeling of total desolation and emptiness. The absence of
these may create significant additional emotional distress and loneliness.
Since parents are the most important persons in a child's life, the loss of the parents is
extremely traumatic. While most separations in child placement are considered
temporary by the placing agency, in the child's mind, a few weeks is an eternity and a few
months is permanent. For the child in lengthy substitute care, the loss is experienced as if
it were a permanent loss.
Children often do not have the cognitive maturity to understand the reasons for their
removal and placement. Young children often think they are at fault and the separation is
a punishment for some misdeed or wrongdoing. “I was sent away because I was bad.”
Children in placement often feel considerable guilt and perceive themselves to be bad and
unwanted by their families.
When children are placed in foster homes, they are likely to be separated from other
significant people, including neighbors, friends, extended family and siblings. Usual
sources of support and comfort are often not available. The social worker must
remember that a child has a limited view of the world. The child's limited perspective
greatly increases anxiety about even small changes.
Understanding Separation and Loss—By Age/Stages
INFANCY (birth to 18 months)
Cognitive development
The infant has not developed object permanence; when things are out of sight, they
are gone. Even temporary losses of significant caregivers are experienced as total.
They cannot comprehend that mother will be right back.
Infants have short attention spans and memory. They do not understand change; they
only feel it. Because they don’t understand, changes and unfamiliar sensory
experiences (sights, noises, people) frighten them.
They have little or no language ability and cannot communicate, except by crying.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Emotional development
Infants are emotionally dependent upon others for survival, nurturance, and care to
meet their basic needs.
Infants generally form strong attachments to their primary caregiver and develop a
sense of trust in that person. They often cannot be comforted by others when
distressed.
After 5 to 6 months of age, infants can easily discriminate between people and
display anxiety in the presence of unknown persons.
The infant experiences anxiety in the face of change. Emotional stability depends
upon similarity, continuity, and stability in the environment and the continued
presence of their primary caregiver.
Social development
Without language, infants have few ways to communicate their needs. Most
communications are nonverbal. If adults are not familiar with their cues and do not
recognize their distress, their needs may remain unmet.
Social attachments are limited to immediate caregivers and family members.
Infants have immature social skills and do not easily engage in relationships with
unfamiliar persons. Adults must generally initiate and reinforce interactions.
Implications for Separation and Placement
Infants’ cognitive limitations greatly increase their experience of stress. Infants will
be extremely distressed simply by changes in the environment and the absence of
trusted caregivers.
Infants have few internal coping skills. When deprived of adults whom they have
learned to trust and upon whom they can depend, they are more vulnerable to the
effects of internal and external stresses.
The infant experiences the absence of caregivers as immediate, total, and complete.
Infants who have lost their primary caregivers often cannot be comforted by workers,
foster parents, or others.
If separation occurs during the first year, it can interfere with the development of
trust and reciprocal connectedness.
Infants experience their new environment in a sensory manner. Many different smells,
tastes, sounds, and textures can be distressing for them.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Infants’ distress will be lessened if their new environment can be made very
consistent with the old one and if the biological parent(s) can visit regularly,
preferably daily, and provide direct care to the infant in the placement setting.
PRESCHOOL (2 to 5 years)
Cognitive development
The child uses language to communicate but has a limited vocabulary and does not
understand complex words or concepts.
The child does not have a well-developed understanding of time. The child cannot
discriminate between “next week,” “next month,” and “next year.”
The child has difficulty understanding cause and effect and is often unable to discern
how events relate to one another, to explain why things happen or to predict what
may happen next.
The child may display magical thinking and fantasy to explain events. The child may
feel that his actions or thoughts have precipitated events in his environment.
Children at this age display primarily egocentric thinking, and are incapable of
understanding perspectives that are different from their own. Other people's
explanations of events may make no sense, and children stubbornly cling to their own
explanations.
The child may not generalize experiences from one situation to another. For
example, despite the fact that a child’s house and all the child’s friends’ houses have
bathrooms, he/she may still doubt the existence of a bathroom in the foster home.
Emotional development
The child is still dependent on adults to meet emotional and physical needs. The loss
of adult support brings feelings of loneliness, vulnerability and anxiety.
Development of autonomy and a need for self-assertion and control make it extremely
difficult for a child this age to have things “done to the child” by others. When
thwarted by adults, the child is likely to create and engage in battles with adults to
maintain some degree of control.
Social development
The child is beginning to relate to peers in reciprocal, cooperative, and interactive
play. The child relates to adults in playful ways and is capable of forming
attachments with adults other than parents. The child can turn to other adults to meet
needs.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Good and bad acts are defined by their immediate, personal consequences. Children
who are bad are punished; children who are good are rewarded. The child’s selfesteem is often influenced by how good he/she believes him/herself to be.
Cultural expectations regarding how and what the child plays will influence the
child’s play patterns. For example, there are often cultural expectations regarding the
degree to which children are expected to explore their environments.
Implications for Separation and Placement
The child is still essentially dependent and has limited coping abilities. Emotionally
healthy children of this age, however, can turn to substitute caregivers or a known
and trusted worker for help and support during the placement process.
The preschool child is likely to have an inaccurate and distorted perception of the
placement experience. Due to an immature conception of time, any placement of
more than a few weeks is experienced as permanent. Without frequent contact with
the parents, the child may assume that the parents are gone and are not coming back.
The child will often view separation and placement as a punishment for bad behavior.
Egocentric thinking limits children’s understanding. Children cannot understand
that they were taken out of a home because of factors unrelated to them. This selfblame is a threat to the child's self-esteem and increases anxiety.
Because the child cannot generalize experiences from one situation to another, all
new situations are unknown and therefore, more threatening, which greatly increases
the anxiety experienced by the child.
The child will display considerable anxiety about the new home. He/She will be
concerned about being cared for, but may not have adequate language to express the
concerns in detail. His insecurity may be expressed with questions such as, “Do they
have Band-Aids at their house? Does the dog bite children?” Children must be
reassured that they will be fed and clothed and taken care of.
Most often, while verbal reassurances are helpful, the child needs to experience the
environment to feel comfortable in it.
Forced placement, without good preparation, may generate feelings of helplessness
and loss of control, which may interfere with the development of self-directed,
autonomous behavior. Children may learn that they cannot influence the environment
and consequently become placid and unassertive, or engaged in a power struggle
with adults in an attempt to assert and assure their autonomy.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
SCHOOL AGE (6 to 9 years)
Cognitive development
The child has developed cognitively to the stage of concrete operations. Children
understand cause and effect and logical relationships between events. However, they
will have difficulty understanding abstract relationships.
The ability to understand perspectives other than the child’s own is beginning to
develop. Children begin to understand that events occur for which they are not at
fault.
The world is usually experienced in concrete, black and white terms. Children are
most comfortable if the environment is clearly structured and they understand the
rules about how things should be done, and what is right and wrong. Children of this
age are concerned with fairness and often have difficulty accepting ambiguity or
changes in previously defined rules.
Emotional development
The child is a performer. Self-esteem is strongly affected by how well daily activities
are performed, including academics and play activities.
Children may become anxious where there is limited structure or they do not
understand the rules of a situation. If expectations for the child’s behavior are
ambiguous, the child does not know what is right and often feels helpless.
The child’s primary identification is with family. Identity and self-esteem are closely
tied to the child’s perception of their family's worth. If other people talk about the
child’s family in negative terms, this reflects upon the child as well.
Social development
The child can form significant attachments to adults outside the family, and to peers.
The child derives considerable security from belonging to a same-sex social group.
For many children of this age, their circle of friends is the focus of most activities and
social interactions.
The child recognizes that being a foster child is somehow “different” from the other
children, at a time when conformity is very important.
The child’s relationships can be characterized as loyal and exclusive. Children may
have difficulty choosing between relationships with more than one person. The child
may not understand how to love both the biological and foster mother.
At this age a child’s value system has developed to include right and wrong, and
children experience feelings of guilt when they have done something wrong.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Implications for Separation and Placement
The child can develop new attachments and turn to adults for fulfillment of needs. If
previous relationships with unrelated adults have been positive, the child will be
likely to seek out help from adults when needed. This enhances coping abilities and
strategies in stressful situations.
The child's perception of the reason for the separation may be distorted. Children
may verbalize that they are not at fault, particularly if this is reinforced trusted
caregivers. The child will not want to accept that the child’s parents are at fault
either. Self-esteem is closely tied with self-worth, and children need to view
themselves positively. However, in a child’s cognitively concrete world, someone
must be blamed, and often the worker, the agency, or the foster parents are faulted.
The child will compare foster caregivers to biological parents, and the caregivers
will generally lose the competition.
The loss of a child’s peer group and friends may be almost as traumatic as the loss of
parents. Making new friends may be difficult. The child may be embarrassed and
self-conscious about his/her “foster child” status, and feel isolated. Maintaining
contact with the child’s old peer group is helpful.
The child will be very confused if the rules and expectations in the foster home are
different from what the child is used to. Children will be anxious and uncomfortable
until they fully understand what is expected of them.
The child has a better understanding of time. Being out of the home can be tolerated,
if the child understands he/she will eventually return home. Longer periods of stay
may be experienced as permanent. Because children need concreteness, if they
cannot be told exactly when they will return home, anxiety increases.
If the child was placed after some perceived misbehavior, this may cause feelings of
responsibility, guilt and anxiety.
Each placement, in effect, is cross-cultural in that the specific culture of each family
is unique. The degree of difference between the culture of the child's former home
and the child’s foster home will vary and be most pronounced if there are ethnic
differences. The child may experience confusion, hostility, and resentment regarding
these differences.
PRE-ADOLESCENCE (10 to 12 years)
Cognitive development
Most of the child’s thinking is still concrete. However, some preadolescent children
show a beginning ability to think and reason abstractly, and to recognize complex
causes of events.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Children can understand perspectives other than their own. Some children have
developed insight and can recognize and respond to the needs and feelings of others.
They may recognize that their parents have problems that contributed to their need for
placement.
The child’s time perspective is more realistic. Children are able to recall events that
occurred months and years, earlier and can maintain a sense of continuity over time.
The child can generalize experiences from one setting to another. (Understands that
all houses have bathrooms.)
The child understands that rules often change depending upon the situation. The
child can more easily adapt behavior to meet the expectations of different situations.
Emotional development
Self-esteem and identity are still largely tied to the family. Negative comments
regarding the family reflect upon him as well.
The child has increased ability to cope independently for short periods of time. He
can feed, dress, and care for himself and travel independently around the
neighborhood. He can manage some problems and resolve them without assistance
from adults. He still turns to significant adults, however, for approval, support, and
reassurance when things are difficult.
Children by be embarrassed by their foster care status and feel self-conscious about
being different.
The pre-adolescent has integrated cultural information into his/her identity and has
developed pride in his/her heritage. Cultural codes of conduct and values provide
guidance regarding the mastery of several adolescent developmental tasks such as
managing emerging sexuality, becoming independent, and relationships with peers.
Social development
The child’s social world has expanded to include many people outside the family.
Peers are extremely important. Most peer relationships are of the same sex.
Opposite sex friendships exist, but unless the child has been prematurely introduced
to sexuality, these are of no special interest or concern.
The child still needs trusted adults for leadership, support, nurturance, and approval.
“Right” and “wrong” are complicated and evolving concepts. For most children this
age, right and wrong are determined by principles that they believe apply to all people
including their parents. They can begin to understand that their parents have the
capacity to do wrong.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Implications for Separation and Placement
The child has an increased ability to understand the reasons for the separation. With
help, the child may be able to identify the causes of the family disruption and
realistically assess his role in the situation.
The child can benefit from supportive adult intervention, such as casework
counseling, to help sort through feelings about the situation. Some children at this
age are able to acknowledge their anger and ambivalence.
If given permission, the child may be able to establish relationships with caregivers
without feeling disloyal to birth parents.
The child is aware of the perceptions and opinions of other people. Children are
embarrassed and self-conscious about their family’s problems feel inadequate with
respect to their foster care status.
The child may be worried about his family as a unit and may demonstrate
considerable concern for siblings and parents .Children need reassurance that they
are O.K. and are getting the help they need.
The loss of best friends and peers may be particularly difficult for the child. It may be
difficult to replace these relationships in the foster care setting. The child may be
lonely and isolated.
Preadolescents may be preoccupied with fantasies of returning to earlier attachment
figures (primary parents, kin, earlier foster parents). These fantasies can interfere
with the child’s successful attachment and adjustment in the new home.
EARLY ADOLESCENCE (13 to 14 years)
Cognitive development
The adolescent’s emerging ability to think abstractly may make complicated
explanations of reasons for placement more plausible. While some teens may be
developing an ability to understand complicated events, others will not. As with
adults, such ability may depend upon the individual's intellectual potential.
Adolescents may have an increased ability to identify their feelings and to
communicate concerns and distress verbally.
Emotional development
Early adolescence is a time of emotional ups and downs. The teen may experience
frequent mood swings and fluctuations. At its worst, it can be a chaotic time. At best
the teen is still volatile, unpredictable, and emotionally charged.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Physical and hormonal changes, including significant and rapid body changes,
generate a beginning awareness of sexuality. The adolescent experiences many new
feelings, some of which conflict and are contradictory. Emotional changes may be
accompanied by solicitous and exaggerated behavior toward the opposite sex, or
anxious withdrawal.
The adolescent begins to feel a desire to be independent. Independence is expressed
by verbally rejecting parental values and rules and adhering to the values of peers.
Despite a verbalized rejection of adult rules and values, the adolescent experiences
considerable anxiety when deprived of structure, support, and rules.
Social development
The teen may be embarrassed to admit need for adult approval, support, and
nurturance. This makes it difficult for adolescents to enter into relationships with
adults.
The adolescent is status conscious. Much of the teen’s self-esteem is derived from
peer group acceptance and from being in the right peer group. These groups, and
their membership, may change from day to day.
Adolescents may feel a need to keep up appearances and may defend family in public
and to adults, even if they personally believe their parents to be at fault.
The teen is beginning to become aware of social roles, and experiments with different
roles and behaviors. Consistent social role models are needed. Because sexual
identity is becoming an issue, improper sexual behavior on the part of the child’s
parents (sexual abuse, promiscuity) may be of increasing concern.
Although many children will have developed a moral attitude with clearly defined
“rights” and “wrongs,” these values may take a back seat to their friends’ opinions
and attitudes regarding their thoughts and actions.
Implications for Separation and Placement
Early adolescence is an emotionally chaotic period. The teen experiences many
stresses as a result of internal, biological changes and changes in the environment's
expectations for her behavior. Additional stress has the potential of creating a stress
overload situation for the child and may precipitate crisis.
The adolescent may resist relationships with adults and describe adults in
uncomplimentary terms. Adolescents may not be able to admit a need for support,
nurturance, and structure from adults. Without these, however, the adolescent may
flounder and experience considerable anxiety. By rejecting adults, the teen is
deprived of an important source of coping support.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
Adolescents may deny feelings of discomfort and pain. This prevents the them from
constructively coping with these feelings, and they may be expressed through volatile,
sometimes antisocial, behavior.
Separation from parents, especially if the result of family conflict and unruly
behavior on the part of the adolescent, may generate guilt and anxiety.
At a time when identity is an emerging issue, the adolescent may have difficulty in
realistically dealing with shortcomings of the parents. The parents may either be
idealized and their shortcomings denied, or they may be discounted, verbally
criticized, and rejected.
Entry into sexual relationships may be very frightening without the support of a
consistent, understanding adult.
Persistent, repeated attempts to engage the adolescent by the worker can have
positive results. Even if the teen never acknowledges that the worker is of help, they
may greatly benefit from the support and guidance of the worker.
Young adolescents may feel they are unable to “fit in” to their new social
environments, especially if there are obvious cultural differences between the foster
child and his/her peers. This can result in considerable anxiety, and at times
depression. These issues also affect the late stages of adolescent development.
Cultural differences between the young teen’s previous home and the foster home
(such as expectations regarding dress, language, dating, and level of freedom) may
affect the success of the young teen’s placement. The foster parent and caseworker
should talk openly with the youth about these differences and develop ways to help
the youth feel comfortable and “at home.”
MIDDLE ADOLESCENCE (15 to 17 years)
Cognitive development
The adolescent may have the cognitive ability to understand complex reasons for
separation, placement, and family behavior. He/She may understand that things
happen for many reasons, that no one person may be at fault. The ability to be selfaware may be of help in coping with the situation and conflicting feelings about it.
Adolescents are more able to think hypothetically. They can use this ability to plan
for the future and to consider potential outcomes of different strategies.
Emotional development
The adolescent is developing greater self-reliance. He/She is more able to
independently make, or contribute to making, many decisions about life and
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
activities. This helps retain a degree of mastery and control, which helps reduce
anxiety.
The development of positive self-esteem is as dependent upon acceptance by peers of
the opposite sex as it is on being accepted by same-sex peers.
The adolescent is beginning to formulate many beliefs and opinions. Many behaviors
and ways of dealing with situations are tried and adopted or discarded in an attempt to
determine what feels right.
Social development
Opposite-sex relationships are as important as same-sex relationships. Much social
behavior is centered around dating. Group identification is important, but less so.
Individual relationships are becoming more important.
The adolescent is interested in adults as role models. Adolescents will be responsive to
adults who are honest and who will talk about their ideas without enforcing
behavioral expectations or values.
The adolescent is beginning to focus on future planning and emancipation. They may
be developing and experimenting with self-reliance. Teens still need the consistent
backing of family but are essentially growing away from the family.
Toward the end of middle adolescence, many teens may begin to question previously
held beliefs and ideas regarding right and wrong, and they may be less influenced by
peer attitudes. An emergence of independent ethical thinking may be evident.
Implications for Separation and Placement
The adolescent will probably experience ambivalence towards family. He/She may
need to reject them to support family in order to gain a sense of independence.
However, the adolescent requires backing, support, and caring from the family.
Separation from the family undermines the opportunity to work out this conflict
within the family setting. With help and reassurance that ambivalence is normal, the
adolescent may be able to accept internal feeling. Moreover, the adolescent may be
capable of feeling angry and love for the family simultaneously.
The adolescent’s need for independence may affect response to placement in a family
setting, especially if the substitute family expects that he “become one of us.” The
teen’s identity maybe tied to the birth family and the teen could be unwilling to accept
the substitute family as more than a place to stay. This may be perceived as the
teen’s failure to adjust to the placement even though it is a healthy and expected
response.
Adolescents may not remain in a placement if it does not meet their needs. Some teens
this age would rather find solutions and caregivers one their own.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
The adolescent may constructively use casework counseling to deal with the conflicts
of separation and placement in a way that meets the teen’s needs without threatening
self-esteem and independence. A strong relationship with a trusted worker can
provide support, offer guidance and direction, and help develop realistic, accurate
perceptions of the situation and the adolescent’s role.
Common Core | Placement & Permanency: Trainee Content | Version 1.1, November 2006
California’s Seven Common Core Courses
1. The Framework for Child Welfare Practice in California
2. Child and Youth Development in a Child Welfare Context
3. Child Maltreatment Identification, Part 1: Neglect, Physical Abuse, and Emotional
Abuse
4. Child Maltreatment Identification, Part 2: Sexual Abuse
5. Critical Thinking in Child Welfare Assessment: Safety, Risk and Protective Capacity
6. Family Engagement in Case Planning and Case Management
7. Placement & Permanency
* Plus more courses required by your county
Five Themes Woven Throughout the Common Core
Accountability & Outcomes
Evidence-Based & Promising Practices
Fairness & Equity
Strength-Based Practices & Programs
Family & Youth Engagement
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Day 1, Segment 1, Activity 2A
Adoption and Safe Families Act (ASFA) 1997
Performance Goals and Outcomes for Children
Goal: Safety
Outcomes:
Children are, first and foremost, protected from abuse and neglect.
Children are safely maintained in their own homes whenever possible and appropriate.
Goal: Permanency
Outcomes:
Children have permanency and stability in their living situations.
The continuity of family relationships and connections is preserved for children.
Goal: Well-Being
Outcomes:
Families have enhanced capacity to provide for their children’s needs.
Children receive appropriate services to meet their educational needs.
Children receive adequate services to meet their physical and mental health needs.
System Factors
Statewide information system (CWS/CMS)
Case review system
Quality assurance system
Staff training
Service array
Agency responsiveness to the community
Recruitment, licensing and retention of foster and adoptive parents
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
What Will Success Look Like?
7 Outcome Indicators
Fewer children are abused/ neglected
Fewer children are in foster care
Fewer children re-enter foster care
Fewer multiple placements for children in foster care
Reduced length of time to reunify children with parents or caregivers
Reduced length of time to achieve adoption (less than 24 months)
Increased levels of health and education support for children in foster care
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Summary of Disproportionality Data
Based upon Calendar Year 2006 Information for California
(Source: Barbara Needell, PowerPoint presentation: Child Welfare: Ethnic/Racial Disproportionality and Disparity,
Center for Social Services Research, University of California, Berkeley.)
Black children are referred for maltreatment proportionally more than any other
group.
Black children compose 7% of the total child population, but account for 15% of
referrals.
There are 97/1000 Black children referred compared to 44/1000 for White children.
Once referred, there is little difference in the percent substantiated.
Overall 22% of children with a referral have it substantiated, with Hispanic, Asian and
Native American children having somewhat higher percentages of substantiation.
Black children are the more likely to enter foster care than children of other
ethnicities.
Black children enter care at a rate of 10.8 per 1,000 and Native American children
enter care at a rate of 5 per 1,000, compared to 3.8 per 1,000 for White children and
Hispanic children, and 1 per 1,000 for Asian children.
In care incidence rates show that Black children are in foster care at a rate over 4
times that of White children.
White children are in foster care at a rate of 6.6/1000 compared to Black children who
are in care at the rate of 29.8/1000. California’s disparity for Black children in care is
higher than that of the overall US rate, but lower than states such as Illinois and New
York.
Black children are less likely than White children to exit foster care to permanency
within 6 years of entry.
Sixty percent of White children versus 50% of Black children reunify within 6 years
from entry. Overall, 79% of Black children exit to permanency (i.e., reunification,
adoption, guardianship) within 6 years compared to 88% of White children.
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
What Do We Mean by Strength-Based?
Strength defined:
“capacity for exertion or endurance; a strong attribute or inherent asset” (Moore et al,
2002)
The goals of family strengths work in this field are:
To identify family strengths and resources that can be used in providing services and
supporting a family.
To use family strengths as benchmarks to assess the status of a family over the course
of time.
To use community-wide information of family strengths to develop resources in the
community.
Family strengths:
Are developed from a set of supportive relationships.
Are processes that support and protect families and family members, especially during
times of adversity and change.
Help to maintain family cohesion while also supporting the development and wellbeing of individual family members.
The absence of strengths can be as problematic for children as the presence of
deficits.
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Core Values of Strength-Based Family-Centered Practices
All families have strengths
Families are the experts on themselves and their own family histories
Families deserve to be treated with dignity and respect
Families can make well-informed decisions about keeping their children
safe when supported
When families and resources are involved in decision-making, outcomes
can improve
A team is often more capable of creative and high quality decisionmaking than an individual
The family’s culture is a source of strength
Culturally responsive practices honor the family’s customs, values and
preference
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
Strength-Based Language
Focuses on what is strong, not just what is wrong
Encourages families to do their personal best within the framework of
their cultures
Reframes deficits as opportunities for growth
Acknowledges and builds on successes
Presumes a desire for and the possibility of a positive outcome
Holds the belief that families can and do change, with support and
resources
Includes feelings and words that match
Models empathy and offers support
If you were “in the system,” which of these would you hope your child
welfare worker was committed to practicing?
Do you believe any of these are culture-specific? Race specific? Gender specific?
Common Core | Framework for Child Welfare Practice: Trainee's Guide | Version 1.2, May 2008
COMMON CORE CURRICULUM
- TRAINER’S AND TRAINEE'S GUIDES -
MASTER GLOSSARY
366.26
The legal process by which the court determines the most appropriate permanent living
arrangement for the child, either through adoption, legal guardianship, or a planned
permanent living arrangement.
387 petitions
A petition filed under Welfare & Institutions Code Sec. 387, requesting a child’s removal
to a more restrictive placement. 387 petitions must be filed to request removal from a
parent on a Family Maintenance plan, removal from a relative to foster care, and removal
to a higher level of foster care.
388 petitions
A petition filed under Welfare & Institutions Code Sec. 388, requesting a change of a
court order. Any interested party can file a 388 petition.
AB 458
The California Foster Care Non-Discrimination Act (AB 458) went into effect in 2004
and prohibits discrimination in the California foster system on the basis of “actual or
perceived race, ethnic group identification, ancestry, national origin, color, religion, sex,
sexual orientation, gender identity, mental or physical disability, or HIV status.”
[California Welfare & Institutions Code 16013(a)]. AB 458 also mandates and
encourages anti-discriminatory training for group home administrators, child welfare
workers, foster parents, relative caregivers and foster family agency staff.
AB 490
Ensuring Educational Rights and Stability for Foster Youth (AB 490, Steinberg, 2003).
Expands and stipulates authority for school records of foster, homeless, and incarcerated
youth. Establishes legislative intent that foster youth are ensured access to the same
opportunities to meet academic achievement standards to which all students are held,
maintain stable school placements, be placed in the least restrictive educational
placement, and have access to the same academic resources, services, and extracurricular
and enrichment activities as all other children. Makes clear that education and school
placement decisions are to be dictated by the best interest of the child.
AB 636
The Child Welfare System Improvement and Accountability Act of 2001 (AB 636,
Steinberg). Identifies and replicates best practices to improve child welfare service
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
outcomes through county-level review processes. Also referred to as California–Child
and Family Service Review (C-CFSR).
AB 3632
The Special Education Pupils Program (AB 3632) was passed in 1984, which assigned
responsibility to state agencies and counties for meeting the goals of an Individualized
Educational Plan (IEP). Basically, this legislation assigned schools the responsibility to
educate, the state Department of Mental Health (DMH) the responsibility to provide
mental health services, and the state Department of Social Services the responsibility to
provide out-of-home care.
Ability to Locate
The determination of where the child(ren) and/or family are located. [This includes
information gathered as part of the hotline information gathering process and that is
essential to facilitate the ability of the responding ER social worker to locate the child.
Specifics regarding hard-to-find locations should be gathered as part of this assessment.]
(#12 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Ability to Meet Child’s Needs
The ability of the caregiver to provide a safe, stable home and meet the basic needs of
children in their care. [This includes the ability to respond to a child’s age and condition
by providing care in a way that supports the child’s health, mental health, education,
development, and physical and emotional well-being.] (#10 in the Standard Areas for
Review of the Statewide Assessment System Matrix)
Addiction
Dependence on a chemical substance to the extent that a physiological and/or
psychological need is established. This may be manifested by any combination of the
following symptoms: tolerance; preoccupation with obtaining and using substance; use of
the substance despite anticipation of probable adverse consequences; repeated efforts to
cut down or control substance use; and withdrawal symptoms when the substance is
unavailable or not used.
Adoption
The court terminates the rights of the legal parent, usually the biological parent, and
orders that another person is now the legal parent of the child.
Adoption & Safe Families Act (ASFA)
National Child Welfare Act of 1997, setting performance goals, outcomes, and indicators
for social work system practice.
Alternative Dispute Resolution
Various processes by which legal disputes are settled without going to trial.
Alternative Permanency
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Arrangements whereby youth for whom family restoration is not possible or appropriate
establish enduring emotional ties with unrelated adult caregivers who are willing and able
to offer a stable and supportive continuing relationship whether within or outside of the
legal channels of adoption or guardianship.
APGAR Test
A test administered at one minute and five minutes (and may be repeated at a 10-minute
interval) after birth to help health care providers assess critical aspects of a baby’s health
at birth.
AOD (Alcohol and Other Drugs) Abuse
A pattern of substance use that threatens one’s health or impairs one’s social or economic
functioning.
Attention Deficit Hyperactivity Disorder (ADHD)
A condition that typically manifests itself in childhood and is characterized by
inattention, hyperactivity, and/or impulsivity. There are three main types of ADHD. One
type is characterized by inattentiveness; one type is characterized by hyperactive or
impulsive behavior. The third type is combined, when children exhibit signs of both
inattentiveness and hyperactivity.
Attorney for Defacto Parents
An attorney that represents the defacto parents, often to seek permanent custody of a
foster child.
Autistic Spectrum Disorder
A group of developmental disabilities that are related to brain function including autistic
disorder, pervasive developmental disorder–not otherwise specified (PDD-NOS,
including atypical autism), and Asperger’s disorder. People with ASD tend to have
difficulties with common culturally agreed upon social and communication skills and are
likely to repeat certain behaviors and resist change in their daily activities. Many people
with ASD also have unusual ways of learning, paying attention, or reacting to different
sensations. ASD begins during childhood and lasts throughout a person's life however,
early intervention can be critical in improving prognosis.
Basic Needs
The fundamental needs of a child and family for food, shelter, clothing, medical care, and
the child’s need for supervision. (#26 in the Standard Areas for Review of the Statewide
Assessment System Matrix)
Batterer Intervention
Intervention focused on helping the batterer learn to be non-violent.
Bias-Free Written Language
Communication that makes a conscious effort to avoid perpetuating biases in language
that emerge as a result of assumptions or attitudes on the basis of race, gender, religion,
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
or nationality. This includes rephrasing for gender neutrality, use of inclusive
terminology, appropriate forms of address and titles, and avoiding stereotypes.
(http://www2.state.ga.us/Courts/supreme/biasfree.htm)
Bench Officer
Judges, Referees, and Commissioners who hear the evidence presented and make
decisions about the families who come before the court.
Best Interest of the Child
One of the fundamental goals of the dependency system; to achieve the best outcome for
each individual child.
Burden of Proof
A party’s responsibility to prove something in dispute.
Bottle Rot
Severe dental decay which appears as blackened baby teeth, caused by improper feeding
including allowing milk or other liquid to pool in the baby’s mouth during sleep. Can
cause damage to permanent teeth and gums if not treated properly by a dentist.
Bruise
Bleeding under the skin which results in discoloration. A bruise may take on the pattern
of the object which caused the injury.
California Child Welfare Outcomes and Accountability System
California’s accountability mechanism that tracks and monitors child welfare outcomes,
measures performance on a county and statewide basis, and enforces continuous quality
improvement by requiring counties to set and meet improvement goals.
Caregiver
Parent(s), guardian(s), or other adult fulfilling the parental role and entrusted with the
responsibility to care for the child(ren).
Caregiver-Child Interaction
The verbal and non-verbal communication and behavior between a caregiver and child,
which reflect the quality of the relationship and the degree to which it is reciprocal. [This
includes behaviors that are associated with the degree to which a child’s parent caregivers
demonstrate an awareness of the child’s emotional state, empathy, bonding, and
appropriate responses to the child, as well as behaviors associated with child discipline.]
(#11 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Caregiver’s Compliance/Progress toward Case Plan Objectives
The progress of the parent(s) in achieving the objectives of the change-oriented
interventions specified in the case plan. [This includes the frequency and extent of the
parent’s participation in case plan activities, and the degree to which the parent
demonstrates that these activities have resulted in change consistent with case plan
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
objectives. Compliance is not the sole basis for considering preservation/restoration, but
is one element in assessing the parent’s success in achieving the objectives of the case
plan and preparation to act as a responsible parent.]
Caregiver’s Personal History of Abuse
The information gathered and utilized by the social worker in the assessment process to
determine whether the caregiver has ever been a victim of child abuse or neglect
him/herself, and whether that history impacts the caregiver’s protective capacity.
Caregiver Protective Capacity
The ability and willingness to utilize internal and external resources to mitigate or
ameliorate the identified safety and risk concerns, and to support the on-going safety of
the child. [Such capacities include, but are not limited to, attachment to the child,
parental caretaking skills, awareness of and ability to interpret the child’s needs, positive
motivation to nurture or meet the child’s needs, willingness to seek and use help, and
willingness/ability to act protectively when the child is threatened with harm. Protective
capacity elements are the focus of both safety plans and case plans for change-oriented
intervention. They point to the inherent capacities of the family or the resources that
could be mobilized to contribute to the ongoing protection of the child as well as to the
ability or motivation of the parents to change.] (#8 in the Standard Areas for Review of
the Statewide Assessment System Matrix)
Caregiver Willingness to Change
The caregiver’s motivation to change those conditions that threaten child safety and/or
those ineffective/inappropriate behaviors that were identified in the initial assessment.
(#22 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Case Plan
The written document which is developed based on an assessment of the circumstances
which required child welfare services intervention, and in which the social worker
identifies a case plan goal, the objectives to be achieved, the specific services to be
provided, and case management activities to be performed. [Div 31-002(c)(2)]
Change-Oriented Services
CPS interventions that increase protective capacities of the caregivers by modifying
conditions or ineffective/inappropriate behaviors that threaten child safety, reconciling
the competing demands of urgency and the gradual nature of meaningful change
processes.
Child and Family Services Review (CFSR)
Authorized by 2000 Federal Rule as part of ASFA. Formal review of state child welfare
programs conducted every three years by the federal government using specific
benchmarks designed to assess achievement of child safety, permanency, and well-being
outcomes and to identify the state’s strengths, needs, and requirements for technical
assistance.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Child and Family Support Assessment (CAFSA)
The Child and Family Support Assessment is comprised of an initial face-to-face
assessment of child safety, risk for maltreatment, and parental protective capacity
followed by a more comprehensive child and family assessment.
Child Development
The child’s language, cognitive, social/emotional, sensory, and motor development. [The
social worker will note any diagnosed developmental problems or apparent need for
developmental testing.] (#29 in the Standard Areas for Review of the Statewide
Assessment System Matrix)
Child Neglect
Acts of omission or commission which result in minimal standards of care not being met.
Child Strengths and Vulnerability
Strengths refer to the child’s behaviors and attitude that support his o her own safety,
permanency, and well-being including health, education, and social development. The
child’s vulnerability refers to his or her susceptibility to suffer abuse or neglect based on
age, health, size, mobility, social/emotional state, and the ability of the caregiver to
provide protection. [Key characteristics indicating increased child vulnerability include
developmental disability, mental illness, (including withdrawn, fearful, or anxious
behavior) and lack of self protection skills; children with substance abusing parents;
homeless children; and children experiencing chronic neglect.] (#3 in the Standard Areas
for Review of the Statewide Assessment System Matrix)
Child Welfare High Risk Response (see also Differential Response)
Intervention in situations in which children are at moderate to high risk for continued
child abuse/neglect, and actions have to be taken to protect the child with or without the
family’s agreement. May involve the filing of criminal charges against the adult(s) who
caused harm.
Child Well-Being
A primary outcome goal for child welfare services focused on how effectively the
developmental, behavioral, cultural, and physical needs of children are met.
Child’s Attorney
An attorney that represents the child in court and informs the court of the child’s wishes
and the child’s best interests.
Child’s Immediate and Ongoing Needs
The identified developmental, behavioral, cultural, and physical needs of a child
including his or her immediate and ongoing needs for safety and security/permanency.
[This includes ensuring that children and families receive sufficient support and services
when and where they need them in order to maintain all aspects of their functioning that
may be compromised by risk factors associated with abuse and neglect. Immediate and
ongoing safety, permanency, and well-being needs include medical, dental, mental
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
health, and developmental needs; housing, food, clothing, education, and emotional
support (i.e., healthy family and peer relationships).] (#15 in the Standard Areas for
Review of the Statewide Assessment System Matrix)
Child’s Permanency Needs
The maintenance and/or establishment of enduring family attachments. This includes a
broad array of individualized permanency options, including Reunification, Adoption,
Legal Guardianship, and alternative permanent living arrangements for all children and
youth to promote their safety, permanence, and well-being. [Permanency is both a
process and a result that includes involvement of the child/youth as a participant or leader
(when possible) in finding a permanent connection with at least one committed adult,
who provides:
a safe, stable and secure parenting relationship,
love,
unconditional commitment,
lifelong support in the context of reunification, a legal adoption, or
guardianship, where possible, and in which the child/youth has the
opportunity to maintain contacts with important persons, including brothers
and sisters.
A broad array of individualized permanency options exist for all children and youth to
promote their safety, permanence, and well-being: reunification and adoption are two
important ones among many that may be appropriate. California Permanency for Youth
Task Force.] (#20 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Child’s Relationship with Peers and Adults
The quality of connectedness (defined as close and positive attachment) by the child to
significant adults or peers in his or her life. [This quality is measured by the degree in
which these relationships meet or enhance the child’s emotional, developmental, social,
mental, and/or educational needs. These significant relationships may include immediate
family, friends, professionals, or extended family but can include anyone who has an
impact on the child’s life and cannot be measured solely by frequency of contact with the
child.] (#32 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Collateral Contacts
The person or persons from whom pertinent information is gathered to make a decision
regarding the allegations of child maltreatment and the potential risk of abuse in the
future. [The social worker will make contact with known persons who may have
knowledge about the family, if the worker believes that person will provide pertinent
information regarding risk and safety of the child. The social worker will follow policies
and regulations regarding the release of confidential information in making collateral
contacts.]
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Common Continuum of Alcohol and Drug Dependency & Response [Cycle
of Addiction]
Describes the pattern of use that can lead to dependency: non-use/selective abstinence;
experimental use/initial use; response use, “at risk” use; situational/crises, or binge
use/abuse; unhealthy use, chronic abuse; chemical dependency/addiction; recovery and
relapse; and “in recovery.”
Community Response (see also Differential Response)
A pro-active response to and assessment of situations involving families under stress who
come to the attention of the Child Welfare System but who do not present an immediate
risk for child maltreatment. Provides families with access to services to address identified
issues without formal entry into the system.
Concurrent Planning
The process of coupling aggressive efforts to restore the family with careful planning for
the possibility of adoption or other permanency options should circumstances prevent the
child from returning to her/his family of origin.
Confidentiality
The protection of information from release to organizations or individuals not entitled by
law to such information.
Contributing Factors Requiring Intervention
Refers to the circumstances that require child welfare services intervention (WIC
16501.1(f)(1). (#23 in the Standard Areas for Review of the Statewide Assessment
System Matrix)
County Counsel
An attorney that represents the child welfare agency in court. (The child welfare agency,
not the individual child welfare worker, is the client.)
Court Appointed Special Advocate (CASA)
CASA is a program designated by the local presiding juvenile court judge to recruit,
screen, select, train, supervise, and support lay volunteers to be appointed by the court to
help define the best interest of the child. CASA volunteers visit the child regularly and
write reports for the court.
Cultural and Language Considerations
The consideration and exploration of the family’s cultural framework in the assessment
and the development of safety plans and case plans. [This includes social work
intervention, services, and assessments that are culturally competent and linguistically
sensitive, including the provision of services in the language of the client population
served.] (#4 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Current and Previous Social Services
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Any social services currently or previously provided by a public child welfare agency or
any social services agency. [These services may include CalWORKS, mental health
services, counseling services, family resource services, etc. This information is used by
the social worker to determine the response type, to conduct safety assessments, to
perform case management, and to make decisions regarding service interventions,
placement, permanency goals, and readiness for case closure.] (#24 in the Standard
Areas for Review of the Statewide Assessment System Matrix)
Current and Prior CWS History
The information gathered by the social worker from reviews of the CWS/CMS and other
available documentation to determine whether or not the child and family have current or
past involvement with the public child welfare agency. (#2 in the Standard Areas for
Review of the Statewide Assessment System Matrix)
Current and Prior Maltreatment
Maltreatment refers to an act of omission or commission by a parent or any person who
exercises care, custody, and ongoing control of a child which has resulted in, or has
placed the child at risk of, developmental, physical, or psychological harm. [The social
worker will gather information provided by reporting parties and collateral contacts
(when appropriate) about that person’s knowledge of current maltreatment of a child.
The social worker will also gather information about any previous incidents of child
maltreatment involving the child or family.] (#1 in the Standard Areas for Review of the
Statewide Assessment System Matrix)
CWS Response (see also Differential Response)
A proactive response to and assessment of situations involving families in which low to
moderate risk is present. Includes the engagement of families, voluntarily wherever
possible, in development and implementation of a service plan directed at protection of
the child.
CWS Stakeholders
More than 60 invited representatives of all aspects of the child welfare community who
met monthly over the course of three years to identify and recommend changes in
California’s Child Welfare Services, leading to better outcomes for children and their
families.
Cycle of Addiction
Describes the pattern of use that can lead to dependency: non-use/selective abstinence;
experimental use/initial use; response use, “at risk” use; situational/crises, or binge
use/abuse; unhealthy use, chronic abuse; chemical dependency/addiction; recovery and
relapse; and, “In recovery.”
Decision Making Model
A general model adapted from Stein and Rzepnicki to assist new workers in the process
of decision making (Miller, 2005). This general model includes the following steps:
Step 1: Information Gathering
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Step 2: Application of Rules of Criteria
Step 3: Discussion/Feedback
Step 4: Decision/Professional Judgment
Step 5: Reassessment
Defacto Parent Status
A person who is the current or recent caregiver of a child and has been found by the court
to have assumed, on a day to day basis, the role of parent to the child, and who has
assumed that role for a significant period. Defacto parents have the right to be present at
dependency proceedings, to be represented by counsel, and to present evidence.
Definitions of Physical Abuse, Sexual Abuse, Emotional Abuse, Neglect
and/or Exploitation
Penal Code 11165 et seq.
Delinquency Proceeding
The court is asked to declare a minor a ward of the court based on the minor’s behavior
which would be considered criminal behavior if the minor were an adult. (Welfare and
Institutions Code Sec. 602.)
Delinquent Behavior
Behavior by a person under the age of 18 that is persistently or habitually in conflict with
the reasonable orders of his guardians and/or is in violation of any laws of this state or the
United States. (Welfare & Institutions Code Sec. 601, 602) (#35 in the Standard Areas
for Review of the Statewide Assessment System Matrix)
Dental/Medical Care
The needs of a child and family for basic dental care, including routine examination,
diagnosis, or treatment by a licensed dentist. The needs of a child and family for basic
medical care, including routine examination, diagnosis or treatment, and hospital care
under the general or special supervision or advice, are to be rendered by a licensed
physician.
Dependency Proceeding
The court is asked to adjudge a minor to be a dependent of the court based on one or
more of the grounds of child abuse and neglect specified in Welfare and Institutions Code
Sec. 300.
Detention Hearing
The first judicial proceeding in a dependency case where the judge decides whether the
child should remain in custody, away from his or her parents, while an investigation into
the reasons for the removal is conducted. At this hearing, the court will appoint counsel,
advise parents of their rights, explain the court process, order visitation when appropriate,
inquire about possible relative caretakers, and inquire into the child’s paternity and
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
determine whether the Indian Child Welfare Act might apply. This hearing must be held
within three days of the physical removal of the child.
Differential Response (see also Child Welfare High Risk Response,
Community Response, and CWS Response)
A system for triaging referrals received by the Child Abuse Hotline/Intake that provides a
broader range of responses by the Child Welfare System to assure child safety and family
maintenance that includes partnerships with community based agencies and works with
families to identify community supports and strength-based solutions appropriate to their
circumstances.
Differentiation
The process by which neurons become specialized in response to neurochemical and
micro environmental cues. These cues tell each neuron which combination of genes to
activate in expressing a “unique neurochemistry, neuroarchitecture and functional
capability….Each neuron undergoes a series of “decisions” to determine its final location
and specialization” (p. 83). Any experience that interrupts or alters the cues and signals
sent to neurons can affect the process of differentiation, “thereby altering the functional
capacity of the neural networks in which these neurons reside” (p. 83).
Adapted from: Perry, B.P. (2002). Childhood Experience and the Expression of Genetic Potential: What
Childhood Neglect Tells Us About Nature and Nurture. Brain and Mind, 3, 79-100 to supplement the
screening of Dr. Perry’s videotape.
Dismissal
The court dismisses the dependency petition, and the court case is over. This can happen
because a child is returned home and supervision is no longer necessary, or because a
child has reached the age of majority and the agency has met all the dismissal
requirements in WIC Sec. 391.
Disparity
Disparity means unequal treatment when comparing a racial or ethnic minority to a nonminority. This can be observed in many forms including decision points (e.g., reporting,
investigation, substantiation, foster care placement, exit), treatment, services, or
resources. Research shows that children of color in foster care and their families are
treated differently from—and often not as well as—white children and their families in
the system. (Robert Hill, October 2006)
Disposition
At this hearing, the court considers what it should do to protect and help the child and his
or her family. The court decides whether to dismiss the case, order informal services for
the family without making the child a dependent, appoint a guardian with the consent of
the parents, declare the child a dependent of the court and leave the child in the home of
the parents with family maintenance services, remove the child from the home and order
reunification services for the parents, or remove the child from the home and not order
reunification services for one of the reasons in WIC Sec. 361.5(b). The court also
approves the case plan submitted to the court which outlines the services to be provided
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
to the child and family. This hearing can occur at the same time as the jurisdiction
hearing and must occur within 10 court days of the jurisdiction hearing for detained
children and within 30 court days for a non-detained child.
Disproportionality
Disproportionality refers to the differences in the percentage of children of a certain
racial or ethnic group in the country as compared to the percentage of the children of the
same group in the Child Welfare System. For example, in 2000 Black children made up
15.1% of the children in this country but 36.6% of the children in the Child Welfare
System. (Robert Hill, Oct. 2006)
Division 31
The State of California’s regulations that provide policy and procedures on the delivery
of child welfare services. These regulations are broken into programs that are funded by
Title IV-E federal funds. Each county develops more specific policy and procedures
from these state regulations.
Domestic Violence
A pattern of assaultive and coercive behaviors used against intimate partners (including
physical, sexual, and psychological attacks, as well as economic coercion). [Refer to the
legal definitions in Family Code Sec. 6211. Also recommend using the National Council
of Juvenile and Family Court Judges’ Effective Interventions in Domestic Violence and
Child Maltreatment Cases: Guidelines for Policy and Practice (Green book Project).]
(#34 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Due Process
The conduct of legal proceedings according to rules and principles to protect private
rights, including notice and the right to a fair hearing.
Early Reunification
Efforts directed at enhancing parental protective capacity in order to permit the child to
return to his or her family within 30 to 60 days of placement.
Educational Needs
The level of the child’s academic performance which takes into account the child’s age
relative to assigned grade level, the child’s performance as recorded, monitored, and
measured by the child’s educational institution, and any barriers that are identified that
may interfere with the child’s successful academic performance. (#30 in the Standard
Areas for Review of the Statewide Assessment System Matrix)
Educational Surrogate
The responsible adult appointed for a child with exceptional educational needs. The
educational rights of the child’s parents are limited and vested in this person.
Ethnographic Interviewing
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
A skillful and engaging method of interviewing designed to elicit comprehensive
information about a client’s life experience in terms of values, beliefs, customs, history,
and family composition, etc., often relying on open-ended questions.
Evidence-based Practice
A set of tools and resources for finding and applying the best current research evidence to
service delivery, and integrating this information with clinical expertise and client values.
External Resources
The formal or informal resources outside the individual or the family, (i.e., community
connections, support of friends, church, or community organizations, etc.) that strengthen
their capacity to mitigate risk and to support the on-going safety of a child.
Failure to Thrive (FTT)
Condition that exists when a child under age 2 is below the fifth percentile on normal
growth charts for height, weight, and head circumference. Organic causes should be
ruled out. Non-organic failure to thrive is a result of caloric deprivation and there is often
a corresponding lack of bonding between the baby and the primary caregiver.
Fairness and Equity
A principle of best practice that promotes policies, procedures, practices, and service
arrays that support all children and families in obtaining similar benefit from child
welfare interventions and equal opportunity to attain positive outcomes. Fairness and
equity embodies the ideals of social justice and cultural competency.
Family and Household Relationships
Refers to the interactions between those persons who are related by blood, marriage, or
adoption and/or who reside together in the same dwelling.
Family and Youth Engagement
Practices and strategies congruent with relevant sociocultural dynamics that effectively
engage parents, youth and extended family members in a respectful and collaborative
manner in the assessment, intervention and case planning processes.
Family to Family
An initiative designed in 1992 and field tested in communities across the country that
effectively incorporates a number of strategies consistent with the values and objectives
of Redesign, including comprehensive assessment, family team decision-making,
neighborhood placement in families, and concurrent planning to assure children
permanent families in a timely manner. (Promising Practice)
Family Well-Being
A primary outcome goal for California’s child welfare services whereby families
demonstrate self-sufficiency and the ability to adequately meet basic family needs (e.g.,
safety, food, clothing, housing, health care, financial, emotional, and social support) and
provide age-appropriate supervision and nurturing of their children.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Fetal Alcohol Spectrum Disorders
An umbrella term referring to all disorders occurring due to an alcohol exposed fetus
including Fetal Alcohol Syndrome (FAS), Fetal Alcohol Effects (FAE), Alcohol-Related
Neurodevelopmental Disorders (ARND), Partial FAS and Static Encephalopathy,
Alcohol Exposed.
Folk Treatments
Cultural practices and natural healing methods which are used to treat illnesses and
injuries.
Fontanel
Any of the soft membranous gaps between the incompletely formed cranial bones of a
fetus or an infant.
Fracture
Broken bone. The type of fracture may help determine if it was caused accidentally or
non-accidentally.
Guardian Ad Litem
A person appointed after a hearing to make decisions about case strategy for an
incompetent parent.
History of Child Abuse and Neglect
Refers to caregiver’s identification as a perpetrator of substantiated child abuse or neglect
as defined by a child protection agency.
History of Criminal Behavior
Caregiver’s previous or current illegal activity as defined by federal and state law that
may impact the caregiver’s protective capacity. [Typical sources include self-report,
drug test results, and law enforcement records.] (#25 in the Standard Areas for Review of
the Statewide Assessment System Matrix)
Home Environment
The physical condition of the home including safety hazards and health concerns. (#9 in
the Standard Areas for Review of the Statewide Assessment System Matrix)
Inclusive Governance
A characteristic of effective community partnerships that ensures that the diverse
perspectives of the people affected by a decision, especially groups currently and
historically under-represented, are taken into account in making and shaping decisions.
Independent Living
A program for children age 16 and older that provides services to help youth become
self-sufficient by the time they leave the foster care system. All children must be offered
enrollment in this program.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Indian Child Welfare Act (ICWA)
Indian Child Welfare Act. Congress passed these laws in 1978 to protect the best interests
of Indian children and to promote the stability and security of Indian tribes and families
by establishing specific standards that must be met before an Indian child can be removed
from his or her family and placed in an adoptive or foster care placement. Congress was
concerned about the high rate of Indian children being removed from their homes and
placed with non-Indian families and the negative consequences this has on Indian
children, families, and tribes. This federal law is codified in California statute and rule of
court.
Individualized Educational Program (IEP)
A written document developed for each public school child who is eligible for special
education services. The IEP is created through a team effort and reviewed at least once a
year.
Initial Assessment
The [California child welfare improvement] intake function, the focus of which is to learn
more about the immediate safety issues for the child, as well as obtain background
information about the parent through collateral contacts.
Internal Resources
Those resources that exist within each individual in the family and the family as a whole
(i.e., emotional and psychological strengths, etc.) that strengthen their capacity to
mitigate risk and to support the on-going safety of a child.
Intimate Partner Violence (IPV) (see Domestic Violence)
Jurisdiction Hearing
At this hearing, the court decides whether or not the allegations in the petition filed by the
child welfare agency are true, and whether the child has been abused or neglected, as
described in Welfare and Institutions Code Sec. 300. This hearing must be held within 15
days of the detention hearing.
Juvenile Dependency
A legal system where children become dependents of the court due to parental abuse or
neglect. California’s system simultaneously strives to preserve the family unit, while
obtaining permanency for children.
Kin
Includes relatives, such as grandparents or siblings as well as fictive kin such as members
of a child’s tribe or clan, godparents, stepparents, or any other adults who share a kinship
bond with a child.
Kinship Care
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Kinship care is the full time care, nurturing, and protection of children by relatives,
members of their tribes or clans, godparents, stepparents, or any adult who has a kinship
bond with a child.
Legal Guardianship
The court suspends, but does not terminate, parental rights, and another adult is appointed
to be responsible for the child.
Level of Care to Meet Child’s Needs
The assessment and determination of the appropriate services and placement type that
best meets the child’s physical and emotional needs. [This includes considerations of
placing the child in the least restrictive, most family like setting; addressing the child’s
personal characteristics and cultural background; maintaining the child’s connections to
family and siblings whenever possible; allowing the child to remain in current school if
possible; allowing for reasonable visitation, reunification, and permanency planning; and
providing for any special needs of the child. Based on Div 31-400 in general.] (#16 in
the Standard Areas for Review of the Statewide Assessment System Matrix)
Maltreatment (see Current and Prior Maltreatment)
Mediation
A guided discussion, outside of court, about a case, where all parties meet to agree on a
plan for a child. Mediation provides a problem-solving forum for all interested persons to
develop a plan in the best interests of the child, emphasizing family preservation and
strengthening.
Mediator
A person who guides the discussion at mediation in a neutral manner with the aim of
bringing the parties to consensus.
Medical/Dental Care
The needs of a child and family for basic medical care, including routine examination,
diagnosis, or treatment, and hospital care under general or special supervision or advice
to be rendered by a licensed physician. The needs of a child and family for basic dental
care, including routine examination, diagnosis, or treatment by a licensed dentist. (#27 in
the Standard Areas for Review of the Statewide Assessment System Matrix)
Mental Health/Coping Skills
Emotional and psychological well-being, including the ability of an individual to use his
or her cognitive and emotional capabilities to handle day-to-day stressors of life and
function effectively in society. (#28 in the Standard Areas for Review of the Statewide
Assessment System Matrix)
Migration
The process by which neurons “cluster, sort, move and settle into their final ‘resting’
place” (p. 83). Primarily guided by neuroglial cells, neurons migrate out from where they
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
are produced in the center of the developing brain to where they will eventually settle
(i.e. the brainstem, cortex, etc.). Although most neuronal migration takes place in utero
and during in the perinatal period, it continues to occur throughout childhood.
Environmental factors and “intrauterine and perinatal insults” can affect the migration of
neurons, thus influencing the formation as well as the function of the developing neural
network.
Adapted from: Perry, B.P. (2002). Childhood Experience and the Expression of Genetic Potential: What
Childhood Neglect Tells Us About Nature and Nurture. Brain and Mind, 3, 79-100 to supplement the
screening of Dr. Perry’s videotape.
Minimum Sufficient Level of Care (MSLC)
The social standard for the minimum of caregiver behavior below which a home is
inadequate for the care of a child. Factors to consider in establishing what the MSLC is
for a particular child include those that relate to:
the child’s needs,
contemporary social standards, and
community standards.
Multi-Disciplinary Teams
A group of professionals and paraprofessionals representing an array of disciplines (e.g.,
resource families, service providers, law enforcement, juvenile courts, and other
community organizations) who interact and coordinate efforts with parents and families,
pooling their skills to offer comprehensive, coordinated services.
Munchausen Syndome by Proxy
A simulated illness or condition produced by a parent in a child in order to meet the
emotional needs of the parent. Symptoms occur only in the presence of the parent.
May be captured by covert video.
Mutual Combatants
Two persons, equally involved in the commission of a crime against the other person, and
neither person was acting in self-defense.
Neurogenesis
The process by which new nerve cells, and the delicate network of branched cells and
fibers that supports the tissue of the central nervous system (“neuroglia”), are generated.
This “birth” of neurons takes place primarily during the second and third trimesters of
pregnancy. The great majority of neurons that will be used throughout one’s lifetime are
present at birth. However, most neurons are not fully specialized or organized at birth.
After birth, the connections that are formed between neurons eventually become the
“functional neural networks of the mature brain”.
Adapted from: Perry, B.P. (2002). Childhood Experience and the Expression of Genetic Potential: What
Childhood Neglect Tells Us About Nature and Nurture. Brain and Mind, 3, 79-100 to supplement the
screening of Dr. Perry’s videotape.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Non-Adversarial Approaches
Practices, including dependency mediation, family group conferencing, or decisionmaking and settlement conferences, designed to engage family members as respected
participants in the search for viable solutions to issues that have brought them into
contact with CWS.
Noticing
Formal provision of the date, time, location, and purpose of the hearing.
Overrepresentation
Overrepresentation refers to the current situation in which particular racial/ethnic groups
of children are represented in foster care at a higher or lower percentage than their
representation in the general population. (Ruth McRoy, 2005)
Outcomes-Informed Practice
Practice that supports and is informed by federal and state outcomes. All training in
California supports the federal outcomes of Safety, Permanency and Well-Being.
California also has developed state-specific performance measures.
Parent’s Attorney
Represents the parent’s wishes in court, and ensures the parent is afforded due process in
the proceedings.
Parenting Skills
The skills a parent demonstrates regarding their capacity to effectively care for, guide,
and discipline the child(ren) in their custody. (#31 in the Standard Areas for Review of
the Statewide Assessment System Matrix)
Party
A participant in the case who has the right to notice and to present evidence to the court.
Peer Quality Case Reviews
A key component of the C-CFSR designed to enrich and deepen understanding of a
county’s actual practices in the field by bringing experienced peers from neighboring
counties to assess and identify the subject county’s strengths and areas needing
improvement within the child welfare services delivery system and social work practice.
Performance Indicators
Specific, measurable data points used in combination to gauge progress in relation to
established outcomes.
Permanence
A primary outcome goal for child welfare services whereby all children and youth have
stable and nurturing legal relationships with adult caregivers that create a shared sense of
belonging and emotional security enduring over time.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Permanency Hearing
The hearing where the court determines the most appropriate permanent plan for the
child. This can be at disposition if the court does not order reunification services under
WIC Sec. 361.5(b) or at a hearing where the court terminates reunification services. The
permanent plans in California in order of preference are: return home, adoption, legal
guardianship, permanent placement with a relative, or permanent placement with an
identified placement and a specific goal. If the court chooses adoption or legal
guardianship, it must set a hearing under WIC 366.26 which is referred to as a .26
hearing or a selection and implementation hearing.
Perpetrator
The person alleged to have committed the abuse and/or against the child.
Perpetrator Access
The perpetrator’s relationship to the child; frequency and intimacy of their contact with
the child. (#5 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Pediatric Radiologist
A medical expert who interprets X-rays regarding fractures and internal injuries in
children.
Pettichaie
Pinpoint hemorrhages often associated with suffocation.
Physical Abuse
Non-accidental, inflicted injury/trauma to a child.
Positive Toxicology Screen (pos tox)
A screening test of newborn urine which indicates that a substance has been ingested and
which shows positive results for a drug. Mothers who test positive for drugs upon
delivery will have infants who also have ingested the same substance. Generally these
results indicate usage by the mother within the past 72 hours.
Post Permanency Hearing
Review hearings after the development of a permanent plan for the child. The court
reviews the case and case plan. Must be held no less than every six months.
Posttraumatic Stress Disorder (PTSD)
An emotional illness that develops as a result of an event involving actual or threatened
death, serious injury, rape or childhood sexual abuse and is out of the normal experience
for that individual (or may be accumulative or repeated). The stressor must be extreme,
not just severe and causes intense subjective responses, such as fear, helplessness or
horror. Key symptoms include:
Re-experiencing the event
Avoidance
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Emotional numbing
Increased arousal
Pre-Placement Preventative Services
Those services designed to help children remain with their families by preventing or
eliminating the need for removing the child from the home. [These services are
emergency response services and family maintenance services. Div 31-002 (p) (8).] (#14
in the Standard Areas for Review of the Statewide Assessment System Matrix)
Prevention
Service delivery and family engagement processes designed to mitigate the circumstances
leading to child maltreatment before it occurs.
Program Improvement Plan (PIP)
A comprehensive response to findings of the CFSR establishing specific strategies and
benchmarks for upgrading performance in all areas of nonconformity with established
indicators.
Protective Capacity
Refers to the ability and willingness to utilize internal and external resources to mitigate
risk and to support the on-going safety of a child.
Reasonable Efforts
A legal determination as to whether or not the child welfare agency has provided the
family with adequate services, which can include visitation, referrals, and other case
management. Reasonable efforts must be made to reunify the family or to finalize a
permanent plan for the child.
Recovery
Recovery refers to both internal conditions experienced by persons who describe
themselves as being in recovery—hope, healing, empowerment, and connection—and
external conditions that facilitate recovery—implementation of the principle of human
rights, a positive culture of healing, and recovery-oriented services.
http://www.psychservices.psychiatryonline.org/cgi/content/full/52/4/482
Relapse
Relapse is common in recovery from addiction and not considered a treatment failure.
As with other chronic illnesses, significant improvement is considered successful
treatment even if complete remission or absolute cure is not achieved.
Relapse Prevention
Relapse prevention requires the development of a plan tailored to maintaining new
behavior. The plan involves integrating behavior diversion activities, coping skills, and
emotional support.
Resource Families
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Relative caregivers, licensed foster parents, and adoptive parents who meet the needs of
children who cannot safely remain at home. Resource families participate as members of
the multidisciplinary team.
Restraining Order [Protection Order]
A restraining order is a court order that can protect you from being physically abused,
threatened, stalked, or harassed.
Reunification
If the court determines there is not a substantial danger to the child, the court can return
the child to the physical custody of the parent.
Risk
The likelihood that a child will be abused, neglected, or exploited.
Risk Assessment
The process utilized by a social worker to determine the likelihood that a child will be
abused, neglected, or exploited. [This could include the use of a variety of tools and/or
experience, training, and professional judgment, as well as other research-based tools
(including evidence-based decision-making tools) to:
facilitate the interviewing of children, families, and community members,
gather and evaluate information from collateral contacts,
gather and evaluate psycho-social information regarding the parent,
review and evaluate past history (including use of CWS/CMS data).
Risk elements are the focus of the case plan for change-oriented interventions—they
indicate what has to be addressed as the child protection system works with the family to
change the conditions that put the child at risk, as well as potential future safety
challenges. The assessment of risk also incorporates the elements of protective capacity.]
Safety
A primary outcome for child welfare services whereby all children are, first and
foremost, protected from abuse and neglect.
Safety Assessment
The process utilized by a county social worker to determine if a child is currently safe
from physical abuse, sexual abuse, emotional abuse, neglect, and/or exploitation. [This
could include the use of a variety of tools and/or experience, training, and professional
judgment, as well as other research-based tools (including evidence-based decisionmaking tools) to make that determination. The safety assessment is conducted as part of
the initial CPS intervention and continues throughout the life of the case. A safety
assessment is not the same thing as a risk assessment.]
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Safety Interventions
The actions, services, arrangements, and circumstances intended to mitigate the threat of,
repeat abuse of, or maltreatment of the child. [This includes the development of a safety
plan for providing services to promote the health and safety of the children in the family.
The safety plan addresses what threats of severe harm exist; how they will be managed,
including by whom, under what circumstances, with what specified time requirements,
etc.] (#13 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Safety Threshold
The point when family conditions, in the form of behaviors, emotions, intent, situations,
etc., are manifested in such a way that they are beyond risk factors and threaten the
child’s safety.
SARB
School Attendance Review Boards, which handle most attendance issues for school
jurisdictions without the involvement of Child Protective Services.
Secondary Trauma
Trauma affects those who experience it indirectly. Secondary, or vicarious trauma, refers
to those people who care for, or are involved with, those who have been directly
traumatized.
Shaken Infant Syndrome
Severe trauma to a child under age 5, and generally under age 1, as a result of severe
shaking resulting in whiplash-type of injury. Retinal hemorrhages are symptomatic.
Requires a significant amount of force.
Shared Family Care
Temporary placement of children and parents in the homes of trained community
members who, with the support of professional teams, mentor the families to the point
that they develop the necessary skills, supports, and protective capacity to care for their
children independently.
Shared Responsibility
This concept encourages community residents to get involved in child protection. It
offers opportunities for participation and stresses the importance and impact of the whole
community’s responsibility for child safety and well being. This does not negate the
ultimate accountability of the CWS agency for child protection. Rather, it engenders a
community mindset to develop the necessary capacity to protect children and to
strengthen and preserve families.
Sibling Placement
The efforts made in all out-of-home placements, including those with relatives, to place
siblings together in order to maintain the continuity of the family unit. [Sibling is defined
as a person related to the child by blood, adoption, or affinity through a common legal or
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
biological parent. Welfare & Institutions Code Sec. 16002(a)(b)] (#19 in the Standard
Areas for Review of the Statewide Assessment System Matrix)
SIDS
Sudden Infants Death Syndrome is the unexplained, unexpected death of an otherwise
healthy child up to age 1. There is an absence of an explanation of the cause of death via
autopsy, and the death scene investigation should be conducted to rule out other causes of
death.
Skeletal Survey
A body X-ray of a child age 2 or under to determine if there are other fractures or internal
injuries.
Slate Gray Spot (formerly known as Mongolian spots)
A birth mark which resembles a bruise in appearance. May be colored brown or may be
greenish-purple in color. Often on the lower back/buttocks but can be anywhere. More
common on children of color, this condition is often mistaken for child abuse.
Social Environment
The social interactions of those living in or having significant contact in the home that
support or compromise the child’s health and safety. [This includes the degree to which
communications, interactions, and relational networks with the home or surrounding the
child support or compromise the child’s health and safety. Also included are the current
and historical conditions within the home which are associated with the caregiver’s
capability to rely on an appropriate social network, ability to solve problems, and ability
to communicate effectively. Positive aspects of the social environment may mitigate risk
to the child.] (#7 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Stages of Change
The five stages of change are: pre-contemplation, contemplation, preparation, action, and
maintenance.
Standardized Safety Approach
A uniform approach to the safety, risk, and protective capacity of the adult caregiver to
assure basic levels of protective responses statewide and to assure that fairness and equity
is embedded in criteria used for case decisions.
Status Offender Proceeding
The court is asked to declare a minor a ward of the court based on the minor’s refusal to
obey reasonable orders of the minor’s parents. (Welfare and Institutions Code Sec. 601.)
Status Review Hearing
At this hearing, held every six months, the judge reviews the case and the case plan. The
judge must decide in family maintenance cases, if the conditions that brought the family
within the court’s jurisdiction still exist or if such conditions are likely to exist if
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
supervision is withdrawn. In family reunification cases, during the period in which
reunification services are being provided, the court must return the child home unless the
agency can show that return of the child to the home would create a substantial risk of
detriment to the child’s safety, protection, or physical or emotional well-being.
Strengths-Based Casework
An approach to working with families which recognizes that the families themselves hold
the greatest knowledge about the resources and strengths in that family system and which
honors and respects the family members and offers to join with the family in reaching
goals for improvement in family functioning.
Strength-based Practices
Those practices that focus on family or individual strengths when assessing and
intervening with families. These include:
-Using language that focuses on strengths
-Specific interviewing skills
-Specific assessment criteria
-Specific model practices
-Specific casework practices
-Engagement of the neighborhood and the community
-Agency practices with staff and the community
Subsequent Referrals
Reports received by the child welfare agency regarding new allegations after the initial
report of child maltreatment. (#36 in the Standard Areas for Review of the Statewide
Assessment System Matrix)
Substance Abuse
The abuse of alcohol and other drugs (AOD) by the parent, caregiver, or the child.
[Considering substance abuse in making safety assessments will include the severity and
impact of the AOD use on each member of the family. Some cases will require
differentiating between substance use, abuse, or dependence for the adult or adolescent
family members.] (#33 in the Standard Areas for Review of the Statewide Assessment
System Matrix)
Substance Abuse Assessment
Screening and/or assessment to determine the presence of an AOD abuse disorder. This
assessment process should: employ cultural sensitivity; use a standardized tool such as
the Addiction Severity Index (ASI); use Standardized Placement Criteria such as the
American Society of Addiction Medicine (ASAM) Placement Criteria; and ensure that
re-assessments occur with concomitant case plan adjustment.
Substitute Care Provider
A foster parent or relative/non-relative extended family member who is responsible for a
child’s care during his or her placement in out-of-home care. [The non-relative extended
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
family member may be a person who has an established familial or mentoring
relationship with the child.]
Substitute Care Provider’s Strength and Willingness to Support the Child’s
Case Plan
The active participation of the caregiver in activities that promote and support the child’s
safety, permanency, and well-being including health, education, and social development.
(#18 in the Standard Areas for Review of the Statewide Assessment System Matrix)
Substitute Care Provider’s Willingness/Ability to Provide Care, Ensure
Safety
The substitute care provider’s ability and commitment to the care and safety of the child.
[This includes the willingness to accept the child into their home and provide for the
child’s daily care and maintenance.] (#17 in the Standard Areas for Review of the
Statewide Assessment System Matrix)
Successful Youth Transition
The desired outcome for youth who experience extended stays in foster care, achieved by
the effective provision of a variety of services (e.g., health and mental health, education,
employment, housing, etc.), continuing through early adulthood, while simultaneously
helping youth to maintain, re-establish or establish strong and enduring ties to one or
more nurturing adults. (Promising Practice)
Support System
Refers to an informal network of people, resources, and/or organizations whose
assistance and encouragement strengthen an individual's or family’s functioning.
System Improvement Plan (SIP)
A key component of the C-CFSR, this operational agreement between the county and the
state outlines a county’s strategy and actions to improve outcomes for children and
families.
Uniform Practice Framework
A fully articulated approach to all aspects of child welfare practice that:
Uses evidence-based guidelines for the start-up phase and ongoing incorporation
of known “best” or “promising” practices
Aligns with sound child and family policy
Is responsive to unique needs of diverse California counties
Can be integrated with a Differential Response system
Addresses shared responsibility with the community
Emphasizes non-adversarial engagement with caregivers
Integrates practice work products from the Full Stakeholders Group and the
Statewide Regional Workgroups.
Violence Propensity/Capability
A pattern of aggressive, coercive, threatening, or potentially harmful behavior or history
on the part of a parent or household member. [The presence of family violence in the
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
home, social isolation, and prior criminal convictions may indicate safety and/or risk
concerns for the child. These include concerns about the child witnessing domestic
violence.] (#6 in the Standard Areas for Review of the Statewide Assessment System
Matrix)
Visitation
The formalized face-to-face contact between a child and a parent(s)/guardian, siblings,
grandparents, or others deemed appropriate by the county or juvenile court to promote the
continuity of parent-child relationships and permanency. (Div 31-002 (v)(1)(B)) [The
duration, frequency, location, and supervision of the contacts will be based on the safety
goals of the case plan, the child’s developmental needs, and the parents’ strengths and
needs. Regular and frequent contacts between parent and child and/or between the child
and his or her siblings help to maintain family relationships, empower parents, minimize
children’s separation trauma, and provide an opportunity for family members to learn and
practice new skills and interactive behaviors.] (#21 in the Standard Areas for Review of
the Statewide Assessment System Matrix)
Voluntary Relinquishment
Process by which parents voluntarily surrender their parental rights and allow their child
to be adopted.
Vulnerable Families
Families who face challenges in providing safe, nurturing environments for their
children, including those demonstrating patterns of chronic neglect; those with young
children (ages 0-5); those impacted by alcohol and drug abuse, homeless/poverty
families, victims of domestic violence; and those with members whose mental health is
compromised.
Welfare and Institutions Code
A series of laws that govern California’s dependency system.
California Common Core Curricula for Child Welfare Workers | Trainer’s and Trainee’s Guide |
Version 1.1, November 2008
Vol. 3, No. 1• January 2002
Helping Workers Apply What They
Learn in Training
When it comes to personnel matters, supervisors and
administrators in social services agencies want one simple
thing: workers who can do the job. To enhance the performance
of their employees, they often send workers to training designed to cultivate
the skills and knowledge workers need. So far, so good.
But no matter how good the training, no matter how engaging and talented
the trainers, if the employee doesn't apply what she learned during the
training when she returns to the agency, then the agency has effectively lost
any benefit it might have derived from the training.
Fortunately, it doesn't have to be this way. According to Mary Urzi,
Director of Family Support Services at Wake County Human Services and
an expert on transfer of learning, there are specific things supervisors and
administrators can do to capitalize on their investment in training.
The following are her suggestions for helping workers apply what they
learn in the classroom to their work with families.
Tips for Administrators
See training as a partnership. Training alone cannot help workers integrate
learning well enough to apply it competently on the job. Nor can
supervisors do it all—they depend on classroom trainers and training
events to organize and formalize learning opportunities and sequences. The
professional development of workers should be seen as a partnership
between supervisors and the child welfare training system.
Proclaim your support. Perhaps the single most important thing agency
directors and administrators can do is to give their "blessing" to training.
They can do this by sending out a letter to staff once a year stating,
"Training is very important to your growth and development. I personally
support and encourage your participation."
Demonstrate your support by providing the resources (time, money)
necessary to send people to training. If your budget is such that you can
send only ten people a year, make sure those ten really feel they have the
support of the agency behind them.
Tips for Supervisors
Ask your own supervisor for support. Explain to her why you believe
training is important and describe specific ways she can support you and
your workers in this area.
Strive for the "three rights." Agencies benefit the most from training if they
send the right person to the right training at the right time. Urzi gives the
following example: "Right now, many new workers are not getting to the
200 series until they've been on the job for nine months or a year. That's not
the optimal timing for the 200 series, which should really occur within the
first three to six months of someone coming to child welfare."
Clarify your expectations prior to training. In brief, individualized pretraining conferences, discuss the learning outcomes of the training and help
workers make the connections between the training they're attending, their
own performance, and the goals and mission of the program.
Emphasize the importance of "action plans." Incorporated into much of the
training offered by the Division, action plans take many forms, but
generally challenge workers to think of strategies for enhancing their
practice based on what they learn in the classroom.
Hold a post-training conference with the trainee. Supervisors can do this
as part of regular supervisory conferences or as a special meeting where the
two of you might review a service plan and discuss how the worker applied
what he learned to the creation of the service plan.
Be purposeful. Be clear about why you're sending workers to a particular
training, why it's important, and what you want them to get out of it.
Communicate all of this to workers and then follow up with words and
actions that encourage them to integrate what they've learned into their
practice. Do this, and chances are you'll be getting everything you can out of
training.
Supervisor Interventions to Enhance
Transfer of Learning
Before Training
1.
2.
3.
4.
Conduct pre-training conference with trainee
Discuss workshop expectations with supervisee
Begin to plan for action plan
Convey training as a priority
During
1. Insure there are no distractions (cover for trainee, if necessary)
2. Convey training is a priority
3. Discuss training and application of what she has learned with
worker between sessions, if multiple-day training
4. Attend training
After
1. Meet with supervisee within a week to review key points in training
and action plan
2. Provide worker opportunity to try out new skills
3. Provide reinforcement for use of new skills
4. Reduce barriers to application of new skills
Source: Curry, D.H., Caplan, P., & Knuppel, J. (1994). Transfer of training and adult learning
(TOTAL). Journal of Continuing Social Work Education, 6(1), 8-14.
Register for Training On-line!
Registering for child welfare training is easier than ever, thanks to the
newly developed web site for the North Carolina Statewide Training
System (NCSTS). This site allows individuals to register for upcoming
training events directly on-line. After they register, individuals receive a
registration confirmation via U.S. mail.
Like the biannual training calendar, this site also provides a description of
the training objectives and target audience for each curriculum offered, as
well as detailed information about specific training events.
The NCSTS is sponsored by the NC Division of Social Services and
developed by the Jordan Institute for Families at the UNC-Chapel Hill
School of Social Work. The Division and the Jordan Institute are excited
about this new means of facilitating the registration process and conserving
paper.
We hope you'll visit our web site soon! The address is
http://sswnt5.sowo.unc.edu/ncsts/pub/index.htm
© 2001 Jordan Institute for Families