Ortho Wrist
advertisement

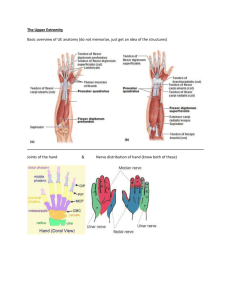
1 ORTHOPEDIC TESTS-WRIST, HAND ELBOW (NPLEX) ROM Wrist Elbow Extension Flexion 80 Radial Deviation Ulnar Deviation 30 70 Flexion 20 Fingers Extension Flexion Abduction Adduction Extension 135 + Pronation Supination 0-5 90 90 Thumb 30-45 90 Abduction Adduction 70 0 20 0 1) Phalen's Sign Procedure: The wrists are held together in complete flexion for 30-60 seconds. The sign is positive if there is discomfort, numbness, tingling paresthesia. Significance: Median nerve compression as in Carpal Tunnel Syndrome. 2) Tests for Ligamentous Stability A) Flexor Digitorum Superficialis Test Procedure: Hold the patient's fingers in extension - except for finger being tested. Instruct patient to flex finger in question at the proximal interphalangeal joint. If he can not, the tendon is either cut or absent. B) Flexor Digitorum Profundus Test Procedure: Isolate the distal interphalangeal joint by stabilizing the metacarpophalangeal and interphalangeal joints in extension. Ask the patient to flex his finger at the distal interphalangeal joint. If he can not - then tendon may be cut or the muscle denervated. C) Assess the Stability of the Medial and Lateral Collateral Ligaments of the Elbow Procedure: The examiner cups the posterior aspect of the patients elbow in one hand and holds the wrist with the other hand. Instruct the patient to flex his elbow a few degrees as you force his arm laterally, producing a valgus stress on the joint's medial side. Note any gaping medially. Reverse the direction and push the forearm medially, producing a varus stress to the elbow's lateral side. Inspect for gaping laterally. 3) Tinel's Sign Procedure: Tap the area of the nerve in the groove between the olecranon and the medial epicondyle. If positive there will be a tingling sensation down the forearm to the ulnar distribution in the hand. Significance: Neuroma This test can be done along the course of an injured nerve to differentiate between the complete and partial peripheral nerve interruption. 4) Tennis Elbow Test/Cozen Test Procedure: Stabilize the patient's forearm and instruct him to make a fist and extend his wrist. Apply pressure with your hand to the Dorsum of his fist to attempt to force his wrist into flexion. If positive, the patient will experience pain at the lateral epicondyle. Ortho Tests-Arm 2 5) Bunnel-Littler Test Procedure: To test the tightness of the intrinsic muscles, hold the metacarpophalangeal joint in a few degrees of flexion. Try to move the proximal interphalangeal joint into the flexion. If the proximal interphalangeal joint can be flexed, the intrinsics are not tight and aren't limiting flexion. If it can't be flexed = tight intrinsics or joint contractures. To distinguish between the intrinsic muscle tightness and joint capsule contractures, let the involved finger flex a few degrees at the metacarpophalangeal joint and move the proximal interphalangeal joint into flexion. If the joint is now capable of full flexion = tight intrinsic. If the joint won't flex completely = proximal interphalangeal joint capsule contractures. Significance: To evaluate the tightness of the intrinsic hand muscles and to determine whether flexion limitations in the proximal interphalangeal joint is due to tightness of the intrinsic or to joint capsule contractures. 6) Retinacular Test Procedure: Hold the proximal interphalangeal joint in neutral position and try to move the distal interphalangeal joint into flexion. If the joint does not flex = joint capsule contractures or due to retinacular tightness. To distinguish between these two, flex the proximal interphalangeal joint slightly to relax retinaculum. IF the distal interphalangeal joint flexes = the retinacular ligaments are tight. If the joint doesn't flex, the distal interphalangeal joint capsule is probably contracted. 7) Allen Test Procedure: Have patient open and close his fist several times and then squeeze his fist tightly so that the venous blood is forced out of the palm. Place your thumb over the radial artery and your index and middle fingers over the ulnar artery. Press them and occlude them. With the vessels occluded, have the patient open his fist. The hand should be pale. Release one of the arteries while maintaining pressure on the other one. The hand should flush immediately. If is does not = occlusion. The other artery should be tested similarly. Significance: To test radial and ulnar arteries supplying the hand. Ortho Tests-Arm