1 Tier 2 MSK Clinic GP Message of the Month August 2014 PART I
advertisement

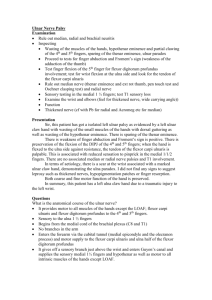
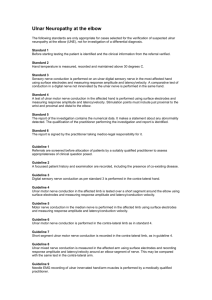
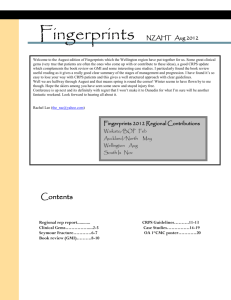
Tier 2 MSK Clinic GP Message of the Month August 2014 PART I Wasting of the hand muscles. This month’s MoM presents a clinical case study to test your knowledge! A 30-year-old Spanish gentleman presented to the MSK Tier 2 clinic in July 2014, complaining of weakness in the hand, and a ‘thinning’ of the muscle bulk between his thumb and index finger (Fig. 1), and ‘curling up’ (clawing) of the little and ring fingers (Fig. 2). He said that he started to experience pain and ‘tingling’ in the left arm/hand some months ago but that the aforementioned hand problems had progressed rapidly, over a period of a few weeks. He could recall no history of trauma and was otherwise in good health (apart from ulcerative colitis). WHAT DO YOU THINK COULD BE GOING ON HERE? Fig. 1 Atrophy of the first dorsal interosseous muscle (from Wang et al, 2014) Fig. 2 Claw hand deformity 1 Part II EMG studies performed 2 weeks ago in Spain had shown a left ulnar mononeuropathy affecting the deep palmar branch of the ulnar nerve with severe axonal involvement (axonotmesis) i.e. the ulnar nerve was severely compressed at the level of the wrist/palm. Key notes for general practice Differential diagnosis of ulnar neuropathy at wrist or palm: -­‐ Motor neurone disease should always be considered where there is a pure motor ulnar neuropathy -­‐ Syringomyelia -­‐ Lesions of lower brachial plexus (T1 root, especially) e.g. cervical rib, lung pathology -­‐ Cervical radiculopathy -­‐ Spondylitic myelopathy Possible causes of ulnar nerve lesion at wrist or palm: -­‐ External pressure e.g. occupation, cyclists’ palsy, use of crutches, handcuffs -­‐ Hereditary liability to pressure palsies -­‐ Post injury e.g. # -­‐ Acquired lesions in wrist/palm e.g. ganglion, giant cell tumour, ulnar artery pathology, chondroblastoma of hamate, local calcifications or arthritis, lipoma etc. -­‐ Congenital problems e.g. anomalous course of ulnar nerve, muscle abnormalities, tortuosity of ulnar artery, fusion between hamate and pisiform -­‐ Infections e.g. leprosy Clinical pearl I: In the presentation of the clawed hand, the ‘ulnar paradox’ refers to the fact that a high ulnar nerve lesion (at the level of the elbow) produces, paradoxically, a less marked deformity than a low lesion (at the level of wrist). This is because in a low lesion the long flexors (supplied by the ulnar nerve just below the elbow) are unaffected. See link below for further information http://teachmeanatomy.info/upper-limb/nerves/ulnar-claw-vs-hand-of-benediction/ 2 Clinical pearl II: The clawed hand seen with an ulnar nerve lesion and the Benedictine hand (Fig. 3) produced with a median nerve lesion can look similar. However, the Benedictine hand is only apparent when the patient is asked to make a first (due to the inability to flex the first and second fingers at the PIP joint). Fig. 3 Hand of Benediction (Pope’s hand) from Standford University website References Wang, B. et al. (2014) Ulnar nerve deep branch compression by a ganglion: A review of nine cases. Injury, Jul;45(7):1126-30. Resources The following two websites might be of interest: - The Hand in Diagnosis http://stanfordmedicine25.stanford.edu/the25/hand.html - Teach Me Anatomy http://teachmeanatomy.info/upper-limb/nerves/ulnarclaw-vs-hand-of-benediction/ Authors Dr Janet Suckley: Consultant Physiotherapist & Registered Osteopath, Tier 2 MSK Clinic, Longsight Health Centre (0161 248 1214/1255). Dr Bharat Nanavati: General Practitioner, Ailsa Craig GP Practice, and GPwSI in MSK medicine. Please forward any comments/queries to janet.suckley@cmft.nhs.uk Next month’s MOM: inflammatory back pain 3