Enhanced Activity of the Purine Nucleotide Cycle of the Exercising
advertisement

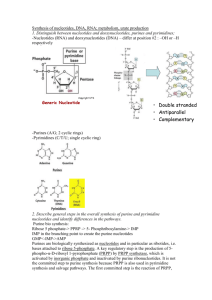
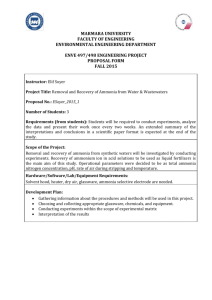
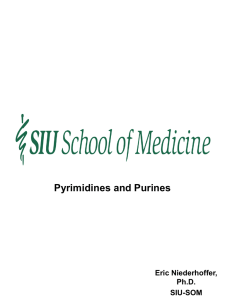
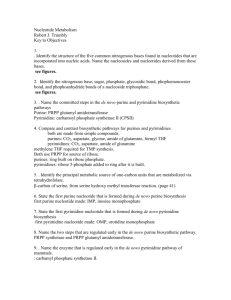
0021-972X/01/$03.00/0 The Journal of Clinical Endocrinology & Metabolism Copyright © 2001 by The Endocrine Society Vol. 86, No. 5 Printed in U.S.A. Enhanced Activity of the Purine Nucleotide Cycle of the Exercising Muscle in Patients with Hyperthyroidism HIROKO FUKUI, SHIN-ICHI TANIGUCHI, YOSHIHIKO UETA, AKIO YOSHIDA, AKIRA OHTAHARA, ICHIRO HISATOME, AND CHIAKI SHIGEMASA First Department of Internal Medicine, Tottori University Faculty of Medicine, Yonago 683, Japan ABSTRACT Myopathy frequently develops in patients with hyperthyroidism, but its precise mechanism is not clearly understood. In this study we focused on the purine nucleotide cycle, which contributes to ATP balance in skeletal muscles. To investigate purine metabolism in muscles, we measured metabolites related to the purine nucleotide cycle using the semiischemic forearm test. We examined the following four groups: patients with untreated thyrotoxic Graves’ disease (untreated group), patients with Graves’ disease treated with methimazole (treated group), patients in remission (remission group), and healthy volunteers (control group). To trace the glycolytic process, we measured glycolytic metabolites (lactate and pyruvate) as well as purine metabolites (ammonia and hypoxanthine). In the untreated group, the levels of lactate, pyruvate, and ammonia released were remarkably higher than those in the control I T IS WELL known that myopathy often develops as a complication of hyperthyroidism and is present in 33– 60% of thyrotoxic cases. Even though no muscular symptom is observed, muscle hypotonia or fatigue can appear during exercise (1, 2). Muscular symptoms will subside rapidly in parallel with the recovery of thyroid function. According to a study that involved 240 Japanese patients with thyroid myopathy, major symptoms, such as muscle hypotonia or amyotrophy, were related to the prevalence period and the age of the patients at the time of thyrotoxicosis (3). Under thyrotoxic conditions, ATP is promptly depleted, and myopathy easily develops, as the im glycogen content decreases due to the suppression of glycogenesis and glycogenolysis. This appears to be due to the same factors that cause glycogen storage disease, which is accompanied by a low capacity to perform exercise. During vigorous exercise, glycogen is rapidly consumed, and ATP consumption by the skeletal muscles increases more than the ATP supply. At that time, the purine nucleotide cycle tries to catch up with the insufficient ATP supply (Fig. 1) (4). The purine nucleotide cycle consists of three intermediates, namely, AMP, inosine monophosphate (IMP), and adenylosuccinic acid. Three enzymes, adenylate kinase, 5⬘-nucleotidase, and AMP deaminase, regulate the purine nucleotide cycle. The purine nucleotide cycle plays a critical role in removing AMP from the exercising muscles to keep a high Received October 23, 2000. Revision received January 18, 2001. Accepted February 8, 2001. Address all correspondence and requests for reprints to; Shin-ichi Taniguchi, M.D., Ph.D., First Department of Internal Medicine, Tottori University Faculty of Medicine, Yonago 683, Japan. E-mail: stani@ grape.med.tottori-u.ac.jp. group. Hypoxanthine release also increased in the untreated group, but the difference among the patient groups was not statistically significant. The accelerated purine catabolism did not improve after 3 months of treatment with methimazole, but it was completely normalized in the remission group. This indicated that long-term maintenance of thyroid function was necessary for purine catabolism to recover. We presume that an unbalanced ATP supply or conversion of muscle fiber type may account for the acceleration of the purine nucleotide cycle under thyrotoxicosis. Such acceleration of the purine nucleotide cycle is thought to be in part a protective mechanism against a rapid collapse of the ATP energy balance in exercising muscles of patients with hyperthyroidism. (J Clin Endocrinol Metab 86: 2205–2210, 2001) adenylic acid energy level (ATP⫹0.5ADP/ATP⫹ADP⫹AMP), which reflects ATP balance within the muscle cell. Skeletal muscles have a high degree of AMP deaminase activity and a low degree of 5⬘-nucleotidase activity compared with the myocardium (5). Therefore, skeletal muscles convert AMP to IMP, which is a membrane-impermeable nucleotide, keeping IMP within the myocyte and promptly produce AMP through adenylosuccinate via activation of adenylosuccinate synthetase and adenylosuccinate lyase. The purine nucleotide cycle is known to work only after vigorous long-term exercises. When the im ATP content decreases after hard exercise, the AMP degradation (IMP3inosine3hypoxanthine) progresses to maintain a high constant intracellular energy level, and simultaneously ammonia production increases due to AMP deamination (AMP3 IMP⫹NH4). Accordingly, increases in hypoxanthine and ammonia, which are membrane-permeable metabolites, are supposed to be important parameters of purine catabolic reactions. In glycogen storage disease types III, V, and VII, which are due to a disorder of glycogenolysis, AMP deamination is greatly accelerated because of an insufficient ATP supply from glycogenolysis. As a consequence, large amounts of ammonia and hypoxanthine are released into the blood. In addition to glycogen storage diseases, an enhanced degradation of purine nucleotides is often observed in muscles of patients with hypoparathyroidism or myopathy associated with electrolyte disorders such as hypokalemia and hypophosphatemia (6), so enhanced production of purine metabolites could be associated with the impairment of ATP balance within skeletal muscles. We presume that myopathy in hyperthyroidism may also belong to the group of skeletal muscle catabolic disorders 2205 2206 FUKUI ET AL. FIG. 1. The glycogenolysis/glycolysis and purine catabolism pathway in muscle. 1) Adenylate kinase; 2) AMP deaminase; 3) 5⬘-nucleotidase. caused by an impairment of ATP balance. Based on this assumption, we used a semiischemic forearm exercise test to investigate purine nucleotide cycle activity in the skeletal muscles of patients with hyperthyroidism. Subjects and Methods Semiischemic forearm exercise test As hard exercise is not an appropriate way to evaluate the purine nucleotide cycle activity in patients with myogenic symptoms, we employed the semiischemic forearm exercise test. This test induces a rapid decrease in the ATP content of the muscle and stimulates the purine nucleotide cycle. After resting in the supine position for 30 min, a manschette tourniquet was placed around the patient’s forearm, and a pressure equivalent to the mean of the systolic/diastolic pressure was applied. The patient was then asked to repeat a handgrip exercise at 70% of maximum using a dynamometers at a rate of one handgrip per s for 2 min. Blood was sampled from the forearm vein to measure lactate, pyruvate, ammonia, and hypoxanthine, at rest, immediately after exercise, and 10 min thereafter. The samples were kept at ⫺80 C, except for those used to determine ammonia, which were collected in a frozen heparinized test tube and measured within a few hours. Serum lactate, pyruvate, and ammonia were analyzed using an enzymatic method (COBAS-FARA, Roche, Basel, Switzerland). The procedure used to measure hypoxanthine was similar to those described previously (7, 8). In brief, samples were centrifuged at 2600 ⫻ g at 4 C for 15 min. Methanol (1.6 mL) was added to 0.4-mL plasma samples, which were then centrifuged at 29,000 ⫻ g for 5 min. Supernatants (1.0 mL) were decanted at 40 C, and 0.2 mL 0.3% ammonia was added. The plasma hypoxanthine concentration was then measured by high pressure liquid chromatography (model 510, Waters Corp., Milford, MA). To determine the maximum increase (⌬) in each metabolite during exercise, ⌬lactate, ⌬pyruvate, and ⌬ammonia (immediately after exercise ⫺ at rest) and ⌬hypoxanthine (10 min after ⫺ at rest) were calculated. Although it is reasonable to measure the difference between arterial and venous (A-V) concentrations of the metabolites to examine muscle metabolism, we measured the changes in the metabolites in the venous samples instead. In a preliminary study we compared the changes in A-V concentration difference of ⌬hypoxanthine, ⌬ammonia and ⌬lactate in the semiischemic forearm with the changes in venous blood samples taken from the antecubital vein (n ⫽ 5). As shown in Fig. 2, there were no significant differences between the increases in the A-V difference in ⌬hypoxanthine, ⌬ammonia, or ⌬lactate and their increases in the antecubital vein. This means the increases in metabolites in blood JCE & M • 2001 Vol. 86 • No. 5 FIG. 2. Comparison of the changes in A-V concentration difference in hypoxanthine, ammonia, and lactate with their changes in the venous sample of control subjects (n ⫽ 5). V, Concentration in the venous sample; V-A, A-V concentration difference. Note that there were no significant differences between them. from the antecubital vein after exercise were almost equivalent to those in the A-V concentration difference in the metabolites after exercise, indicating that the changes in the level of metabolites in the venous sample reflected the metabolism of the skeletal muscles instead of the A-V concentration difference of the metabolites. Subjects Subjects were divided into four groups as follows: the untreated group (untreated patients with Graves’ disease), the methimazole (MMI)-treated group (patients with Graves’ disease treated with methimazole), the remission group (patients with Graves’ disease in remission), and the control group (healthy volunteers) (Table 1). We explained the purpose of the study to all subjects and obtained their informed consent. The 20 patients in the untreated group consisted of 3 men and 17 women with a mean age of 44.4 yr who were complaining of finger tremors, palpitation, weight loss, and squatting and/or arm-up limitation in daily life. Diagnosis of Graves’ disease was confirmed by the elevated free T3 level (24.88 ⫾ 9.22 pmol/L), the undetectable TSH level, and the positive TSH binding inhibitory Ig and/or thyroid-stimulating antibody. Their CPK, lactate dehydrogenase, and GOT levels were within normal range (data not shown). Patients with periodic paralysis were not included. MMI-treated subjects, basically drawn from the untreated group, were treated with MMI and performed the semiischemic forearm test again. Free T4 (17.25 ⫾ 5.41 pmol/L) normalized at 3 months after daily administration of 30 mg MMI. Patients who were in a hypothyroid state during MMI treatment were not included in the second trial. Eleven of the 20 patients in the MMI-treated group who performed the second exercise test still complained of muscle symptoms. The remission group included treated patients in whom normalized thyroid function and absence of thyroid-stimulating antibody and TSH binding inhibitory Ig lasted for at least 1 yr. Statistical analysis The values of ⌬lactate, ⌬pyruvate, ⌬ammonia, and ⌬hypoxanthine in each group were determined and compared by ANOVA. Differences with P ⬍ 0.05 were considered statistically significant. The correlation between lactate and ammonia was also estimated, and the regression line was calculated. ENHANCED ACTIVITY OF THE PURINE NUCLEOTIDE CYCLE IN HYPERTHYROIDISM 2207 TABLE 1. Serum free T3, free T4, and TSH concentrations in untreated Graves’ disease, MMI-treated Graves’ disease, remission, and control groups Graves’ disease Untreated (n ⫽ 20) Treated (n ⫽ 11) Remission (n ⫽ 13) 44.4 ⫾ 5.99 (f17/m3) 24.88 ⫾ 9.22 60.49 ⫾ 23.17 ⬍0.02 37.8 ⫾ 24.7 362 ⫾ 279 44.3 ⫾ 17.8 (f9/m2) 4.30 ⫾ 1.64 17.25 ⫾ 5.41 1.98 ⫾ 0.83 25.8 ⫾ 14.2 211 ⫾ 152 40.8 ⫾ 15.2 (f11/m2) 4.92 ⫾ 0.61 12.87 ⫾ 3.86 1.50 ⫾ 0.42 8.2 ⫾ 4.9 115 ⫾ 23 Age/sex Free T3 (pmol/L) Free T4 (pmol/L) TSH (mU/L) TBII (%) TSAB (%) Values are the mean ⫾ Control (n ⫽ 15) 50.6 ⫾ 20.7 (f11/m4) 5.53 ⫾ 0.92 18.02 ⫾ 5.15 1.86 ⫾ 0.38 Range 4.61– 8.91 11.53–28.31 0.3– 4.0 ⫺10 to 10 ⬍150 SD. FIG. 3. Glycolytic metabolite production in the untreated group during exercise. ⌬Lactate and ⌬pyruvate in the control (n ⫽ 15) and untreated groups (n ⫽ 20) were estimated (immediately after exercise ⫺ at rest). The raw values of lactate were as follows: control group: at rest, 1.01 ⫾ 0.34 mmol/L; after exercise, 2.44 ⫾ 0.66 mmol/L; and untreated group: at rest, 1.00 ⫾ 0.19 mmol/L; after exercise, 4.59 ⫾ 2.67 mmol/L. The raw values of pyruvate were as follows: control group: at rest, 67.01 ⫾ 23.03 mol/L; after exercise, 114.47 ⫾ 44.59 mol/L; and untreated group: at rest, 47.02 ⫾ 16.45 mol/L; after exercise, 133.72 ⫾ 60.54 mol/L. Results Release of glycolytic metabolites after exercise in the untreated group As expected, handgrip forearm exercise under semiischemic conditions resulted in poor ATP supply from aerobic glycolysis and induced anaerobic glycolysis, which produces lactate and pyruvate. After performing the handgrip exercise for 2 min, lactate (3.58 ⫾ 2.62 vs. 1.94 ⫾ 1.20 mmol/L; P ⬍ 0.05) and pyruvate (90.0 ⫾ 57.4 vs. 32.1 ⫾ 20.7 mol/L; P ⬍ 0.05) were significantly higher in the untreated group than in the control group (Fig. 3, A and B). Purine metabolic products after exercise in the untreated group Then we estimated purine metabolic products. After performing the handgrip exercise for 2 min, the level of ammonia released was significantly higher in the untreated group (80.6 ⫾ 81.3 vs. 18.3 ⫾ 18.9 mol/L; P ⬍ 0.05) than in the control group. The level of hypoxanthine released was also increased in the untreated group, but there was no significant difference between the untreated group and the control group (5.85 ⫾ 5.25 vs. 3.45 ⫾ 3.08 mol/L; P ⫽ 0.184; Fig. 4, A and B). Changes in muscle metabolic products in association with the recovery of thyroid function To study the direct effect of thyrotoxicosis on purine nucleotide catabolism, the semiischemic forearm exercise test was carried out in both the MMI-treated and remission groups. Figure 5 shows the responses of glycolytic and purine metabolites in the untreated, MMI-treated, and the remission groups. Lactate release did not decrease significantly in the MMI-treated group. In the remission group, the release of lactate markedly decreased, but the reduction was not significant either (Fig. 5A). The release of pyruvate and ammonia decreased in the MMI-treated group, but the reduction was not significant. However, in the remission group, the levels of pyruvate and ammonia normalized (Fig. 5, B and C). We also measured the level of hypoxanthine in the remission group (3.87 ⫾ 2.99 mol/L), and it was almost identical to that in the control group (data not shown). 2208 FUKUI ET AL. JCE & M • 2001 Vol. 86 • No. 5 FIG. 4. Purine metabolite production in the untreated group during exercise. ⌬Ammonia and ⌬hypoxanthine in the control (n ⫽ 15) and untreated groups (n ⫽ 20) were estimated (⌬ammonia, immediately after exercise ⫺ at rest; ⌬hypoxanthine, 10 min after exercise ⫺ at rest). The raw values of ammonia were as follows: control group: at rest, 28.87 ⫾ 13.61 mol/L; after exercise, 69.55 ⫾ 59.30 mol/L; and untreated group: at rest, 22.76 ⫾ 7.13 mol/L; after exercise, 87.67 ⫾ 79.28 mol/L. The raw values of hypoxanthine were as follows: control group: at rest, 1.43 ⫾ 1.64 mmol/L; after exercise, 4.66 ⫾ 3.57 mmol/L; and untreated group: at rest, 2.69 ⫾ 3.08 mmol/L; after exercise, 7.36 ⫾ 5.21 mmol/L. FIG. 5. Change in glycolytic and purine metabolite production by treatment of thyrotoxicosis. ⌬Lactate, ⌬pyruvate, and ⌬ammonia in the untreated (n ⫽ 20), MMI-treated (n ⫽ 11), and remission (n ⫽ 13) groups. The raw values of lactate (A)were as follows: untreated group: at rest, 1.00 ⫾ 0.19 mmol/L; after exercise, 4.59 ⫾ 2.67 mmol/L; MMI-treated group: at rest, 1.08 ⫾ 0.21 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L; and remission group: at rest, 0.98 ⫾ 0.30 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L. The raw values of pyruvate (B)were as follows: untreated group: at rest, 1.00 ⫾ 0.19 mmol/L; after exercise, 4.59 ⫾ 2.67 mmol/L; MMI-treated group: at rest, 1.08 ⫾ 0.21 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L; and remission group: at rest, 0.98 ⫾ 0.30 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L. The raw values of hypoxanthine (C) were as follows: untreated group: at rest, 1.00 ⫾ 0.19 mmol/L; after exercise, 4.59 ⫾ 2.67 mmol/L; MMI-treated group: at rest, 1.08 ⫾ 0.21 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L; and remission group: at rest, 0.98 ⫾ 0.30 mmol/L; after exercise, 4.36 ⫾ 1.59 mmol/L. Correlation between ⌬lactate and ⌬ammonia To estimate the relationship between glycolysis and the purine nucleotide cycle, we compared ⌬lactate and ⌬ammonia in these groups. A significant positive correlation between ⌬lactate and ⌬ammonia was found in all groups (Fig. 6). Therefore, ammonia production is supposed to be closely related to lactate production. When regression lines were calculated and compared among all groups, the slopes of the regression line in the untreated, MMI-treated, remission and control groups were 28.04, 34.5, 14.3, and 9.9, respectively. Based on these results, as the slope value of the regression line in the untreated group was much higher than that in the control group, ammonia production seemed to be much more accelerated than that of lactate in hyperthyroidism. Therefore, purine catabolism through the activation of the purine nucleotide cycle appeared to be more accelerated than ENHANCED ACTIVITY OF THE PURINE NUCLEOTIDE CYCLE IN HYPERTHYROIDISM 2209 FIG. 6. Correlation between ⌬lactate and ⌬ammonia. The regression lines of the untreated (f), MMI-treated (䡺), remission (F), and control (E) groups were calculated, and each regression formula is shown. glycolysis in hyperthyroidism. Such an enhancement of purine catabolism persisted for at least 3 months during MMI treatment, and it normalized after long-term maintenance of thyroid function. Simultaneously, we also estimated the correlation between ⌬lactate and ⌬hypoxanthine in each of the four groups, but there was no significant correlation between them (data not shown). This discrepancy between ⌬ammonia and ⌬hypoxanthine seemed to be a feature peculiar to patients with Graves’ disease. Discussion It is well known that patients with hyperthyroidism present muscle hypotonia, fatigue, and myopathy. Several studies pointed out that hyperthyroidism alters the ATP energy balance of skeletal muscle by increasing glycolysis or glycogenolysis (9 –11). In the present study we focused on purine nucleotide metabolism of muscles, which is regulated by the purine nucleotide cycle in hyperthyroidism and also contributes to ATP energy balance. In this study an elevation of serum lactate and pyruvate was observed after forearm exercise in patients with hyperthyroidism. Lactate and pyruvate are the metabolic products of glycolysis/glycogenolysis, and the glycolysis/glycogenolysis process is supposed to be accelerated in hyperthyroidism. This was not surprising, as the consumption of ATP in hyperthyroidism is known to be much greater than that in the normal state. Under semiischemic conditions, aerobic glycolysis tends to be suppressed, and instead, anaerobic glycolysis starts to work to catch up with the reduction of aerobic ATP supply. Then lactate, an anaerobic glycolytic metabolite, should be produced and released into the blood flow. The enhancement of muscle glycolysis in hyperthyroidism has been demonstrated by Kruk et al. (12). They observed that the lactate level was higher in hyperthyroidism than in healthy controls. These results indicated that in hyperthyroidism the muscle ATP content decreased, and this decrease was followed by enhanced glycolysis/glycogenolysis. Furthermore, an elevation of hypoxanthine and ammonia after forearm exercise was observed in thyrotoxic patients. This indicated that the activity of the purine nucleotide cycle was clearly accelerated in hyperthyroidism. In general, an acceleration of purine catabolism occurs due to the disturbances of the glycolytic systems similar to that in muscle phosphorylase deficiency (glycogen storage disease type V) (7). This is because ADP is rapidly converted to AMP by adenylate kinase when the ATP supply is disturbed by impairment of the glycolytic system. Additionally, once the purine nucleotide cycle is activated (IMP3inosine3hypoxanthine), hypoxanthine and ammonia production is augmented by AMP deamination. We observed a significant increase in ammonia after exercise in patients with hyperthyroidism. However, the difference in hypoxanthine release between hyperthyroidism and healthy controls was not significant, although the average value appeared to be higher in thyrotoxic patients. This result was puzzling, because accelerated purine catabolism should produce hypoxanthine in parallel with ammonia as metabolites. In glycogen storage disease type V, which accompanies the acceleration of the purine nucleotide cycle, hypoxanthine production strongly correlates with ammonia production (7). We propose the following possibilities to explain this discrepancy. When IMP is converted to hypoxanthine, the salvage process (IMP to AMP) also works, which influences the release of hypoxanthine independently of the release of ammonia (13). Although the conversion of IMP to inosine is regulated by 5⬘-nucleotidase (Fig. 1), this enzyme is controlled by the intracellular pH. In hyperthyroidism, semiischemic exercise rapidly increases im lactate, and accumulated lactate reduces the im pH level. Such a pH reduction may suppress 5⬘-nucleotidase activity, and the conversion of IMP to inosine would be suppressed; therefore, 2210 JCE & M • 2001 Vol. 86 • No. 5 FUKUI ET AL. the subsequent hypoxanthine production may also be decreased. Another explanation is that thyrotoxicosis directly suppresses 5⬘-nucleotidase activity, and then hypoxanthine production is suppressed. To elucidate the hypoxanthine result, it will be necessary to measure 5⬘-nucleotidase activity and IMP and inosine production in the exercising muscle in patients with hyperthyroidism. It is now clear that both glycolysis and purine nucleotide catabolism are remarkably accelerated in hyperthyroidism. There are several explanations for the mechanisms involved in the acceleration of purine metabolism. In hyperthyroidism, a large amount of ATP is supposed to be consumed during exercise compared with that in healthy controls, and the ATP supply from the glycolytic system is rapidly depleted, which automatically advances to purine catabolism (14). Other studies pointed out changes in the composition of muscle fiber type induced by hyperthyroidism. Fitts et al. reported that type II fibers (anaerobic glycolytic muscle) in rat muscles were increased by the administration of T3 and T4 (15). The content of type I fibers in hypothyroidism is higher than that in healthy subjects, and it is decreased by T4 administration (16). Moreover, Celsing et al. found that type I fibers could be converted to type II fibers in skeletal muscles of patients with hyperthyroidism (17). It is well known that AMP deaminase activity of type II fibers is higher than that of type I fibers. Therefore, the whole AMP deaminase activity in muscle could be enhanced by the conversion of type I to type II fibers in hyperthyroidism. Moreover, it was reported that the im glycogen content in hyperthyroidism was remarkably lower than that in healthy controls. Celsing et al. demonstrated that the glycogen content was markedly lower in type I fibers in hyperthyroidism using biopsy specimens of muscles (17). Taken together, we presume the following possibilities for enhanced purine catabolism in hyperthyroidism: 1) an increase in ATP consumption due to the augmented basal metabolic rate; 2) the acceleration of AMP deaminase activity by the conversion of muscle fiber type; and 3) a poor supplementation of ATP due to the low im glycogen content. As mentioned above, purine catabolism contributes to the ATP energy balance in skeletal muscle. The acceleration of purine catabolism results in the rapid conversion of AMP to IMP, which maintains the im energy charge. Thus, acceleration of purine catabolism may be a protective adjustment of skeletal muscles of patients with hyperthyroidism to avoid a rapid collapse of ATP energy balance. It seemed important to determine whether the improvement of hyperthyroidism was associated with the normalization of glycolysis and purine nucleotide catabolism. As shown in Fig. 5, purine catabolism normalized in parallel with the recovery of thyroid function. All responses of metabolites, except lactate, completely improved in the remission group. This result again confirms that purine metabolism of skeletal muscles is directly affected by thyrotoxicosis. In this respect it is noteworthy that a positive correlation between lactate and ammonia was observed and that the regression line did not improve after 3 months of treatment with MMI (Fig. 5, untreated vs. MMI-treated group). This result suggests that purine catabolism (AMP3 IMP ⫹ NH4) is more accelerated in hyperthyroidism than in anaerobic glycolysis (glycogen3lactate). The maintenance of thyroid function for 2 months was not enough to improve the accelerated purine catabolism in skeletal muscles. However, the values of the regression line in the remission group were almost identical to those in healthy controls, indicating that long-term maintenance of thyroid function is necessary to improve the purine metabolic change in muscles in hyperthyroidism. Complete recovery of fiber type change or glycolysis in hyperthyroidism may require a long-term maintenance of thyroid function. This observation is compatible with clinical findings, as muscular symptoms in patients with Graves’ disease tend to continue even after the complete recovery of thyroid function by MMI treatment. In conclusion, our study revealed that glycolysis and purine catabolism were remarkably accelerated in hyperthyroidism, purine catabolism would normalize in association with a long-term maintenance of thyroid function, and thyrotoxic myopathy could be closely related to the acceleration of purine catabolism. Acknowledgment We thank Prof. Kazumitsu Hirai for his continuous encouragement. References 1. Hofmann WW, Smith RA. 1970 Hypokalemic periodic paralysis studies in vitro. Brain. 93:445– 474. 2. Edelman IS, Ismali-Beigi F. 1970 Mechanism of thyroid calorogenesis: role of active sodium transport. Proc Natl Acad Sci USA. 67:1071–1078. 3. Ruff RT. 1986 Endocrine myopathies. Myology. 1881–1887. 4. Aragon JJ, Tornheim K, Goodman MN, et al. 1981 Replenishment of citric acid cycle intermediates by the purine nucleotide cycle in rat skeletel muscle. Curr Top Cell Regul. 18:131. 5. Zoref-Shani E, Shainberg A, Kessler-Icekson G. 1986 Production and degradation of AMP in cultured rat skeletal and heart muscle: a comparative study. Adv Exp Med Biol. 195:485– 491. 6. Hara N, Mineo I, Kono N, Shimizu T, et al. 1987 Enhanced release of ammonia and hypoxanthine from exercising muscles in patients with idiopathic hypoparathyroidism. Muscle Nerve. 10:599 – 602. 7. Mineo I, Kono N, Shimizu T, et al. 1985 Excess purine degradation in exercising muscles of patients with glycogen storage disease types V and VII. J Clin Invest. 76:556 –560. 8. Kono N, Mineo I, Sumi S, et al. 1984 Metabolic basis of improved exercise tolerance: muscle phosphorylase deficiency after glucagon administration. Neurology. 34:1471–1476. 9. Gustafsson R, Tara JR, Lindberg O, et al. 1965 The relationship between the structure and activity of rat skeletal muscle mitochondria after thyroidectomy and thyroid hormone treatment. J Cell Biol. 26:555–570. 10. Kubista V, Kubista J, Petle D. 1971 Thyroid hormone induced changes in the enzyme activity pattern of energy supplying metabolism of fast (white), slow (red), and heart muscle of the rat. Eur J Biochem. 18:553–560. 11. Tara JR, Ernster L, Lindberg O, et al. 1963 The action of thyroid hormone at the cell level. Biochem J. 86:408 – 428. 12. Kruk B, Brzezinska Z, Kaciuba-Uscilko H, and Nazar K. 1988 Thyroid hormones and muscle metabolism in dogs. Horm Metab Res. 20:620 – 623. 13. Hisatome I, Kitamura H, Saitoh M, et al. 1991 Excess release of hypoxanthine from exercising muscle in two Gout patients with partial HGPRTase deficiency: lack of ammonia release. Am J Med. 90:533–535. 14. Hisatome I, Ishiko R, Mashiba H, et al. 1990 Excess purine degradation in skeletal muscle with hyperthyroidism. Musle Nerve. 13:558 –559. 15. Fitts RH, Winder WW, Brooke MH, et al. 1980 Contractile, biochemical and histochemical properties of thyrotoxic rat soleus muscle. Am J Physiol. 238:C15–C20. 16. McKeran O, Slaving G, Andrews TM, et al. 1975 Muscle fiber type changes in hypothyroid myopathy. J Clin Pathol. 28:659 – 663. 17. Celsing F, Blomstrand F, Melichna J, et al. 1986 Effect of hyperthyroidism on fibre-type composition, fibre area, glycogen content and enzyme activity in human skeletal muscle. Clin Physiol. 6:171–181.