Theories of Blood Coagulation - Association of Pediatric
advertisement

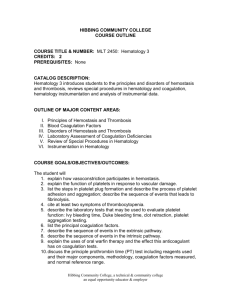
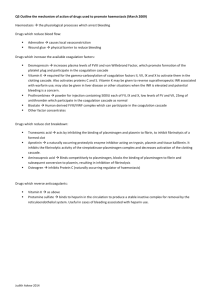
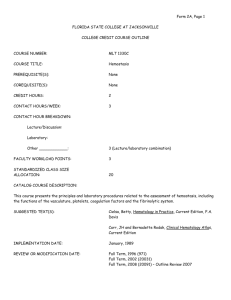
Theories of Blood Coagulation James P. Riddel Jr, MS, RN, CPNP Bradley E. Aouizerat, PhD Christine Miaskowski, RN, PhD David P. Lillicrap, MD, FRCPC Although the concept of the coagulation cascade represented a significant advance in the understanding of coagulation and served for many years as a useful model, more recent clinical and experimental observations demonstrate that the cascade/waterfall hypothesis does not fully and completely reflect the events of hemostasis in vivo. The goal of this article is to review the evolution of the theories of coagulation and their proposed models to serve as a tool when reviewing the research and practice literature that was published in the context of these different theories over time. Key words: coagulation, coagulation cascade, cellbased theory of coagulation, bleeding disorders H emostatic mechanisms have evolved to protect against the threat of fatal hemorrhage. The interaction between platelets and clotting factors results in the generation of a protective hemostatic plug, whose function is to staunch the flow of blood at the site of vascular injury. To balance this, the fibrinolytic system has evolved to recanalize occluded vessels as healing occurs to restore perfusion through an injured vessel in which the protective clot has formed. Despite the existence of many fail-safe mechanisms designed to regulate hemostasis, a variety of disorders exist that are associated either with a hemorrhagic or a prothrombotic diathesis (Loscalzo, 2003). © 2007 by Association of Pediatric Hematology/Oncology Nurses DOI: 10.1177/1043454206298693 The purpose of this article is to describe the changes that have occurred in the understanding of physiologic processes involved in hemostasis. Overview of Hemostasis Hemostasis is a dynamic process whereby blood coagulation is initiated and terminated in a rapid and tightly regulated fashion (Nathan, Orkin, Ginsburg, & Look, 2003). Blood coagulation (the cessation of blood loss from a damaged vessel) is part of an important host defense mechanism. Upon vessel injury, platelets adhere to macromolecules in subendothelial tissues at the site of injury and then aggregate to form the primary hemostatic plug. Platelets stimulate the local activation of plasma coagulation factors, which leads to the generation of a fibrin clot that reinforces the platelet aggregate. Later, as wound healing occurs, the platelet aggregate and fibrin clot are broken down and removed. Hemostasis is regulated by 3 basic components— namely, the vascular wall, platelets, and the coagulation James P. Riddel Jr, MS, RN, CPNP, is a pediatric nurse practitioner and doctoral student in the Division of Hematology at Children’s Hospital and Research Center Oakland, Oakland, California. Bradley E. Aouizerat, PhD, is a basic scientist and professor of genetics in the Department of Physiological Nursing & Institute for Human Genetics at the University of California, San Francisco. Christine Miaskowski, PhD, RN, is a nurse scientist and professor of nursing in the Department of Physiological Nursing at the University of California, San Francisco. David P. Lillicrap, MD, FRCPC, is a hematologist and professor in the Department of Pathology & Molecular Medicine at Queen’s University, Kingston, Ontario, Canada. Address for correspondence: James P. Riddel Jr, MS, RN, CPNP, Division of Hematology, Children’s Hospital and Research Center Oakland, 747 52nd Street, Oakland, CA 94609-1809; e-mail: jriddel@mail.cho.org. Journal of Pediatric Oncology Nursing, Vol 24, No 3 (May-June), 2007: pp 123-131 123 Riddel et al Thrombokinase* Calcium Prothrombin Thrombin Fibrinogen Fibrin Figure 1. Classic Theory of Coagulation as Proposed by Paul Morawitz, in Which the Prothrombin, by Calcium Activation, Yielded Thrombin, Converting Fibrinogen to Fibrin cascade. Normal hemostasis occurs as the result of a set of regulated processes to accomplish 2 functions; first, it maintains blood in a fluid, clot-free state, and second, it induces a rapid and localized hemostatic plug at the site of vascular injury (Kumar, Abbas, & Faousto, 2005). Blood coagulation occurs when the enzyme thrombin is generated that proteolyzes soluble plasma fibrinogen, forming the insoluble fibrin polymer or clot. Mechanisms that restrict the formation of platelet aggregates and fibrin clots to sites of injury are necessary to maintain the fluidity of the blood (Hoffbrand, Catovsky, & Tuddenham, 2005). Historical Sketch Hippocrates, Aristotle, Celsius, and Galen were fully aware of the fact that freshly drawn blood usually clots within minutes. They described in detail various internal and superficial bleeding tendencies. A common observation was that blood congealed on cooling. It was thought that by leaving a wound in contact with air, the blood cooled, stopping the hemorrhage. However, they did not associate blood coagulability with a concept of hemostasis (Nichols & Bowie, 2001). Two thousand years later in the early 1720s, French surgeon Jean-Louis Petit noted that hemostasis after amputation of a limb was caused by clots forming in the blood vessels. This observation was the first time blood clotting was related to hemostasis. In 1828, Swiss physician Friedrich Hopff (Nichols & Bowie, 2001) noted that the well-known familial bleeding tendency in males was associated with pronounced hypocoagulability, now recognized as hemophilia, an X chromosome–linked disorder. Therefore, coagulability was essential to prevent bleeding. This recognition of abnormal coagulation and its association with bleeding led to a rapid increase in research into the 124 phenomenon of blood coagulation. During the 19th century, German pathologist Rudolf Virchow in 1860 (Nichols & Bowie, 2001) described thrombi (blood clots) and their tendency to embolize. Platelets were discovered, and their function was established, along with discovery of the various components of the coagulation process. These advances led to the classic theory of coagulation described by Paul Morawitz in 1905 (Morawitz, 1958). He convincingly assembled 4 “coagulation factors” in his scheme of coagulation (Figure 1). In the presence of calcium and thromboplastin, prothrombin was believed to be converted to thrombin. In turn, the thrombin converted fibrinogen to fibrin, enabling the formation of a fibrin clot. Morawitz posited that all the ingredients of clotting were present in circulating blood and that the fact that such blood did not normally clot was due to the lack of a wettable surface in the blood vessels. This classic theory persisted for 40 years. The Coagulation/Waterfall Cascade The modern understanding of the biochemical processes of coagulation began in the 1940s, when Paul Owren (1947) recognized that a bleeding diathesis in a young woman could not be explained by the 4-factor concept, positing that she lacked a fifth coagulation factor in her plasma. Throughout the 1940s and 1950s, several more coagulation factors were discovered. Coagulation factors were designated by roman numerals. Importantly, the numeric system that was adopted assigned the number to the factor according to the sequence of discovery and not to the point of interaction in the cascade. By 1957, the following factors were described: von Willebrand factor (VWF) (von Willebrand, 1931), factor (F) V (Owren, 1947), FVII (Alexander, Goldstein, Landwehr, & Cook, 1951), FVIII (Patek & Stetson, 1936), FIX (Aggeler et al., 1952; Briggs et al., 1952; Shulman & Smith, 1952), and FXI (Rosenthal, Dreskinoff, & Rosenthal, 1953). Two groups described FX deficiency (Hougie, Barrow, & Graham, 1957; Telfer, Denson, & Wright, 1956). However, what was not clear was how these multiple factors interacted to convert prothrombin to thrombin, resulting in the formation of a fibrin clot. The development of this knowledge proved to be an essential contribution to the understanding of the blood coagulation mechanism (Roberts, 2003). Journal of Pediatric Oncology Nursing 24(3); 2007 Theories of Blood Coagulation In the 1960s, 2 independent groups of biochemists introduced a model of coagulation as a series of steps in which activation of each clotting factor led to the activation of another, culminating in a burst of thrombin generation. The article proposing the cascade model by Macfarlane (1964) appeared in the journal Nature and was shortly followed by the waterfall model reported by Davie and Ratnoff (1964) in the journal Science. This model (Figure 2) described each clotting factor as a proenzyme that could be converted to an active enzyme. The “cascade” and “waterfall” models suggested that the clotting sequences were divided into 2 pathways. Coagulation could be initiated via an “intrinsic pathway,” so named because all the components were present in blood, or by an “extrinsic pathway,” in which the subendothelial cell membrane protein, tissue factor (TF), was required in addition to circulating components. The initiation of either pathway resulted in activation of FX and the eventual generation of a fibrin clot through a common pathway (Luchtman-Jones & Broze, 1995). FIXa and 2 downstream products of the cascade, FXa and thrombin, proteolytically cleave FVIII, forming FVIIIa, a cofactor in the next reaction. Finally, FIXa and FVIIIa together with Ca2+ (which may come largely from activated platelets) and negatively charged phospholipids (the major constituents of cell membranes) form a trimolecular complex termed tenase. Tenase then converts FX to FXa, yet another protease (Boron & Boulpaep, 2005). In a parallel series of interactions, FXa binds to the cofactor FVa, itself a downstream factor that participates in positive feedback with the present reaction to generate a complex with enzymatic activity known as prothombinase. This complex converts the proenzyme prothrombin to its enzyme form, thrombin. Thrombin acts on fibrinogen to generate the fibrin monomer, which rapidly polymerizes to form the fibrin clot. During clinical laboratory analysis of blood clotting, the intrinsic pathway of blood coagulation is evaluated using the activated partial thromboplastin time (PTT) (R. Hoffman et al., 2005). Extrinsic Pathway Intrinsic Pathway The intrinsic pathway consists of a cascade of protease reactions initiated by factors that are present within the blood. When in contact with a negatively charged surface such as glass or the membrane of an activated platelet, a plasma protein called FXII (Hageman factor) becomes FXIIa (the suffix “a” indicates that this is the activated form of FXII). A molecule called high molecular weight kininogen (HMWK), a product of platelets that may in fact be attached to the platelet membrane, helps anchor FXII to the charged surface and thus serves as a cofactor. However, this HMWK-assisted conversion of FXII to FXIIa is limited in speed. Once a small amount of FXIIa accumulates, this protease converts prekallikrein to kallikrein, with HMWK as an anchor. In turn, the newly produced kallikrein accelerates the conversion of FXII to FXIIa, an example of positive feedback. In addition to amplifying its own generation by forming kallikrein, FXIIa (together with HMWK) proteolytically cleaves FXI, forming FXIa. In turn, FXIa (also bound to the charged surface by HMWK) proteolytically cleaves FIX to FIXa, which is also a protease. Journal of Pediatric Oncology Nursing 24(3); 2007 The extrinsic pathway also includes protein cofactors and enzymes. This pathway is initiated by the formation of a complex between TF on cell surfaces and FVIIa that is located outside the vascular system. Nonvascular cells constitutively express the integral membrane protein TF (variably known as FIII or tissue thromboplastin), which is a receptor for the plasma protein FVII (Kumar et al., 2005). When an injury to the endothelium allows FVII to come into contact with TF, the TF nonproteolytically activates FVII to FVIIa. The mechanism of the initial conversion of the zymogen FVII to FVIIa is still debated but is most likely due to autocatalytic activation and not a TF effect (M. Hoffman & Monroe, 2005). This binding of FVIIa to TF forms an enzyme complex that activates FX to FXa. The FVIIa/TF complex, similar in function to the tenase complex, converts FX to its active form (FXa), which binds to the cofactor FV and is bound on membrane surfaces in the presence of calcium ions to generate the prothrombinase complex. The prothrombinase complex converts prothrombin to thrombin, which converts fibrinogen to fibrin to generate the fibrin clot. During laboratory analysis of blood clotting, the extrinsic pathway of blood coagulation is 125 Riddel et al Figure 2. The Coagulation Cascade Model The point of integration between the intrinsic and extrinsic pathways in this model occurs with factor IX activation. HMWK, high molecular weight kininogen. 126 Journal of Pediatric Oncology Nursing 24(3); 2007 Theories of Blood Coagulation evaluated using the prothombin time (PT) (R. Hoffman et al., 2005). Regardless of whether FXa arises by the intrinsic or extrinsic pathway, the cascade then proceeds along the common pathway. complex of FVIIa and TF activated not only FX but also FIX. More recent observations have led to the conclusion that activity of the FVIIa/TF complex is the major initiating event in hemostasis in vivo (M. Hoffman & Monroe, 2005). Common Pathway The common pathway begins with the activation of FX within the intrinsic pathway, the extrinsic pathway, or both. FXa from either the intrinsic or extrinsic pathway is the first protease of the common pathway. FXa, in the presence of FV, Ca2+, and phospholipids, converts prothrombin to its active form, thrombin (Harmening, 2002). The main action of thrombin is to catalyze the proteolysis of the soluble plasma protein fibrinogen to form fibrin monomers that remain soluble. Fibrin monomers then polymerize to form a gel of fibrin polymers that trap blood cells. Thrombin also activates FXIII, which is converted to FXIIIa and mediates the covalent cross-linking of the fibrin polymers to form a mesh termed stable fibrin, which is less soluble than fibrin polymers (Boron & Boulpaep, 2005). Thrombin can catalyze the formation of new thrombin from prothrombin and can catalyze the formation of the cofactors FVa and FVIIIa, resulting in efficient amplification of coagulation. Because the common pathway contains the factors FX, FV, and FII (any deficiency in which may lead to a hemorrhagic disorder), these factors may be monitored by both the PT and the PTT (Harmening, 2002). Although these concepts represented a significant advance in the understanding of coagulation and served for many years as a useful model, more recent clinical and experimental observations demonstrate that the cascade/waterfall hypothesis does not fully and completely reflect the events of hemostasis in vivo (M. Hoffman & Monroe, 2001). In recent years, deficiencies of this scheme have become apparent. First, no explanation existed for the absence of a clinical bleeding tendency in deficiencies of FXII, prekallikrein, or high molecular weight kininogen, even though deficiencies in any one of these factors markedly prolong surface-activated coagulation assays for hemostasis in vitro. Second, no explanation existed for why FVIII or FIX deficiency caused clinically severe bleeding, even though the extrinsic pathway would be expected to bypass the need for FVIII and FIX (Hoffbrand et al., 2005). These key observations led to a revision of earlier models of coagulation. A vital observation was that a Journal of Pediatric Oncology Nursing 24(3); 2007 Cell-Based Model of Coagulation A major development over the past 15 years was the discovery that exposure of blood to cells that express TF on their surface is both necessary and sufficient to initiate blood coagulation in vivo. This finding led to the belief that the intrinsic pathway (the contact system) does not have a true physiological role in hemostasis (Hoffbrand et al., 2005). Very recent evidence suggests that although FXII deficiency does not result in bleeding problems, the absence of FXII does protect against pathological thrombosis (Kleinschnitz et al., 2006). This hypothesis and the experimental evidence to support it were collected by several investigators and presented in a series of articles authored by a group from the Department of Pathology at Duke University and the University of North Carolina (G. A. Allen, Monroe, Roberts, & Hoffman, 2000; M. Hoffman & Monroe, 2001; M. Hoffman, Monroe, & Roberts, 1996; Kjalke, Monroe, Hoffman, Oliver, & Ezban, 1998; Kjalke, Monroe, Hoffman, Oliver, Ezban, et al., 1998; Monroe, Hoffman, & Roberts, 1996). In the cell-based model, hemostasis requires the formation of an impermeable platelet and fibrin plug at the site of vessel injury, but it also requires that the procoagulant substances activated in this process remain localized to the site of injury. The process of blood coagulation is initiated by the exposure of cells expressing TF to flowing blood. Tissue factor is expressed constitutively on cells such as smooth muscle cells and fibroblasts but not on resting endothelium. Tissue factor is present in the membranes of cells surrounding the vascular bed but is normally not in contact with blood (Dahback, 2005). It is exposed to the circulating blood by disruption of the endothelium or by activation of endothelial cells or monocytes (O’Shaughnessy, Makris, & Lillicrap, 2005). Mounting evidence suggests that TF is present in blood on cellular microparticles. These membrane fragments derive from various cell types: white blood cells, endothelium, and platelets, which may play a more important role in pathological hemostasis (thrombosis) as opposed to normal clotting (Osterud & Bjorklid, 2006). 127 Riddel et al Table 1. Summary of the 4 Phases of Coagulation, as Proposed by the Current Cell-Based Theory of Coagulation Process Stages in Hemostasis Initiation Vascular endothelium and circulating blood cells are perturbed; interaction of plasma-derived FVIIa with tissue factor Amplification Propagation Termination Thrombin activates platelets, cofactors FVa and FVIII on the platelet surface, and FXI on the platelet surface Results in the production of a significant level of thrombin activity, generation of a stable plug at the site of injury, and cessation of blood loss Clotting process is limited to avoid thrombotic occlusion in surrounding normal areas of the vasculature It is best to consider the highly interwoven array of physical, cellular, and biochemical processes that contribute to hemostasis as a series of process stages (phases) rather than pathways. The phases of initiation, propagation, and termination illustrate the intricate processes involved in the maintenance of vascular integrity (Loscalzo, 2003). The 4 phases of coagulation comprising the current cell-based theory of coagulation are summarized in Table 1. Initiation Phase The initiation phase is localized to the cells that express TF, which are found normally outside the vasculature. The FVIIa/TF complex activates small amounts of FIX and FX. FXa associates with its cofactor, FVa, and forms a prothrombinase complex on the surface of the TF-bearing cell (M. Hoffman, 2004; Monroe et al., 1996). FV can be activated by FXa (Monkovic & Tracy, 1990) or by noncoagulation proteases (D. H. Allen & Tracy, 1995) to produce the FVa required for prothrombinase assembly (M. Hoffman, 2004; Loscalzo, 2003). Low-level activity of the TF pathway occurs at all times within the extravascular space. Coagulation proteins percolate through tissues, leaving the vasculature, and are found in the lymph roughly in proportion to their molecular size (Le, Borgs, Toneff, Witte, & Rapaport, 1998). It is likely that FVII is bound to extravascular TF even in the absence of an injury (M. Hoffman, 2004), and the extravascular FX and FIX can be activated as they pass through the tissues. The coagulation process proceeds to the amplification phase only when damage to the vasculature allows platelets and FVIII (bound to VWF) to spill out into the extravascular tissues and to adhere to TF-bearing cells at the site of injury. Extrinsic is an appropriate name for the TF pathway because it can be thought of as operating outside the vasculature (M. Hoffman, 2004; Loscalzo, 2003). 128 Amplification Phase A small amount of thrombin generated on the TFbearing cell has several important functions. A major function is the activation of platelets, exposing receptors and binding sites for activated clotting factors. As a result of this activation, the platelets release partially activated forms of FV onto their surfaces. Another function of the thrombin formed during the initiation phase is the activation of the cofactors FV and FVIII on the activated platelet surface. In this process, the FVIII/VWF complex is dissociated, permitting VWF to mediate additional platelet adhesion and aggregation at the site of injury. In addition, small amounts of thrombin activate FXI and FXIa on the platelet surface during this phase (Loscalzo, 2003; Oliver, Monroe, Roberts, & Hoffman, 1999). Propagation Phase As large numbers of platelets are recruited to the site of injury, the propagation phase of clot formation occurs on the surface of activated platelets. First, FIXa activated during the initiation phase can now bind to FVIIIa on the platelet surface. Second, additional FIXa can be supplied by platelet-bound FXIa. Third, because FXa cannot move effectively from the TF-bearing cell to the activated platelet, FXa must be provided directly on the platelet surface by the FIXa/FVIIIa complex. Fourth, the FXa rapidly associates with FVa bound to the platelet during the amplification phase. Finally, the completion of this platelet prothrombinase assembly leads to a burst of thrombin generation of sufficient magnitude to clot fibrinogen (Dahback, 2005; M. Hoffman, 2004; Loscalzo, 2003). Journal of Pediatric Oncology Nursing 24(3); 2007 Theories of Blood Coagulation Termination Phase Once a fibrin platelet clot is formed over an area of injury, the clotting process must be limited to avoid thrombotic occlusion in surrounding normal areas of the vasculature. Unless controlled, clotting could propagate throughout the entire vascular tree (M. Hoffman, 2004). Three types of natural anticoagulants regulate clotting: antithrombin (ATIII) inhibits the activity of thrombin and other serine proteases, such as FIXa, FXa, FXIa, and FXIIa. Binding to heparin-like molecules on endothelial cells activates antithrombin. Proteins C and S are characterized by their ability to inactivate the procoagulant cofactors FVa and FVIIIa. Protein C is a vitamin K–dependent plasma glycoprotein that, when activated, functions as an anticoagulant by inactivating FVa and FVIIIa. Protein C activity is enhanced by another vitamin K–dependent inhibitory cofactor, protein S. Protein S functions as a cofactor to protein C by enhancing its activity against FVa and FVIIIa (Hoppe & Matsunaga, 2002). In addition, TF pathway inhibitor (TFPI), a protein secreted by endothelium, complexes to FXa and to TF/FVIIa, inactivating them to rapidly limit coagulation (Kumar et al., 2005). Protein C is activated by thrombin that is bound to the transmembrane protein thrombomodulin (TM) on the surface of intact endothelial cells. In human plasma, about 30% of protein S circulates as free protein; the remainder is bound to the complement regulatory protein C4b-binding protein. Only the free form of protein S functions as a cofactor to activated protein C (Dahback, 2005). Platelet-Protein Interactions As previously discussed, primary hemostasis is triggered in response to the damage of the vascular wall and the exposure of blood to subendothelial tissue. Several coordinated interactions among tissue components, plasma proteins, and receptors on platelets lead to the initial sealing of the damaged vessel wall. Platelets are specialized blood cells that play a central role in the physiologic processes of hemostasis. The formation of the primary platelet plug is temporally and spatially coordinated with the activation of the blood coagulation system. Through the process of adhesion and aggregation, mediated by VWF and fibrinogen, the platelets form an occlusive plug or “clot.” Upon damage to the vascular wall, platelets undergo a series of events such as adhesion, aggregation, release Journal of Pediatric Oncology Nursing 24(3); 2007 of granule content, and morphological changes that lead to the formation of the platelet plug. Primary platelet adhesion is dependent on the interaction between platelets and VWF, a large multimeric plasma protein composed of multiple disulphidelinked monomers. The VWF undergoes proteolytic processing in plasma; this processing is mediated by a metalloprotease termed ADAMTS 13—a disintegrinlike and metalloprotease (reprolysin type) with thrombospondin type 1 motif—which generates VWF multimers of all sizes and with different functional efficiency. The larger multimers are more efficient in platelet adhesion than the smaller ones. The VWF mediates platelet adhesion by serving as a bridge between the tissue and the platelets, binding both to collagen exposed at sites of vascular injury and to the platelet membrane glycoprotein Ib-V-IX (GPIb-VIX) (Dahback, 2005; Sadler, 2005). Excessive bleeding can result from an increased fragility of vessels, platelet deficiency or dysfunction, derangement of coagulation, or a combination of these. The physiologic significance of the coagulation pathways is evident given the number of genetic deficiencies that result in bleeding disorders. The activities of platelets and coagulation factors are closely related. With the exception of FXII deficiency, which does not cause bleeding, a deficiency in every other clotting factor has been reported to cause a bleeding disorder (Kumar et al., 2005). Three common hereditary bleeding disorders are hemophilia A (FVIII deficiency), hemophilia B (FIX deficiency), and von Willebrand disease (VWD), with the latter being the most common albeit less symptomatic disorder. Hemophilia A and hemophilia B are both caused by a functional deficiency of a plasma protein inherited in an X-linked manner. Physiologically, the tissue factor pathway of FX activation requires FVIII and FIX for normal thrombin generation, and the absence of either protein severely impairs the ability to generate thrombin and fibrin. Because of the primary clotting factor deficiency in hemophilia A or hemophilia B, clot formation is delayed and is not robust. Thus, patients with hemophilia do not bleed more rapidly; rather, there is delayed formation of an abnormal clot (Nathan et al., 2003). The genes for both FVIII and FIX are located near the telomere of the long arm of the X chromosome. Therefore, both hemophilia A and hemophilia B are inherited as X-linked recessive traits. Numerous 129 Riddel et al mutations within the FVIII gene have been identified that result in hemophilia A. The most common genetic alteration is a gene inversion. In families in which the index patient has a known molecular abnormality, genetic screening and carrier detection are highly accurate (Nathan et al., 2003). In contrast to the complexity of the FVIII gene, the FIX gene is considerably smaller, and its defects have been studied more extensively. More than 60% of the FIX gene defects are due to missense point mutations, and an identifiable defect in the gene can be found in nearly all patients (Nathan et al., 2003). The von Willebrand factor is indispensable for the efficient initiation of platelet adherence to collagenrich matrices under high shear. There are 2 other important platelet collagen receptors: GPVI and the integrin, alpha-2-beta-1, which become engaged after the binding of VWF to GPIb and rapidly amplify the collagen-dependent response. An additional function of VWF is to stabilize the procoagulant cofactor FVIII in the circulation and to serve as FVIII’s carrier protein in plasma. FVIII is a critical regulatory cofactor in the eventual deposition of the fibrin clot. The von Willebrand factor protects FVIII from premature protein C–mediated proteoloytic degradation, prolonging its half-life in circulation and efficiently localizing it at the site of vascular injury (Gill, 2004). Any change in plasma VWF level usually leads to an associated change in FVIII plasma concentration. Thus, VWF performs 2 major roles in hemostasis. First, it mediates the adhesion of platelets to sites of vascular injury, making it essential for platelet plug formation. Second, it functions as a carrier protein that stabilizes coagulation factor FVIII. It is the dysregulation of VWF multimer processing that is associated with the common bleeding disorder, VWD (Dahback, 2005). von Willebrand disease is notable for the considerable heterogeneity of its molecular basis. The population distribution of VWF levels is broad and does not exhibit a simple genetic basis. Although molecular studies have been successful in defining the genetic defects associated with VWD types 2 and 3, VWD type 1, the most common form of VWD, remains a challenge (Brown, Aledort, & Lee, 2002; Sadler, 2004). Since 1989 when the structure of the gene for human VWF was identified, numerous studies have attempted to identify potential VWF defect(s) that may lead to an earlier and more accurate diagnosis of VWD type 1. Due to the complexity of the gene structure, 130 this has proven a difficult task. Fortunately, 2 recent studies completed in Europe and Canada have shed some light on this topic. The studies have confirmed that the genetic basis of VWD type 1 is highly variable and that there are genes in addition to the VWF gene that can result in low plasma VWF levels. However, this work requires validation in independent studies, and additional work needs to be conducted on this subject (James & Lillicrap, 2006). It is expected that these advances in both our understanding of hemostasis and knowledge of the organization of the human genome will pave the way to novel insights into the genetics of bleeding disorders. This ultimately will lead to more precise diagnostic tools and therapeutic interventions. References Aggeler, P. M., White, S. G., Glendenning, M. B., Page, E. W., Leake, T. B., & Bates, G. (1952). Plasma thromboplastin component (PTC) deficiency: A new disease resembling hemophilia. Proceeding of the Society of for Experimental Biology and Medicine, 79, 692-694. Alexander, V., Goldstein, R., Landwehr, G., & Cook, C. (1951). Coagulation serum prothrombin conversion accelerator (SPCA) deficiency: A hitherto unrecognized coagulation defect with hemorrhage rectified by serum and serum fraction. Journal of Clinical Investigation, 30, 596-608. Allen, D. H., & Tracy, P. B. (1995). Human coagulation factor V is activated to the functional cofactor by elastase and cathepsin G expressed at the monocyte surface. Journal of Biological Chemistry, 270, 1408-1415. Allen, G. A., Monroe, D., Roberts, H. R., & Hoffman, M. (2000). The effect of factor X level on thrombin generation and the procoagulant effect of activated factor VII in a cell-based model of coagulation. Blood Coagulation Fibrinolysis, 11(Suppl. 1), S3-S7. Boron, W. F., & Boulpaep, E. L. (2005). Medical physiology (Updated ed.). Philadelphia: Elsevier. Briggs, R., Douglas, A. S., Macfarlane, R. G., Dacie, J. V., Pitney, W. R., Merskey, C., et al. (1952). Christmas disease: A condition previously mistaken for haemophilia. British Medical Journal, 2, 1378-1382. Brown, S. A., Aledort, L., & Lee, C. A. (2002). Haemostasis: From bench to bedside. Haemophilia, 8, 685-693. Dahback, B. (2005). Blood coagulation ad its regulation by anticoagulant pathways: Genetic pathogenesis of bleeding and thrombotic diseases. Journal of Internal Medicine, 257, 209-223. Davie, E. W., & Ratnoff, O. D. (1964). Waterfall sequence for intrinsic blood clotting. Science, 145, 1310-1312. Gill, J. C. (2004). Diagnosis and treatment of von Willebrand disease. Hematology/Oncology Clinics of North America, 18, 1277-1299. Harmening, D. M. (2002). Clinical hematology and fundamentals of hemostasis. Philadelphia: F. A. Davis. Journal of Pediatric Oncology Nursing 24(3); 2007 Theories of Blood Coagulation Hoffbrand, V. A., Catovsky, D., & Tuddenham, E. (Eds.). (2005). Postgraduate haematology (5th ed.). Malden, MA: Blackwell. Hoffman, M. (2004). Remodeling the blood coagulation cascade. Journal of Thrombosis and Thrombolysis, 16(1/2), 17-20. Hoffman, M., & Monroe, D. (2001). A cell-based model of hemostasis. Thrombois and Haemostasis, 85, 958-965. Hoffman, M., & Monroe, D. (2005). Rethinking the coagulation cascade. Current Hematology Reports, 4, 391-396. Hoffman, M., Monroe, D., & Roberts, H. R. (1996). Cellular interactions in hemostasis. Haemostasis, 26(Suppl. 1), 12-16. Hoffman, R., Benz, J., Edward, J., Shattil, S. J., Furie, B., Cohen, H. J., et al. (2005). Hematology: Basic principles and practice. Philadelphia: Elsevier. Hoppe, C., & Matsunaga, A. (2002). Pediatric thrombosis. Pediatric Clinics of North America, 49, 1257-1283. Hougie, C., Barrow, E. M., & Graham, J. B. (1957). Segregation of an hereditary hemorrhagic state from the heterogenous group heretofore called ‘stable factor’ (SPCA) proconvertin, factor VII deficiency. Journal of Clinical Investigation, 36, 485-496. James, P., & Lillicrap, D. (2006). Genetic testing for von Willebrand disease: The Canadian experience. Seminars in Thrombosis and Hemostasis, 32, 546-552. Kjalke, M., Monroe, D., Hoffman, M., Oliver, J., & Ezban, M. (1998). Active site-inactivated factors VIIa, Xa, and IXa inhibit individual steps in a cell-based model of tissue factorinitiated coagulation. Thrombosis Haemostasis, 80, 578-584. Kjalke, M., Monroe, D., Hoffman, M., Oliver, J., Ezban, M., & Hedner, U. (1998). The effects of activated factor VII in a cellbased model for tissue factor-initiated coagulation. Blood Coagulation Fibrinolysis, 9(Suppl. 1), S21-S25. Kleinschnitz, C., Stoll, G., Bendszus, M., Schuh, K., Pauer, H., Burfeind, P., et al. (2006). Targeting coagulation factor XII provides protection from pathological thrombosis in cerebral ischemia without interfering with hemostasis. Journal of Experimental Medicine, 203(3), 513-518. Kumar, V., Abbas, A. K., & Faousto, N. (2005). Robbins and Cotran: Pathologic basis of disease (7th ed.). Philadelphia: Elsevier. Le, D., Borgs, P., Toneff, T., Witte, M., & Rapaport, S. I. (1998). Hemostatic factors in rabbit limb lymph: Relationship to mechanisms regulating extravascular coagulation. American Journal of Physiology, 274, H769-H776. Loscalzo, J. S. A. I. (2003). Thrombosis and hemorrhage (3rd ed.). Philadelphia: Lippincott Williams & Wilkins. Luchtman-Jones, L., & Broze, J. (1995). The current status of coagulation. Annals of Medicine, 27(1), 47-52. Macfarlane, R. G. (1964). An enzyme cascade in the blood clotting mechanism, and its function as a biological amplifier. Nature, 202, 498-499. Monkovic, D. D., & Tracy, P. B. (1990). Activation of human factor V by factor Xa and thrombin. Biochemistry, 29, 1118-1128. Monroe, D., Hoffman, M., & Roberts, H. R. (1996). Transmission of a procoagulant signal from tissue factor-bearing cell to platelets. Blood Coagulation Fibrinolysis, 74, 459-464. Morawitz, P. (1958). The chemistry of blood coagulation [Die Chemie der Blutgerinnung] (R. Hartmann & P. F. Guenter, Trans.). Springfield, IL: Charles C Thomas. Nathan, D. G., Orkin, S. H., Ginsburg, D., & Look, T. A. (2003). Nathan and Oski’s hematology of infancy and childhood (6th ed.). Philadelphia: Saunders. Nichols, W. L., & Bowie, E. J. (Eds.). (2001). A history of blood coagulation: Charles A. Owen, Jr. Rochester, MN: Mayo Foundation for Medical Education and Research. Oliver, J. A., Monroe, D. M., Roberts, H. R., & Hoffman, M. (1999). Thrombin activates factor XI on activated platelets in the absence of factor XII. Arteriosclerosis, Thrombosis, and Vascular Biology, 19, 170-177. O’Shaughnessy, D., Makris, M., & Lillicrap, D. (Eds.). (2005). Practical hemostasis and thrombosis. Malden, MA: Blackwell Publishing Ltd. Osterud, B., & Bjorklid, E. (2006). Sources of tissue factor. Seminars in Thrombosis and Hemostasis, 32, 11-23. Owren, P. A. (1947). The coagulation of blood: Investigations on a new clotting factor. Acta Medica Scandinavica, 194, 521-549. Patek, J., & Stetson, R. H. (1936). Hemophilia: I. The abnormal coagulation of blood and its relation to the blood platelets. Journal of Clinical Investigation, 15, 531-542. Roberts, H. R. (2003). Oscar Ratnoff: His contributions to the golden era of coagulation research. British Journal of Haematology, 122, 180-192. Rosenthal, R. L., Dreskinoff, O. H., & Rosenthal, N. (1953). New hemophilia-like disease caused by a deficiency of a third plasma thromboplastin factor. Proceedings of the Society for Experimental Biology and Medicine, 82, 171-174. Sadler, J. E. (2004). Slippery criteria for von Willebrand disease type 1. Journal of Thrombosis and Haemostasis, 2, 1720-1723. Sadler, J. E. (2005). New concepts in Von Willebrand disease. Annual Reviews in Medicine, 56, 173-191. Shulman, I., & Smith, C. H. (1952). Hemorrhagic disease in an infant due to deficiency of a previously undescribed clotting factor. Blood, 7, 794-807. Telfer, T. R., Denson, K. W., & W1989 whenright, D. R. (1956). A “new” coagulation defect. Seminars in Hematology, 6, 479-493. von Willebrand, E. A. (1931). Uber hereditare pseudohamophilie [On hereditary pseudohemophilia]. Acta Medica Scandinavica, 76, 521-549. Continuing Education Credit The Journal of Pediatric Oncology Nursing is pleased to offer the opportunity to earn pediatric hematology/oncology nursing continuing education credit for this article online. Go to www.aphon.org and select “Continuing Education.” There you can read the article again or go directly to the posttest assessment. The cost is $15 for each article. You will be asked for a credit card or online payment service number. The posttest consists of 10 questions based on the article, plus several assessment questions (e.g., how long did it take you to read the article and complete the posttest?). A passing score of 80% (8 of 10 questions correct) on the posttest and completion of the assessment questions yields one hour of continuing education in pediatric hematology/oncology nursing for each article. Journal of Pediatric Oncology Nursing 24(3); 2007 131