Allograft of ovarian cortex between two genetically non

Journal: HUMAN REPRODUCTION
Article Id: dem211
Article Title: Allograft of ovarian cortex between two genetically non-identical sisters: a case report
First Author: J. Donnez
Corr. Author: J. Donnez
AUTHOR QUERIES - TO BE ANSWERED BY THE CORRESPONDING AUTHOR
The following queries have arisen during the typesetting of your manuscript. Please answer these queries by marking the required corrections at the appropriate point in the text.
Q1
Q2
Author: please check.
Please provide telephone number of the corresponding author.
Q3
Q4
Q5
Q6
Q7
Q8
Q9
As per the publisher's style, abstract should be structured as
'BACKGROUND, METHODS, RESULTS, CONCLUSIONS'. So please set the abstract in a structured format.
Author: please check.
Author: please check.
Author: please check.
Author: please check and add reference—sentence added in response to reviewer 1.
Author: please check.
Author: please check concentration against Fig. 5.
Human Reproduction pp. 1–6, 2007
Copy Edited by: B.M
doi:10.1093
/ humrep / dem211
Allograft of ovarian cortex between two genetically
5
Q1
non-identical sisters: a case report
10
J. Donnez
1,2,3
, M.M. Dolmans
1,2
, C. Pirard
1
, A.Van Langendonckt
2
, D. Demylle
1
, P. Jadoul
1
and J. Squifflet
1
15
1
Department of Gynecology, Cliniques Universitaires St. Luc, Universite´ Catholique de Louvain, Avenue Hippocrate 10, B-1200 Brussels,
Belgium;
2
Gynecology Research Unit, Universite´ Catholique de Louvain, Brussels, Belgium
70
Q2
3
Correspondence address. Fax: þ 32 2 764 95 07; E-mail: donnez@gyne.ucl.ac.be
20
25
Q3
BACKGROUND: Aggressive chemotherapy and radiotherapy generally result in the loss of both endocrine and reproductive functions. In 1990, a woman aged 20 years, presenting with b -thalassemia major, underwent chemotherapy (busulfan and cyclophosphamide) and total body irradiation (TBI) before bone marrow transplantation (BMT), the donor being her 17-year-old HLA-compatible sister. The treatment resulted in premature ovarian failure. CASE
REPORT: In 2006, after excision of ovarian cortical fragments from the HLA-compatible sister, these fragments were immediately sutured to the ovarian medulla of the patient. Both procedures were performed by laparoscopy. Six months after reimplantation, vaginal ultrasonography and hormone concentrations indicated recovery of ovarian secretion and function. From 6 to 11 months, the patient experienced menstrual bleeding and the development of a follicle concomitant with high estradiol levels. Eleven months after reimplantation, two follicles were detected and punctured under vaginal ultrasonographic control. Two mature oocytes were retrieved and inseminated by ICSI.
Two embryos (2- and 3-cell) were obtained. CONCLUSIONS: Allotransplantation of fresh ovarian tissue was laparoscopically performed between two genetically non-identical sisters. Restoration of ovarian function was achieved after six months. Oocyte retrieval and embryo development were demonstrated .
75
80
85
30
Keywords: allograft; ovarian tissue; ovarian recovery; ovarian transplantation.
90
65
60
35
40
45
50
55
Introduction
Aggressive chemotherapy and radiotherapy generally result in the loss of both endocrine and reproductive function and, in most female patients, these treatments lead to ovarian failure.
Cyclophosphamide is the agent most commonly implicated in causing damage to oocytes and granulosa cells in a dosedependent manner. Total body irradiation (TBI), required before bone marrow transplantation (BMT), associated with chemotherapy constitute the treatment combination presenting the greatest risk of premature ovarian failure (POF) (Sanders et al ., 1996; Teinturier et al ., 1998; Meirow and Nugent,
2001; Larsen et al ., 2003; Wallace et al ., 2005; Donnez et al ., 2006a).
A large retrospective survey of pregnancy outcomes after hematopoietic stem cell transplantation (SCT) (peripheral blood or BMT) involving 37 362 patients revealed that only 0.6% of patients conceived after autologous or allogenic SCT (Salooja et al ., 2001; Lutchman Singh et al .,
2005). It is thus obvious that high doses of alkylating agents, irradiation and advancing age increase the risk of gonadal damage.
Several options are available to preserve fertility in patients facing POF, including immature and mature oocyte cryopreservation, embryo cryopreservation and ovarian tissue cryopreservation. The last option is the only possible alternative for patients who need immediate chemotherapy.
Both orthotopic and heterotopic autologous transplantation of cryopreserved ovarian cortical tissue have been described, as reviewed by Donnez et al . (2006a). Three live births after orthotopic autotransplantation of cryopreserved ovarian tissue have been reported (Donnez et al ., 2004; Meirow et al ., 2005, 2007;
Andersen et al . (2007) personal communication). Two further pregnancies, both ending in miscarriage, were also documented
(Schmidt et al ., 2005; Demeestere et al ., 2006). Five pregnancies following transplantation of fresh ovarian tissue between monozygotic twin sisters were reported by Silber et al . (Silber et al ., 2005; Silber and Gosden, 2007), who clearly described the technique of ovarian cortex removal in the recipient before fixation of donor ovarian cortex to the recipient medulla.
Here, we describe the first case of orthotopic allotransplantation of fresh ovarian tissue between two genetically nonidentical sisters.
95
100
105
110
115
# The Author 2007. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology.
All rights reserved. For Permissions, please email: journals.permissions@oxfordjournals.org
Page 1 of 6
Donnez et al.
Case report
120
125
130
Q4
135
140
145
150
155
160
165
Patient
In 1990, a 20-year-old woman presenting with b -thalassemia major underwent chemotherapy (busulfan 16 mg / kg and cyclophosphamide 200 mg / kg) and TBI (750 cGy) before
BMT, the donor being her 17-year-old HLA-compatible sister.
The patient was successfully treated but, at the time, no procedure was available to preserve her fertility.
She became amenorrhoeic shortly after initiation of chemotherapy and radiotherapy. Six weeks later, concentrations of FSH were 108 mIU / ml, LH 54 mIU / ml and estradiol (E
2
)
, 10 pg / ml.
This ovarian failure profile was confirmed one month later and hormone replacement therapy was initiated. It was stopped in
August 2004. Thereafter, the patient remained norrhoeic. No ovarian activity was detected and bimonthly measurements of
FSH, LH and 17 b -E
2 confirmed complete ovarian failure (FSH
.
100 mIU / ml, LH .
50 mIU / ml and E
2
, 10 pg / ml).
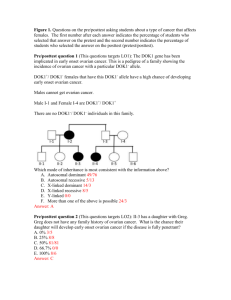
In July 2005, the patient (now aged 35 years) consulted us about the possibility of ovarian tissue transplantation from her sister. Oocyte donation with ICSI was proposed and discussed at this point, since the husband’s spermogram showed a low sperm count (5.8
10
6
/ ml spermatozoa) with poor motility (progressive motility ¼ 12%) and a low percentage of normal forms
(5% according to Kruger’s criteria). The patient’s sister, the donor
(now aged 32 years), was nulligravid. Having already provided bone marrow in 1990, she badly wanted to help her sister by donating some of her own ovarian cortex. She had been taking estroprogestogen contraceptive pills for .
10 years.
HLA group analysis revealed complete chimerism (HLA compatibility) between the two sisters, proving that no immunosuppressive treatment would be necessary, although the two sisters were genetically non-identical. Chimerism was confirmed by molecular biology using the short tandem repeat technique. Transplantation of organs like kidneys had already been performed between HLA-compatible sisters who had previously undergone BMT, with one sister acting as donor to the other.
Indeed, Hamawi et al . (2003) reported six cases of kidney transplantation after BMT, the kidney donor being the BMT donor in all cases. The patients did not receive immunosuppressive treatment and there was no sign of rejection. Hamawi et al . thus concluded that BMT recipients who receive a kidney from their bone marrow donor do not require immunosuppression.
In this case, the patient very much wanted to consider the option of using her sister’s ovarian tissue. After repeated discussions with the patient and her sister, and after having obtained their written informed consent, the decision to reimplant fresh ovarian tissue from sister to sister was taken. This was authorized by the Ethics Committee of the Catholic
University of Louvain which, back in 1995, had approved such research protocols, including reimplantation of ovarian tissue to preserve or restore fertility in women treated with high doses of chemotherapy, which could induce ovarian failure.
170
Surgery
Twenty days before surgery, the recipient patient was given an injection of GnRH agonist (Zoladex, AstraZeneca, Brussels,
Page 2 of 6
Belgium), and estroprogestogen therapy was started for a period of two months to decrease endogenous FSH levels, as previously suggested in case of reimplantation of cryopreserved ovarian tissue (Donnez et al ., 2006a). The donor had been taking estroprogestogens for .
2 years.
The operating rooms of the gynecology department are two communicating surgical suites (ORI, Storz, Tuttlingen,
Germany). The procedures were carried out as follows:
In February 2006, the patients were anaesthetized at the same time and laparoscopy was simultaneously performed on both patients. A 10-cm trocar was inserted into the umbilicus and three 5-mm trocars into the suprapubic area. At laparoscopy, the uterosacral ligaments of the donor showed perito-
175
180
185 neal endometriosis.
Then, both atrophic ovaries of the recipient (measuring
1.5
1 cm) were decorticated by laparoscopy, according to the same technique that Silber et al . (Silber et al ., 2005;
Silber and Gosden, 2007) applied during laparotomy for transplantation between monozygotic twins . (Fig. 1A and B). Since
190
Q5 the ovaries were atrophic, approximately two-third of the cortical tissue was removed in order to accommodate the graft, and sent for histological analysis.
When the ovaries of the recipient were ready to receive donor ovarian cortex, one large biopsy measuring 8 6 mm was taken from the right donor ovary (Fig. 2A and B) and immediately sutured laparoscopically to the recipient ovary using 7-0 Prolene (Ethicon, Johnson and Johnson, USA). A second biopsy measuring 6 4 mm was taken from the left ovary and also immediately sutured as before. Finally, a third biopsy measuring 6 4 mm was taken and once again
195
200
205
210
215
220
225
230
Figure 1: ( A ) Left ovary measuring 15 10 mm
( B ) Decorticated ovary. Approximately two-third of the cortical tissue was removed
Q6
235
240
245
250
255
Figure 2: ( A ) Right donor ovary
( B ) A large biopsy (8 6 mm) was taken from the right ovary, respecting the medulla and its vascularization. Note the absence of bleeding
Allograft of ovarian cortex immediately sutured to the recipient ovary. The fragments were thus sutured to the recipient ovarian medulla as soon as they were recovered. No medium or ice was used. The time interval between cortex removal and the start of suturing was , 1 min, and suture was achieved within 5 min of the fragment being excised. The edges of the cortical fragments were sutured to the decorticated edges, so that contact between the donor cortex and receiver medulla was optimal (Fig. 3A and B).
295
Biopsies were taken from both donor ovaries as we have previously found that this preoceedure carries no risk of mechan300 ical infertility as no adhesions are generated . A small biopsy Q7
(4 1 mm) was also taken from the donor ovary for histological analysis. The patients were discharged from hospital the day after surgery.
305
Ovarian biopsy
Serial sections of the recipient ovarian cortex did not show the presence of any follicles at all (Fig. 4A). Serial sections of the donor ovary revealed the presence of two primordial follicles and one primary follicle out of 11 serial sections (Fig. 4B).
310
Hormone levels (Fig. 5)
Before administration of GnRH agonist and estroprogestogens, the patient’s FSH value was 112.5 mIU / ml, LH 54 mIU / ml and 17 b -E
2
, 10 pg / ml. Three weeks after starting GnRH 315
260
320
265
325
270
330
275
335
280
340
285
290
Figure 3: ( A ) The donor cortical fragment was then sutured to the decorticated edges of the left recipient ovary
( B ) Right recipient ovary, where two donor cortical fragments were sutured
Figure 4: ( A ) Cortex of recipient ovary removed during surgery. No follicles are present (original magnification 50)
( B ) Biopsy of the donor ovary, showing one healthy primordial follicle
(original magnification 50)
345
Page 3 of 6
Donnez et al.
350
410
355
415
360
Figure 5: Sequential concentrations of FSH ( D ; mIU / ml) and 17 b -E
2
( S ; pg / ml)
A first peak in E
2 was observed after six months. A second peak was observed after seven months, followed by cycles with high E
2 levels, characterized by low FSH levels
Figure 6: Two follicles (10 mm in size) are visible by transvaginal ultrasonography on the day of oocyte retrieval
420
370
375
Q9
380
385
390
395
400
405 agonist (day of transplantation), FSH and LH levels were, respectively, 0.8 and 1 mIU / ml and remained very low for 8 weeks, as did 17 b -E
2
, before returning to castrated levels.
Six months after reimplantation, a first increase in E
2
(65 pg / ml) was observed, concomitant with follicular development (11 mm). FSH and LH levels were, respectively, 31.5 and
26.1 mIU / ml.
Seven months after reimplantation, a second peak in E
2 was observed, reaching 159 pg / ml , which was followed by menstrual bleeding. The patient then experienced menstrual cycles characterized by E
2 peaks of .
200 pg / ml, follicular size between 18 and 21 mm and a thickened endometrium
(between 8 and 10 mm). From 9 to 11 months after reimplantation, FSH and LH values decreased to 15.2 and 4.9 mIU / ml, concomitant with an E
2 concentration of 292 pg / ml and a progesterone level of 4.3 ng / ml. Cycle length was between
30 and 48 days.
Since ICSI was required because of sperm quality, it was decided to optimize follicular development when follicles reached 12 – 13 mm by administering 150 mIU of recombinant
FSH (Serono, Geneva, Switzerland) for a period of 5 days.
Twelve months after reimplantation, when follicular size reached 15 mm, 0.25 mg GnRH antagonist (Cetrorelix, Serono,
Geneva, Switzerland) was added daily. When follicular size reached 18 – 20 mm, 5000 mIU hCG (Pregnyl, Organon, Oss, the Netherlands) was given and follicle aspiration was performed 35 h later.
On day 10, the E
2 level was 262 pg / ml. By day 13 (day of hCG administration), it had risen to 497 pg / ml. Transvaginal ultrasonography demonstrated the presence of two follicles of
20 mm, which were punctured (Fig. 6). Two mature oocytes with a large cumulus were retrieved (Fig. 7A and B).
The occytes were fertilized with the husband’s sperm by ICSI. At 24 h post-fertilization, a two-cell embryo was observed (Fig. 8). At 36 and 48 h post-fertilization, no further cleavage was observed in the 2-cell embryo. The other oocyte developed up to the 3-cell stage and then its development ceased. No embryos were transferred to the uterus because of this developmental arrest.
Page 4 of 6
The patient experienced two more cycles. During the second one, the previously described stimulation protocol was applied, but no oocyte was retrieved from the aspirated follicle.
425
Discussion
430
In 2005, Silber published a report on successful ovarian transplantation between monozygotic twins (Silber et al ., 2005), and the series has recently been extended (Silber and Gosden,
2007). We report a case of ovarian transplantation between two genetically non-identical sisters.
The recipient patient experienced iatrogenic POF due to chemotherapy and TBI. It is particularly important to stress that the recipient had also received bone marrow from that same sister. HLA group analysis revealed complete chimerism
(HLA compatibility) between the two sisters.
Oocyte donation was thoroughly discussed with the patient, who refused this option. However, we are of the firm opinion that the ovarian tissue allotransplantation was ethically acceptable. First, the donor needed to undergo a laparoscopy for suspected endometriosis because of dysmenorrhoea and pelvic pain. Second, the recipient refused oocyte donation and specifically requested a graft. Third, her sister expressly asked to be the tissue donor and refused to undergo ovarian stimulation for oocyte donation. Fourth, the ovarian tissue transplantation was carried out by laparoscopy, known as minimally invasive surgery. It should be pointed out that the recipient presented with documented POF, her ovaries were atrophic and serial sections failed to demonstrate the presence of any follicles.
Indeed, POF was confirmed by very high FSH and LH levels, very low E
2 concentrations and the absence of any follicles in large biopsies removed from the patient’s atrophic ovaries during transplantation.
Several options now exist to preserve fertility in women who need to undergo aggressive chemotherapy, allowing them to become mothers when they have overcome their disease: embryo cryopreservation, oocyte cryopreservation and ovarian tissue cryopreservation (for review, see Donnez et al .,
2006a,b). Unfortunately, when this patient was treated in
1990, none of these options could be proposed.
435
440
445
450
455
460
Allograft of ovarian cortex
465
525
470
530
475
535
480
485
490
495
500
505
510
515
520
Figure 8: Two-cell embryo 36 h after ICSI
Figure 7: ( A ) First mature oocyte cumulus oophorus (top)
Same oocyte prepared for ICSI procedure (bottom). ( B ) Second mature oocyte (top). Same oocyte prepared for ICSI procedure
(bottom). The polar body is clearly visible in both oocytes
540
Successful fertilization and pregnancy culminating in a live birth has been achieved after oocyte collection from fresh transplanted ovarian tissue in a primate (Lee et al ., 2004), and Silber et al . (Silber et al ., 2005; Silber and Gosden,
2007) have reported successful orthotopic transplantation of fresh ovarian cortex between monozygotic twin sisters, one of whom was suffering from POF. In both cases, the grafted tissue functioned without any surgical connection to major blood vessels.
Survival of primordial follicles has also been histologically proved in humans after orthotopic grafting of fresh ovarian cortex (Donnez et al ., 2005), but follicular density was found to have decreased due to the fall in number of primordial follicles.
In the case we describe, vaginal echography and 17 b -E
2 levels revealed a follicular structure six months after transplantation. The appearance of the first follicle in the grafted tissue six months after reimplantation is totally consistent with the development of primordial follicles. According to Gougeon
(1996), follicles at early growth stages need .
85 days to reach the antral stage. Primordial follicles therefore obviously need even more. The time interval seen in the present case between implantation of cortical tissue and follicular development is consistent with data on frozen ovarian cortex implantation in both sheep and humans, but longer than that observed in humans by Silber et al . (2005), who reported the first rise in E
2
71 days after implantation. In his recently published series, the time to first menses after transplantation was found to vary between 65 and 93 days (Silber and
Gosden, 2007).
FSH values remained above 40 mIU / ml during the first cycles in our case. We twice observed an FSH surge between the first cycles. It was probably associated with slower follicular growth from a depleted follicular reserve due to the loss of primordial follicles that occurs before the graft is completely revascularized. It could also be that the ovarian reserve of the donor, aged 33 years, was relatively low, either due to her age or to endometriosis, since some women with endometriosis show a reduced ovarian follicular reserve (Donnez et al ., 1996;
D’Hooghe and Hummelshoj, 2006). However, even if the
545
550
555
560
565
570
575
580
Page 5 of 6
585
590
595
600
605
610
615
620
Donnez et al.
ovarian reserve of the donor was not optimal in the analysed biopsy (two primordial follicles and one primary follicle out of 11 sections), it does not preclude a normal follicular reserve in other ovarian areas, since we know that a small fragment may not be truly representative, and that primary ovarian follicles are located in clusters in the ovary (Qu et al ., 2000;
Gook et al ., 2003; Schmidt et al ., 2005).
From 11 months after reimplantation to date, E
2 levels have remained high, concomitant with follicular development and low FSH and LH concentrations. The fact that serial sections of two-third of the recipient patient’s cortex failed to demonstrate the presence of any primordial follicles supports the notion that the origin of steroid secretion was indeed the transplanted tissue. It is extremely unlikely that restoration of ovarian function in this woman, who had received two alkylating agents and TBI (750 cGy) before BMT, was due to residual follicles in the atrophic native ovary, from which the majority of the cortex was removed.
The ovary is a good location for transplantation, allowing revascularization from the medulla after decortication. This technique was previously applied for transplantation of cryopreserved tissue and proved highly effective (Donnez et al .,
2004, 2006a,b), constituting a strong argument in favour of leaving at least one ovary in place, even if the risk of POF after treatment is practically 100%. Silber et al . (Silber et al .,
2005; Silber and Gosden, 2007) also considered the ovarian medulla to be an excellent site for fresh ovarian cortex transplantation.
Our findings offer hope to young patients facing POF, who have not had the chance to cryopreserve their oocytes, embryos or ovarian cortex. As stressed by Silber and Gosden, these promising results should encourage continued efforts to preserve fertility in patients having to undergo chemotherapy and / or radiotherapy.
Acknowledgements
The present study was supported by grants from the Fonds National de la Recherche Scientifique N 8 7.4519.06, the Fondation St. Luc, the
Belgian Federation Against Cancer (non-profit organization), Baron
Albert Fre`re and Comte de Spoelberch.
References
625
630
635
Demeestere I, Simon P, Buxant F, Robin V, Fernandez-Aguilar S, Centner J,
Delbaere A, Englert Y. Ovarian function and spontaneous pregnancy after combined hetorotopic and orthotopic cryopreserved ovarian tissue transplantation in a patient previously treated with bone marrow transplantation: case report.
Hum Reprod 2006; 21 :2010 – 2014.
D’Hooghe T, Hummelshoj L. Multi-disciplinary centres / networks of excellence for endometriosis management and research: a proposal.
Hum
Reprod 2006; 21 :2743 – 2748.
Donnez J, Nisolle M, Gillet N, Smets M, Bassil S, Casanas-Roux F. Large ovarian endometriomas.
Hum Reprod 1996; 11 :614 – 646.
Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J,
Martinez-Madrid B, Van Langendonckt A. Livebirth after orthotopic transplantation of cryopreserved ovarian tissue.
Lancet 2004; 364 :
1405 – 1410.
Donnez J, Squifflet J, Dolmans MM, Martinez-Madrid B, Jadoul P, Van
Langendonckt A. Orthotopic transplantation of fresh ovarian cortex: a report of two cases.
Fertil Steril 2005; 84 :1018.
Donnez J, Martinez-Madrid B, Jadoul P, Van Langendonckt A, Demylle D,
Dolmans MM. Ovarian tissue cryopreservation and transplantation: a review.
Hum Reprod Update 2006a; 12 :519– 535.
Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirad C, Squifflet J,
Martinez-Madrid B, Van Langendonckt A. Restoration of ovarian function after orthotopic (intraovarian and periovarian) transplantation of cryopreserved ovarian tissue in a woman treated by bone marrow transplantation for sickle cell anaemia: case report.
Hum Reprod
2006b; 21 :183– 188.
Gook DA, Edgar DH, Borg J, Archer J, Lutjen PJ, McBain JC. Oocyte maturation, follicle rupture and luteinization in human cryopreserved ovarian tissue following xenografting.
Hum Reprod 2003; 18 :
1772 – 1781.
Gougeon A. Regulation of ovarian follicular development in primates: facts and hypotheses.
Endocr Rev 1996; 17 :121 – 155.
Hamawi K, De Magalhaes-Silverman M, Bertolatus JA. Outcomes of renal transplantation following bone marrow transplantation.
Am J Transplant
2003; 2 :301 – 305.
Larsen EC, Muller J, Schmiegelow K, Rechnitzer C, Andersen AN. Reduced ovarian function in long-term survivors of radiation- and chemotherapytreated childhood cancer.
J Clin Endocrinol Metab 2003; 88 :5307 – 5314.
Lee DM, Yeoman RR, Battaglia DE, Stouffer RL, Zelinski-Wooten B, Fanton
JW, Wolf DP. Live birth after ovarian tissue transplant.
Nature
2004; 428 :137– 138.
Lutchman Singh K, Davies M, Chatterjee R. Fertility in female cancer survivors: pathophysiology, preservation and the role of ovarian reserve testing.
Hum Reprod Update 2005; 11 :69 – 89.
Meirow D, Nugent D. The effects of radiotherapy and chemotherapy on female reproduction.
Hum Reprod Update 2001; 7 :534 – 543.
Meirow D, Levron J, Eldar-Geva T, Hardan I, Fridman E, Zalel Y, Schiff E,
Dor J. Pregnancy after transplantation of cryopreserved ovarian tissue in a patient with ovarian failure after chemotherapy.
N Engl J Med
2005; 353 :318– 321.
Meirow D, Levron J, Eldar-Geva T, Hardan I, Fridman E, Yemini Z, Dor J.
Monitoring the ovaries after autotransplantation of cryopreserved ovarian tissue: endocrine studies, in vitro fertilization cycles, and live birth.
Fertil
Steril 2007; 87 :418.e7 – 418.e15.
Qu J, Godin PA, Nisolle M, Donnez J. Distribution and epidermal growth factor receptor expression of primordial follicles in human ovarian tissue before and after cryopreservation.
Hum Reprod 2000; 15 :302 – 310.
Salooja N, Szydlo RM, Socie G, Rio B, Chatterjee R, Ljungman P, Van Lint
MT, Powles R, Jackson G, Hinterberger-Fischer M et al , for the Late
Effects Working Party of the European Group for Blood, Marrow
Transplantation. Pregnancy outcomes after peripheral blood or bone marrow transplantation: a retrospective survey.
Lancet 2001; 358 :271– 276.
Sanders J, Hawley J, Levy W, Gooley T, Buckner CD, Deeg HJ, Doney K,
Storb R, Sullivan K, Witherspoon R et al.
Pregnancies following high-dose cyclophosphamide with or without high-dose busulfan or total body irradiation and bone marrow transplantation.
Blood 1996; 87 :
3045 – 3052.
Schmidt KL, Yding Andersen C, Loft A, Byskov AG, Ernst E, Nyboe Andersen
A. Follow-up of ovarian function post-chemotherapy following ovarian cryopreservation and transplantation.
Hum Reprod 2005; 20 :3539 – 3546.
Silber SJ, Lenahan KM, Levine DJ, Pineda JA, Gorman KS, Friez MJ,
Crawford EC, Gosden RJ. Ovarian transplantation between monozygotic twins discordant for premature ovarian failure.
N Engl J Med 2005;
353 :58 – 63.
Silber SJ, Gosden RG. Ovarian transplantation in a series of monozygotic twins discordant for ovarian failure.
N Engl J Med 2007; 356 :1382 – 1384.
Teinturier C, Hartmann O, Valteau-Couanet D, Benhamou E, Bougneres PF.
Ovarian function after autologous bone marrow transplantation in childhood: high-dose busulfan is a major cause of ovarian failure.
Bone
Marrow Transplant 1998; 22 :989 – 994.
Wallace WH, Anderson RA, Irvine DS. Fertility preservation for young patients with cancer: who is at risk and what can be offered?
Lancet Oncol 2005; 6 :209 – 218.
640
645
650
655
660
665
670
675
680
685
690
Submitted on May 2, 2007; resubmitted on June 11, 2007; accepted on June 14,
2007
695
Page 6 of 6