Notebook
Care of the Patient with Hematological
Disorders
Lesson 1: Hematologic and Immunologic System Anatomy
and Physiology
Lesson 2: Assessment, Diagnostic Tests and Monitoring
Systems
Lesson 3: Pathologic Conditions Patient
Inside:
•
Module Outline
•
Lesson Objectives
•
Lesson Summary
•
Lesson Resource Files
•
Lesson Practice Pearls
2
Module Outline
Module 9 - Care of the Patient with Hematological Disorders
Lesson 1 - Hematologic and Immunologic System Anatomy and Physiology
Topic 1: Structures, Components and Functions
Topic 2: Coagulation Mechanism and Fibrinolysis
Topic 3: Immunologic Basics
Lesson 2 - Assessment, Diagnostic Tests and Monitoring Systems
Topic 1: Hematology Studies
Topic 2: Coagulation Studies
Topic 3: Immunology Studies
Lesson 3 - Pathologic Conditions
Topic 1: Anemia
Topic 2: Thrombocytopenia
Topic 3: Disseminated Intravascular Coagulation
Topic 4: Immunocompromise
Topic 5: Other Coagulopathies
Lesson 1
Hematologic and Immunologic
System Anatomy and Physiology
Included in this Lesson:
• Structures, Components and Functions
• Coagulation Mechanism and Fibrinolysis
• Immunologic Basics
4
Lesson: Hematologic System Anatomy & Physiology
Objectives
Topic:
Introduction
Upon completion of this lesson you will be able to:
•
Identify and discuss function of components of hematologic systems
-
Describe the structures and functions of the components of the
hematologic system
-
Discuss the mechanism of coagulation and fibrinolysis
Page of 3
5
Lesson Take-away - Hematologic System Anatomy and Physiology
Topic One: Structures, Components and Functions
Importance of Understanding the Hematologic System
In this lesson we looked at the anatomy and physiology of the hematologic system and learned why an understanding of the
hematologic system is so essential to the acute care clinician. We learned that something as routine as bedrest can lead to
clot formation (deep vein thrombosis) and a pulmonary emboli. We also learned that disseminated intravascular coagulation
(DIC) could result from any tissue damage and that anemia and thrombocytopenia can be common in acutely ill patients.
Assessment of the hematologic system is an essential part of assessing a patient in acute care and it includes:
• Taking a history of any predisposing factors
• Assessing and exploring in depth any personal or genetic history of bleeding, chronic anemia, or systemic diseases such
as renal failure, liver disease, or cancer
• Asking whether the patient is taking any medication affecting the hematologic system such as anticoagulant drugs such as
warfarin, unfractionated or low-molecular weight heparin, antiplatelet drugs such as aspirin or clopidogrel, and steroids or
non-steroidal medications such as ibuprofen
• Noticing any physical signs which may indicate an underlying hematologic problem such as pale or jaundiced skin color, a
history of unexplained bruising or clotting or ecchymosis, and petechiae.
• Noticing other symptoms like hematochezia or melena, hematuria, hemoptysis, and menorrhagia.
Anatomic Structures
The anatomic structures of the hematologic system are as follows:
• Bone marrow – The spongy material in the center of the bones, particularly long bones and also in the skull, vertebrae,
ribs, and pelvis. It is in the bone marrow that the cells of the hematologic system and the immunologic system originate,
mature, and are released into the bloodstream.
• Liver – Removes nonfunctioning erythrocytes from the blood stream.
• Spleen – Removes damaged erythrocytes from the blood.
• The following cellular components:
• Red blood cells or erythrocytes
• Platelets or thrombocytes
• Coagulation factors
• Stem cells – All cells produced by the bone marrow (and therefore all hematologic and immunologic system cells)
originate from the stem cell. Stem cells produce daughter cells which then differentiate into one of the two following
types of cells:
• lymphoid stem cells (these produce ß cells which function in the immune system)
• myeloid stem cells (these produce erythrocytes and thrombocytes)
Erythrocyte production is stimulated during hypoxemia by the kidney which, in response to hypoxemia occurring, produces
the hormone erythropoietin in order to get the stem cells in the bone marrow to make erythrocytes. This erythrocyte
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
Page of 3
6
production is important since erythrocytes have hemoglobin, the substance that transports the needed oxygen to tissues for
aerobic metabolism (ATP production) and removal of CO2 (the byproduct of oxygen metabolism.) This transport by
erythrocytes of oxygen via the blood to tissues throughout the body is called “oxygenation.”
Thrombocyte or platelet production and the coagulation mechanism is stimulated/activated during a tissue injury or blood
vessel injury. When such an injury occurs, platelets rush to the site of injury and form a platelet plug. Cytokines are released,
causing additional platelets to be activated, the coagulation mechanism to continue, and an immune response to be
stimulated.
Topic Two: Coagulation Mechanism and Fibrinolysis
Two Main Functions
The hematologic system’s two main functions are oxygenation (discussed above) and homeostasis. Homeostasis is the
process of clotting or coagulation in order to prevent hemorrhage and the corresponding mechanism of fibrinolysis, the
dissolving of the blood clot to some degree so that it doesn’t become too large.
Coagulation and Fibrinolysis
Homeostasis is the body’s system of self-regulating and it is accomplished through the coagulation mechanism. The
coagulation mechanism is a combination of two seemingly opposite activities: clotting and “fibrinolysis” (clot-dissolving; the
breaking up of and limiting the size of clots.) This second activity is the body’s way of preventing hemorrhaging while, at the
same time, ensuring that it doesn’t clot too much; only enough to stop the bleeding. Once the bleeding has been stopped,
clot-dissolving begins.
Clot-dissolving occurs by a blood protein dissolving the clot, breaking down the fibrin into fragments. We can get information
about the clot-dissolving activity by measuring the levels of “fibrin split products” or “fibrin degradation products” (the
fragments created when fibrin is broken down.)
We examined this coagulation mechanism in more detail and learned that the coagulation mechanism is a cascade of
events involving 12 factors and several cofactors (plasma proteins.) This cascade of events always ends in the production of
thrombin (Factor IIa.)
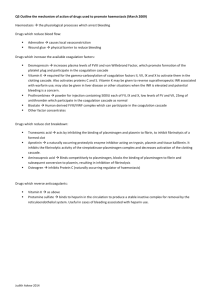
While the cascade of events always ends in thrombin being produced, it begins or is initiated in one of two ways: through an
intrinsic pathway (in response to vessel wall damage,) or through an extrinsic pathway (in response to tissue damage.) The
end result, however, is always the same: thrombin (Factor IIa) is produced. Thrombin splits circulating fibrinogen (Factor I) to
form fibrin and the blood clot.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
Page of 3
7
Related Drugs
In acute and critical care there exist drugs which inhibit or enhance the coagulation mechanism and fibrinolysis. Some of
these drugs are:
• Anticoagulants – prevent coagulation (clotting.) Can be used in viro as a medication for thrombotic disorders.
• Antiplatelet drugs – decrease platelet aggregation and inhibit thrombus formation. Are effective in arterial circulation—an
area where anticoagulants have little effect.
• Thrombolytic agents – can dissolve a blood clot (thrombus) and reopen an artery or vein
• Antifibrinolytic agents – prevent fibrinolysis or lysis of a blood clot
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
8
Lesson: Hematologic System Anatomy & Physiology
Cellular Components
Topic:
Structures, Components and Functions
Cellular Components
Stem cells
Myeloid
stem cell
Erythrocytes
Lymphoid
stem cell
Platelets
B-cells
T-cells
9
Coagulation Mechanism
Lesson: Hematologic System Anatomy & Physiology
Topic:
Structures, Components and Functions
Coagulation Mechanism
Extrinsic Pathway
Intrinsic Pathway
Tissue damage
Vessel wall
damage
VII → VIIa
Tissue factor
XI → XIa
VII → VIIa
IX → IXa
X → 7 Xa
Thrombin
Fibrin
Clot
10
Hematology Drugs
Lesson: Hematologic System Anatomy & Physiology
Topic:
CLASS OF DRUG
Structures, Components and Functions
NAME OF DRUG
THERAPEUTIC USE
Anticoagulants
Indirect Thrombin
Inhibitors
Unfractionated Heparin
Treatment or prevention of
venous thrombosis.
Adjunct to thrombolytic therapy
with ACS
Low Molecular Weight Heparins
Ardeparin (Normiflo)
Enoxaparin (Lovenox)
Dalteparin (Fragmin)
Prevention of venous
thromboemboli
Fondaparinux (Arixta)
Prevention of venous
thromboemboli with the risk of
HIT because the agent is
synthetic not made from animal
proteins which heparin and
LMWH are
Hirudin Derivatives
Lepirudin (Refludan)
Bivalirubin (Angiomax)
Heparin substitute for patients
at risk or experiencing HIT
Argatroban (Acova, Novastan)
Heparin substitute for patients
at risk or experiencing HIT
Recombinant Human
Activated Protein C
(sometimes categorized
as a thrombolytic agent)
Drotrecogin alpha activated (Xigris)
Severe sepsis
Vitamin K Antagonist
Warfarin (Coumadin)
Prevention of venous
thromboemboli development
Direct Thrombin Inhibitors
11
Antiplatelet Drugs
Cyclooxygenase Inhibitor
Aspirin
At antiplatelet dose (75-325mg)
Primary and secondary
prevention and treatment for
ACS. Secondary prevention in
stroke.
Adenosine Diphosphate
Receptor Antagonists
Ticlopidine (Ticlid)
Clopidogrel (Plavix)
Reduction of atherosclerotic
events in patients with recent
stroke or MI.
Vascular disease
Dipyridamole (Persantine)
Thromboembolism prevention
follow cardiac valve surgery
Glycoprotein IIb/IIIa
Receptor Antagonist
Abciximab (ReoPro)
Eptifibatide (Integrelin)
Tirofiban (Aggrastat)
Acute coronary syndrome with
or without percutaneous
coronary intervention (PCI)
Thrombolytic Agents
Streptokinase (Kabikiane, Streptase)
Alteplase (tPA)
Reteplase (rtPA)
Teneteplase (TNKase)
ACS, DVT, PE
Adjunct to PCI
Thrombotic Stroke
Antifibrinolytic Agents
Aminocaproic Acid
(EACA, Amicar, Epsilson)
Aprotinin (Trasylol)
Coagulopathies with
hemorrhage
Lesson 2
Assessment, Diagnostic Tests and
Monitoring Systems
Included in this Lesson:
• Hematology Studies
• Coagulation Studies
• Immunology Studies
13
Lesson: Hematologic Diagnostic Tests
Objectives
Topic:
Hematology Studies
Upon completion of this lesson you will be able to:
•
Analyze basic hematologic and immunologic laboratory test results
-
Identify normal and abnormal complete blood count results
-
Identify normal and abnormal white blood cell differential
-
Identify normal and abnormal erythrocyte sedimentation rate
-
Identify normal and abnormal prothrombin time and international
normalization ratio
-
Identify normal and abnormal partial thromboplastin time
-
Identify normal and abnormal fibrinogen
-
Identify normal and abnormal fibrin split levels/D-dimer
-
Identify normal and abnormal results of basic immunology studies
Page of 4
14
Lesson Take-away - Hematologic Diagnostic Tests
Topic One: Hematology Studies
The Importance of Understanding Hematologic Diagnostic Tests
In this lesson we discussed the diagnostic tests commonly used to identify hematologic disorders and alterations in
coagulation. These common diagnostic tests are important for helping you to evaluate the hematologic status of a patient,
diagnose disorders, and anticipate the type of treatment a patient requires.
The hematologic system is evaluated through the use of several laboratory tests. Laboratory tests are the main source of
assessment data for evaluating hematologic health.
The Complete Blood Count (CBC)
The CBC is a lab test that provides information about many different things which are of significance to the hematologic
system including:
• Platelet count (Remember that platelets are also called thrombocytes.)
• Hematocrit and hemoglobin – These rise and fall linearly with the RBC count, however they are also affected by
intravascular volume status.
• RBC count (Red Blood Cell count.) Remember that mature red blood cells are also called erythrocytes.
• A high RBC could indicate erythrocytosis.
• A low RBC could indicate anemia. A common reason for a low RBC count is bleeding. However, RBC
could also be low due to a lack of production of erythrocytes from bone marrow suppression or early
destruction of red cells from hemolysis or sickle cell disease.
Through the use of mathematical formulas, the following red blood cell indices-which are usually calculated automatically in
a CBC-help the clinician to narrow down the cause of an anemia more clearly, if other than bleeding. The red blood cell
indices are MCV, MCHC, and RDW.
Mean Corpuscular Volume (MCV)
MCV measures the average volume of a red blood cell (by dividing the hematocrit by the RBC) and indicates whether it
(MCV) is normal, decreased, or increased. Also categorizes the red blood cells by size, indicating that they are either
“normocytic” (normal sized,) “microcytic” (smaller sized,) or “macrocytic” (larger sized.) With all of this information, we can
characterize the type anemia present:
• Normocytic anemias have normal-sized cells and a normal MCV
• Microcytic anemias have small red blood cells and a decreased MCV
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
Page of 4
15
• Macrocytic anemias have large red blood cells and an increased MCV
Under a microscope, stained red blood cells having a high or increased MCV also appear macrocytic or larger sized than
those having normal or decreased MCV.
Mean Corpuscular Hemoglobin Concentration (MCHC)
MCHC measures the average concentration of hemoglobin in a red blood cell (by dividing the hemoglobin by the
hematocrit.) and indicates whether the cells are “normochromic” (having a normal concentration of hemoglobin) or
“hypochromic” (having a lower than normal concentration of hemoglobin.) Because there is a physical limit to the amount of
hemoglobin that can fit in a cell, there is no “hyperchromic” category. Remember that it is the hemoglobin in red blood cells
(or erythrocytes) that transports the needed oxygen to tissues in the body. Therefore hemoglobin is very important.
The iron in hemoglobin is what gives blood its characteristic red color. When examined under a microscope, normochromic
cells (red blood cells having a normal amount of hemoglobin and thereby a normal MCHC) stain pinkish red with a paler
area in the center. By contrast, hypochromic cells (red blood cells having too little hemoglobin and thereby a lower MCHC)
are lighter in color with a larger pale area in the center. With the information provided by the MCHC index, we can
characterize the type of anemia present as hypochromic or normochromic.
Cell Distribution Width (RDW)
RDW measures the variation in size in the red blood cells. Usually red blood cells are a standard size. Certain disorders,
however, cause significant variation in cell size.
Other Tests
Besides the CBC, we also looked at these tests for evaluating hematologic health:
• Reticulocyte (immature erythrocyte) count – Measures the amount of reticulytes in order to determine whether or not the
patient is making the correct amount of new red blood cells. (Recall that all hematologic cells originate from stem cells. The
stem cells produce daughter cells which then differentiate into one of two types of cells, one type being myeloid stem cells
from which erythrocytes and thrombocytes are produced.) Once a stem cell becomes an erythrocyte it is a reticulocyte first
for about two weeks. As long as the patient is well nourished, has a functioning liver, and produces a healthy red cell, the
reticulocyte eventually matures into a fully functioning erythrocyte.
• ESR (Erythrocyte Sedimentation Rate, or sed rate) – Measures the heaviness of the red cell.
• An increase in ESR or sed rate reflects inflammation in the body. Although an increased sed rate or ESR does not
tell the cause of the inflammation (sepsis or rheumatoid arthritis,) it at least alerts the clinician that there is
inflammation. The correlation between inflammation and increased sed rate is as follows: When inflammation is
present, a high proportion of fibrinogen is in the blood and this causes red blood cells to stick to each other, forming
stacks called 'rouleaux' which settle faster.
• ESR is decreased in sickle cell anemia, polycythemia, and heart failure.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
Page of 4
16
• Bilirubin levels. Bilirubin is the name for broken up red blood cells. The average life span of a erythrocyte or mature red
blood cell is 120 days at which point it gets broken up and becomes bilirubin. Bilirubin is fat soluble and in order to be
excreted, must be converted to a water soluble form. Ths conversion occurs in the liver.
• An elevation of unconjugated (indirect) bilirubin reflects either an increase in hemolysis or liver dysfunction.
• An elevation of conjugated (direct) bilirubin indicates that the liver has converted the bilirubin but that it was
blocked from being excreted for some reason. One such reason might be the presence of gallstones.
Topic Two: Coagulation Studies
Assessing Patient’s Coagulation State
Recall from Lesson 1 that the hematologic system’s two main functions are oxygenation (red blood cells) and homeostasis.
Homeostasis is the combination of both clotting/coagulation (in order to stop hemorrhage) and fibrinolysis (clot dissolving;
occurs once the bleeding has been stopped and in order to keep clotting from continuing unchecked.)
Coagulation is always initiated either through an intrinsic pathway (vessel wall damage) or through an extrinsic pathway
(tissue damage) and that both events result in thrombin (Factor IIa) being produced. Thrombin is one of many plasma
proteins (12 clotting factors and several co-factors) which play a role in coagulation or clotting. Thrombin forms fibrin and the
blood clot by splitting circulating fibrinogen (Factor I.) In Lesson 1 we also looked at some of the drugs used for inhibiting
and enhancing both coagulation and fibrinolysis.
Recall that clot-dissolving occurs by fibrin being broken down into fragments called “fibrin split products” or “fibrin
degradation products.” Measuring the levels of these fibrin split products or fibrin degradation products can provide us
information about clot-dissolving within a particular patient.
There are several blood studies which can be used to assess whether coagulation and fibrinolysis are occurring normally in
a patient. They are as follows:
• Tests that determine whether a patient has the plasma proteins (clotting factors) needed to form a clot.
• PT (Prothrombin Time) and the INR (International Normalized Ratio) - Help assess the extrinsic pathway of the
coagulation mechanism
• PTT (Partial Thromboplastin Time) - Helps identify the intrinsic pathway of the coagulation mechanism
The PT, INR, and PTT are also used to assess the effectiveness of anticoagulation therapy. For example, the PT is used to
evaluate the effectiveness of warfarin and the PTT is used to evaluate heparin therapy.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
Page of 4
17
• A Bleed Time test - Can help determine vascular integrity and platelet function or the patient’s ability to clot when
necessary.
• A review of the platelet (thrombocyte) count (the count done as part of the CBC) is helpful because it can help determine
the patient’s ability to clot. Recall that platelets and the plasma proteins (clotting factors and co-factors) are what initiate
clotting and form the foundation for the blood clot.
• A look at fibrinogen level. The fibrinogen level reflects the circulating amount of factor I, which is necessary to form a
clot. Fibrogen levels will be low when a patient has made clots and may be elevated with sepsis.
• A look at the level of fibrin split products (also called fibrin degradation products). This looks at the amount of circulating
broken up fibrin or clots is important. For example, elevations in D-Dimer - a type of fibrin split product produced when cross
linked fibrin is broken up - are common when the clots formed are from deep vein thrombosis, disseminated intravascular
coagulation, many cancer states, and sickle cell crisis.
• Thrombin Time (TT) – This test can be helpful in evaluating the effectiveness of anticoagulation thrombolytic agents like
tissue plasminogen activator (tPa) once they have been administered.
• Using the Activating Clotting Time (ACT) test in conjunction with a PTT to evaluate anticoagulation with heparin therapy.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
18
Hematologic Study Table
Lesson: Hematologic Diagnostic Tests
Topic:
Red Blood Cell Laboratory Tests
Hematology Studies
19
Lesson: Hematologic Diagnostic Tests
Coagulation Studies
Topic:
TEST
Platelet Count
Prothrombin Time (PT)
Coagulation Studies
NORMAL RANGE
150,000400,000/mm3
11-15 seconds
International Normalized
Ratio (INR)
0.7 – 1.8
Activated Partial
Thromboplastin Time
(aPTT)
PTT 60 – 70
seconds
Anti-Factor Xa
0 units/mL
DVT tx:
LMWH 0.4 1.1 U/ml
DVT Prophylaxis:
< 0.45 U/ml
Depends on system
Ivy 1-8, Duke 1-3min
70 – 120 seconds
Bleeding Time
Activated Clotting Time
(ACT)
PARAMETER MEASURED
# of Circulating Platelets, Measures
Amount not Functional Ability
Extrinsic & Common Coagulation
Pathways
Evaluation of Warfarin Therapy
Standardized method of reporting the PT
Evaluation of Warfarin Therapy
Intrinsic & Common Coagulation
Pathways
Evaluation of Heparin Therapy
Low Molecular Weight Heparin
Monitoring
Normal Platelet and Tissue Function
with Bleeding
Fibrinogen
Thrombin Time (TT)
200 - 400mg/dL
14 -16 sec
Fibrin Degradation (Split)
Products
D-Dimer
2-10mcg/ml
Intrinsic & Common Coagulation
Pathways
Evaluation of Heparin Therapy
Circulating Fibrinogen
Common Coagulation Pathway and
Quality of the Functional Fibrinogen
Evaluation of tPA therapy
Degree of Fibrinolysis
< 2.5mcg/ml
Specific Fibrin Breakdown Product
Lesson 3
Pathologic Conditions
Included in this Lesson:
• Anemia
• Thrombocytopenia
• Disseminated Intravascular Coagulation
• Immunocompromise
• Other Coagulopathies
21
Objectives
Module: Care of the Patient with Hematologic Disorders
Lesson: Pathologic Conditions
Upon completion of this lesson you will be able to:
•
Describe the etiology, pathophysiology, clinical presentation, management
of critically ill patients with:
- Anemia
- Thrombocytopenia
- Disseminated intravascular coagulation
•
Describe the etiology, pathophysiology, clinical presentation, and
management of critically ill patients with other coagulapathies
22
Page of 8
Lesson Take-away - Pathologic Conditions
Topic One: Anemia
Common Hematologic Disorders
In Lesson 3 we covered hematologic disorders commonly encountered in the critically ill patient population. Understanding
anemia, thrombocytopenia, and disseminated intravascular coagulopathy (DIC) depends on one understanding the
coagulation pathways as well as the diagnostic tests used to identify the various disorders.
Anemia Basics
Anemia by definition is a low red blood cell count. Anemia is seen in many critically ill patients. Employing interventions that
minimize blood loss will help prevent anemia.
The human body is fueled by oxygen. The oxygen is delivered to all the cells and organs by hemoglobin. When there is a
lack of or inadequate delivery of oxygen, the body will not function normally. The primary problem with anemia is a
decreased number of red blood cells. Since red blood cells have hemoglobin, decreased red blood cells means decreased
ability for the body to have adequate oxygen delivery.
The etiologies for anemia can be classified into these three categories:
• Blood Loss - This is certainly the easiest to
• Early Elimination/Destruction of red blood cells
understand and also the most frequent cause of anemia
Destruction of red blood cells, called “hemolysis,” can be
in the hospitalized patient. The loss could be from
enhanced by things like the cardiopulmonary bypass
trauma, surgery, gastrointestinal bleeding or conditions
machine, intra-aortic balloon pumping, and mechanical
that increase the bleeding such as disseminated
heart valves. Activation of the immune response can cause
intravascular coagulation, anticoagulant administration
a hemolytic anemia as can sickle cell anemia/disease,
and excessive blood draws.
G6PD deficiency, and thrombotic thrombocytopenia
• Underproduction of red blood cells This could occur
purpura.
from malnutrition, chronic illness, malignancies and
cancer therapies or from organ dysfunction specifically
liver or renal.
By definition, anemia is a low red blood cell count. It
becomes clinically significant when the cells/organs are not
receiving enough oxygen and the body begins initiating
compensatory mechanisms, all of which have the single
goal of increasing oxygen delivery.
Symptomatic anemia will present on assessment with
tachycardia, weak pulses, orthostatic hypotension, ECG
changes, an increased respiratory rate and work of
breathing, pale skin and mucous membranes, decreased
urinary output, and a decreased level of consciousness.
The degree of symptoms related directly to the degree of
anemia and also the timeframe within which the anemia
has developed. At the point that oxygen delivery becomes
inadequate for the body’s demands, the patient crosses the
line from anemia into hypovolemic shock. The acutely or
chronically ill adult may not have the physiological reserve
to mount a strong compensatory response to anemia.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
23
Page of 8
The primary goal in anemia management in acute care is
adequate oxygen delivery. So the treatment options are
guided by the severity of the patient’s symptoms more than
by the absolute number listed on the CBC for RBC count or
hemoglobin.
To accomplish adequate oxygen delivery, packed red
blood cells are administered. Additional treatments include
supplemental oxygen, minimizing activity, and optimizing
cardiac output and pulmonary function. The administration
of recombinant human erythropoietin or supplemental
vitamins and minerals might also help the development and
Sickle Cell Disease (SSD)
Sickle Cell Disease (SSD,) frequently referred to as sickle
cell anemia, manifests as a life-long hemolytic anemia. To
have SSD a person must inherit the “hemoglobin S” (HgbS)
trait from both of their parents. The abnormal Hgb causes
an altered shape (sickle shape) which results in a
decreased ability to carry oxygen and a decreased lifespan
by the red blood cells, thereby accounting for the anemia.
A person with SSD may also experience crises from the
microvascular hypoxia and clotting that can occur. Crises
may be stimulated by an infection, cold temperature,
acidosis, dehydration, or changes in atmospheric oxygen
(altitude.) The patient will present with severe pain, fever,
fatigue, tachycardia, tachypnea, and hematuria.
release of healthy red blood cells from the bone marrow.
The cause for the anemia must be identified and treated.
Blood conservation policies should be considered on all
acute and critically ill patients and heightened for those
with anemia. Strategies that may help decrease the
incidence of anemia are:
• Limiting blood draws
• Using autotransfusion whenever possible
• Administering gastrointestinal bleeding
prophylaxis medications
Laboratory findings include a low RBC, HCT, Hgb, and
elevated reticulocyte (immature red blood cells) counts
typically with a microcytic anemia. Patients with coexisting
vascular disease are at high risk for stroke or ACS during
crises.
There is no cure for SSD so treatment is currently directed
at anemia management and crises prevention. Should
crises occur, our goal is to manage symptoms. The primary
methods are:
• Hydration
• Oxygen administration
• Pain medication administration
Plasma exchange and hyperbaric chamber therapy have
also been used.
Sickle Cell Crisis Patterns
There are now four recognized patterns of acute sickle cell crisis:
• Bone Crisis - An acute or sudden pain in a bone can occur, usually in an arm or leg. The area may be tender. Common
bones involved include the large bones in the arm or leg: the humerus, tibia, and femur. The same bone may be affected
repeatedly in future episodes of bone crisis.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
24
Page of 8
• Acute Chest Syndrome - Sudden acute chest pain with coughing up of blood can occur. Low-grade fevers can be
present. The person is usually short of breath. If a cough is present, it often is nonproductive. Acute chest syndrome is
common in a young person with sickle cell disease. Chronic (long-term) sickle cell lung disease develops with time because
the acute and subacute lung crisis leads to scarred lungs and other problems.
• Abdominal Crisis - The pain associated with the abdominal crisis of sickle cell disease is constant and sudden. It
becomes unrelenting. The pain may or may not be localized to any one area of the abdomen. Nausea, vomiting, and
diarrhea may or may not occur.
• Joint Crisis -Acute and painful joint crisis may develop without a significant traumatic history. Its focus is either in a single
joint or in multiple joints. Often the connecting bony parts of the joint are painful. Range of motion is often restricted because
of the pain.
Hemophilia
Hemophilia is an X chromosome-linked inherited bleeding
disorder. Although females can carry the gene, only males
can have the disease. Hemophiliacs lack the normal
amounts of either clotting factor VIII or clotting factor IX.
Because of their inadequate clotting ability, they are at high
risk their entire life for mild, moderate, and severe bleeding.
When not bleeding this patient will have a normal PT, TT,
and Bleeding Time but a prolonged aPTT, and of course
low factor VIII or IX levels. During bleeding episodes, the
above coagulation studies will be elevated.
The treatment for hemophilia is to prevent bleeding risk.
When bleeding does occur, the goal is to limit blood loss
and, if necessary, transfuse the patient with packed red
blood cells, FFP, platelets, and cryoprecipitate (which has
factor VIII.) Patients might also be given sterile factor
concentrates of factor VIII to help enhance clotting and limit
bleeding.
Recombinant human factor VIIa (“rhVIIa”) has been
approved for the use of bleeding associated with
hemophilia. Medications to enhance clotting like DDAVP or
antifibrinolytic agents might also be utilized to control
hemorrhage.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
25
Page of 8
Topic Two: Thrombocytopenia
Thrombocytopenia Basics
Like anemia, Thrombocytopenia is also fairly common in
critically ill. It is one of the most common coagulation
disorders identified in the acutely ill adult population. Some
common interventions such as the administration of
heparin may lead to the development of thrombocytopenia.
difficult. In fact, the term “idiopathic thrombocytopenic
purpura” or ITP—a term for thrombocytopenia where the
clinical team is unable to determine the origin of the low
platelet count—is the most common documented etiology
for thrombocytopenia.
Thrombocytopenia is defined as an abnormally low number
of platelets resulting in inadequate hemostasis. Since
platelets play a major role in clotting the primary concern
with thrombocytopenia is bleeding. It is one of the most
common coagulation disorders identified in the acutely ill
adult population.
Thrombocytopenia is often associated with conditions
resulting from altered immunity such as systemic lupus
erythmatosus (SLE) and AIDS, malignancies, bone marrow
suppression, liver disease, eclampsia, splenomegaly,
hemorrhage, and massive transfusions. Also, excessive
alcohol intake and the use of some medications (i.e., the
use of thiazide diuretics in elderly) are common
precipitating causes of thrombocytopenia.
Although thrombocytopenia or low platelet count is
common, identifying the cause of low platelet count is often
Etiologic causes of thrombocytopenia are related to one of
the following five pathogenic processes:
• decreased platelet production
• decreased platelet survival
• excessive consumption of platelets
• splenic sequestration of platelets
• platelet dilution (massive volume administration)
The end result of each of these processes is an insufficient
number of platelets available for maintaining adequate
homeostasis, and therefore hemorrhage occurs. In some
disorders, the process of platelet destruction activates the
thrombocytes (platelets) and causes them to stick together
stimulating thrombosis production.
In some
thrombocytopenic states, the outcome is a potential for
increased clotting; not bleeding.
The severity of clinical signs and symptoms of
thrombocytopenia increase as platelet count falls. The
clinical presentation can be assessed on a physical exam
where internal or external bleeding signs are present.
Signs and Symptoms
Common signs and symptoms of Thrombocytopenia are as follows:
• Renal signs: Hematuria
• Laboratory signs: Platelet count is severely
• Gastrointestinal signs: Hematemesis, melena,
diminished. Red cell count and hemoglobin levels will be
hematochezia
normal. Coagulation studies will be normal.
• Neurological signs: Severe headache, nausea and/or
• Integumentary signs: Petechial hemorrhage of lower
vomiting, seizures, focal neurologic deficits, decreased
extremities, ecchymoses, gingival bleeding, spontaneous
level of consciousness.
epistaxis
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
26
Page of 8
• Miscellaneous signs: Retinal hemorrhage, heavy menses in women
Diagnoses
The diagnosis of thrombocytopenia is made by the
presence of a low platelet count and a prolonged bleeding
time. PT and aPTT will be normal. Examination of platelet
morphology can provide clues as to the origin of
thrombocytopenia.
ITP
Recall that ITP—thrombocytopenia where the origin of the
low platelet count cannot be determined—is the most
common documented etiology for thrombocytopenia. Two
other etiologies for thrombocytopenia are seen in acutely ill
patients as well— Heparin Induced Thrombocytopenia
(HIT) and Thrombotic Thrombocytopenic Purpura (TTP.)
This process can happen to any patient who has had
heparin administered but is most frequently seen in the
cardiac and orthopedic populations, probably because
heparin is a common therapy in those specialties. The
heparin can be from any source — intravenous,
subcutaneous, through catheter flushes, and even through
heparin bonded catheters.
HIT is diagnosed with clinical findings and blood work. The
primary diagnosis is thrombocytopenia with an unexplained
drop (usually > 50% their baseline) somewhere between
days 5 and 10 after heparin administration. The drop may
be more rapid if the patient had been administered heparin
in the past and developed antibodies. Blood can be sent for
antibody screening to confirm HIT.
TTP
The potential etiologies for Thrombotic Thrombocytopenic
Purpura (TTP) can be congenital, idiopathic, or secondary.
HIT
Heparin Induced Thrombocytopenia (HIT) with or without
thrombus (HITT) is an uncommon immune reaction to
heparin therapy. It is a transient acquired hypercoagulable
syndrome. Because the drug heparin is made from bovine
or porcine proteins, the patient’s immune system might
produce antibodies to the antigens on the animal protein, in
turn leading to platelet destruction and thrombocytopenia.
The platelet destruction might lead to thromboemboli
development.
Thrombus development occurs in about 35-58% of patients
having HIT. The clots can be venous or arterial and have
presented as all of the following: DIC, stroke, myocardial
infarction, renal infarction, and at the sites of surgical
grafts.
Treatment for HIT is to first stop the heparin administration
and to administer a non-heparin anticoagulant until the
patient’s platelet count has returned to his or her baseline.
Caution should be taken when administering platelets to a
patient with suspected HIT. Platelet transfusions are
typically not done unless the patient has severe bleeding.
The patient should be identified as having a heparin allergy
although the incidence of a repeat of HIT with subsequent
heparin administration is unknown at this time because the
antibody development is not permanent.
The most common secondary cause is medications;
however other secondary causes are infection,
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
27
Page of 8
malignancies, autoimmune disorders, immunizations, and
hypertensive crisis.
This disorder presents with a low platelet count and a
hemolytic anemia (drop in red blood cell count from early
destruction or hemolysis.) Despite the fact that the platelet
count will be low in a person with TTP, the person may also
present with microvascular thrombi. The mechanism that
destroys the platelets also activates them and platelet
aggregation is stimulated. While systemic microvascular
thrombi may occur, the most common sites are renal and
CNS. Fever is also common. In addition to the
thrombocytopenia and hemolytic anemia, other laboratory
Another hematologic condition with thrombocytopenia
exists as well and it is called HELLP or HELLP syndrome.
This is a life-threatening condition of pregnancy seen in
hospitals with large high-risk obstetric populations. The
acronym describes the clinical presentation—Hemolysis
with Elevated Liver enzymes and Low Platelets is exactly
how these women present.
HELLP is a result of pregnancy induced hypertension (PIH)
or “preeclampsia.” The subsequent severe vasoconstriction
causes destruction of red blood cells and platelets and the
potential for ischemia to any organ bed although the
hepatic and renal systems are most commonly affected.
findings in TTP include elevated reticulocyte count and
serum lactate dehydrogenase (LDH,) but normal
fibrinogen, PT and aPTT.
Treatment for TTP is to identify and stop the cause.
Antiplatelet agents are frequently given to decrease the
likelihood of clot formation. Plasma exchange,
immunosuppressive therapy, and splenectomy have also
been shown to be useful in treating TTP. Platelet
administration is not done unless the patient is bleeding
since giving a patient with TTP platelets might give them
more cells to destroy and be used for thrombus formation.
The laboratory findings include the following: low RBC,
Hemglobin, Hematocrit, and platelet count, high liver
function tests, BUN, creatinine and D-Dimer, and normal
PT and aPTT.
The treatment for HELLP is the same as for PIH; namely,
to treat the hypertension and deliver the fetus in order to
stop the cause of the PIH and prevent subsequent
complications of the vasoconstriction. Attempt to minimize
blood loss and treat and support the organ dysfunction that
might have resulted from the severe vasoconstriction.
Disorders of a Qualitative Nature – Normal Platelet Count but Abnormal Platelet Function
While Thrombocytopenia is a quantitative platelet disorder (a disorder related t platelet or thrombocyte count,) there are
qualitative platelet disorders as well. In such types of disorders, the patient might have a normal thrombyte count and yet
their platelets are not functioning normally, leading to bleeding. Two examples of qualitative platelet disorders follow:
• A patient who has taken an antiplatelet drug like
aspirin, clopidogrel (Plavix,) dipyridamole (Persantine,)
and the GPIIb/IIIa inhibitors abciximab (ReoPro,)
eptifibatide (Integrelin,) and tirofiban (Aggrastat.) These
drugs disrupt platelet function, limiting the formation of a
platelet clot.
• VonWillebrand’s disease - a congenital or acquired
decrease or absence of the plasma protein co-factor
“vonWillebrand’s factor” which is needed to stabilize
clotting factor VIII and which helps fibrinogen hold platelets
together.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
28
Page of 8
The primary focus of patient management is on identifying and correcting the underlying cause of the thrombocytopenia.
This may include discontinuing any medications that may alter platelet function such as aspirin and NSAIDs. The use of
corticosteroids to increase platelet production may be indicated. The most common treatment for thrombocytopenia with
associated bleeding is the administration of human platelets.
Plasmapheresis—the mechanical removal of platelet-free plasma from the patient’s circulation— may be considered. If the
spleen is believed to be involved, a splenectomy may be performed.
Topic Three: Disseminated Intravascular Coagulation
Disseminated Intravascular Coagulation Basics
While DIC is less common than anemia or thrombocytopenia, it is potentially life threatening. Disseminated Intravascular
Coagulation, or DIC, occurs when the normal coagulation and fibrinolytic mechanisms are altered and there is abnormal
activation of coagulation and secondary fibrinolysis simultaneously.
DIC occurs secondary to other major illnesses such as:
• Obstetric complications (the most common cause.)
These can include chemicals from the uterus being
released into the blood, or from amniotic fluid embolisms,
and eclampsia . Another obstetric condition which can
cause DIC is abruptio placentae.
• Sepsis, particularly with gram-negative bacteria
• Tissue trauma such as burns, accidents, surgery, and
shock
• Liver disease
• Incompatible blood transfusion reactions or a massive
blood transfusion (more than the total circulatory volume)
• Cancers, widespread tissue damage (e.g. burns,) or
hypersensitivity reactions that produce the chemicals
• Acute promyelocytic leukemia
• Viral hemorrhagic fevers
• Envenomation by some species of venomous snakes,
such as those belonging to the genus Echis (saw-scaled
vipers.)
Although the risk factors contributing to the initiation of DIC are diverse, there are three common physiologic responses.
When tissue damage, platelet damage, and endothelial damage occur, the intrinsic or extrinsic coagulation mechanism
becomes activated and microvascular thrombi develop. This is the normal response to tissue and cellular damage.
As thrombi are formed, vascular occlusion and tissue ischemia may develop affecting end organ perfusion and therefore
function. The normal physiological response to thrombi development is the fibrinolytic response, where fibrinolysis is initiated
and fibrin split products (FSP) and D-Dimer are released.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
29
Page of 8
FSPs function as anticoagulants, enhancing the breaking up of clots. The area where clot formation occurred may begin to
bleed again and then clot again. As coagulation factors are rapidly consumed, excessive bleeding results. If not reversed,
this process will result in severe blood loss and hemorrhagic shock, increased microvascular clotting,
hypoperfusion/ischemia, and multi-organ dysfunction/failure which would eventually lead to death.
The patient’s history will reveal a concurrent condition known to precipitate DIC and spontaneous bleeding in the absence of
known coagulation abnormalities:
• Unexplained petechiae, ecchymoses, and hematomas
may be present upon assessment of the skin.
• Spontaneous epistaxis, bleeding from the conjunctiva,
bleeding from the hematuria, or intracranial bleeding may
be noted.
• Unusually excessive or prolonged oozing or bleeding
following venipuncture or from existing IV sites or
wounds may be seen.
Abnormal coagulation studies will confirm the diagnosis of DIC:
• All of the following will be elevated: PT, aPTT, fibrin split products, and D-dimer. Elevation of fibrin split products in
the presence of elevated D-dimer is highly indicative of DIC.
• Platelet and fibrinogen levels will be decreased because they have been consumed in the formation of the clots.
Because DIC is secondary to other conditions, the primary focus is to identify and correct the underlying cause and support
the patient symptomatically. Depleted coagulation factors must be replaced by using packed red blood cells, fresh frozen
plasma, platelets, or cryoprecipitate. Additional treatment goals include decreasing all bleeding risks to the patient and
monitoring and treating pain aggressively.
The use of heparin to treat DIC remains controversial. Its use has never been validated with a double blind research study.
However, many believe it has a beneficial effect in deactivating the coagulation or clotting process which started the
physiological cascade of clotting and bleeding.
© 2008 American Association of Critical-Care Nurses (AACN). All rights reserved.
30
Anemia Symptoms
Lesson: Care of the Patient with Hematologic Disorders
Topic: Anemia
Cardiovascular System
Pulmonary System
Neurologic Symptoms
Gastrointestinal System
Integumentary System
Tachycardia
Palpitations
Angina
Increased cardiac output
Decreased capillary refill
Hypovolemic shock
Orthostatic hypotension
ECG abnormalities
Dyspnea on exertion
Tachypnea
Fatigue
Headache
Faintness
Light-headedness
Restlessness
Irritiability
Splenomegaly
Hepatomegaly
Cool skin temperature
Muscle cramps
Pallor of skin and mucous membranes
Dusky nailbeds
Intermittent claudication
31
Blood Component Therapy 1,2
Component
Whole blood
Red Blood Cells (RBCs)
(increase oxygen-carrying
capacity)
• Packed
• Frozen
• Washed/re-centrifuged
• Irradiated
• Fresh frozen plasma
(source of plasma proteins
for patients who are
deficient in or have
defective plasma proteins –
contains all coagulation
factors. Can be used for
plasmaphersis.)
Indications
Additional Information
Red Blood Cell Containing Components
Acute hemorrhage, most often trauma
• Less available
• Need algorithms to guide usage
• Must be ABO identical with recipient
Active bleeding: maintain volume,
• May contain approximately 20-150 mL of residual plasma
Hemoglobin stability
• May be used for exchange transfusion
Not active bleeding:
• Should not be used for volume expansion or for anemias that can be
Hgb < 5 or 6 g/dL: universal
corrected with medications (iron, vitamin B12, folic acid,
Hgb over 10 g/dL: never
erythropoietin)
Hgb >5 and < 10 g/dL: based on
• Must be ABO compatible with recipient
signs, symptoms, physiology*
• Each unit contains enough hemoglobin to ↑ concentration
approximately 1 g/dL
(hematocrit ↑ by 3 percentage points)
• Give as fast as pt can tolerate but over less than 4 hours
Plasma and Plasma Fractions
• Preoperative or bleeding patients who
• Each mL of undiluted plasma contains 1 international unit (IU) of each
require replacement of multiple plasma
coagulation factor.
coagulation factors (dilutional
• Do not use when coagulopathy can be corrected with specific therapy
coagulopathies)
(Vitamin K, cryoprecipitated AHF, or Factor VIII)
• Patients with massive transfusion who
• Do not use for volume expansion when blood volume can be replaced
have clinically significant coagulation
safely with other volume expanders
deficiencies
• Compatibility tests are not necessary
• Patients on warfarin who are bleeding or • Must be ABO compatible with recipient red cells
need to undergo invasive procedure
• Monitor with lab assays of coagulation function
before Vit K could reduce effect
• Can be given by rapid bolus infusion; otherwise over less than 4 hours.
• Patients with thrombotic thrombocytic
• Vitamin K reversal of Warfarin can take up to 6-8 hours.
purpura (TTP)
• Patients with coagulation factor
deficiencies for which no specific
plasma concentrates are available
32
• Cryoprecipitate
(source of Factor VIII,
vonWillebrand Factor,
Factor XIII)
• Control of bleeding associated with
fibrinogen deficiency
• Treatment of Factor XIII deficiency.
• DIC
• Compatibility testing is unnecessary
• ABO compatibility is preferred, Rh type not considered
• Should contain > 80 IU Factor VIII and 150 mg of fibrinogen per 15
mL of plasma
• Give over less than 4 hours.
• Laboratory studies must indicate specific hemostatic defect for use of
this product
Platelet Components
Platelets
NO bleeding present:
• Requirements increase if other coagulopathy present or if platelets not
Pooled Platelets
• Prophylaxis for CNS bleed in bone
functioning normally.
Leukocyte Reduced
marrow failure
• Check count after 1 hour in bleeding patient.
Platelets
• Prophylaxis for major surgical procedure • Compatibility testing is not necessary.
(essential for hemostasis,
• RARELY need prophylaxis for minor
• Should be ABO compatible with recipient in infants or with large
transfuse to provide
surgery
volumes of transfusion.
adequate numbers of
BLEEDING Patient:
• One unit of platelets should increase platelet count in 70-kg adult by 5normally functioning
• Transfuse to > 50,000/mm3 if possible
10,000 mm3
platelets for prevention or
• Usual adult dose is 4-8 units.
cessation of bleeding)
• Can transfuse as fast as tolerated, must be less than 4 hrs.
• Lifespan of transfused platelets = 3-4 days
• Some patients may require single donor vs. pooled platelets.
Granulocyte Components
Granulocytes
• Treatment of neutropenic patients who
• Collected by hemapheresis – each concentrate = > 1.0 x 1010
(decrease level of bacterial
have documented infections and have
granulocytes
and fungal infection in
not responded to antibiotics
• Must be ABO compatible
neutropenic patients)
• Hereditary neutrophil function defects
• Should be irradiated to prevent graft vs host disease (GVHD).
• Rarely associated with increment in patient’s granulocyte count
• Transfuse as soon as possible; each unit to be given over 2-4 hours.
• Use standard blood transfusion set.
*American Association of Blood Banks Audit Criteria
33
General Principles for Transfusion1
• All blood components must be transfused through a filter designed to remove clots and aggregates (generally a standard 170-260 micron filter).
• No medications or solutions may be routinely added to or infused through the same tubing with blood or components with the exception of 0.9%
Sodium Chloride, Injection (USP), unless a) they have been approved for this use by the FDA or b) there is documentation available to show that
the addition is safe and does not adversely affect the blood or component.
• Lactated Ringer’s, Injection (USP) or other solutions containing calcium should never be added to or infused through the same tubing with blood or
components containing citrate.
• Sterility must be maintained.
• The intended recipient and the blood container must be properly identified before the transfusion is started.
• Blood components may be warmed if clinically indicated for situations such as exchange or massive transfusions, or for patients with cold-reactive
antibodies. Warming must be accomplished using an FDA-cleared warming device so as not to cause hemolysis.
• Transfusion should be completed within 4 hours and prior to component expiration.
• Some life-threatening reactions occur after the infusion of only a small volume of blood. Therefore, unless otherwise indicated by the patient’s
clinical condition, the rate of infusions should initially be slow. Periodic observation and recording of vital signs should occur during and after the
transfusion to identify suspected adverse reactions. If a transfusion reaction occurs, the transfusion must be discontinued immediately and
appropriate therapy initiated. The infusion should not be restarted unless approved by transfusion service protocol.
• All adverse events related to transfusion, including possible bacterial contamination of a blood component or suspected disease transmission, must
be reported to the transfusion service according to its local protocol.
References:
1
American Association of Blood Banks, America’s Blood Centers, American Red Cross. Circular of Information for the Use of Human Blood and
Blood Components. http://www.aabb.org/Documents/About_Blood/Circulars_of_Information/coi0702.pdf. 2002. Accessed April 17, 2006.
2
Luce J. Blood and blood products, blood substitutes. Presentation at ACCP Critical Care Board Review, August 2005.
3
Luce J. The bleeding patient in the ICU. Presentation at ACCP Critical Care Board Review, August 2005.
4
Pagana K, Pagana T. Mosby’s Manual of Diagnostic and Laboratory Tests.3rd Ed. St. Louis: Mosby, Inc; 2006.
34
Coagulation Monitoring3,4
Monitoring
Tissue and
vascular factors
Platelets
Fibrin generation
Thrombin
generation
Indications*
DIC, abnormal platelet
volume or function,
uremia, warfarin overdose,
anti-inflammatory drugs
DIC, liver failure, massive
transfusion (dilutional
coagulopathies), platelet
disorders (ITP, TTP),
platelet function
abnormalities (drugs such
as aspirin, IIB/IIIA
inhibitors) uremia, HIT
DIC, liver failure, massive
transfusion
DIC, heparin
administration, massive
transfusion, acquired Vit K
deficiency, HIT, warfarin
administration
DIC, anticoagulation
therapy
Measurement
Bleeding time
Normal
1-9 minutes (Ivy method)
Critical Values
> 15 minutes on repeat eval
Platelet count
Adult:150,000 – 400,000/mm3
Child: 150,000 – 400,000/mm3
Infant:200,000 – 475,000/mm3
Premature Infant: 100,000-300,000/mm3
Newborn: 150,000 – 300,000/mm3
Platelet
Antibodies
Fibrinogen
None identified
• > 10,000/mm3 prevents
spontaneous CNS hemorrhage
• > 50,000/mm3 prevents most
medical/surgical bleeding
• >100,000/ mm3 when
anticipating bypass, vascular,
other major surgery.
PT
PTT
Adult: 200-400 mg/dL or 2-4 g/L (SI units)
Newborn: 125-300 mg/dL
11.0-12.5 seconds; INR 1.5-2.0
APTT: 30 - 40 seconds
PTT: 60 – 70 seconds
<100 mg/dL can be associated
with spontaneous bleeding
Therapeutic INR = 2-3.5
Therapeutic PTT: 1.5 – 2x normal
Critical values: APTT > 70 secs
PTT > 100 secs
Factor Assays
Normals vary according to specific factor
Unclotting or
FDP
<10mcg/mL or <10 mg/L (SI units)
Critical value: >40 mcg/mL
Thrombosis
D-dimers
Qual – negative
Quant <250ng/mL or <250 mcg/L (SI units)
indicators
*Listing not all inclusive
DIC – Disseminated intravascular coagulation ITP – Immune thrombocytopenic purpura TTP – Thrombotic thrombocytopenic purpura
HIT - Heparin induced thrombocytopenia PT – Prothrombin time PTT – Partial thromboplastin time FDP – Fibrin degradation products
35
Risk Factors for DIC
Lesson: Care of the Patient with Hematologic Disorders
Topic:
GENERAL
CLASSIFICATIONS
Anemia
PRIMARY
EVENT/DISORDER
PRIMARY
EVENT/DISORDER
Tissue Damage
Major Surgery
Major Trauma
Heat Stroke
Head Injury
Burns
Transplant Rejection
Extracorporeal Circulation
Snake Bites
Obstetric
Complications
HELLP
Amniotic Emboli
Abruptio Placenta
Fetal Demise
NS Abortion
Eclampsia
Placenta Accreta
Placenta Previa
Shock States
Cardiogenic Shock
Septic Shock (severe
infection or inflammation)
Hemorrhagic Shock
Dissecting Aneurysm (large
vessels)
Massive Blood and Volume
Resuscitation
Drowning
Anaphylaxis
Neoplasms
Acute & Chronic Leukemia
Acute & Chronic Lymphoma
Solid Tumors
Hamangiomas
Hematologic
Disorders
Thrombotic
Thrombocytopenic Purpura
(TTP)
Transfusion Reactions
Collagen Vascular
Disorders
Thrombocythemia
Sickle Cell Crisis
Specific System
Dysfunction
Acute & Chronic Renal Dis
Ulcerative Colitis
DKA, Acid Ingestion
HIV Disease
ARDS
Acute Pancreatitis
Liver Dysfunction/Failure
SIRS & MODS
Pulmonary Embolism
Fat Embolism
36
Care of the Patient with
Hematologic and Immunologic
Disorders
Lesson: Pathologic Conditions
Topic: Anemia
Practice Pearls
Etiologies for Anemia
G6PD deficiency is an inherited condition in which the body doesn't have enough of the
enzyme glucose-6-phosphate dehydrogenase, or G6PD, which helps red blood cells
(RBCs) function normally.
G6PD deficiency is most common in African-American males. Many African-American
females are carriers of G6PD deficiency, meaning they can pass the gene for the
deficiency to their children, but do not have symptoms; only a few are actually affected
by G6PD deficiency. People of Mediterranean heritage, including Italians, Greeks,
Arabs, and Sephardic Jews, also are commonly affected. The severity of G6PD
deficiency varies among these groups–it tends to be milder in African-Americans and
more severe in people of Mediterranean descent.
Symptomatic Anemia
The hemoglobin or red blood cell levels that are indicative of anemia have not been
firmly established. This is a debate that continues in the critical care and hematology
literature. When dealing with anemia, the focus should be on the clinical symptoms of
the patient rather than the hemoglobin or RBC value.
Anemia Management
Transfusion Related Acute Lung Injury (TRALI) is defined as an acute lung injury that is
temporally related to a blood transfusion; specifically, it must occur within the first six
hours following a transfusion. It is the third leading cause of transfusion-related deaths.
The etiology is still not known, but it is thought to be a result of the presence of
antibodies in multiparous females or patients who have received previous transfusions.
Symptoms include dyspnea, hypotension and fever.
37
Care of the Patient with
Hematologic and Immunologic
Disorders
Lesson: Pathologic Conditions
Topic: Thrombocytopenia
Signs and Symptoms of Thrombocytopenia
With a platelet count of 50,000/mm3, increased bruising and bleeding following minor
trauma may be noted. Petechiae and purpura manifest as the platelet count falls below
50,000/mm3. When platelet counts fall dangerously low, below 20,000/mm3,
hemorrhage occurs, particularly in the mucosa, deep tissues, and intracranial space.
38
Care of the Patient with
Hematologic and Immunologic
Disorders
Lesson: Pathologic Conditions
Topic: Disseminated Intravascular Coagulation
Use of Heparin
There are currently several treatments that have not been approved by the FDA being
used to treat DIC. These are Activated Protein C, Antithrombin III and rhFVIIa. These
treatments are currently being studied and showing promise in the treatment of DIC.
39
Care of the Patient with
Hematologic and Immunologic
Disorders
Lesson: Pathologic Conditions
Topic: Lesson Review
Lesson Summary
Emerging science is strengthening the connection between sepsis and DIC. Assessing
for the presence of DIC and early intervention are increasingly common in the critically
ill.
40
Care of the Patient with
Hematologic and Immunologic
Disorders
Glossary
Cryoprecipitate
the precipitate that forms when plasma is frozen then thawed.
Particularly rich in fibronectin and blood clotting Factor VIII.
Cytokines
non-antibody proteins secreted by both inflammatory leukocytes and
some non-leukocytic cells that act as intercellular mediators. They
differ from classical hormones in that they are produced by a
number of tissue or cell types rather than by specialized glands.
They generally act locally in a paracrine or autocrine (rather than
endocrine) manner.
D-dimer
the cross-linked fibrin degradation fragment. Elevations in this
fragment are seen in primary and secondary fibrinolysis, during
thrombolytic or defibrination therapy with tissue plasminogen
activator, as a result of thrombotic disease such as deep-vein
thrombosis, pulmonary embolism or DIC, in vase-occlusive crisis of
sickle cell anemia, in malignancies, and in surgery.
Ecchymosis
a small hemorrhagic spot, larger than a petechia, in the skin or
mucous membrane forming a non-elevated, rounded or irregular,
blue or purplish patch.
Erythropoietin
a Glycoprotein (46 kD) hormone produced by specialized cells in the
kidneys that regulates the production of red blood cells in the
marrow. These cells are sensitive to low arterial oxygen
concentration and will release erythropoeitin when oxygen is low.
Erythropoeitin stimulates the bone marrow to produce more red
blood cells (to increase the oxygen-carrying capacity of the blood.)
The measurement of this hormone in the bloodstream can indicate
bone marrow disorders or kidney disease. Normal levels of
erythropoietin are 0 to 19 mU/ml (milliunits per milliliter.) Elevated
levels can be seen in polycythemia rubra vera. Lower than normal
values are seen in chronic renal failure. Recombinant erythopoietin is
now being used therapeutically in patients.
41
Extrinsic
an inherited disorder that causes abnormal blood clotting due to the
congenital absence of one of the 20 different plasma proteins
involved in the coagulation process. Symptoms include bleeding of
the gums, nosebleeds, easy bruising, bleeding in muscles or joints,
and excessive menstrual bleeding. Treatment includes the
administration of plasma concentrates of Factor VII (extrinsic factor
i.e. dietary vitamin B12.)
Fibrin split
products
the insoluble protein formed from fibrinogen by the proteolytic
action of thrombin during normal clotting of blood. Fibrin forms the
essential portion of the blood clot.
Hematochezia
the passage of bright red blood per rectum. This symptom may be
associated with hemorrhoids, anal fissure, rectal polyp, cancer,
diverticulitis or inflammatory bowel disease.
Hematuria
the finding of blood in the urine
Hemoptysis
the expectoration of blood or of blood stained sputum
Intrinsic
a mucoprotein normally secreted by the epithelium of the stomach
and that binds vitamin B12; the intrinsic factor/B12 complex is
selectively absorbed by the distal ileum, though only the vitamin is
taken into the cell.
Lupus
erythmatosus
skin disease in which there are red scaly patches, especially over the
nose and cheeks. May be a symptom of systemic lupus
erythematous (a disease of humans, probably autoimmune with
antinuclear and other antibodies in plasma.) Immune complex
deposition in the glomerular capillaries is a particular problem.
Lymphoid cells
cells derived from stem cells of the lymphoid lineage. Large and
small lymphocytes, plasma cells.
Melena
the passage of black and tarry (sticky) stools stained with blood
pigments or with altered blood
42
Menorrhagia
excessive uterine bleeding occurring at the regular intervals of
menstruation, the period of flow being of greater than usual duration
Morphology
a study of the configuration or structure of animals, cells, tissue, etc.
Myeloid cells
one of the two classes of marrow derived blood cells, includes
megakaryocytes, erythrocyte precursors, mononuclear phagocytes
and all the polymorphonuclear granulocytes. That all these are
ultimately derived from one stem cell lineage is shown by the
occurrence of the Philadelphia chromosome in these, but not
lymphoid, cells. Most authors tend, however, to restrict the term
myeloid to mononuclear phagocytes and granulocytes and
commonly distinguish a separate erythroid lineage.
Petechiae
small red spots on the skin that usually indicate a low platelet count.
Pinpoint, non-raised, perfectly round, purplish red spots caused by
intradermal or submucous hemorrhage.
Plasmapheresis
centrifuging blood that has been removed from the body to separate
the cellular elements from the plasma
Stem cells
relatively undifferentiated cells of the same lineage (family type)
that retain the ability to divide and cycle throughout postnatal life to
provide cells that can become specialized and take the place of those
that die or are lost