De-constructing the Value Proposition of a Service Innovation
advertisement

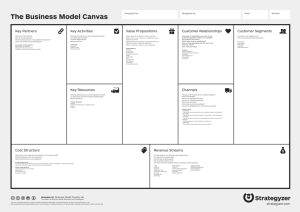
Deconstructing the Value Proposition of a Service Innovation Exemplar The value proposition has become one of the terms most widely used in business (Anderson, Narus & van Rossum, 2006). Webster (2002) suggests that the value proposition “should be the firm’s single most important organizing principle” (p.61). Research into the identification and development of value propositions has been highlighted as one of the key research priorities for the period 2010-2012 by the Marketing Science Institute (MSI, 2010). However, despite its importance there is surprisingly little academic research on how value propositions are identified and constructed. A literature review revealed few examples or illustrations of how value propositions are developed by organizations and little effort aimed at deconstructing value propositions into their constituent components. The process of deconstructing an organization’s value proposition is important, as it permits identification of the key building blocks by which superior value is offered to customers. This gap in the literature, together with the importance of this topic (Webster, 2002), motivates this study. The aim of this paper is to (1) develop an approach for deconstructing the value proposition of a service innovator and (2) identify the key components of this proposition that constitute value. The paper is structured as follows. First, we provide a brief overview of the value proposition concept. Second, we discuss the concept of deconstruction and explain how we selected one service enterprise, Shouldice Hospital, for analysis. Shouldice is an exemplar enterprise that has revolutionized the service experience of repairing hernias, by offering a highly innovative value proposition. Third, we outline the data sources and research method. Fourth, we deconstruct the Shouldice value proposition into its constituent components. Finally, the research contribution, managerial implications and future research are discussed. The Value Proposition It is not our purpose to rehearse a detailed review of the literature on value propositions. For a review of this literature, see Frow and Payne (2008). Rather, we wish to provide a brief overview of the concept which was first introduced by Bower and Garda (1985). Some years later, Lanning and Michaels (1988) described a value proposition as “what precise benefit or benefits at what price will be offered to what customer group, at what cost” (p. 3). Despite more than two decades passing, this topic has received relatively little detailed academic attention. We identify three key themes relating to work in this area. First, value propositions and the identification of competitive strategies. For example, Treacy and Wiersema (1995) describe value propositions in the context of three value disciplines and Kambil, Ginsberg and Blosch (1996) develop a value map aimed at identifying strategies relating to the benefits and price of different competitive propositions. Second, some limited work considers the construction of value propositions. For example, Anderson, Narus and Van Rossum (2006) propose that organizations typically adopt one of three approaches in developing value propositions: all benefits; favorable points of difference; and resonating focus. Rintamaki, Kuusela and Mitronen (2007) propose four broad categories of value propositions including those that reflect: economic value; functional value; emotional value; and symbolic value. Third, value propositions described in the context of experiential value. For example, Lanning (1998) emphasizes the co-creation perspective with less emphasis on ‘delivery’ of value propositions. Vargo and Lusch (2004; 2008) extend these ideas in their foundational premise dealing with value propositions. Our overview of the value proposition literature and earlier work (Frow & Payne, 2008) suggests that there is limited research on this topic and none that addresses a structured process for deconstruction of existing value propositions. We contend that an in-depth analysis of best-in-class exemplar companies through value propositions deconstruction is important as it can yield new insights for managers seeking to develop their own innovative value propositions. 1 Deconstruction and Selection of a Best-in-Class Exemplar Deconstruction is a form of analysis that involves the critical practice of literally taking apart the meanings of that which is socially-constructed (Goodall, 1991). The purpose of deconstruction is to question what is ‘taken for granted’ and how things ‘got this way’ (Eisenberg & Phillips, 1991). Within the management marketing literatures there is an increasing interest in the concept of deconstruction (Ehrensberger et al., 2000) in a number of industry and managerial contexts. The business system concept developed by consulting firm McKinsey & Co. (Gluck, 1980; Bauron, 1981; Bales et al., 2000) provides a structure for analyzing and deconstructing an enterprise’s value proposition. The value chain developed by Porter (1985) draws heavily on the notion of the business system concept. In this paper we utilize the business system concept as a framework, rather than the value chain for several reasons. First, we are less concerned with the value chain’s ‘support activities’ (Porter, 1985). Second, the linkage between the value proposition and the business system is more explicitly made in the literature (Coyne, 2009). Third, the business system addresses criticisms of linearity and unidirectionality (e.g., Normann & Ramírez, 1993), which argue that the value chain representation does not sufficiently emphasize the value-creating system itself. We used three criteria in determining a suitable service enterprise. First, to identify a service enterprise that is a highly regarded best-practice exemplar within its sector. Second, to select an enterprise recognized as having an outstanding and innovative value proposition. Finally, given recent emphasis on co-creation of value, to select an enterprise where cocreation makes an important contribution to the value proposition. The researchers independently compiled a shortlist of alternatives case studies and using the three selection criteria, they choose Shouldice Hospital. It is described as one of the world's best service companies and the ‘world’s best hospital’ (e.g., Heskett, Schlesinger & Sasser, 2003), with an outstanding, innovative value proposition (Hwang, 2009) and cocreation forms an integral part of its service system (Heskett, Sasser & Wheeler, 2008). Data Collection and Method In the context of academic research, scholars such as Yardley (2000) emphasize that it is desirable to employ “triangulation of data collection” in order “to achieve a rounded multilayered understanding of the research topic” (p. 222) by gathering data from different sources and by different methods. Our data generation involved triangulation of data collected from different sources and by different methods, as shown in Appendix 1. As outlined in Appendix 1 in the ‘research method’ section, using these data sources, the researchers progressively examined and interpreted the data to: provide an overview of the operation of Shouldice Hospital; identify Shouldice’s value proposition; determine the discrete elements of Shouldice’s business system; and, more substantively, identify and categorize the many components of value adding activity that collectively represent a deconstruction of Shouldice’s value proposition. Given the scope of Shouldice’s activities, we purposively selected these multiple data sources to gain a comprehensive, rich understanding of the organization and to permit triangulation of data. Shouldice Hospital - a Best-Practice Exemplar The Shouldice Hospital Hernia Centre is located in a suburb of Toronto, Canada. The hospital is renowned globally for its innovation and sole specialization in repair of external abdominal hernias. Dr. E. E. Shouldice founded the Shouldice Hospital focusing on a surgical technique he developed during World War II. At this time, this form of surgery normally involved three weeks of hospitalization. Dr Shouldice reduced this time to less than one week. This new 2 innovative method of hernia surgery involved several breakthrough ideas. First, the hernia operation can be performed with a local anesthetic, rather than a general anesthetic. Second, early ambulation following surgery contributes to a faster recovery. Third, Dr Shouldice proposed the design of a totally integrated hospital environment for hernia repair and recovery that would facilitate patients moving about and exercising to hasten recover. The Shouldice Method, as practiced at Shouldice Hospital, is recognized as the gold standard in hernia repair (Hay et al., 1995). It has proved to be an exceptionally reliable, safe and cost-effective method of external abdominal hernia repair. Because the operation is carried out under local anesthesia, the risks associated with general anesthesia are avoided. Shouldice Hospital also benefits from scale and standardization. An average general surgeon might only perform 25-50 hernia operations in one year. Shouldice Hospital surgeons each perform up to 700 operations a year. Shouldice has repaired more than 330,000 hernias with a greater than 99% success rate. As Gummesson (2009) points out, the almost nil recurrence rate is as close to zero defects, or Six Sigma, that you can possibly get in a hospital. Shouldice Hospital does not have a formal explicit statement of its value proposition (Urquart, 2010). This is not surprising. Some implicit value propositions are successful because an entrepreneur has a clear vision (Lanning & Michaels, 1988), as is the case with Shouldice. Lanning and Michaels (1988), propose a structure for representing a value proposition through a formal statement of: the target customers; the key benefits offered; the price relative to the competition; and a concise summary of the value proposition. Using this structure and following a subsequent member check (Hirschman, 1986; Wallendorf & Belk, 1989) with Shouldice’s Business Development Director, where minor adjustments were made, we present a value proposition statement for Shouldice Hospital in Figure 1. Figure 1: Shouldice Hospital Value Proposition Ta rg et cu s to m ers : • O th e rw is e h e a lth y m a le s w ith e x te rn a l in g u in a l h e rn ia w illin g to tra v e l to O n ta rio C a n a d a to re ce iv e ‘g o ld s ta n d a rd ’ h e rn ia re p a ir K ey b en ef its o f f ered : • h ig h ly s k ille d a n d s p e cia liz e d s u rg e o n s p e rf o rm in g ju s t o n e f o rm o f o p e ra tio n • f a s t s p e e d o f s u rg e ry • h ig h s u cce s s ra te • e x ce p tio n a lly lo w co m p lica tio n s a n d re cu rre n ce • f a s t re co v e ry a n d re tu rn to n o rm a l d u tie s • lo w lik e lih o o d o f in f e ctio n • a n x ie ty a n d te n s io n re d u ctio n • clu b - lik e a tm o s p h e re a n d g ro u p th e ra p y – m o re lik e a re s o rt h o te l th a n a h o s p ita l • A f te rca re , ch e ck u p s f o r lif e a n d lo n g - te rm re la tio n s h ip s P rice rela tiv e to co m p etitio n : • Lo w , h ig h ly co m p e titiv e p rice - ty p ica lly a b o u t h a lf co m p a ra b le co s ts f o r h e rn ia s u rg e ry a n d re co v e ry S u m m a ry o f v a lu e p ro p o s itio n : • H ig h ly s u cce s s f u l h e rn ia s u rg e ry u s in g a p ro v e n te ch n iq u e – “T h e S h o u ld ice M e th o d ” - u n d e rta k e n in a co m f o rta b le a n d s u p p o rtiv e e n v iro n m e n t, w ith f a s t re co v e ry a n d little lik e lih o o d o f f u tu re p ro b le m s Deconstruction of the Shouldice Value Proposition We adopted a deconstruction methodology, breaking down the business system into component parts and analyzing their contribution to the value creation process in terms of differentiators and cost drivers. The key business system activities for Shouldice identified during the research process (see Appendix 1) consist of seven elements: facilities design; 3 diagnosis; admission & pre-operation; the operation; patient recovery; post-operative service; and marketing. The business system concept also provides a structure for understanding the cost drivers and differentiators that collectively form the key components of the Shouldice value proposition. As outlined in in Appendix 1, our analysis identified 116 component differentiators and cost drivers through a process of independent coding of the data by the two researchers. Appendix 2 summarizes these key cost drivers and differentiators for each part of the business system. Given the page limits, it is not feasible to discuss all these differentiators [D] and cost drivers [C]. Instead, for each of the seven elements of the business system, we provide some brief illustrations of them below and we provide a detailed summary of the full range of differentiators and cost drivers in Appendix 2. (1) Facilities Design: The facilities have been carefully designed to make the patient’s experience positive and memorable rather than a traumatic one [D]. The facilities of Shouldice Hospital have also been configured with low-cost in mind. All the bedrooms in the hospital are double occupancy and have a high room utilization rate [C]. (2) Diagnosis: Carefully planned procedures have been developed to ensure that only patients who are healthy, apart from their hernia, are operated on at Shouldice [C&D]. All aspects of diagnosis carried out before arriving at Shouldice and before admission are aimed at providing a suitably qualified and screened patient base [D]. (3) Admission and Pre-operation: On arrival at the hospital, patients are examined by a surgeon to confirm that they are acceptable for admission. Following a check, they are admitted and undertake a new patient orientation [D]. After dinner and recreation they retire to bed in preparation for the operation on the next day. (4) Operation: As outlined above, the development of the Shouldice Method involved several highly innovative concepts including undertaking hernia operations under a local anesthetic [C&D], utilizing early ambulation after surgery to facilitate faster recovery [C&D], and the benefits of a totally integrated hospital environment that involves ‘mental medicine’ and ‘group healing’ [D]. (5) Recovery: Shouldice encourages patients to interact extensively with one another and build relationships with each other during their recovery [D]. Many aspects of the recovery process act as both a cost driver and a differentiator. (6) Post-operative service: Once the patient leaves Shouldice Hospital, considerable effort is placed on maintaining the patient relationship [D]. In what is possibly the longest running post-operative follow-up medical research program in the world, Shouldice gathers post-operative condition and satisfaction reports from all former patients annually [D]. (7) Marketing: Shouldice is in an enviable position in that much of the marketing is through the word-of-mouth of patients and their relatives, as well as intermediaries such as referring doctors [C]. The identification of cost drivers and differentiators discussed above and summarized in Appendix 2 provides a framework for understanding the key components of Shouldice’s value proposition. Our representation in the central element of Appendix 2 develops the business system further and, importantly, highlights its systemic nature. It also addresses criticisms (e.g., Normann & Ramirez, 1993) which argue that a value chain representation is too linear and unidirectional and does not sufficiently emphasize the value-creating system itself. Our development of the business system concept in Appendix 2 explicitly recognizes that value arises from the customer’s processes as well as those of the firm. This is shown in the central section of Appendix 2. It highlights the value-in-use (e.g., Vargo & Lusch, 2004; 2008) that results from the communication encounter, the service encounter and the usage encounter. The importance of these three elements has been highlighted both conceptually and empirically in recent literature (Payne, Storbacka & Frow, 2008; Lemke, Clark & Wilson, 2010) 4 Conclusions, Managerial Implications and Future Research A key Marketing Science Institute research priority for 2010-2012 is the identification and development of value propositions. Our research makes two contributions to the literature on the identification and development of value propositions. First, we develop a structured approach to the identification, analysis and deconstruction of the value proposition and we use this approach to explore the anatomy of a service innovation exemplar. Second, existing conceptualizations of the business system fail to explicitly acknowledge the value-in-use (Vargo & Lusch, 2004; 2008) that results from key encounters and to reflect the interactive and recursive nature of learning processes within the business system. Our extension of the business system concept, shown in the central section of Appendix 2, explicitly addresses these aspects of value creation. This research has important managerial implications for both the health care sector and industry more generally. Developing improved value propositions through deconstructing the business system and identifying differentiators and cost drivers as outlined above, should result in better health outcomes. Hernia repair is the most common operation in general surgery. In the US alone, some 700,000 patients seek hernia treatment and nearly 800,000 patients seek to avoid hernia surgery, often claiming disability because of the presence of a hernia – this represents a health care cost of over US$3 billion (Stylopoulos, Gazelle & Rattner, 2003). Further, there is a cost to the economy incurred by some 15 million per annum lost working days because of hernias (Memon & Fitgibbons, 1998). A further important managerial implications is that specialisation in healthcare is likely to create better outcomes (differentiation) and realize lower costs (cost drivers). Some more general managerial implications also emerge from our study. Whilst the focus of this paper has been on the service sector, managers in firms in all industry sectors need to consider their value propositions. They should consider how their value proposition might be deconstructed and consider under what conditions value could be reconfigured. Importantly, the deconstruction of the value proposition outlined in this paper frees executives from only gaining general learning from best-in-class case studies. As one executive we exposed this research to commented: “It permits a shift from ‘it’s really interesting what they have done’ to ‘this is how they did it’. This provides great insight into how we can develop an improved value proposition for my company”. Research into value propositions is at an early stage of development, hence the discovery-oriented approach adopted in this study. This topic has considerable research potential. There are also limitations relating to the current study which suggest areas for potential future research. First, more general research into the value proposition concept is required. There is the need for a definitive review of the value proposition concept, its adoption in industry and the development of a conceptual framework that integrates different perspectives, contributions and insights from the literature. Second, this study has focused on value proposition deconstruction for only one service innovator. Future research could extend the analysis to other health care exemplars, other organizations in the service sector, and other industry sectors such as business-to-business and consumer goods. Third, application of the learning from value proposition deconstruction in other best-in-class companies represents an area with considerable potential. Finally, the role of co-creation in developing improved value propositions requires further investigation. Prahalad and Ramaswamy (2004) highlight the co-creation opportunities resulting from the transformation of customers from ‘passive audiences’ to ‘active players’. The obvious benefits of co-creation in enhancing Shouldice’s value proposition and the recent heightened interest in co-creation in the literature suggest this as an area of research opportunity. 5 Appendix 1: Data Collection, Sources and Research Method Data Sources Source Details Interviews, discussion and correspondence Business Development Director, Shouldice Hospital Formal Presentation Business Development Director, Shouldice Hospital Video documentary and audio transcript Observation and analysis of transcription of video from Canadian Broadcasting Commission Documentation from Shouldice Hospital Written materials and extensive on-line materials produced by Shouldice Discussion forum involving 35 former patients on website In-depth case studies of Shouldice Hospital Shouldice Hospital patient surveys Health forum website (ehealthforum.com, 2010) Observation of hernia operation Observation in operating theatre of a hernia clinic during an operation Review of academic and managerial literature on Shouldice Hospital Heskett, Schlesinger & Sasser, 2003; Herzlinger, 2004; Urquhart & O'Dell, 2004; Christensen, 2007; Ferguson, Paulin & Leiriao, 2007; Frei, 2008; Gummesson, 2009 Review of medical literature on Shouldice Method and other methods of hernia repair Bendavid, 1989; 1995; 2003; Froom et al., 2001; Papadakis & Greenburg 2002; Shouldice, 2003; Welsh and Alexander, 1993; Hay, et al., 1995; Rutkow, 1998; Bax et al.,, 1999; Schneider et al. 2008 Heskett & Hallowell, 2004; Pope, Stephenson & Haywood, 1997 Ferguson, Paulin & Leiriao, 2007; Ferguson, Paulin & Bergeron, 2010 Research Method 1. This exploratory research used mixed methods and data sources that were selected to provide a rich picture of the organisation, its business system and value creation. Initially, extant literature was reviewed, with additional literature and data sources purposively selected to enrich understanding and provide a comprehensive picture of Shoudice, its business system and value proposition. 2. Starting with the most detailed and comprehensive sources, including a transcription of the video documentary, each set of data was studied in detail to ensure a ‘rich picture’ (Hoskisson, Hitt, Wan & Yiu, 1999) of the organization, including its unique context and idiosyncrasies. 3. The two researchers independently reviewed the data sources outlined above and made detailed notes on their views of Shouldice’s value proposition. Using the structure suggested by the originators of the value proposition concept, they iteratively developed a final draft of a value proposition statement for Shouldice. This draft was subject to a ‘member check’ (Wallendorf & Belk, 1989) by the Business Development Director of Shouldice and following minor modification, a final value proposition statement was developed. 4. The researchers next considered Shouldice’s business system. A draft of the business system elements was developed independently by the researchers and then compared. An initial business system representation was then developed. This went through some minor modification and a member check before finalization. It aimed at providing a framework for value proposition deconstruction rather than attempting to include mundane day-to-day ‘support activities’ common to other organizations. 5. The researchers then considered cost drivers and differentiators for each element of the business system. In order to achieve ‘triangulation across researchers’ (Belk, Wallendorf & Sherry, 1989), which permits with a check on completeness and interpretation from different researchers’ viewpoints, the researchers worked independently. The researchers each highlighted relevant sections in separate copies of the text of the materials and transcript and noted what they observed in the video material. They then coded each identified component, including where each cost driver or differentiator fitted within the business system. Analysis followed the constant comparative method (e.g., Glasser & Strauss, 1967), whereby findings from the next piece of data were progressively compared to previous data. The researchers continued this process until they each felt confident that they had identified key components of Shouldice’s value proposition. 6. The researchers reviewed and refined their findings during several lengthy review sessions in order to determine the key components of the deconstructed value proposition. Finally, they developed a joint list of some 116 component differentiators and cost drivers. These components were then coded in a spreadsheet so their role as a differentiator or cost driver for different parts of the business system was classified. Overall, there was a very high degree of unanimity amongst the two researchers in their representation of the deconstruction of the value proposition, although there were some minor differences. A small number of variances were resolved through discussion, revisiting the data sources and the subsequent ‘member check’ by Shouldice’s Business Development Director. Thus, the cost driver and differentiation elements, the structure of the business system and the description are based on research that reflects researcher consensus substantiated by member check. 6 DI FERE NT I ATOR S Appendix 2: Deconstruction of the Shouldice Hospital Value Proposition COS T DR I VE RS BUSINESS SYSTEM • Country club, rather than a hospital • Operating theatres out of sight in basement • Investments in assets important to patient comfort and recovery • Areas where patients can meet and engage in social interaction and group activities • Beautiful landscaped grounds • Club-like atmosphere • “Guest” not patient • Low-rise stairs facilitates mobility. • A thorough diagnosis is made before admission • Very specific target market. • “Shouldice is for me” • Low risk • Patients receive assurance • Communication of the substantially higher success rate and lack of complications • Branding: “the Shouldice Method • Overall cost - benefit for patient of having their operation performed at Shouldice • Procedure is explained in detail and sets patient expectations , patients are not kept in the dark • Expectations are set :“you will survive -- everybody does” • Briefing represents the start of Shouldice’s “sharing” culture and aims at reduction of patient fear and anxiety • Reassurance and managing mental state of patients • Length of stay. • Educating the patient FACILITIES DESIGN DIAGNOSIS ADMISSION & PREOPERATION • Suburban rather than an expensive city centre location • Facilities represent low cost by today's standards • One type of operation • Integrated basement activities • Rooms in the hospital are double occupancy • Rooms have a high utilization rate • Bedrooms have "low capital investment" • Meals are served in the dining room rather than being delivered to patients’ rooms • Wide catchment area for its patients, including USA, lowers average cost of diagnosis • Low cost initial selfdiagnosis using on-line Medical Information Questionnaire • Screen out unhealthy patients. • Patients who are overweight are retained, they are counseled to lose weight and be at an acceptable weight before Shouldice will admit them • Low cost lay staff review questionnaires • Group briefing is undertaken by a nurse with around 30 new patients • Meals before operation taken in a communal dining room rather than served in patient bedrooms. • Minimal need for trolleys and orderlies to take and collect meal trays from rooms • Patients teamed up with roommates who have experience of operation and can answer patient queries them afterwards • Innovative technique • Proven technique • High order reliability • Very skilled surgeons • Local anesthetic rather than general anesthetic • Patients are awake during surgery • Surgeons who are experts in procedure • Vast amount of total accumulated experience • Short time in the operating theatre • Quality control • High success rate • Low risk associated with the operation. • Fast recovery time • No recurrence is ever likely • Fun atmosphere • Exercise classes • Group activities golf putting pool/billiards exercise in extensive grounds • Length of stay • Experience sharing • Low risk • Hospital staff encourages continual engagement with other patients • Group therapy • Self healing • Low recurrence rate for hernia repairs undertaken at Shouldice • Members of an alumni club • Regular newsletter contact • Over 130,000 annual follow-up letters • Five travelling clinics are conducted annually • 12,000 patient follow-up examinations each year • Part of a “club” • Shouldice patient alumni reunion • Continuing relationship • ‘Esprits de corps’ OPERATION RECOVERY POSTOPERATIVE SERVICE • Only one operation type • 340,000 operations • Specialized & standardized procedure • High throughput • No errors/rework • Experience curve • ‘Surgeons assisting surgeons program’ • Relatively low technology • Limited medical equipment required • Local anesthetic • Specialized anesthetist not required • Specialized & inexpensive surgical pack • Focused training for doctors and for nurses • Patient s are encouraged to manage their own recovery • Group exercise classes involve around 60 patients and are conducted by relatively low cost nurse. • Group therapy through patient to patient interaction makes contact with the doctors & nurses less necessary. • No meals in rooms (except for first one after operation) • Less post-operative recovery rooms needed for patients • Low recurrence leads to less post-operative contact with hospital staff • Patient follow-up data helps identify medical issues that can be addressed at earlier stage • Follow-up program uses low cost e-mail • Post-operative follow-up data build support and endorsement by the medical community. • Follow-up program helps builds patient confidence and high levels of postoperative satisfaction • Track record • Patients confidence • 65 years of operations • 340,000 success stories • High customer advocacy • Branding “the Shouldice method” • Overall cost/benefit • No-one dies! • Little chance of problems • Clergy probono operations • Strong alumni bond • Extensive media exposure • Reputation: “the best hospital in the world • Stay 72 hours vs. 6 days MARKETING • High level of referrals means no sales force is needed • Extensive free publicity including press coverage and TV coverage • Clergy act as an referral source • Low cost exposure though academic sources e.g., over 300,000 copies of one case study sold • Check-up keeps Shouldice “top of mind” • Reputation of the hospital is so strong a very large number of patients are recruited from outside Canada 7 REFERENCES Anderson, J, Narus, J, & Van Rossum, W. (2006). Customer value propositions in business markets. Harvard Business Review, (March), 91-99. Bales, C F., Chatterjee, P. C., Gluck, F. W., Gogel, D., Puri, A. & Watters, D. C. (2000). The microeconomics of industry supply. McKinsey Quarterly, (June), 22-25. Bauron, R (1981). New game strategies. The McKinsey Quarterly, (Spring), 24-40. Bax, T., Sheppard, B. & Crass, R. (1999). Surgical options in the management of groin hernias. American Academy of Family Physicians, 59 (1), 143–56. Belk, R. W., Wallendorf, M. & Sherry, J. F. (1989). The sacred and profane in consumer behavior: theodicy on the odyssey. Journal of Consumer Research, 16, (June), 1-38. Bendavid, R. (1989). New techniques in hernia repair. World Journal of Surgery, 13, 522–31. Bendavid, R. & Shouldice, E. E. (1995). A biography. Problems in General Surgery, 12, (1), 1– 5. Bendavid, R. (2003). Biography: Edward Earle Shouldice (1890–1965). Hernia, 7, 172–177. Bendavid, R., Froom, P., Melamed, S., Nativ, T., Gofer, D. & Froom, J. (2001). Low job satisfaction predicts delayed return to work after laparoscopic cholecystectomy. Journal of Occupational and Environmental Medicine, 43 (7), 657–662. Bower, M. & Garda, R.A. (1985). The role of marketing in management. The McKinsey Quarterly, 3, 34-46. Christensen, C. (2007). Disruptive innovation in education & health care. Presentation at Harvard Business School, (November). Coyne, K. (2009). Enduring ideas: the business system. McKinsey Quarterly, (June), https://www.mckinseyquarterly.com/Enduring_Ideas_The_business_system_2379. [Accessed 2 April 2010]. Ehrensberger, S., Opelt, F., Rubner, H. & Schmiedeberg, A. (2000). Dealing with deconstruction. In R. K. F. Bresser, M. A. Hitt, R. D..Nixon & D. Heuskei (Eds.), Winning Strategies in a Deconstructing World (pp.191-200). Chichester, England: John Wiley & Sons, Ltd., Eisenberg, E. & Phillips, S. (1991). Miscommunication in organizations. In N. Coupland, H. Giles & J. M. Wiemann (Eds.), Miscommunication and Problematic Talk (pp. 244-58). Newbury Park, CA: Sage, Ferguson, R. J., Paulin, M, & Bergeron, J. (2010). Customer sociability and the total service experience: antecedents of positive word-of-mouth intentions. Journal of Service Management, 20 (1), 25-44. Ferguson, R. J., Paulin, M. & Leiriao, E. (2007). Loyalty and positive word-of-mouth: patients and hospital personnel as advocates of a customer-centric health care organization. Health Marketing Quarterly, 23 (3), 59 – 77. Frei, F. (2008). The four things a service business must get right. Harvard Business Review, 86 (4), 70–80. Frow, P. & Payne, A. (2008). The value proposition concept: evolution, development and application in marketing. Academy of Marketing Conference, Aberdeen, July. 8 Glasser, B. & Strauss, A. (1967). The Discovery of Grounded Theory: Strategies of Qualitative Research. London: Wiedenfeld & Nicholson. Gluck, F .W. (1980). Strategic choices and research allocation. The McKinsey Quarterly, 1, 22– 33. Goodall, H. L. (1991). Living in the Rock n Roll Mystery: Reading Self, Others, and Context as Clues. Carbondale, IL: Southern Illinois University Press. Gummesson, E. (2009). Marketing as Networks: The Birth of Many-to-Many Marketing. Stockholm, (forthcoming , preliminary translation). Hay, J.M., Boudet, M.J., Fingerhut, A., Pourcher, J., Hennet, H., Habib, E., Veyrieres, M. & Flamant, Y. (1995). Shouldice inguinal hernia repair in the male adult: the gold standard? Annals of Surgery, 222 (6), 719–727. Herzlinger, R E. (2004). Consumer-Driven Health Care: Implications for Providers, Players, and Policy-Makers. San Francisco: Jossey-Bass. Heskett, J. L. & Hallowell, R. (2004). Shouldice Hospital Limited. Harvard Business School Case Study, 9-805-002. Boston, Ma: Harvard Business School. Heskett, J. L., Schlesinger, L. A. & Sasser, W. E. (2003). The Value Profit Chain: How to Manage Employees like Customers and Customers like Employees. Boston: Harvard Business School Press. Heskett, J. L., Sasser, W. E. & Wheeler, J. (2008). The Ownership Quotient. Boston: Harvard Business School Press. Hoskisson, R., Hitt, M., Wan, W. & Yiu, D. (1999). Theory and research in strategic management: swings of a pendulum. Journal of Management, 25 (3), 417-456. Hwang, J. (2009). Keynote Address - The innovator's prescription: an examination of the future of health care through the lenses of disruptive innovation. Archives of Pathology & Laboratory Medicine, 133 (4), 513-520. Kambil, A., Ginsberg, A. & Bloch, M. (1996). Re-inventing value propositions. NYU Centre for Research on Information Systems. Working Paper IS 96-21, New York: New York University. Lanning, M. (1998). Delivering Profitable Value: A Revolutionary Framework to Accelerate Growth, Generate Wealth and Rediscover the Heart of Business. New York: Perseus Publishing. Lanning, M. & Michaels, E. (1988). A business is a value delivery system. McKinsey Staff Paper, No. 41, (July). Lemke, F., Clark, M. & Wilson, H. (2010). Customer experience quality: an exploration in business and consumer contexts using repertory grid technique. Journal of the Academy of Marketing Science, DOI: 10.1007/s11747-010-0219-0 (forthcoming). Memon, M. A. & Fitgibbons, R.J. (1998). Assessing risks, costs, and benefits of laparoscopic hernia repair. Annual Review of Medicine, 49 (February), 95-109. MSI Research Priorities 2010-2012. Boston: Marketing Science Institute, 2010. Normann, R. & Ramirez, R. (1993). From value chain to value constellation. Harvard Business Review, (July-August), 65-77. 9 Papadakis, K. & Greenburg, A. G. (2002). Preperitoneal hernia repair. In R J, Fitzgibbons & A. G. Greenburg (Eds.), Nyhus & Condon’s Hernia (pp. 181-198). Philadelphia: Lippincott Williams & Wilkins. Payne, A., Storbacka, K. & Frow, P. (2008). Managing the co-creation of value. Journal of the Academy of Marketing Science, 36 (1), 83-96. Pope, J., Stephenson, L. & Haywood, J. (1997), Shouldice Hospital Limited. Richard Ivey School of Business, Case Study 9A98D015, University of Western Ontario. Porter, M. E. (1985). Competitive Advantage. New York: Free Press. Prahalad, C. K. & Ramaswamy, V. (2004), The Future of Competition: Creating Unique Value with Customers. Boston, MA: Harvard Business School Press, Rintamaki, T., Kuusela, H. & Mitronen, L. (2007), Identifying competitive customer value propositions in retailing. Managing Service Quality, 17 (6), 621-634. Rutkow I. M. (1998), Epidemiologic, economic, and sociologic aspects of hernia surgery in the United States in the 1990s. Surgical Clinics of North America, 78 (6), 941-951. Schneider, J. E., Miller, T. R., Ohsfeldt, R. L., Morrisey, M. A., Zelner, B.A. & Pengxiang L. (2008). The economics of specialty hospitals. Medical Care Research and Review, 65 (5), 531-563. Shouldice, E. B. (2003). The Shouldice repair for groin hernias. Surgical Clinics of North America, 83, 1163–1187. Stylopoulos, N., Gazelle, G. S. & Rattner, D. W. (2003). A cost-utility analysis of treatment options for inguinal hernia in 1,513,008 adult patients. Surgical Endoscopy, 17, 180-189. Treacy, M. & Wiersema, F. (1995). The Discipline of Market Leaders. Reading, MA: AddisonWesley. Urquart, D. J. B. (2010). Interview and correspondence. September. Urquhart, D. J. B. & O’Dell, A. (2004). A model of focused health care delivery. In R. E Herzlnger, (Ed.), Consumer-Driven Health Care: Implications for Providers, Payers, and Policy-Makers (pp. 627–634). San Francisco: Jossey-Bass. Vargo, S. L & Lusch, R. F. (2004), Evolving to a new dominant logic for marketing. Journal of Marketing, 68, (January), 1-17. Vargo, S. L. & Lusch, R. F. (2008). Service-dominant logic: continuing the evolution. Journal of the Academy of Marketing Science, 36 (1), 1-10. Wallendorf, M. & Belk, R. W. (1989). Assessing trustworthiness in naturalistic consumer research. In Special Volume: Interpretive Consumer Research, Association for Consumer Research, 69-84. Webster F E. (2002). Market-Driven Management: How to Define, Develop, and Deliver Customer Value. (Second Edition) , Hoboken, New Jersey: John Wiley& Sons, Welsh, D. R. & Alexander, M. A. (1993). The Shouldice repair. Surgical Clinics of North America, 73 (3), 451–69. Yardly, L. (2000). Dilemmas in qualitative health research. Psychology and Health, 15, 215228. 10