Athletic Profile Freeport High School Name Date Sport Address
advertisement

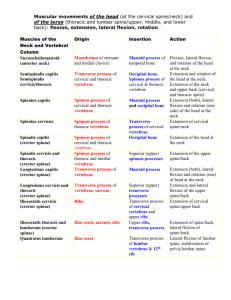
Athletic Profile Freeport High School Name Date Sport Address Birthdate Family Physician Height Weight Blood Pressure Heart Rate Vertical Jump 40-yard Dash Notes: Telephone Athletic Pre-Participation Physical Evaluation Form Part A: Health History Questionnaire (to be completed by parent and student) Directions: Please answer the following questions about the student’s medical history. Explain all “yes” responses. Please respond to all questions. (Circle letter and responses) 1. Have you had or do you currently have: A. a sports physical within the past 365 days? B. an injury or illness since your last exam? C. a chronic or ongoing illness (such as diabetes or asthma)? D. any prescribed or over-the counter medications that you take on a regular basis? (list below) Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know E. surgery, hospitalization, or any emergency room visit(s)? Y / N / Don’t Know F. any allergies to medications? Y / N / Don’t Know G. any allergies to bee sting, pollen, latex, or foods? Y / N / Don’t Know 1. Any type of reaction: rash hives other skin conditions Y / N / Don’t Know (circle all that apply) 2. Take any medication / Epipen taken for allergy symptoms? Y / N / Don’t Know H. Any anemia or blood disorders? Y / N / Don’t Know 2. Have you had or do you currently have any of the following head related conditions since your last physical? A. Concussions requiring a physician’s evaluation? Y / N / Don’t Know How often and when? B. Memory loss or been knocked-out? C. A seizure? D. Frequent or severe headaches? Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know 3. Have you had or do you currently have any of the following heart related conditions since your last physical? A. Chest pains? Y / N / Don’t Know B. Heart murmur? Y / N / Don’t Know C. High blood pressure or elevated cholesterol levels? Y / N / Don’t Know D. Restricted from sports because of a heart problem? Y / N / Don’t Know E. Any family members or relatives: 1. die of a heart problem before age 35? Y / N / Don’t Know 2. die of a heart problem before age 50? Y / N / Don’t Know 3. die with no known reason? Y / N / Don’t Know 4. die while exercising? During or after? (circle one) Y / N / Don’t Know 5. with Marfan’s Syndrome? Y / N / Don’t Know 4. Have you had or do you have any of the following eye, ear, nose, mouth, or throat conditions since your last physical? A. Vision problems? Y / N / Don’t Know Wear contacts, eyeglasses, or protective eye wear? (circle one) B. Hearing loss or problems? Y / N / Don’t Know Wearing hearing aids or implants? Y / N / Don’t Know C. Nasal fractures or frequent nose bleeds? Y / N / Don’t Know D. Wear braces, retainers, or protective mouth gear? Y / N / Don’t Know E. Frequent strep or any other conditions of the throat? Y / N / Don’t Know 5. Have you had or do you have any of the following neuromuscular orthopedic conditions since your last physical? A. A burner, stinger, or pinched nerve? Y / N / Don’t Know B. A sprain or strain? Y / N / Don’t Know D. Pain or swelling in any muscle, tendon, bone, or joint? Y / N / Don’t Know E. A dislocated joint? Y / N / Don’t Know F. Upper or lower back pain? Y / N / Don’t Know G. Do you wear any protective braces from a prior injury? Y / N / Don’t Know 6. Have you had or do you have any of the following general or exercise related conditions since your last physical? A. Difficulty breathing? During exercise? (circle one) Y / N / Don’t Know 1. After running one mile Y / N / Don’t Know 2. Coughing, wheezing, or shortness of breath in weather changes? Y / N / Don’t Know 3. Exercise induced asthma Y / N / Don’t Know Controlled with medications? Y / N / Don’t Know Experience dizziness, passing-out, or fainting Y / N / Don’t Know B. Viral infections (e.g. Hepatitis or mono) C. Become tired more quickly than your friends D. Any of the following skin conditions: 1. Acne, contact dermatitis, ringworm, warts, herpes? 2. Sun sensitivity? E. Weight gain / loss greater than 10 pounds? F. Ever had feelings of depression? G. Heat-related problems (dehydration, dizziness, fatigue, or headache)? Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know Y / N / Don’t Know 1. Heat exhaustion (cool, clammy, or damp skin)? 2. Heat stroke (hot, red, dry skin)? Y / N / Don’t Know Y / N / Don’t Know 7. Check one: This is the FIRST TIME this health questionnaire has been completed for the upcoming school year. There is NO CHANGE to the previous health questionnaire filled out this school year. There are CHANGES to the previous health questionnaire filled out this school year. 8. FEMALES ONLY: Age of onset of menstruation: Date of last menstruation: Most number of days between menstruation cycle(s): Explain all Yes answers here (include relevant dates) I understand that although a physical exam is still required for the upcoming sports season, it is my responsibility to keep my medical history questionnaire updated through the school of participation. We certify that the information provided herein is accurate to the best of our knowledge as of the date of these signatures. Parent / Guardian Signature: Date: Student Signature: Date: Part B: Musculoskeletal Exam (to be completed by examining therapist or trainer) ROM STRENGTH Normal / Abnormal (circle one) ROM STRENGTH Normal / Abnormal (circle one) SPINE - CERVICAL LOWER EXTREMITY N A Flexion / Extension N A Hip N A Rotation right / left N A Hip Flexors / Gluteals N A Lateral flexion right / left N A Abduction / Adduction – Groin / TT N A SPINE – THORACIC N A Interior / exterior rotation SPINE – LUMBAR N A Knee N A Flexion / Extension N A Patellar Tendon N A Rotation right / left N A Tibial Tuberosity N A Lateral flexion right / left N A MCL / LCL N A Abdominal / Obliques (STR) N A ACL / PCL UPPER EXTREMITY N A Cartilage Testing N A Shoulder N A Quads / Hamstrings N A Forward flexion / extension N A Gast / Soleus Complex N A Abduction / adduction N A Patella N A Internal / external rotation N A Crepitus N A Horizontal abduction / adduction N A Tracking N A A C Joint / Clavicle N A Ankle N A Stability Testing N A Plantar / Dorsiflexion N A Biceps flexion / extension N A Inversion / Eversion N A Elbow N A Subtalar Joint N A Supination / pronation N A Ligament Testing N A Wrist / hand N A Feet / Toes GENERAL FLEXIBILITY N A Hamstrings N A Quadriceps N A Lumbar Spine N A Achilles Part C: Special Testing for Above Body Parts (to be completed by examining therapist or trainer) Cervical Spine Vertebral Artery Test Foraminal Compression Test (Spurling) Foraminal Distraction Test Valsalva’s Maneuver Swallowing Test Tinel’s Sign Notes N/A N/A N/A N/A N/A N/A Thoracic Spine Kernig / Brudzinski Signs Lateral Rib Compression Test Anterior / Posterior Rib Compression Test Inspiration / Expiration Breathing Test Lumbar Spine Valsalva’s Maneuver Stoop Test 90-90 Straight Leg Raise Test Bowstring Test (Cram Test) Unilateral Straight Leg Raise Test Bilateral Straight Leg Raise Test Well Straight Leg Raise Test Slump Test Thomas Test Spring Test Notes N/A N/A N/A N/A Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A Shoulder Empty Can (Supraspinatus) Test Yergason Test Speed’s Test Drop Arm Test Apley’s Scratch Test Cross-Over Impingement Test Sternoclavicular (SC) Joint Stress Test Acromioclavicular (AC) Joint Distraction Test Apprehension Test (Anterior) Apprehension Test (Posterior) Brachial Plexus Stretch Test Shoulder Abduction Test Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A Elbow Resistive Tennis Elbow Test (Cozen’s Test) Resistive Tennis Elbow Test Passive Tennis Elbow Test Golfer’s Elbow Test Hyperextension Test Elbow Flexion Test Varus Stress Test Valgus Stress Test Tinel’s Sign Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A Wrist and Hand Compression Test Long Finger Flexion Test Finkelstein Test Phalen Test Tinel’s Sign Bunnel Littler Test Murphy’s Sign Valgus Stress Test Varus Stress Test Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A Knee Patellar Apprehension Test Quadriceps or Q-Angle Test Medial-Lateral Grind Test Bounce Home Test Patellar Grind Test (Clarke’s Sign) Hughston’s Plica Test Posterior Sag Test (Gravity Drawer Test) Reverse Pivot Shift (Jakob Test) Anterior Lachman’s Test Anterior Drawer Test Slocum Test with Internal Tibial Rotation Slocum Test with External Tibial Rotation Pivot Shift Test Posterior Drawer Test Posterior Lachman’s Test 27 External Rotation Recurvatum Test Valgus Stress Test Varus Stress Test McMurray Test Apley Compression Test Rectus Femoris Contracture Test Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A Ankle and Foot Anterior Drawer Test Talar Tilt Test (Inversion) Talar Tilt Test (Eversion) Thompson Test Tap or Percussion Test Interdigital Neuroma Test Compression Test Long Bone Compression Test Swing Test Tinel’s Sign Notes N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A