Genetic Causes of Bronchiectasis: Primary Ciliary Dyskinesia
advertisement

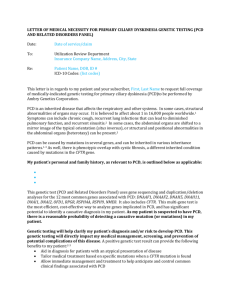
Thematic Review Series 2007 Respiration 2007;74:252–263 DOI: 10.1159/000101783 Genetic Causes of Bronchiectasis: Primary Ciliary Dyskinesia Hilda N. Morillas Maimoona Zariwala Michael R. Knowles University of North Carolina, Chapel Hill, N.C., USA Key Words Bronchiectasis Mucociliary clearance Primary ciliary dyskinesia DNAH5 DNAI1 Situs inversus Kartagener’s syndrome Abstract Primary ciliary dyskinesia (PCD) is a genetically heterogeneous disorder reflecting abnormalities in the structure and function of motile cilia and flagella, causing impairment of mucociliary clearance, left-right body asymmetry, and sperm motility. Clinical manifestations include respiratory distress in term neonates, recurrent otosinopulmonary infections, bronchiectasis, situs inversus and/or heterotaxy, and male infertility. Genetic discoveries are emerging from familybased linkage studies and from testing candidate genes. Mutations in 2 genes, DNAI1 and DNAH5, frequently cause PCD as an autosomal recessive disorder. A clinical genetic test has been recently established for DNAI1 and DNAH5, which involves sequencing 9 exons that harbor the most common mutations. This approach will identify at least one mutation in these 2 genes in 25% of PCD patients. If biallelic mutations are identified, the test is diagnostic. If only one mutation is identified, the full gene may be sequenced to search for a trans-allelic mutation. As more disease-causing gene mutations are identified, broader genetic screening panels will further identify patients with PCD. Ongoing © 2007 S. Karger AG, Basel 0025–7931/07/0743–0252$23.50/0 Fax +41 61 306 12 34 E-Mail karger@karger.ch www.karger.com Accessible online at: www.karger.com/res investigations are beginning to identify genetic mutations in novel clinical phenotypes for PCD, such as congenital heart disease and male infertility, and new associations are being established between ‘ciliary’ genetic mutations and clinical phenotypes. Copyright © 2007 S. Karger AG, Basel Introduction Mucociliary clearance (MCC) is a key component of pulmonary defense mechanisms, which enables the airways to protect the lungs from potentially harmful substances in the surrounding environment, such as infectious organisms, allergens, irritants and chemicals. MCC involves the regulation of ion transport by airway epithelium, ciliary function, and mucus secretion [1]. Disruption of this intricate defense system leads to clinical manifestations of lung disease. Cystic fibrosis (CF) is one example of a recessive disorder in which genetic mutations of CFTR (cystic fibrosis transmembrane conductance Previous articles in this series: 1. Contopoulos-Ioannidis DG, Kouri IN, Ioannidis JPA: Genetic predisposition to asthma and atopy. Respiration 2007;74:8–12. 2. Sztrymf B, Yaïci A, Girerd B, Humbert M: Genes and pulmonary arterial hypertension. Respiration 2007;74:123–132. Hilda N. Morillas, MD CF/Pulmonary Research and Treatment Center University of North Carolina at Chapel Hill 7006 Thurston Bowles Building, CB# 7248, Chapel Hill, NC 27599-7248 (USA) Tel. +1 919 966 6780, Fax +1 919 966 7524, E-Mail hmorilla@med.unc.edu regulator) cause a derangement of ion transport and subsequent ineffective MCC and cough clearance. Primary ciliary dyskinesia (PCD; MIM 242650) is a genetic disorder of motile cilia, and the clinical manifestations reflect ciliary dysfunction in lungs, sinuses, middle ear, male fertility and organ lateralization [2]. Approximately 1 in 30,000 individuals are estimated to have PCD [3], but this could be underestimated because of challenges in establishing the diagnosis. It is a genetically heterogeneous disorder; however, in the majority of cases it is inherited as an autosomal recessive trait. Patients with PCD have impaired MCC, but retain cough clearance as a defense mechanism [4]. Genetics have recently emerged as a critical feature to understand the molecular pathogenesis of PCD and to facilitate the diagnosis and allow better definition of the clinical phenotypes. This article is designed to provide the most current information on the status of genetic discoveries in PCD, which currently stem from family-based genetic linkage studies, and from testing candidate genes derived from knowledge of ciliary structure/function. Understanding the structure and function of cilia can lead to identifying more candidate genes and allow better correlation between genetic mutations and clinical phenotype. Table 1. Clinical manifestations of PCD Organ Clinical manifestation Lung Respiratory distress in term neonates Bronchitis/recurrent infections Bronchiectasis Ears Otitis media Hearing loss Cholesteatoma (after tympanostomy) Nares/sinus Chronic sinusitis Polyposis Genitourinary tract Male infertility Organ laterality Situs inversus totalis Situs ambiguus (heterotaxy), including (a) Polysplenia or asplenia (b) Vascular anomalies (c) Complex congenital heart disease Central nervous system Hydrocephalus (rare) Genetic-based (‘primary’) dysfunction of motile cilia and sperm-tail flagella explains the complex PCD phenotype [3]. Common clinical presentations of the disease include respiratory distress in full-term neonates, situs inversus, recurrent otosinopulmonary infections, bronchiectasis, and male infertility; however, these manifestations vary by age and among patients [5] (table 1). In the lung, MCC is coordinated by motile cilia that line the upper and lower airways. These rod-like organelles extend from the airway epithelial cell surface and move extracellular mucus by synchronized beating. Immotile or dyskinetic respiratory cilia cause defective MCC, and affected individuals have recurrent respiratory infections that lead to chronic infections and inflammation of the upper and lower airways [6]. The disease typically progresses to overt bronchiectasis during late childhood or early adulthood and can ultimately cause chronic respiratory failure [5]. Additionally, intrabronchial calcium deposition with associated lithoptysis has been observed in a subset of older patients [7]. The majority (95%) of PCD patients has a history of recurrent otitis media requiring repeated an- tibiotic treatments, and sinusitis is a universal feature in PCD, demonstrating that ciliary function in the eustachian tube and sinuses is also critical for protection of these organs [5]. Almost all male PCD patients are infertile, due to sperm immobility or dysmotility. In an individual patient, ultrastructural defects of sperm flagella usually resemble those seen in respiratory cilia, but not always [3]. Ciliary dysfunction in the fallopian tubes may contribute to subfertility in affected women [8], although this is difficult to validate. Dysfunction of the embryonic node monocilia is associated with the complete mirror image of the usual arrangement of thoracic and abdominal organs (situs inversus totalis) in approximately half of the PCD patients due to randomization of left-right body asymmetry [9] (fig. 1, 2). PCD with chronic sinus and airway infections, coupled to situs inversus, is also referred to as Kartagener’s syndrome (MIM 244400) [10]. Some PCD patients have neither situs solitus nor situs inversus totalis, whereby some internal organs are located in the usual position, but others are in a mirrored position or in duplicate [11]. This abnormality of organ location is termed situs ambiguus or heterotaxy. A recent review of 337 PCD patients revealed that at least 6.3% (n = 21) had situs ambiguus; 12 of those 21 patients with heterotaxy had cardiac and/or vascular abnormalities, and most (n = 8) had complex congenital heart disease [11]. Thus, cilia-related genes are excellent candidate genes for heterotaxy and congenital PCD and Genetic Mutations Respiration 2007;74:252–263 Defective Cilia and the Clinical Phenotype of PCD 253 Fig. 1. Random left-right asymmetry seen in patients with PCD. Chest radiographs of monozygotic twins with PCD and ultrastructural defects of the IDA [5]. a Dextrocardia and dextrogastria in a patient with situs inversus totalis. b Situs solitus. Arrow is pointing to gastric bubble. heart disease. Patients with situs inversus or heterotaxic anomalies, particularly those with unexplained respiratory symptoms, are at risk of having an underlying defect in ciliary structure, function, and genetics, and should be evaluated for PCD. Conversely, PCD patients should have a cardiac evaluation, particularly those with situs inversus or heterotaxy. Management of PCD Fig. 2. High-resolution chest tomography. The patient is a 24- year-old female with PCD. Her ciliary electron micrograph showed absent ODA and IDA. She has bronchiectasis (B) and situs inversus totalis as demonstrated by a bilobed right lung and the aorta (A) lying along the right side of the thoracic cavity. 254 Respiration 2007;74:252–263 There are currently no treatments to correct the ciliary dysfunction of PCD and standardized treatment has not been defined [12]. Clinicians typically follow the general guidelines for treatment of bronchiectasis, which frequently employs approaches used in CF. Clinical management involves enhancing MCC with physiotherapy, postural drainage, exercise, and/or mechanical oscillatory vest percussion. Although there are no specific research data on the efficacy of hypertonic saline, it can be used empirically to improve MCC. Cough suppressants should be avoided because cough is the only intact mechanism for MCC in these patients [12]. A key component in the management is prevention or rapid treatment of respiraMorillas/Zariwala/Knowles Fig. 3. Electron micrographs (EM) of respiratory cilia. a EM image of a cilium from nasal epithelium of an unaffected individual. Normal-appearing ODAs (black arrow), IDAs and central apparatus are seen. b EM image of a cilium from nasal epithelium of a patient with PCD homozygous for 10815delT mutation in DNAH5. This patient has absent IDAs and ODAs. c EM image of a cilium from nasal epithelium of a patient with PCD. This patient has normal-appearing ODAs but absent IDAs. tory tract infections. Acute infectious exacerbations should be managed with appropriate oral, intravenous or inhaled antibiotics directed by the sputum culture [5, 12]. Patients should receive routine immunizations for respiratory pathogens, avoid exposure to pathogens, and avoid smoking and other irritants that may increase mucus production. Localized bronchiectasis has previously been managed by lobectomy, but its benefit is limited and should be undertaken only after the involvement of experts. Surgical interventions may be required for specific complications of chronic suppurative otitis media and sinusitis such as tympanostomy, nasal polypectomy, and surgical sinus drainage. Lung transplant may be an option for patients with end-stage lung disease [12]. The diagnosis of PCD is often delayed, which contributes to poor outcomes [13]. Early diagnosis in childhood may allow treatment to delay, and possibly prevent, the occurrence of bronchiectasis. For example, in the term newborn, neonatal respiratory distress syndrome and tachypnea can be the first signs of PCD, but this has only recently been highlighted [5, 14, 15]. Therefore, educating clinicians of the typical and atypical clinical features, in addition to molecular and genetic research, is extremely important. The current gold standard for the diagnosis of PCD is determining the ciliary ultrastructure defect via trans- mission electron microscopy (TEM) or clearly documenting ciliary dysfunction via high-speed video microscopy using standardized methodologies [15]. Studies in humans have revealed a spectrum of ultrastructural defects (fig. 3), but the most common defects are absence of the outer dynein arms (ODA) and/or inner dynein arms (IDA). The frequency of isolated ODA defects range between 29 and 43%, isolated IDA defects range between 10 and 29%, and ODA plus IDA defects range between 7 and 57% [5, 16–18]. Other reported defects include absence of the radial spokes, transposition (a peripheral microtubule pair migrates to the center of the cilia because the central pair is missing), and loss of central microtubules [5, 19]. As many as 15% of currently diagnosed PCD patients have no ultrastructural defects [5, 16, 18, 20], but this number is likely to escalate as genetic testing becomes more available, and the diagnosis can be firmly established in the absence of gross ultrastructural abnormalities. A major challenge for the diagnosis of PCD is that TEM does not easily demonstrate all ‘primary’ (i.e., genetic) ultrastructural defects. For example, IDA defects are difficult to define on TEM because of the low contrast and the complexity of the composition and distribution of the IDA. Carlen and Stenram [21] described that the mean number of IDA per cilium was ! 0.6 for subjects with PCD and 3–5 for control subjects, whereas the mean number of ODA per cilium was !1.6 for subjects with PCD, but 7.5–9.0 in control subjects. Computer-assisted analysis of TEM cross-section photographs can sometimes improve IDA visualization [20]. PCD and Genetic Mutations Respiration 2007;74:252–263 Diagnosis of PCD 255 From a genetic standpoint, different mutations are associated with specific ciliary ultrastructural phenotypes. In cases in which no ultrastructural defects are identified, the diagnosis of PCD can be established only if the patient has a compatible clinical phenotype, including situs inversus or heterotaxic defects, together with assessments of ciliary beat frequency and waveform, measurements of nasal nitric oxide (nNO) levels, or the use of immunohistochemical immunofluorescence studies (see details below) [6, 15]. Some patients with PCD may have normal appearing ciliary activity, if viewed only with light microscopy. Acquired, or ‘secondary’, defects can occur with infection, allergic inflammation or environmental exposures, and must be distinguished from primary genetic defects. There are multiple changes in ciliary ultrastructure that have been described as secondary changes, but loss of ODA and/or IDA has not been described [22]. To aid in distinguishing between primary and secondary ultrastructure abnormalities, respiratory epithelial cells can be cultured, but only a few centers perform these techniques and a significant amount of cell material is necessary [18]. The current gold standard for determining ciliary dysfunction is high-speed video microscopy. Ciliated respiratory epithelium should be obtained via a brushing or scraping of the inferior nasal turbinate. Strips of epithelium should be directly examined for ciliary beat frequency and pattern within 2 hours of obtaining the sample at centers familiar with the technique. There are several different methods to measure ciliary beat frequency and to characterize the waveform of ciliary activity, but there are no published data to support the superiority of one method. The normal range is approximately 11–16 Hz, but this varies by temperature and other methodological variables, and experience is required in scoring ciliary activity. It is important to remember that the patient should not have a respiratory infection at the time of sampling because acute infections can cause secondary changes in the function of cilia [15]. The production of nNO is reduced in patients with PCD as demonstrated by Noone et al. [5] and Lundberg et al. [23]. The test is performed by inserting an NO sampling line into one nostril and having the patient inhale deeply and then close the soft palate. Although the mechanism in which nNO is reduced in patients with PCD is still unclear, this test can clearly be used as a screening tool, because there is a significant difference between the nNO level in patients with PCD compared to normal and disease controls [5]. However, it is key to rule out CF, 256 Respiration 2007;74:252–263 since nNO levels in CF patients can overlap with levels of PCD patients. Additionally, it is not invasive, simple to perform, and compared to the saccharin test can be performed on small children. The saccharin test was previously used as an inexpensive and simple procedure to screen adults and older children. A 1- to 2-mm piece of saccharin is placed 1 cm from the anterior tip of the inferior nasal turbinate. The patient sits quietly with his or her head bent forward and refrains from sniffing, coughing or eating during the test. The time it takes for the patient to taste the saccharin is measured. An abnormal test is any length of time greater than 60 min. A normal saccharin test clearly demonstrates normal MCC but the test is time consuming and can be difficult to perform in patients unable to cooperate [15]. This test is very nonspecific and now that more definitive tests, such as TEM and videomicroscopy, and genetic test are available, the saccharin test has no clinical value. Structure of Normal Cilia Cilia are projections from the cell surface that are bound by the cell membrane, and derived from the centriole. The ciliary axoneme is the cytoskeleton of the cilium composed of microtubules. Mammalian ciliary axonemes are formed with 2 major patterns. One pattern, 9 + 2, has nine doublet microtubules surrounding a central pair of singlet microtubules. Cilia containing this axonemal structure are usually motile and several hundred of these cilia are located on airway epithelial cells. Major structures that attach to the microtubules are the ODA and IDA, which are the force-producing units of cilia and flagella. There are approximately 4,000 dynein arms in pairs per cilium. Other defined protein complexes are the radial spokes, which radiate from the central pair, and the nexin links, which connect the outer doublets [24, 25]. The other pattern is 9 + 0, in which the central pair is absent. These cilia are usually solitary and the molecular motors, axonemal dyneins, which are responsible for ciliary movement, are also absent; therefore, these cilia are nonmotile [26]. One exception is the embryonic node cilium, which is a motile, specialized monocilium with a 9 + 0 pattern with dynein arms [9]. It moves in a vortical pattern distinct from the bending movement of the 9 + 2 cilia and plays a key role during embryogenesis for determination of left-right asymmetry, which is thought to result from the movement of liquid surrounding the nodal cilium in a leftward direction [9, 27]. Morillas/Zariwala/Knowles Ultrastructure of ODAs To further understand the normal structure and function of human motile cilia, axonemal genes and proteins of Chlamydomonas reinhardtii, a unicellular green alga with two flagella that extend from its anterior end, have been studied. Axonemal genes are highly conserved throughout evolution [28], and human orthologs have been identified for most genes that encode for axonemal proteins. The ultrastructure of the Chlamydomonas flagellum has a distinctive ODA complex containing 3 heavy chains (HCs), 2 intermediate chains, 9 light chains, and 3 docking complex proteins. The three HCs are , and . Three human orthologs have been identified for the Chlamydomonas HC, DNAH9 (chromosome 17p12), DNAH11 (chromosome 7p21), and DNAH17 (chromosome 17q25). Two human orthologs have been identified for the Chlamydomonas HC, DNAH5 (chromosome 5p15) and DNAH8 (chromosome 6p21) [29]. There have been no human orthologs identified for the Chlamydomonas HC. This is consistent with the concept that the ODA of vertebrates only have 2 HCs. Because multiple orthologs have been identified, it is thought that humans might have several types of ODA complexes, and recent data support that notion. Fliegauf et al. [30] used specific antibodies against DNAH5 and DNAH9 and confocal immunofluorescence to localize the ODA HC complexes along the axoneme. In wildtype respiratory cells, DNAH5 is present throughout the entire length of the ciliary axoneme, whereas DNAH9 localizes only to the distal portion of the cilium. In contrast, in sperm cells the DNAH9 protein is present along the entire length of the sperm tail and DNAH5 localizes solely to the proximal part of the flagellum. Thus, there are at least 2 types of ODA present in respiratory cilia and sperm flagella. Type 1 stains positive for DNAH5 and negative for DNAH9, and type 2 ODA stains positive for both DNAH5 and DNAH9. This difference in localization of different HCs in ODA complexes along the longitudinal axis likely contributes to the characteristic beating pattern of respiratory cilia and sperm flagella [30]. patterns along the doublet microtubule of the flagellar axoneme. The IDA has several subunits of heavy, intermediate, and light chains that are unique from the composition of ODA subunits, indicating different functions for these proteins [31]. Numerous human IDA HC genes have been identified (DNAH1, DNAH2, DNAH3, DNAH6, DNAH7, DNAH10, DNAH12, and DNAH14). DNAH10 and DNAH2 are human orthologs of the Chlamydomonas genes for the IDA HC1 and IDA HC1, respectively. The othologs for the other 6 IDA HC genes have yet to be identified. In addition, IDA intermediate-chain genes and IDA light-chain genes have been identified and additional ortholog analyses are ongoing [29]. Mutations in DNAI1 The ultrastructure and function of the IDAs are diverse and their arrangement along the axoneme is complex. Chlamydomonas exhibits seven different IDA isoforms which are organized with distinct localization Genome-wide linkage analyses have determined that there are likely multiple loci responsible for the mutations that cause the PCD phenotype, which is compatible with the observation that there are at least 250 proteins that make up the ciliary axoneme [32]. Pennarun et al. [33] confirmed the hypothesis that mutations in human genes homologous to Chlamydomonas genes are responsible for PCD by demonstrating that mutations in DNAI1 are present in patients with PCD lacking ciliary ODAs. A mutation in IC78, the Chlamydomonas homolog of DNAI1, results in the inability to assemble the ODA and decreased motility of Chlamydomonas [34]. DNAI1 was the first human gene identified in which mutations cause known ultrastructural defects described in PCD patients. DNAI1, located at chromosome 9p13-21, is expressed in the tracheobronchial tree and testes and is composed of 20 exons [33]. In the initial study, two loss-of-function mutations of DNAI1 (IVS1+2_3insT and 282_283insAATA) were identified in a patient with immotile cilia and absent ODA [33]. Subsequent studies of 226 unrelated PCD patients identified 18 different mutations in DNAI1, ranging from nonsense mutations to splice and missense mutations [35–37] (table 2). A high prevalence (55%) of the mutant alleles had the IVS1+2_3insT mutation, which is known to be a founder mutation. The most common mutant alleles were found to cluster in intron 1 and exons 13, 16 and 17. Approximately 50% of unrelated patients carried at least one mutant allele in these 3 exons. In addition, DNAI1 mutations were present in 11% of 1200 unrelated Caucasian patients tested and in 14% of patients with ODA defects. It is notable that none of the patients PCD and Genetic Mutations Respiration 2007;74:252–263 Ultrastructure of IDAs 257 Table 2. DNAI1 mutations in patients with the classic clinical phenotype for PCD Type of mutation Nucleotide mutation Protein change Exon/intron Nonsense or frameshift 282_283insAATA 463delA 874C>T 1212T>G 1307G>A 1644G>A 1657_1668del 1704G>A 1926_1927insCC G95NfsX24 T155LfsX18 Q292X Y404X W436X W548X T553_F556del W568X I643PfsX48 exon 5 exon 6 exon 10 exon 13 exon 13 exon 17 exon 17 exon 17 exon 19 Splice IVS1+2_3insTa–c IVS7–2A>G IVS10–4_7delGTTT 1490G>Ac IVS19+1G>Ac truncation of protein splice mutation splice mutation R468_K523del A607_K667del intron 1 intron 7 intron 10 exon 16 intron 19 Missense 1222G>A 1543G>Ab 1612G>Ab 1703G>C V408M G515S A538T W568S exon 13 exon 16 exon 17 exon 17 Genetic material from 226 unrelated patients has been analyzed for DNAI1 mutations. Common mutations cluster in intron 1 and exons 13, 16 and 17. 55% of the mutant alleles had the IVS1+2_3insT mutation. Identification of these common mutations has led to the development of a diagnostic genetic test panel (see text for details). Mutations within the DNAI1 gene are always associated with ODA defects [37]. a Founder mutation; leads to truncation of protein. b Found in 2 or more unrelated patients. c RNA tested. with IDA defects had mutations in DNAI1 [37]. Thus, the founder mutation, IVS1+2_3insT, and the exon cluster of mutations, are useful genetic markers for PCD. Mutations in DNAH5 Mutations in the Chlamydomonas HC of the ODA cause a slow swimming Chlamydomonas with ultrastructural abnormalities in the ODA [38]. The human HC ortholog, DNAH5 (chromosome 5p15), was identified as a gene responsible for causing PCD by homozygosity mapping in a large consanguineous Arabic family, where affected individuals lacked ODAs by TEM. The DNAH5 genomic region spans 250 kb and is made up of 79 exons and 1 alternative exon [39]. Sequencing the 80 exons in a total of 134 unrelated patients with PCD for the presence of DNAH5 mutations revealed a large number of mutations [40]. Mutations in DNAH5 were identified as disease-causing in 28% of all unrelated patients, and present in over half (53%) of the unrelated patients with ODA de258 Respiration 2007;74:252–263 fects. None of the individuals with IDA ultrastructural defects had mutations in DNAH5. Therefore, DNAH5 mutations are a major cause of ODA ultrastructural defects. It is noteworthy that approximately 75% of patients had biallelic mutations in DNAH5, whereas approximately 25% had only one mutation, despite complete sequencing of the coding region [40]. We speculate that many of these patients will have small exonic deletions, as seen in other recessive disorders, such as CF [41], and studies to test this hypothesis are underway. There are multiple types of mutations in DNAH5, including nonsense or frameshift mutations, missense mutations, and splicing mutations [40] (table 3). Six mutations (10815delT; 5563_5564insA; 13458_13459insT; IVS76+5G1A; 8528T1C, and 8440_8447delGAACCAAA) were found in more than one unrelated families. Three of the mutations were related to ancestral founders: 10815delT; IVS76+5G1A, and 8528T 1C. It was also noted that the 10815delT mutation was more common in a population of USA patients, as compared to patients from Germany [40]. Morillas/Zariwala/Knowles Table 3. DNAH5 mutations in patients with the classic clinical phenotype for PCD Type of mutation Nucleotide mutation Protein change Exon/intron Nonsense or frameshift 232C>T 252T>G 832delG 1426_1427delTT 1627C>T 1828C>T 3905delT 4360C>T 5130_5131insA 5281C>T 5482C>T 5563_5564insAb 5599_5600insC 6037C>T 7914_7915insA 7915C>T 8440_8447delGAACCAAAb 8029C>T 8167C>T 8314C>T 8404C>T 8910_8911delATinsG 10815delTa, b 13194_13197delCAGA 13426C>T 13458_13459insTb 13486C>T R78X Y84X A278RfsX27 F476SfsX26 Q543X Q610X L1302RfsX19 R1454X R1711TfsX36 R1761X Q1828X I1855NfsX5 I1867PfsX35 R2013X R2639TfsX19 R2639X E2814fsX1 R2677X Q2723X R2772X Q2802X 2970SfsX7 P3606GfsX23 D4398EfsX16 R4476X N4487fsX1 R4496X exon 3 exon 3 exon 7 exon 11 exon 12 exon 14 exon 25 exon 28 exon 32 exon 33 exon 33 exon 34 exon 34 exon 36 exon 48 exon 48 exon 50 exon 49 exon 49 exon 50 exon 50 exon 53 exon 63 exon 76 exon 77 exon 77 exon 77 Splice 1730G>Cc IVS17+2T>C IVS27+1G>A IVS74–1G>Cc IVS75–2A>T IVS76+5G>Aa, b N549_R577delfsX5 splice mutation splice mutation S4304DfsX6 splice mutation splice mutation exon 13 intron 17 intron 27 intron 74 intron 75 intron 76 Missense 4361G>A 5147G>T 6791G>A 7039G>A 7502G>C 8528T>Ca, b 10226G>C 10555G>C 11528C>T 12614G>T R1454Q R1716L S2264N E2347K R2501P F2843S W3409S G3519R S3843L G4205V exon 28 exon 32 exon 41 exon 43 exon 45 exon 51 exon 60 exon 62 exon 67 exon 73 The most common mutations cluster within exons 34, 50, 63, 76 and 77. These 5 exons contain >50% of the DNAH5 mutations seen in 134 unrelated patients that were analyzed. Identification of these common mutations has led to the development of a diagnostic genetic test panel (see text for details) [40]. a Founder mutation. b Found in 2 or more unrelated patients. c RNA tested. PCD and Genetic Mutations Respiration 2007;74:252–263 259 Electron-microscopic photographs of respiratory cilia from three unrelated patients with homozygous mutations of DNAH5 were compared to correlate genotype and phenotype. Mutations causing premature translational termination of DNAH5 (I1855NfsX5 and E2814fsX1) resulted in a complete absence of all ODA in respiratory cilia. In contrast, a splice site mutation (IVS74– 1G1C) did not cause total absence of ODA, but rather an ODA ‘stub’, indicating a partial ODA structural deficiency with loss of function [42]. Testing for Mutations in DNAI1 and DNAH5 The extensive research on the genetic mutations causing PCD has led to the development of a genetic test. Utilizing the information of founder mutations and the clustering of mutations in certain exons, selective mutational analysis of DNAI1and DNAH5 can reduce the labor-intense process of sequencing entire genes searching for mutations. By sequencing only 9 (out of 100) exons and the adjacent splice sequences that harbor the most common mutations in DNAI1 or DNAH5, at least one mutant allele can be detected in approximately 38% of PCD patients [37]. This test becomes diagnostic if biallelic mutations are identified. If only one mutation is identified, the full gene will be sequenced to search for a trans-allelic mutation [37]. Identification of other additional diseasecausing genes will facilitate the diagnosis in PCD, including patients with a nonclassic clinical phenotype, and help to screen other patient populations at risk. Other Genes with Disease-Causing Mutations Other mutations that cause PCD are found in 3 genes: DNAH11, RPGR and OFD1. DNAH11 is located on chromosome 7, along with CFTR, and encodes for an axonemal ODA HC. There was 1 patient with a homozygous nonsense mutation in DNAH11 and a homozygous F508 mutation in CFTR, reflecting uniparental isodisomy, in which both chromosome pairs were inherited from only one parent. This patient had situs inversus and severe respiratory phenotype, but normal ciliary ultrastructure [43]. The iv/iv mouse has a homozygous missense mutation in the mouse ortholog (Dnah11; lrd) that causes the embryonic node cilia to be immotile. Affected mice have random left-right axis asymmetry, but lack respiratory symptoms. It is still unknown whether DNAH11 mutations are a cause of PCD or only cause random left260 Respiration 2007;74:252–263 right asymmetry [44]. There are ongoing studies to further evaluate the possibility that mutations in DNAH11 can cause the full clinical phenotype of PCD. Retinitis pigmentosa (RP) is a rare heterogeneous genetic disorder that affects the photoreceptors on the retinal epithelium and leads to vision loss. RPGR (RP guanosine triphosphate regulator) facilitates the transport of proteins across the connecting cilium of rod and cone photoreceptors and is expressed in bronchial and sinus epithelial cells [45, 46]. In one study, 2 siblings with RP and symptoms of PCD, such as otosinopulmonary disease, had abnormal ciliary function and structure. Both patients had some cilia with normal-appearing structures and other cilia missing IDAs and/or ODAs. A deletion and a missense mutation in RPGR were identified in both patients, while molecular studies in 13 other unrelated families with PCD did not reveal any mutations in RPGR [47]. Oral-facial-digital type 1 (OFD1) syndrome is an Xlinked dominant developmental disorder characterized by craniofacial malformations, digital abnormalities and mental retardation, caused by mutations in OFD1 and is usually lethal in males [48]. OFD1 is localized at the centrosome and basal body of the primary cilia, and is required for the formation of primary cilia. Mice with heterozygous Ofd1 mutations have several phenotypes, including embryonic lethality, the absence of cilia in the embryonic node, and midline defects of the cardiac tube [49]. A large Polish family with a novel X-linked recessive mental retardation syndrome and ciliary dysfunction had 9 affected males with developmental delay and a clinical phenotype compatible with PCD, including chronic respiratory problems and full-term neonatal respiratory distress. PCD was diagnosed by high-speed video microscopy, which revealed dyskinetic cilia with a disorganized beating pattern. Genomic analysis of the affected members revealed a frameshift mutation in the OFD1 gene, and is the only example thus far linking OFD1 mutations with the clinical features of PCD [50]. Candidate Genes That Have Tested Negative for PCD Human orthologs of Chlamydomonas genes known to cause ultrastructural and functional defects are potential disease-causing genes in patients with similar axonemal defects. Multiple candidate genes have been tested in PCD patients and their families, but no other diseasecausing mutations have been identified (table 4). Morillas/Zariwala/Knowles Table 4. Candidate genes without disease-causing mutations for PCD Ciliary ultrastructure Chlamydomonas protein Human gene Number of PCD families tested ODA HC HC HC HC none identified DNAH9 DNAH17 ODA IC IC2 (IC69) DNAI2 16 Bartoloni et al., 2000 [53]; Pennarun et al., 2002 [54] ODA LC LC1 LC6 LC2 LC8 DNAL1 DNAL4 TCTE3 LC8 86 54 36 58 Horvath et al., 2005 [55] Gehrig et al., 2002 [56] Neesen et al., 2002 [57] Bartoloni et al., 2000 [53] IDA HC unknown unknown DNAH3 DNAH7 7 1 IDA IC IC140 IC140 126 IDA LC P28 HP28 61 Gehrig et al., 2002 [56]; Pennarun et al., 2001 [61] IDA, other none DPCD 51 Zariwala et al., 2004 [62] 2 4 References Bartoloni et al., 2001 [51] Blouin et al., 2003 [52] Blouin et al., 2002 [58] Zhang et al., 2002 [59] Knowles et al., 2006 [60] IC = Intermediate chain; LC = light chain [24]. Conclusion PCD is a genetically heterogeneous disorder that causes abnormalities in the structure and function of cilia and leads to recurrent otosinopulmonary infections, bronchiectasis and is associated with situs inversus and heterotaxy. Two genes, DNAI1 and DNAH5, have been identified to have many disease-causing mutations, and some of these occur in multiple patients. Based on these data, a clinical genetic test is available at the University of North Carolina at Chapel Hill (USA) and the University Hospital Freiburg (Germany). This screening test sequences the 9 exons and adjacent sequences that harbor the most common gene mutations of DNAI1 and DNAH5 and can identify the causative mutation on at least one allele in 25% of all PCD tested. Additional, novel diseasecausing genes will likely be discovered by investigating other candidate genes, and by genome-wide linkage- References PCD and Genetic Mutations based studies in families with a large number of affected individuals and/or in consanguineous families. As more disease-causing gene mutations are identified, they will be added to genetic screening panels to further identify patients with PCD. In addition, investigations to link genetic mutations to clinical phenotypes, such as in patients with congenital heart disease and male infertility, will aid in identifying new associations between genetic mutations and clinical phenotypes. Acknowledgments We thank Peader G. Noone, MD for critically reading the manuscript. We also gratefully acknowledge the UNC clinicians, researchers and collaborators for providing care to PCD patients and continually searching for more information, especially Dr. Margaret Leigh. 1 Knowles MR, Boucher RC: Mucus clearance as a primary innate defense mechanism for mammalian airways. J Clin Invest 2002;109: 571–577. 2 Afzelius BA: A human syndrome caused by immotile cilia. Science 1976;193:317–319. 3 Afzelius BA, Mossberg B, Bergstrom SE: Immotile cilia syndrome (primary ciliary dyskinesia), including Kartagener syndrome; in The Metabolic and Molecular Basis of Inherited Disease. New York, McGraw-Hill, 2001, pp 4817–4827. Respiration 2007;74:252–263 261 4 Noone PG, Bennett WD, Regnis JA, Zeman KL, Carson JL, King M, et al: Effect of aerosolized uridine-5-triphosphate on airway clearance with cough in patients with primary ciliary dyskinesia. Am J Respir Crit Care Med 1999;160:144–149. 5 Noone PG, Leigh MW, Sannuti A, Minnix SL, Carson JL, Hazucha, M, et al: Primary ciliary dyskinesia: diagnostic and phenotypic features. Am J Respir Crit Care Med 2004; 169:459–467. 6 van’s Gravesande KS, Omran H: Primary ciliary dyskinesia: clinical presentation, diagnosis and genetics. Ann Med 2005; 37: 439– 449. 7 Kennedy MP, Noone PG, Carson J, Molina PL, Ghio A, Zariwala MA, et al: Calcium stone lithoptysis in primary ciliary dyskinesia. Respir Med 2007;101:76–83. 8 Halbert SA, Patton DL, Zarutskie PW, Soules MR: Function and structure of cilia in the fallopian tube of an infertile woman with Kartagener’s syndrome. Hum Reprod 1997; 12:55–58. 9 Nonaka S, Tanaka Y, Okada Y, Takeda S, Harada A, Kanai Y, et al: Randomization of leftright asymmetry due to loss of nodal cilia generating leftward flow of extraembryonic fluid in mice lacking KIF3B motor protein. Cell 1998;95:829–837. 10 Kartagener M, Stucki P: Bronchiectasis with situs inversus. Arch Pediatr 1962; 79: 193– 207. 11 Kennedy MP, Omran H, Leigh MW, Dell S, Morgan L, Molina PL, et al: Congenital heart disease and other heterotaxic defects in a large cohort of patients with primary ciliary dyskinesia. Circulation, in press. 12 Leigh MW: Primary ciliary dyskinesia. Semin Respir Crit Care Med 2003; 24: 653– 662. 13 Coren ME, Meeks M, Morrison I, Buchdahl RM, Bush A: Primary ciliary dyskinesia: age at diagnosis and symptom history. Acta Paediatr 2002;91:667–669. 14 Ferkol T, Leigh MW: Primary ciliary dyskinesia and newborn respiratory distress. Semin Perinatol 2006;30:335–340. 15 Bush A, Cole P, Hariri M, Mackay I, Phillips G, O’Callaghan C, et al: Primary ciliary dyskinesia: diagnosis and standards of care. Eur Respir J 1998;12:982–988. 16 Carda C, Armengot M, Escribano A, Peydro A: Ultrastructural patterns of primary ciliar dyskinesia syndrome. Ultrastruct Pathol 2005;29:3–8. 17 Chilvers MA, Rutman A, O’Callaghan C: Ciliary beat pattern is associated with specific ultrastructural defects in primary ciliary dyskinesia. J Allergy Clin Immunol 2003;112:518–524. 18 Jorissen M, Willems T, Van der SB Verbeken E, De Boeck K: Ultrastructural expression of primary ciliary dyskinesia after ciliogenesis in culture. Acta Otorhinolaryngol Belg 2000; 54:343–356. 262 19 Stannard W, Rutman A, Wallis C, O’Callaghan C: Central microtubular agenesis causing primary ciliary dyskinesia. Am J Respir Crit Care Med 2004;169:634–637. 20 Escudier E, Couprie M, Duriez B, RoudotThoraval F, Millepied MC, Pruliere-Escabasse V, et al: Computer-assisted analysis helps detect inner dynein arm abnormalities. Am J Respir Crit Care Med 2002; 166: 1257–1262. 21 Carlen B, Stenram U: Primary ciliary dyskinesia: a review. Ultrastruct Pathol 2005; 29: 217–220. 22 Carson JL, Collier AM, Hu S-CS: Acquired ciliary defects in nasal epithelium of children with acute viral upper respiratory infections. N Engl J Med 1985;312:463–468. 23 Lundberg JO, Weitzberg E, Nordvall SL, Kuylenstierna R, Lundberg JM, Alving K: Primarily nasal origin of exhaled nitric oxide and absence in Kartagener’s syndrome. Eur Respir J 1994;7:1501–1504. 24 Zariwala MA, Knowles MR, Omran H: Genetic defects in ciliary structure and function. Annu Rev Physiol 2007;69:22.1–22.28. 25 Satir P: Tour of organelles through the electron microscope: a reprinting of Keith R. Porter’s classic Harvey Lecture with a new introduction. Anat Rec A Discov Mol Cell Evol Biol 2005; 287:1184–1185. 26 Satir P, Christensen ST: Overview of structure and function of mammalian cilia. Annu Rev Physiol 2007;69:14.1–14.24. 27 Brueckner M: Cilia propel the embryo in the right direction. Am J Med Genet 2001; 101: 339–344. 28 Pazour GJ, Agrin N, Leszyk J, Whitman GB: Proteomic analysis of a eukaryotic cilium. J Cell Biol 2005; 170:103–113. 29 Pazour GJ, Agrin N, Walker BL, Witman GB: Identification of predicted human outer dynein arm genes: candidates for primary ciliary dyskinesia genes. J Med Genet 2006; 43: 62–73. 30 Fliegauf M, Olbrich H, Horvath J, Wildhaber JH, Zariwala MA, Kennedy MP, et al: Mislocalization of DNAH5 and DNAH9 in respiratory cells from patients with primary ciliary dyskinesia. Am J Respir Crit Care Med 2005;171:1343–1349. 31 Porter ME, Sale WS: The 9 + 2 axoneme anchors multiple inner arm dyneins and a network of kinases and phosphatases that control motility. J Cell Biol 2000; 151:F37–F42. 32 Blouin JL, Meeks M, Radhakrishna U, Sainsbury A, Gehring C, Sail GD, et al: Primary ciliary dyskinesia: a genome-wide linkage analysis reveals extensive locus heterogeneity. Eur J Hum Genet 2000;8:109–118. 33 Pennarun G, Escudier E, Chapelin C, Bridoux AM, Cacheux V, Roger G, et al: Lossof-function mutations in a human gene related to Chlamydomonas reinhardtii dynein IC78 result in primary ciliary dyskinesia. Am J Hum Genet 1999;65:1508–1519. Respiration 2007;74:252–263 34 Mitchell DR, Kang Y: Identification of oda6 as a Chlamydomonas dynein mutant by rescue with the wild-type gene. J Cell Biol 1991; 113:835–842. 35 Guichard C, Harricane MC, Lafitte JJ, Godard P, Zaegel M, Tack V, et al: Axonemal dynein intermediate-chain gene (DNAI1) mutations result in situs inversus and primary ciliary dyskinesia (Kartagener syndrome). Am J Hum Genet 2001;68:1030–1035. 36 Zariwala M, Noone PG, Sannuti A, Minnix S, Zhou Z, Leigh MW, et al: Germline mutations in an intermediate chain dynein cause primary ciliary dyskinesia. Am J Respir Cell Mol Biol 2001;25:577–583. 37 Zariwala MA, Leigh MW, Ceppa F, Kennedy MP, Noone PG, Carson JL, et al: Mutations of DNAI1 in primary ciliary dyskinesia: evidence of founder effect in a common mutation. Am J Respir Crit Care Med 2006; 174: 858–866. 38 Rupp G, O’Toole E, Gardner LC, Mitchell BF, Porter ME: The sup-pf-2 mutations of Chlamydomonas alter the activity of the outer dynein arms by modification of the gamma-dynein heavy chain. J Cell Biol 1996;135: 1853–1865. 39 Olbrich H, Haffner K, Kispert A, Volkel A, Volz A, Sasmaz G, et al: Mutations in DNAH5 cause primary ciliary dyskinesia and randomization of left-right asymmetry. Nat Genet 2002;30:143–144. 40 Hornef N, Olbrich H, Horvath J, Zariwala MA, Fliegauf M, Loges NT, et al: DNAH5 mutations are a common cause of primary ciliary dyskinesia with outer dynein arm defects. Am J Respir Crit Care Med 2006;174:120–126. 41 Ferec C, Casals T, Chuzhanova N, Macek M Jr, Bienvenu T, Holubova A, et al: Gross genomic rearrangements involving deletions in the CFTR gene: characterization of six new events from a large cohort of hitherto unidentified cystic fibrosis chromosomes and meta-analysis of the underlying mechanisms. Eur J Hum Genet 2006;14:567–576. 42 Kispert A, Petry M, Olbrich H, Volz A, Ketelsen UP, Horvath J, et al: Genotype-phenotype correlations in PCD patients carrying DNAH5 mutations. Thorax 2003; 58: 552– 554. 43 Bartoloni L, Blouin JL, Pan Y, Gehrig C, Maiti AK, Scamuffa N, et al: Mutations in the DNAH11(axonemal heavy chain dynein type 11) gene cause one form of situs inversus totalis and most likely primary ciliary dyskinesia. Proc Natl Acad Sci USA 2002; 99: 10282–10286. 44 Supp DM, Witte DP, Potter SS, Brueckner M: Mutation of an axonemal dynein affects leftright asymmetry in inversus viscerum mice. Nature 1997;389:963–966. 45 Hong DH, Pawlyk BS, Shang J, Sandberg MA, Berson EL, Li T: A retinitis pigmentosa GTPase regulator (RPGR)-deficient mouse model for X-linked retinitis pigmentosa (RP3). Proc Natl Acad Sci USA 2000; 97: 3649–3654. Morillas/Zariwala/Knowles 46 Iannaccone A, Breuer DK, Wang XF, Kuo SF, Normando EM, Filippova E, et al: Clinical and immunohistochemical evidence for an X-linked retinitis pigmentosa syndrome with recurrent infections and hearing loss in association with an RPGR mutation. J Med Genet 2003;40:e118. 47 Moore A, Escudier E, Roger G, Tamalet A, Pelosse B, Marlin S, et al: RPGR is mutated in patients with a complex X-linked phenotype combining primary ciliary dyskinesia and retinitis pigmentosa. J Med Genet 2006; 43:326–333. 48 Ferrante MI, Giorgio G, Feather SA, Bulfone A, Wright V, Ghiani M, et al: Identification of the gene for oral-facial-digital type I syndrome. Am J Hum Genet 2001;68:569–576. 49 Ferrante MI, Zullo A, Barra A, Bimonte S, Messaddeq N, Studer M, et al: Oral-facialdigital type I protein is required for primary cilia formation and left-right axis specification. Nat Genet 2006;38:112–117. 50 Budny B, Chen W, Omran H, Fliegauf M, Tzschach A, Wisniewska M, Jensen LR, et al: A novel X-linked recessive mental retardation syndrome comprising macrocephaly and ciliary dysfunction is allelic to oral-facial-digital type I syndrome. Hum Genet 2006;120:171–178. 51 Bartoloni L, Blouin JL, Maiti AK, Sainsbury A, Rossier C, Gerhig C, et al: Axonemal beta heavy chain dynein DNAH9: cDNA sequence, genomic structure, and investigation of its role in primary ciliary dyskinesia. Genomics 2001;72:21–33. PCD and Genetic Mutations 52 Blouin JL, Albrecht C, Gehrig C, DuriauxSail G, Strauss JF 3rd, Bartoloni L, et al: Primary ciliary dyskinesia/Kartagener syndrome: searching for genes in a highly heterogeneous disorder (abstract). Am J Hum Genet 2003;73(suppl 5):No 2440. 53 Bartoloni L, Mitchison H, Pazour GJ, Maiti AK, Meeks M, Chung E, et al: No deleterious mutations were found in three genes (HFH4, LC8, IC2) on human chromosome 17q in patients with primary ciliary dyskinesia (abstract). Eur J Hum Genet 2000;8:P484. 54 Pennarun G, Bridoux AM, Escudier E, Dastot-Le Moal F, Cacheux V, Amselem S, et al: Isolation and expression of the human hPF20 gene orthologous to Chlamydomonas PF20: evaluation as a candidate for axonemal defects of respiratory cilia and sperm flagella. Am J Respir Cell Mol Biol 2002;26:362–370. 55 Horvath J, Fliegauf M, Olbrich H, Kispert A, King SM, Mitchison H, et al: Identification and analysis of axonemal dynein light chain 1 in primary ciliary dyskinesia patients. Am J Respir Cell Mol Biol 2005; 33:41–47. 56 Gehrig C, Albrecht C, Duriaus Sail G, Rossier C, Scamuffa N, DeLozier-Blancet C, et al: Primary ciliary dyskinesia: mutation analysis in dynein light chain genes mapping to chromosome 1 (HP28) and 22 (DNAL4) (abstract). European Human Genetics Conference, Strasbourg, 2002, P0305. 57 Neesen J, Drenckhahn JD, Tiede S, Burfeind P, Grzmil M, Konietzko J, et al: Identification of the human ortholog of the t-complex-encoded protein TCTE3 and evaluation as a candidate gene for primary ciliary dyskinesia. Cytogenet Genome Res 2002;98:38–44. 58 Blouin JL, Gehrig C, Armengot M, Rutishauser M, Jorissen M, Jeganathan D, et al: DNAH3: characterization of the sequence and mutation search in patients with primary ciliary dyskinesia (abstract). European Human Genetics Conference, Strasbourg, 2002, P0304. 59 Zhang YJ, O’Neal WK, Randell SH, Blackburn K, Moyer MB, Boucher R, et al: Identification of dynein heavy chain 7 as an inner arm component of human cilia that is synthesized but not assembled in a case of primary ciliary dyskinesia. J Biol Chem 2002; 277:17906–17915. 60 Knowles MR, Leigh MW, Kennedy MP, Noone PG, Lyons SM, Escudier E, et al: An IDA intermediate chain dynein as a candidate gene for primary ciliary dyskinesia (PCD) (abstract 1815B). American Society of Human Genetics Conference, New Orleans, 2006. 61 Pennarun G, Bridoux AM, Escudier E, Amselem S, Duriez B: The human HP28 and HFH4 genes: evaluation as candidate genes for primary ciliary dyskinesia (abstract). Am J Respir Crit Care Med 2001;163:A538. 62 Zariwala M, O’Neal WK, Noone PG, Leigh MW, Knowles MR, Ostrowski LE: Investigation of the possible role of a novel gene, DPCD, in primary ciliary dyskinesia. Am J Respir Cell Mol Biol 2004;30:428–434. Respiration 2007;74:252–263 263