OT/PT Referral Form

Revised 9-09
Kenton County School District
Therapy Services Referral
Student Name: Date of Birth:
School Grade:
(Indicate AM/PM for Pre School or Kdg)
School Contact Person: Phone:
Parent/Guardian: Home Phone : Work Phone:
Diagnosis or Special Education Qualification:
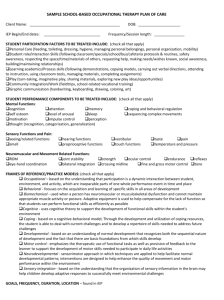
Therapy Services Requested Occupational Therapy (self-help, fine motor)
Physical Therapy (positioning, mobility, gross motor)
Request PT services for Positioning, Mobility, and Gross Motor Skills
Request OT services for Fine Motor Skills, Self Help Skills, and Motor Planning
Student is currently enrolled in special Education** YES NO
Individual Education Program (IEP) has been developed YES NO
Services are required to meet goals and objectives on IEP YES NO
NOTE: ** (student must be enrolled in Special Education and unable to meet IEP goals and objectives without therapy services)
Referral Status Initial Referral for Evaluation
Date ARC signed for permission
Re-evaluation (3 year)
Date Re-evaluation is due
Referral for Services (evaluation completed and attached)
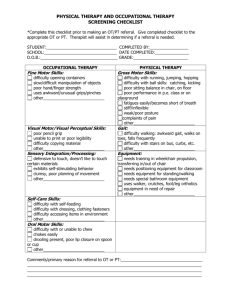
Check the areas of difficulty and the specific problems observed in each area:
Positioning
1.
2.
3.
postural abnormalities (slouched posture, scoliosis)
abnormal muscle tone (rigid, floppy, fluctuating)
equipment (wheelchair, braces, splints)
Mobility
1.
within the classroom
2.
3.
4.
5.
6.
7.
through doorways
hallways
in/out school building
playground
stairs and/or curbs
lunchroom
Gross Motor Activities
1.
2.
3.
4.
unable to sit without support
unable to change positions
unable to stand independently
poor balance
5.
6.
clumsiness
poor body awareness in space
Revised 9-09
3.
4.
5.
6.
7.
Fine Motor
1.
2.
difficulty bringing hands to midline, or to mouth
avoids using one hand
inability to use both hands together (hold paper when writing, lid on jar, etc)
poor handwriting (size, spacing, legibility, pencil pressure, tracing, copying)
letter reversals or omissions
poor eye-hand coordination
lack of hand dominance
Self Help Skills
1.
difficulty in feeding (lip and tongue control, utensil use, drooling, sucking, etc)
2.
3.
4.
5.
poor manipulation of fasteners, orientation of clothes
difficulty in school routine (use of locker, carrying lunch tray, etc)
poor hygiene (toileting, tooth brushing, etc)
Difficulty using alternative communication mode (pointing to pictures, using switches, etc.
Motor Planning
1.
2.
3.
4.
5.
difficulty with rapid learning of new motor tasks
inability to reproduce patterns
inability to imitate gross and fine motor movements
difficulty with sequencing motor tasks
inability to cover surface (wash table, sweep floor, fill up art paper)
Additional Comments and Concerns:
Yes No
Interventions have been implemented for 6-8 weeks with little or no progress.
Area of difficulty has an adverse effect on the student’s educational success.
Evaluation plan has been completed and signed by the ARC.
Student moved into the district with OT/PT already on IEP. If yes: Level of service is
Thank you for completing this form electronically. When completed, save the document with your name and the date, attach it to an email, and send to the appropriate therapist.
For Department Use Only
Therapist Signature:
Date Referral Received:
Evaluation Completed: