2014 Neer Award Paper: Neuromonitoring the Latarjet procedure
advertisement

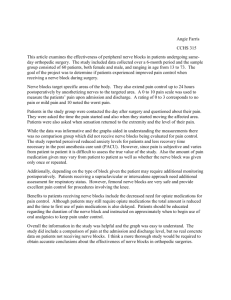
J Shoulder Elbow Surg (2014) 23, 1473-1480 www.elsevier.com/locate/ymse 2014 Neer Award Paper: Neuromonitoring the Latarjet procedure Ruth A. Delaney, MB BCh, BAO, MRCSa, Michael T. Freehill, MDa, David R. Janfaza, MDb, Kamen V. Vlassakov, MDb, Laurence D. Higgins, MDc, Jon J.P. Warner, MDa,* a Boston Shoulder Institute, Massachusetts General Hospital, Boston, MA, USA Department of Anesthesiology, Brigham & Women’s Hospital, Boston, MA, USA c Boston Shoulder Institute, Brigham & Women’s Hospital, Boston, MA, USA b Background: We used intraoperative neuromonitoring to define the stages of the Latarjet procedure during which the nerves are at greatest risk. Methods: Thirty-four patients with a mean age of 28.4 years were included. The Latarjet procedure was divided into 9 defined stages. Bilateral median and ulnar somatosensory evoked responses and transcranial motor evoked potentials from all arm myotomes were continuously monitored. A ‘‘nerve alert’’ was defined as averaged 50% amplitude attenuation or 10% latency prolongation of ipsilateral somatosensory evoked responses and transcranial motor evoked potentials. For each nerve alert, the surgeon altered retractor placement, and if there was no response to this, the position of the operative extremity was then changed. Results: Of 34 patients, 26 (76.5%) had 45 separate nerve alert episodes. The most common stages of the procedure for a nerve alert to occur were glenoid exposure and graft insertion. The axillary nerve was involved in 35 alerts; the musculocutaneous nerve, in 22. Of the 34 patients, 7 (20.6%) had a clinically detectable nerve deficit postoperatively, all correlated with an intraoperative nerve alert. All cases involved the axillary nerve, and all resolved completely from 28 to 165 days postoperatively. Prior surgery and body mass index were not predictive of a neurologic deficit postoperatively. However, total operative time (P ¼ .042) and duration of the stage of the procedure in which the concordant nerve alert occurred (P ¼ .010) were statistically significant predictors of a postoperative nerve deficit. Conclusions: The nerves, in particular the axillary and musculocutaneous nerves, are at risk during the Latarjet procedure, especially during glenoid exposure and graft insertion. Level of evidence: Level IV, Case Series, Treatment Study. Ó 2014 Journal of Shoulder and Elbow Surgery Board of Trustees. Keywords: Instability; Latarjet procedure; neurologic complications; axillary nerve; musculocutaneous nerve Partners Healthcare Institutional Review Board approval: Protocol # 2011P000188. *Reprint requests: Jon J.P. Warner, MD, The Harvard Shoulder Service, 55 Fruit St, Yawkey Center for Outpatient Care, Suite 3200, 3G, Room 3046, Boston, MA 02114, USA. E-mail address: jwarner@partners.org (J.J.P. Warner). The Latarjet procedure is a proven, established method of treating glenohumeral instability, particularly when there is bone loss of the glenoid or after a failed soft tissue instability repair. One large series reported a 5% redislocation rate and 96% patient satisfaction.5 Other large series have reported more than 1000 procedures with an 1058-2746/$ - see front matter Ó 2014 Journal of Shoulder and Elbow Surgery Board of Trustees. http://dx.doi.org/10.1016/j.jse.2014.04.003 1474 R.A. Delaney et al. Figure 1 Typical surgical positioning and neuromonitoring lead placement before (A) and after (B) placement of iodophor surgical drape. (Note that the leads distal to the elbow were placed and protected before the arm was placed in the holder.) instability recurrence of 1%.14,15 There is concern that the nonanatomic transfer of the coracoid alters anatomy of the surrounding nerves. It has been shown in a cadaveric study that the Latarjet procedure resulted in significant alterations in the anatomic relationships of the axillary and musculocutaneous nerves.2 In addition, the challenges of performing a Latarjet procedure have been highlighted in the literature by reports of its complications.17 A recent systematic review concluded that this procedure has a 30% overall complication rate and a 1.8% rate of neurovascular complication.3 Furthermore, short-term complications of the Latarjet procedure were reported to have an overall rate of 25%, with a 10.4% rate of neurologic injury. In that series, there was a 4% rate of neurologic injury that did not improve with conservative measures.12 Neuromonitoring has been used in such varied disciplines as intracranial surgery, vascular surgery, and thyroid surgery and extensively in spine surgery. More recently, neuromonitoring has been used in shoulder surgery, including arthroplasty and proximal humerus fracture fixation.11,16 Given the reported rate of neurologic injury, we undertook to study in more depth the neurologic complications of the Latarjet procedure by using intraoperative neuromonitoring to define the stages of the procedure during which the nerves are at greatest risk for iatrogenic injury. Methods We prospectively performed intraoperative neuromonitoring of 40 patients undergoing the Latarjet procedure for shoulder instability between April 1, 2011, and December 31, 2012, by the two senior surgeons. We excluded 2 patients from the study because of limitation of neuromonitoring to somatosensory evoked potentials (SSEPs) due to a history of brain trauma and the presence of aneurysm clips. Three more patients were excluded because of technical difficulties with the neuromonitoring equipment intraoperatively. One patient required inhalational anesthesia, which degraded the quality of the neuromonitoring, and this patient was excluded from the study. Therefore, 34 patients (28 male patients, 6 female patients) met the inclusion criteria. Mean age at surgery Figure 2 Motor (TcMEP and EMG) baseline tracings at the beginning of a case. was 28.4 years (range, 15-66 years). Eighteen patients (52.9%) had surgery on the dominant extremity. All Latarjet procedures were performed open, in the beach chair position, through a deltopectoral approach. Propofol was used for induction of anesthesia, and a short-acting neuromuscular blocking agent (succinylcholine) was used to facilitate intubation. The standardized anesthesia was total intravenous anesthesia with continuous depth of anesthesia monitoring and without muscle relaxation or peripheral nerve block. The neuromonitoring protocol was based on published literature11,16 and on the advice of two board-certified attending neurophysiologists. After patient positioning, stimulating and recording leads were placed in the scalp and the upper extremities, respectively (Fig. 1). The parameters measured were median Neuromonitoring the Latarjet procedure 1475 Figure 3 Key stages of the Latarjet procedure. (A) Coracoid exposure. (B) Coracoid harvest. (C) Subscapularis split. (D) Glenoid exposure. (E). Graft placement. SSEPs, myogenic motor evoked responses evoked by transcranial electrical stimulation (TcMEPs), and free electromyogram (EMG). TcMEPs and free EMG were recorded from deltoid, triceps, biceps, extensor carpi radialis longus, abductor pollicis brevis, and abductor digiti minimi muscles. Myotomes were selected on the basis of major innervation patterns of the brachial plexus and peripheral nerves considered to be at risk during this procedure. Contralateral median nerve SSEPs as well as contralateral arm TcMEPs and free EMG were recorded for reference. Before incision, adequate reversal of the neuromuscular blocking agent was confirmed by obtaining 4 muscle twitches from the abductor digiti minimi muscle of the nonoperative extremity in response to train-of-4 electrical stimulation of the ulnar nerve, stimulating at 2 Hz at a supramaximal stimulus plus 10%. Baseline TcMEPs were measured 20 minutes after induction, before incision (Fig. 2). These were recorded with the operative arm in neutral position, in external and internal rotation with the arm at the side, and in neutral abduction and abducted external and internal rotation. Depth of anesthesia was monitored throughout the procedure, and if there was any change greater than 15%, new TcMEP baselines were measured. Otherwise, there was no change in stimulation strength for SSEPs to MEPs after baseline responses were collected. A significant nerve alert event, implying impending excessive traction on a neural element, was defined as 50% attenuation and 10% prolongation of latency in SSEPs; 50% attenuation, 10% latency prolongation in TcMEPs (highest peak to lowest trough), 1476 or significant change (80% decrease) in waveform amplitude; or sustained neurotonic discharge on EMG. An early warning alert was called if a polyphasic TcMEP response became biphasic. The Latarjet procedure was divided into 9 stages: (1) incision, (2) coracoid exposure, (3) coracoid harvest, (4) subscapularis split, (5) glenoid exposure, (6) glenoid preparation, (7) graft insertion, (8) subscapularis closure, and (9) skin closure (Fig. 3). The duration of each stage was recorded intraoperatively, as was the total operative time. When a nerve alert was signaled by the neurophysiologist, retractors were removed in a step-wise fashion, beginning with the retractor believed by the surgeon to be most likely causing the stretch or insult of the nerve involved in the alert. If this did not result in improvement of the neuromonitoring parameters, the operative arm was returned to a more neutral position. For each nerve alert, the nerves involved, the stage of the procedure, the number and position of retractors, the position of the operative arm, and the time elapsed until return to above nerve alert threshold were recorded by a separate member of the research team not directly involved in the surgery. After a nerve alert, the procedure continued with an attempt to limit or, where possible, completely avoid the provocative position. Postoperatively, the patient received a complete neurologic examination of the operative extremity at the earliest possible opportunity in the recovery room. Any clinically detectable deficits and their correlation with intraoperative nerve alerts were recorded. The occurrence of a nerve alert and the occurrence of a clinically detectable postoperative neurologic deficit were each analyzed as separate outcomes. Statistical analysis of potential risk factors for each outcome was performed with the Fisher exact test, the Student t-test, and logistic regression. The following factors were analyzed: prior surgery on the operative shoulder, body mass index, total operative duration, and duration of stage of the procedure. Of the 34 patients, 19 had prior surgery on the shoulder undergoing the Latarjet procedure, including 5 patients who had 2 previous failed procedures. The prior procedures included arthroscopic Bankart repair (n ¼ 17 in 14 shoulders), arthroscopic bony Bankart repair (n ¼ 1), open labral repair/capsular shift (n ¼ 4 in 3 shoulders), and arthroscopic repair of humeral avulsion of the glenohumeral ligaments (n ¼ 2 in 1 shoulder). There were no complications related to the neuromonitoring. Two patients, both young men with questionable postoperative compliance and no other overt cause of failure, displaced their coracoid graft within 6 weeks and were revised to an EdenHybinette procedure, both of which were also neuromonitored, with no nerve alerts occurring during either the primary Latarjet procedure or the revision Eden-Hybinette procedure. There were no other recurrences of instability. The patients were seen at regular intervals postoperatively, as is standard for the Latarjet procedure, with the first visit at 10 to 14 days postoperatively and subsequent visits at approximately 6 weeks and 3 months. At each visit, a detailed neurologic examination of the operative extremity was documented. Results Of the 34 patients, 26 (76.5%) had at least 1 nerve alert during their surgery. Of these, 12 patients had 1 nerve alert, 11 patients had 2 nerve alerts, 1 patient had 3 nerve alerts, R.A. Delaney et al. Figure 4 An axillary nerve alert during glenoid exposure. Attenuation of the axillary nerve TcMEP is shown in the top left of the screen (white tracing), in contrast to the normal TcMEP tracing in the right panel for the nonoperative arm. Table I Intraoperative nerve alerts and nerves affected during each stage of the procedure Stage 1. 2. 3. 4. 5. 6. 7. 8. No. of Nerves involved nerve alerts Incision 0 Coracoid exposure 3 Coracoid harvest 4 Subscapularis split 2 Glenoid exposure 12 Glenoid preparation 4 Graft placement 17 0 Subscapularis closure 9. Skin closure 3 d MC, ulnar, Ax þ MC Ax, MC, ulnar, Ax þ MC Ax, Ax þ radial Ax (2), MC (3), Ax þ MC (7) MC (2), Ax þ MC (2) Ax (13), MC (1), Ax þ MC (2) d Ax (3) Ax, axillary nerve; MC, musculocutaneous nerve. Total 45 alerts. and 2 patients each had 4 nerve alert events. Eight patients had no nerve alerts and no clinically detectable deficit postoperatively. The most common nerve to be involved in a nerve alert was the axillary nerve (involved in 35 alerts of 45 total alerts [78%]). Most of the alerts (41 of 45 alerts [91%]) were based on attenuation of TcMEPs to less than 50% of baseline (Fig. 4). Two alerts were based on SSEPs, 1 was based on EMG, and 1 was based on both EMG and TcMEPs. Of the total 45 nerve alerts, 15 alerts involved 2 Neuromonitoring the Latarjet procedure 1477 Figure 5 Number of nerve alerts in relation to whether retractors were in place at the time (yes/no) and arm position at the time of alert (yes/no for each given position). ER, external rotation; ABD, abduction; FLEX, flexion. nerves simultaneously (most commonly axillary and musculocutaneous). No alert involved more than 2 peripheral nerves (Table I). In 20 of the 26 nerve alerts (77%), baseline neuromonitoring parameters were recovered at a mean of 10 minutes (range, 0.5-34 minutes). The number of nerve alerts for different arm positions and presence of retractors is illustrated in Figure 5. In 4 of the 45 alerts (9%), there were no retractors in place at the time of the alert. During these 4 alerts, the arm was in neutral position. One of these alerts involved the ulnar nerve, and the stockinette and arm holder were adjusted, with return to baseline of the ulnar nerve SSEP that had defined the alert. The other 3 alerts occurred in neutral position with no retractors in place during skin closure. These all involved the axillary nerve, and 2 of the 3 patients had previously had an axillary nerve alert during an earlier stage of the procedure. These alerts may reflect failure to fully recover from the previous alert or stretch on the axillary nerve as it accommodates to the new, nonanatomic course imposed on it by the presence of the coracoid graft. Seven patients (20.6%) had a clinically detectable neurologic deficit postoperatively, all involving the axillary nerve and all correlating with an intraoperative axillary nerve alert. These patients’ nerve alerts, intraoperative action taken, and details of the nerve palsies are summarized in Table II. Two patients had previous arthroscopic Bankart repairs; the other 5 had no prior surgery on that shoulder. All seven patients’ nerve palsies had fully resolved by the time of latest follow-up, with a mean time to resolution of 86.6 days (range, 28-165 days) (Table II). In three patients who had a nerve deficit postoperatively, additional steps were taken intraoperatively in an attempt to relieve tension from the axillary and musculocutaneous nerves: repositioning of the coracoid graft (2 patients) and division of fascia over conjoined tendon with specific axillary nerve release (1 patient). In the 2 patients whose coracoid graft was repositioned, the graft was removed because of failure to recover baseline signals in the axillary and musculocutaneous nerves after a nerve alert during graft insertion. In both cases, the graft was reinserted in a more superior position, and in one case, a hand surgeon with expertise in nerve microsurgery scrubbed in and verified that the axillary nerve was grossly intact. Both of these patients had a mild sensory axillary neurapraxia and one had in addition mild deltoid weakness. These clinical findings persisted at 12 days postoperatively in both patients and resolved by 28 and 37 days postoperatively, respectively. In the one patient for whom division of the fascia over the conjoined tendon and release of the axillary nerve from all tension was performed, the axillary nerve did not fully recover on neuromonitoring. Postoperatively, he had a sensory neurapraxia and deltoid weakness. Plain film radiographs demonstrated inferior humeral head subluxation. This had resolved at 120 days postoperatively, with return of full deltoid strength. Statistical analysis showed that prior surgery, body mass index, total operative time, and duration of stage of the procedure were not statistically significant predictors of the occurrence of a nerve alert, although total operative time and duration of stage of the procedure each showed a relationship trending toward significance (P ¼ .063 and P ¼ .061, respectively). Prior surgery, body mass index, and number of nerve alerts during surgery were not predictive of a clinically detectable neurologic deficit postoperatively; however, total operative time and duration of the stage of the procedure in which the concordant nerve alert occurred were statistically significant predictors of a postoperative nerve deficit (Fig. 6). The mean operative time in the group with no clinical nerve deficit was 106 minutes, and the mean operative time in patients with a clinically detectable neurologic deficit was 139.6 minutes (P ¼ .042). The mean duration of a stage 1478 R.A. Delaney et al. Table II Summary of clinically detectable neurologic deficits Study Nerve alerts ID 101 110 115 119 Action taken 1. Axillary Retractor removed Arm repositioned from abduction to adduction 1. Musculocutaneous Retractor removed 2. Axillary Retractors removed 3. Axillary Retractors removed Graft removed and reinserted more superiorly 4. Axillary Retractors removed Conjoined tendon taken down completely and tenodesed, coracoid placed as free graft 1. Axillary þ Retractors removed musculocutaneous 2. Axillary þ Retractors removed musculocutaneous 1. Musculocutaneous Retractors removed 2. Axillary þ Retractors removed musculocutaneous 122 3. Axillary þ Retractor removed musculocutaneous Graft removed and reinserted more superiorly 1. Axillary Retractors removed 124 1. Axillary 126 1. Axillary and Retractors removed musculocutaneous Fascia over the transferred conjoined tendon divided to take tension off axillary nerve Retractors removed of the procedure during which a nerve alert occurred, resulting in a clinical deficit, was 26.8 minutes compared with a mean stage duration of 11.2 minutes when there was a nerve alert but with no resulting clinical nerve deficit from that stage (P ¼ .010) (Fig. 6). Discussion The Latarjet procedure, first described in 1954,8 has regained popularity in North America as a surgical option for the treatment of both primary and recurrent shoulder instability. Latarjet first described a series of 4 patients with recurrent anterior instability of the shoulder in whom he transferred the coracoid process with the conjoined tendon to the anterior scapular neck, securing it with a bone screw. Neuromonitoring return to above alert threshold Clinical deficit Timing of resolution No Yes Mild axillary sensory neurapraxia Yes Yes No Yes Mild axillary sensory and motor neurapraxia Deficit present at 40 days, resolved by 89 days Deficit present at 12 days, resolved by 37 days No No Yes Mild axillary sensory neurapraxia Deficit present at 12 days, resolved by 40 days No Mild axillary sensory Axillary returned; neurapraxia musculocutaneous incomplete No Incomplete recovery of both nerves Yes Mild axillary sensory neurapraxia and deltoid weakness Deficit present at 12 days, resolved by 28 days Yes Yes No No Both deficits present at 12 days; motor resolved by 47 days, sensory resolved by 127 days Deltoid weakness Deficit present at 35 days, resolved by 165 days Deltoid weakness and Both deficits present in recovery room; mild sensory sensory resolved neurapraxia by 12 days, motor resolved by 120 days The original technique of coracoid transfer as described by Latarjet involved cutting the subscapularis tendon; this has subsequently been modified to a subscapularis split in some technique descriptions, preserving the tendon attachment. Helfet described the Bristow procedure in 1958, named for his former chief, W. Rowley Bristow.4 In this procedure, the osteotomized coracoid (although a shorter graft length than the traditional Latarjet) and conjoined tendon were sutured only to the capsuloperiosteal elements of the anterior glenoid. Later, May described a modification to the Bristow procedure that again fixed the transferred coracoid fragment and conjoined tendon with a bone screw in a manner similar to the original Latarjet procedure.10 In Europe, some surgeons use the Latarjet procedure as the primary procedure of choice for anterior instability of the shoulder, with the Eden-Hybinette procedure as the Neuromonitoring the Latarjet procedure Figure 6 Mean duration of the stage of the procedure during which a nerve alert occurred, resulting in a clinical deficit, compared with mean stage duration when no clinical nerve deficit resulted from that stage. procedure of choice for any recurrence of instability after Latarjet.9 High reported failure rates of arthroscopic soft tissue stabilization in cases of glenoid deficiency may explain the resurgence of the Latarjet procedure.1 The incidence of neurologic injury after the Latarjet procedure has been reported to vary from 1.8% to 10.4%.4,12,17 There have also been isolated reports of injury to the musculocutaneous nerve and the suprascapular nerve.7,13 Freehill et al described the alteration in the anatomy of the musculocutaneous and axillary nerves after the Latarjet procedure.2 Their cadaveric study found that the musculocutaneous nerve moved inferior to the anterior glenoid rim after the Latarjet procedure. The axillary and musculocutaneous nerves also became more medial to their original position, which may make them vulnerable to injury if a subsequent procedure is performed. They also showed that the musculocutaneous and axillary nerves consistently overlap each other after a Latarjet procedure, obscuring the future identification of either nerve. However, in that study, the graft was placed after taking the upper subscapularis down vs a split in the muscle, and therefore tensions and positions of nerves may have slight differences on the basis of the technique used. We acknowledge limitations of our study. First, the small sample size was underpowered to demonstrate a difference in incidence of neurologic complication due to neuromonitoring. Second, there was susceptibility to observer bias as the clinicians examining the patients postoperatively looking for a neurologic deficit were aware of the study and the need for a thorough neurologic examination, which may not have been consistently performed in other Latarjet patients outside of this study. Prior studies on the incidence of neurologic injury after the Latarjet procedure have diagnosed injury primarily through the postoperative examination.12 This may cause the reported incidence to be lower, as complete neurologic examination of the postoperative shoulder is often difficult 1479 and limited by pain. Furthermore, given that most nerve injuries are thought to be transient, it is possible that some of the intraoperative nerve injuries resolve before they are recognized clinically. Third, it is challenging to reconcile the high sensitivity of the intraoperative neuromonitoring with clinical significance postoperatively. Some intraoperative nerve alerts, although physiologically valid, had no postoperative clinical relevance as evidenced by the 19 patients in our series who had intraoperative nerve alerts but no clinically detectable neurologic deficit postoperatively. In our series of 34 patients, 26 (76.5%) had intraoperative nerve alerts, necessitating a surgical pause, removal of retractors, and in some cases repositioning of the operative arm to a more neutral position. It is likely that a nerve injury was prevented in at least some of these patients. In 27 of the 45 alerts (79.4%), the operative arm was positioned in external rotation at the time of the nerve alert. External rotation and abduction have been shown biomechanically by Kwaan and Rappaport to produce traction on the brachial plexus,6 supporting the theory that these nerve alerts were most likely caused by stretch of the nerves involved. This finding can be used by surgeons in performing the procedure to periodically relax the arm when it is noted that the axillary nerve is on high stretch. In 5 patients, additional steps were taken in an attempt to reduce the risk of nerve injury. In 2 patients, the graft was removed and repositioned more superiorly when other measures (retractor removal, arm repositioning) did not resolve a nerve alert that had occurred during graft insertion. The altered course of the axillary nerve around the transplanted coracoid appears to risk stretching of the nerve, and a slightly more superior graft position may therefore be protective. However, the coracoid graft must still remain subequatorial if stability is to be reliably achieved. We typically aim for a graft position at 4 to 5 o’clock on the glenoid of a right shoulder. Of the 45 nerve alerts, 29 (64.4%) occurred during either glenoid exposure or graft insertion, highlighting that these stages of the procedure carry the highest risk of neurologic injury. Operative time and duration of high-risk stages of the procedure were shown to be risk factors for a clinically detectable neurologic injury. These data provide a rationale for moving expeditiously through these stages of the procedure and, if there is an intraoperative delay for any reason, removing retractors and repositioning the arm to neutral. Conclusion The nerves of the brachial plexus, in particular the axillary nerve and the musculocutaneous nerve, are at risk during the Latarjet procedure. During neuromonitoring, nerve alerts happen frequently, and it can be 1480 possible for the surgeon to reduce them with some technical measures. Transient neurologic deficits are noted after this surgery that may be missed if careful neurologic examination is not performed. Neuromonitoring may especially have a role in situations in which one might anticipate risk to nerves, such as longer, revision surgery with severe scarring and distortion of anatomy. The most common stages of the Latarjet procedure during which the nerves are under excessive tension are glenoid exposure and graft insertion. During these stages, the arm is often externally rotated, and the surgeon should be especially meticulous and consider duration of retraction during these stages, with potential periods of retractor and arm relaxation. The significant predictors of a clinical neurologic deficit postoperatively were the total operative duration and the duration of these high-risk stages of the procedure, suggesting that the surgery, in particular those high-risk stages, should be completed as expeditiously as possible. R.A. Delaney et al. 2. 3. 4. 5. 6. 7. 8. 9. Disclaimer Michael T. Freehill is a consultant for Smith & Nephew. Laurence D. Higgins receives fellowship support from Arthrocare; DJ Orthopaedics; Arthrex, Inc; Mitek; Breg; and Smith & Nephew. Jon J.P. Warner receives fellowship support from Arthrocare; DJ Orthopaedics; Arthrex, Inc; Mitek; Breg; and Smith & Nephew. He receives royalties from Tornier, Inc, and has equity in Orthospace and Vumedi. The other authors, their immediate families, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. 10. 11. 12. 13. 14. 15. 16. References 17. 1. Burkhart SS, De Beer JF. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000;16:677-94. Freehill MT, Srikumaran U, Archer KR, McFarland EG, Petersen SA. The Latarjet coracoid transfer procedure: alterations in the neurovascular structures. J Shoulder Elbow Surg 2013;22:695-700. http:// dx.doi.org/10.1016/j.jse.2012.06.003 Griesser MJ, Harris JD, McCoy BW, Hussain WM, Jones MH, Bishop JY, et al. Complications and re-operations after BristowLatarjet shoulder stabilization: a systematic review. J Shoulder Elbow Surg 2013;22:286-92. http://dx.doi.org/10.1016/j.jse.2012.09. 009 Helfet AJ. Coracoid transplantation for recurring dislocation of the shoulder. J Bone Joint Surg Br 1958;40:198-202. Hovelius L, Sandstr€om B, Olofsson A, Svensson O, Rahme H. The effect of capsular repair, bone block healing, and position on the results of the Bristow-Latarjet procedure (study III): long-term followup in 319 shoulders. J Shoulder Elbow Surg 2012;21:647-60. http://dx. doi.org/10.1016/j.jse.2011.03.020 Kwaan JH, Rappaport I. Postoperative brachial plexus palsy: a study on the mechanism. Arch Surg 1970;101:612. L€adermann A, Denard PJ, Burkhart SS. Injury of the suprascapular nerve during Latarjet procedure: an anatomic study. Arthroscopy 2012;28:316-21. http://dx.doi.org/10.1016/j.arthro.2011.08.307 Latarjet M. Treatment of recurrent dislocation of the shoulder. Lyon Chir 1954;49:994-7. Lunn JV, Castellano-Rosa J, Walch G. Recurrent anterior dislocation after the Latarjet procedure: outcome after revision using a modified Eden-Hybinette operation. J Shoulder Elbow Surg 2008;17:744-50. http://dx.doi.org/10.1016/j.jse.2008.03.002 May VR Jr. A modified Bristow operation for anterior recurrent dislocation of the shoulder. J Bone Joint Surg Am 1970;52:1010-6. Nagda SH, Rogers KJ, Sestokas AK, Getz CL, Ramsey ML, Glaser DL, et al. Neer Award 2005: peripheral nerve function during shoulder arthroplasty using intraoperative nerve monitoring. J Shoulder Elbow Surg 2007;16:S2-8. http://dx.doi.org/10.1016/j.jse.2006.01. 016 Shah AA, Butler RB, Sung SY, Wells JH, Higgins LD, Warner JJ. Short-term complications of the latarjet procedure. J Bone Joint Surg Am 2012;94:495-501. http://dx.doi.org/10.2106/JBJS.J.01830 Southam JD, Greis PE. Delayed, transient musculocutaneous nerve palsy after the Latarjet procedure. J Shoulder Elbow Surg 2012;21:e811. http://dx.doi.org/10.1016/j.jse.2011.09.025 Walch G. La luxation re cidivante ante rieure de l’e paule. Rev Chir Orthop 1991;77(Suppl 1):177-91. Walch G, Boileau P. Latarjet-Bristow procedure for recurrent anterior instability. Tech Shoulder Elbow Surg 2000;1:256-61. Warrender WJ, Oppenheimer S, Abboud JA. Nerve monitoring during proximal humeral fracture fixation: what have we learned? Clin Orthop Relat Res 2011;469:2631-7. http://dx.doi.org/10.1007/s11999010-1760-3 Young DC, Rockwood CA Jr. Complications of a failed Bristow procedure and their management. J Bone Joint Surg Am 1991;73: 969-81.