Brain Death: Recent Ethical and Religious Considerations in Iran
S.M. Akrami, Z. Osati, F. Zahedi, and M. Raza
ABSTRACT
The Islamic Republic of Iran has a long history of medicine. The principles derived from
core Islamic teachings provide a comprehensive moral, ethical, and legal framework for
the practice of medicine. The issue of brain death has significant impact on the
procurement of organs from cadavers. It is a major subject of debate and interest to
bioscientisits, legal experts, religious scholars, and the general public. Laws related to the
ethical and legal aspects of cadaver organ donation from the brain dead have not been
defined in many Muslim countries. This report presents recent advances in Iranian law
with regard to the ethics of organ transplantation and the definition of brain death.
O
RGAN transplantation (OT) has been advanced for
end-stage failure of vital organs because of the
developments in surgical and immunosuppressive techniques and public awareness. This applied medical knowledge has shown a high impact to save life and improve the
quality of a patient’s life. Success in the implementation of
OT programs in a country depends on different factors
including economic situation, religious permission, public
views, medical expertise, and existing laws. There are some
Islamic countries that have a positive Fatwa (religions
opinion) for OT, but have not adapted it as law, such as
Pakistan, Egypt, and Syria.1 Iranian laws, with majority of
its population as Muslims, are derived from the teachings of
the Quran and the sayings of Prophet Muhammad. With
regard to contemporary problems related to bioethics, such
as brain death and organ donation, Iranian laws during the
last 20 years have been amended to be in accordance with
Islamic teachings with general public approval via the
parliament.
Availability of organs for transplantation is a global
problem. Brain dead cadavers are one of the prime sources
of donated organs. However, public acceptability of brain
death and attitudes toward the brain dead are deeply
influenced by literacy level, prevalent social customs, and
religious backgrounds. Keeping in view these limitations to
cadaver donation, the Iranian Parliament recently passed
an act that has facilitated the procurement of organs from
brain dead patients. In this report, we describe the history
and background of the relevant aspects of brain death and
OT in Iran. We hope that other countries worldwide,
especially Islamic countries, can adopt similar legal measures to raise public awareness and acceptability with
regard to brain death and cadaveric organ donation.
BRAIN DEATH DEFINITION
The concept of brain death has been historically modified
several times.2 The earlier “heart-lung” death definition
was not satisfactory for all conditions. Therefore, it was first
improved by the Harvard criteria in 1968.3 A summary
statement on “Practice Parameters for Determining Brain
Death in Adults” was issued by the American Academy of
Neurology (AAN) in 1995.4 In 1999, a review by Jenkins et
al presented a protocol for rapidly determining brain
death.5 A significant reduction in the time to declare brain
death was obtained by the brain death determination
protocol, which is currently accepted worldwide.6
Brain death is defined as complete and irreversible
cessation of all brain and brain stem functions synchronously. It is characterized by complete apnea, absent brain
stem reflexes, and cerebral unresponsiveness.4,7 Usually the
brain dead patient is in a coma requiring a ventilator with a
known cause of serious brain damage, such as traumatic
injury.
RELIGIOUS AND HISTORIC BACKGROUND
There are more than 1.3 billion Muslims worldwide. The
majority live in Asia or Africa. Iran has land spread over 1.6
million sq km with 99% of its 68 million population being
From the Endocrinology and Metabolism Research Centre
(S.M.A., F.Z., M.R.), Tehran University of Medical Sciences; and
Sadra Islamic Philosophy Research Institute (Z.O.), Tehran, Iran.
Address reprint requests to S. M. Akrami, MD, PhD, 5th Floor,
Shariati Hospital, North Kargar St., Tehran 14114, Iran. E-mail:
akramism@sina.tums.ac.ir
© 2004 by Elsevier Inc. All rights reserved.
360 Park Avenue South, New York, NY 10010-1710
0041-1345/04/$–see front matter
doi:10.1016/j.transproceed.2004.10.046
Transplantation Proceedings, 36, 2883–2887 (2004)
2883
2884
Muslim. Islam has introduced its own moral, ethical, and
social framework for human life. Islam has granted a
certain privilege for saving a human’s life. The Quran
explicitly mentions “who so ever gives life to a soul, it shall
be as if he had given life to mankind altogether” (5:32).
Therefore, any medication, treatment, and prevention considered as a vital step to maintain normal health of mankind
is not only accepted but also recommended. OT is not
exempted from this rule. There is no ruling against organ
donation in Islam as long as it is done with respect to the
deceased and for the benefit of the recipient.
OT has been similarly accepted by different religions such
as Christianity, Judaism, Hinduism, and Islam. Generally,
Christianity accepts the rule “Give it and it will be given to
you” in this matter. Transplantation is believed to be a
life-saving procedure by Judaism, and, according to Hinduism, donation after death alleviates suffering.8
OT was first permitted by Shia scholars in 1964 and Sunni
scholars in 1986. Since then, OT and brain death have been
widely studied by Muslim scientists.9 –12 Islamic scholars
have, however expressed two different views on OT.13 Some
scholars are of the opinion that because human life does not
end by brain death with a beating heart, OT is impermissible from a brain dead person. However, the majority of
scholars believe that as human life ends physically by brain
death, so in the case of need and necessity, OT is permissible.
In a meeting of the Council of Islamic Jurisprudence held
in Amman, Jordan on October 16, 1986, brain death was
accepted14 and the definition of legal death agreed by the
majority of scholars.8 The Third International Conference
of Islamic Jurists in 1986 equated brain death with heart
death.15 Aksoy discussed this issue in more detail regarding
the current understanding of Islamic scholars, especially
from the Sunni schools of thought.9
Ayatollah Khomeini, a prominent Shia scholar, pointed
out in response to an istifta (religious question) regarding
OT from the brain dead with irreversible life, “It is authorized to use organs such as heart, liver, etc. of a definite
brain dead with permission of organ owner for transplantation if someone else’s life is depended on it”.16 In
response to a similar istifta, Ayatollah Khamene’i responded “In such situation, there wouldn’t be any problem
using organs if someone’s life is dependent on the organ”.17
Ayatollah Fazel Lankarani responded to brain death
istifta that taking organs of a person with no hope of life due
to brain infarction or accident but with heart beating is
difficult. However, it is permissible for organs other than the
heart if someone’s life is dependent on it.18 Ayatollah Noori
Hamedani answered that OT of a brain dead patient is
permissible but should be authorized by a Faqhih (religious
scholar) in the case of not having a will from the patient.19
Ayatollah Makarem Shirazi permitted OT from a brain
dead patient if it is completely and definitely diagnosed to
be irreversible.20
AKRAMI, OSATI, AND ZAHEDI
OT HISTORY IN IRAN
During the last two decades, Iran has developed facilities
and education for OT. Most facilities are located in Shiraz
and Tehran university hospitals. In recent years, developments in OT have resulted in a large number of Iranian
expert staff working on cornea, bone marrow, skin, heart,
kidney, liver, cardiac valves, bone, ligament, cartilage, and
lung transplantations. There are 22 hospital wards for
kidney transplantation, 2 for liver, 2 for heart and heartlung transplantation, and 2 for bone marrow transplantation in Iran.21
Iran is a pioneer in kidney transplantation among Middle
Eastern countries with approximately 24 transplantation
per million population per year.22 The first kidney transplantation was done in 1967 in Shiraz (south Iran)23 and the
first hospital ward for kidney transplantation was established in 1985 in Tehran.24 More than 10,000 renal transplantation procedures were performed between 1980 and
2000.22 The expense of renal transplantation is much less in
Iran (approximately $5000 [United States; US]) compared
with European countries.21
In Iran, commercial OT is not a serious issue and donors
and recipients know each other in almost all cases. There is
no unknown origin kidney transplantation. Although approximately 80% of living donors belong to the low economic class, it is the same for more than 50% of the
recipients.25 A rewarded gift (approximately $1000 US) is
paid by the government to the kidney donors via the Charity
Foundation for Specific Disorders (CFFSD), which is a
nongovernmental organization (NGO). This was established according a law approved by the government in 1997.
There are other reasons to overcome this issue, such as the
Islamic culture that looks to organ donation as a charitable
act, the performance of OTs only in governmental university hospitals, and the payment for all hospital expenses by
the government.
In a study of 8409 renal transplantations in Iran, 63.4% of
recipients were men and 36.6% were women, whereas the
majority of donors were men (64.7%) without familial
relations (67.8%) with the recipients.24 Heart transplantation was first performed in 1993. By the end of 2002, more
than 45 procedures were reported in Tehran university
hospitals. The first liver transplantation was performed in
1993 in Shiraz.26 By the end of 2002, there were approximately 72 liver transplantation cases in both Tehran and
Shiraz. For pancreatic -cell transplantation, initial work
has started.
NEED FOR LEGISLATION
Despite the permission of religious scholars, the lack of
legislation was the main problem for the practical implementation of cadaveric OT all in Iran. In this regard, the
issue of brain death was first discussed in the Iranian
Parliament in 1995, but was not approved at that time. It
was again discussed in 1999 in the Parliament. At last the
act of “Deceased or Brain Dead Patients Organ Transplan-
BRAIN DEATH: IRAN
2885
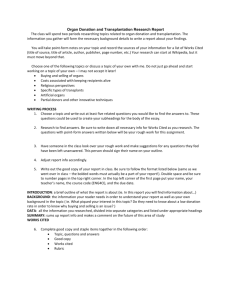
Table 1. Deceased or Brain Dead Patients Organ Transplantation Act
OT-equipped hospitals with written permission of MHME can use the healthy organs of dead patients or brain dead patients granted by
specialists. This is based on the patient’s will or his/her guardian’s agreement to be used in patients whose lives depend on OT.
1. Diagnosis of brain death shall be established by professional experts in a governmental university equipped hospital. Those experts
are appointed by the health minister for 4 years.
2. A member in the brain death diagnosis team should not be the members of the transplantation team.
3. Members of teams would not be entitled to pay diyyah (a fine to harm the body) in compensation for dismembering (or removal of
organ[s]) from the dead body.
Executive bylaw of this act should be prepared by MHME, judicial representative, in correlation with medical council and CFFSD during 3
months and approved by cabinet.
tation” was passed on April 6, 2000 by the Parliament27
(Table 1). Executive bylaw of this act was then passed by the
Cabinet Council on May 15, 200228 on a proposal made by
the Ministry of Health and Medical Education (MHME)29
(Table 2) in compliance with note 3 of above act.
In this regard, a protocol was approved by the MHME to
define criteria for the determination of brain death. According to this protocol, the clinical diagnosis of brain death
involves a neurologist, neurosurgeon, anesthesiologist or
internist, and a doctor from the forensic department. If
necessary (and in doubtful situations), the next stages of
approval of brain death are done by paraclinical standard
tests. In addition, all the necessary conditions for OT and
the patient’s will or approval by first-degree relatives are
mandatory for organ donation. The brain death form is
filled and signed by all 4 professional experts mentioned
above according to article 2 of the executive bylaw (Table 2)
and part 6 of the following protocol.
MHME BRAIN DEATH DETERMINATION PROTOCOL
1. Brain death definition: Brain death can be defined as
irreversibility of all brain function (cortical, subcortical,
and brain stem) synchronously according to clinical and
other parameters mentioned in code of conduct.
2. Conditions determining brain death:
A. Patient in deep coma with no evidence of central
nervous system (CNS) depressant usage, no evidence
of hypothermia (⬍32°C) as causative of coma, and
no evidence of metabolic, toxic, and endocrine disorders as causative of the patient’s coma.
B. Complete cessation of breathing and absence of
spontaneous respiration that cause certain need for a
ventilator. It is essential to exclude the usage of
relaxants (neuromuscular blocker agents) or other
drugs as the cause for respiratory failure.
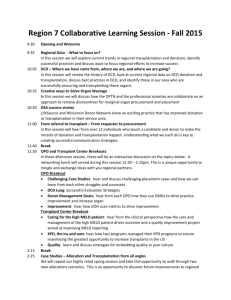
Table 2. Executive Bylaw of Deceased or Brain Dead Patients Organ Transplantation Act
1. Brain death consists of irreversible termination of cortical, subcortical, and brain stem functions. Brain death protocol should be
determined and notified by MHME within this regulation.
2. With this regulation, brain death diagnostic confirmation should be certified by 4 clinicians: a neurologist, a neurosurgeon, an
internalist, and an anesthesiologist.
2-1. Mentioned experts would be chosen and qualified by the minister of MHME for 4 years in any university equipped hospitals.
2-2. Each of the aforementioned clinicians should examine the patient, and complete and sign the special form individually. In the
case of complete agreement of 4 clinicians, brain death would be established.
2-3. It is necessary that the specific form should be confirmed by forensic consultants regarding their related responsibilities.
2-4. The brain death ascertainment and confirmation specific form should be designed by MHME and be accessible to brain death
diagnosis centers.
2-5. Confirmed diagnosis of brain death must be done in governmental university hospitals.
3. Team members of brain death diagnosis and confirmation must not be of the transplantation team.
4. All country hospitals are bound to report brain deaths to the TSDMC, so they can be confirmed by diagnosis team.
5. After confirmed brain death, the next steps will be followed if there is a patient’s will and guardian’s permission.
6. According to the law, the patient’s will with respect to OT could be either oral or in written form and can be approved by written
notice of an heir apparent. If the original will was not available, a special form designed by the MHME would be signed by informed
heirs.
7. The dead’s guardians are heirs apparent who are authorized to consent to OT. Heir’s permission is mandatory.
7-1. The dead’s guardian permission should be written and recorded.
7-2. The dead’s guardian written permission is the basis of evidence.
8. To conduct this code, necessary co-ordination would be done by TSDMC.
9. MHME will inform the MPO for providing expenses for OT (expenses of intensive care unit, cadaver transport, preparation and organ
transport, and organ operation) and educational matters. MPO will also provide necessary funds every year specifically from the
budget of the country.
10. According to the law and this code, other necessary orders would be issued and be communicated to relevant centers.
Abbreviations: MPO, Management and Planning Organization; TGDMC, Transplant and Specific Diseases Management Center.
.
2886
C. The cause of the coma has been defined as far as
possible.
3. Essential clinical evaluations are as follows: absence of
spontaneous movement and no responsiveness to the
hardest painful stimuli. Absence of brain stem reflexes
(Fixed pupils with no response to different levels of light
stimuli, absence of oculovestibular reflex [caloric test],
and absence of response in Gag test).
4. If necessary, clinical findings can be confirmed using
complementary paraclinical tests. First, positive apnea
test: giving 100% oxygen to the patient before separating
from a ventilator then giving 6 Lit/min O2 and letting the
PCO2 increase to 60 mm Hg. No signs of respiration
means a positive apnea test and confirms brain death.
Second, electroencephalograph (EEG) for 20 minutes
on 2 occasions at least 6 hours apart. Two occasions of
iso-electric EEG confirm brain death.
5. All clinical findings and tests should not change for 24
hours.
6. Clinicians determining brain death include 2 neurologists and/or 1 neurologist and 1 neurosurgeon who fill
out the form for brain death. They examine the patient
individually, then sign and stamp the brain death form.
This form should also be signed and stamped by an
anesthesiologist and a doctor from the forensic department after examining and assessing the patient.
Notes: (1) Children younger than 5 years should be kept for
at least 72 hours on the ventilator. (2) The responsible
clinician would start investigating brain death and ask for
medical consultation. (3) The special brain death form
should be completed for every brain death case and sent to
the Transplant and Specific Diseases Management Center
(TSDMC).
The TSDMC affiliated with MHME established the
Iranian Network for Organ Procurement to overcome the
absence of a registry. This central registry facilitates the
communication between referral hospitals, donors and recipients, and transplantation units, as well as handling the
training and research in this matter. A unique organ
donation informed consent was introduced by this network.
This form represents the written or verbal will or consent of
legal heirs of the heart or brain dead patients.
DISCUSSION
The practice of medical ethics is influenced by religion,
social and cultural background, or affiliation. The relevant
aspects of Islamic biomedical ethics can be reviewed in
different reports.9,30,31 Generally, the aim of Islamic medical ethics is to seek a compromise between Islamic custom
and the achievements of modern medicine, as long as basic
Islamic doctrine is not dishonored. Shia school of thought,
whose followers comprise about 15% of the world Muslims,
has historically developed its own jurisprudence and methodology of interpretations in many Islamic issues. However,
on the whole, its bioethical rulings do not differ fundamen-
AKRAMI, OSATI, AND ZAHEDI
tally and overlap with different Sunni schools of
thought.32,33
In the ethics of OT, lack of legislation was the main
problem in Iran.34 However, with the approval of the brain
death act, decree, and MHME protocol, the rate of OT has
increased significantly. OT from brain dead patients has
increased more compared with (“heart-lung”) cadavers.
This legislation has been drafted with consideration of
ethical issues in Iran and worldwide standards. The advantages of this legislation can be highlighted by the exact
definition of brain death, necessity of confirmation by 4
professional experts who are not from the transplantation
team, and emphasis on a consent form. It can contribute to
improving many ethical issues of OT. This legislation
facilitates signing organ donation cards and seeking approval from relatives of brain dead patients.
A minimum level of cultural awareness is a necessary
prerequisite for the delivery of care that is culturally
sensitive. Appreciation of the beliefs, perspectives, and
conceptual frameworks used by people are essential parameters when discussing medical ethics concerns. In this
regard, public awareness has increased recently and more
people have completed organ donation cards and agreed to
donate their organs in cases of brain death. This is also
reflected by an increased rate of OT from brain dead
patients in Iran.22 Because of their impact, the cultural
beliefs and knowledge of different population groups in
Iran regarding OT and brain death need further investigation.
A few additional points require clarification and necessitate revision of the current MHME protocol, including the
limitations of diagnosis and the definition of brain death at
university hospitals based on the precise definition of an
iso-electric EEG. For example, there are some patients with
defined clinical brain death for whom it is not always
possible to have 2 iso-electric EEGs. Clarification of this
point may define the legal status and the timely supply of
organs from a potential cadaver donor, which may not be
otherwise possible.
Renal transplantation first began in Iran with living
related donors (LRD) and later in 1988 as a controlled
program to procure kidneys from living unrelated donors
(LURD).22,35 The number of kidney donations from
LURD has steadily increased because of this program.
Although precise data in the country are unavailable, a
large recent renal transplantation study in Iran showed the
fraction of LURD versus LRD to be 84%.36 However, the
rate of cadaveric kidney transplantation has remained low
due to our respect for the corpse and the illegality of corpse
mutilation in Islamic culture. In the year 2002, although
1520 kidneys were transplanted from live donors, only 90
donations came from cadavers.
We conclude that public understanding of brain death
and cadaver organ donation needs further attention and
participation of media, scholars, physicians, nursing staff,
and leaders of society. We hope that the current legislation
BRAIN DEATH: IRAN
will contribute to increasing public awareness and the rate
of OT from cadaveric donors in Iran.
REFERENCES
1. Al Khader AA: The Iranian transplant programme: comment
from an Islamic perspective. Nephrol Dial Transplant 17:213, 2002
2. Cantrill SV: Brain death. Emerg Med Clin North Am 15:713,
1997
3. A definition of irreversible coma. Report of the Ad Hoc
Committee of the Harvard Medical School to Examine the Definition of Brain Death. JAMA 205:337, 1968
4. Report of the quality standards subcommittee of the American Academy of Neurology. Practice parameters for determining
brain death in adults. Neurology 45:1012, 1995
5. Jenkins DH, Reilly PM, Schwab CW: Improving the approach
to organ donation: a review. World J Surg 23:644, 1999
6. Razek T, Olthoff K, Reilly PM: Issues in potential organ
donor management. Surg Clin North Am 80:1021, 2000
7. Youngner SJ, Landefeld CS, Coulton CJ, et al: ‘Brain death’
and organ retrieval. A cross-sectional survey of knowledge and
concepts among health professionals. JAMA 261:2205, 1989
8. Rizvi A, Naqui A: Current issues and future problems in
transplantation in East Asia. Transplant Proc 33:2623, 2001
9. Aksoy S: A critical approach to the current understanding of
Islamic scholars on using cadaver organs without prior permission.
Bioethics 15:461, 2001
10. Ebrahim AF: Organ transplantation: contemporary Sunni
Muslim legal and ethical perspectives. Bioethics 9:291, 1995
11. Syed J: Islamic views on organ donation. J Transpl Coord
8:157, 1998
12. al Mousawi M, Hamed T, al Matouk H: Views of Muslim
scholars on organ donation and brain death. Transplant Proc
29:3217, 1997
13. Rohani M, Noghani F: Rulings regarding brain death. In:
Rohani M, Noghani F (eds): Ahkam-e Pezeshki. Tehran, Iran:
Teymurzadeh Cultural Publication Foundation; 1997, p 170
14. Third Conference of Islamic Jurists: Fiqh Academy Book of
Decrees. Decree No. 5. Amman, October 11–16,1986
15. el Shahat YI: Islamic viewpoint of organ transplantation.
Transplant Proc 31:3271, 1999
16. Khomeini SR: Rulings regarding brain death. In: Rohani M,
Noghani F (eds): Ahkam-e Pezeshki. Tehran, Iran: Teymurzadeh
Cultural Publication Foundation; 1997, p 174
2887
17. Khamene’i SA: Rulings regarding brain death. In: Rohani
M, Noghani F (eds): Ahkam-e Pezeshki. Tehran, Iran: Teymurzadeh Cultural Publication Foundation; 1997, p 175
18. Fazel Lankarani M: Available at: www.lankarani.org. Accessed July 1, 2004
19. Noori Hamedani H: Available at: www.noorihamedani.com.
Accessed July 4, 2004
20. Makarem Shirazi N: Available at: www.makaremshirazi.org.
Accessed July 5, 2004
21. Iranian Network for Organ Procurement: Available at:
http://www.irantransplant.org/farsi/. Accessed November 13, 2003
22. Ghods AJ: Renal transplantation in Iran. Nephrol Dial
Transplant 17:222, 2002
23. Ghods AJ, Ossareh S, Savaj S: Results of renal transplantation of the Hashemi Nejad Kidney Hospital--Tehran. Clin Transpl
16:203, 2000
24. Nafar M, Einollahi B, Sharifian M, et al: Renal transplantation in Iran. Transplant Proc 33:2649, 2001
25. Ghods AJ, Ossareh S, Khosravani P: Comparison of some
socioeconomic characteristics of donors and recipients in a controlled living unrelated donor renal transplantation program.
Transplant Proc 33:2626, 2001
26. Malek-hosseini SA, Salahi H, Lahsaee M, et al: Initial
experience with liver transplantation in Iran. Transplant Proc
35:375, 2003
27. IR Iran Parliament: Deceased or Brain Dead Patients OT
Act. H/24804-T/9929. June 4, 2000
28. IR Iran Cabinet Council: Executive Bylaw of Deceased or
Brain Dead Patients OT. H/24804-T/9929. May 15, 2002
29. MHME: Proposal of Executive Bylaw on Deceased or Brain
Dead Patients Organ Transplantation. 3730. June 18, 2001
30. Hedayat KM, Pirzadeh R: Issues in Islamic biomedical
ethics: a primer for the pediatrician. Pediatrics 108:965, 2001
31. Daar AS, al Khitamy AB: Bioethics for clinicians: 21. Islamic
bioethics. CMAJ 164:60, 2001
32. Rahman F: Legacy and Prospects. In Islam, 2nd ed. Chicago:
Chicago University Press; 1979, p 235
33. Kamali MH. Urf (custom). Principles of Islamic Jurisprudence. Cambridge: Islamic Texts Society; 1991, p 283
34. Zali MR, Shahraz S, Borzabadi SH: Bioethics in Iran:
legislation as the main problem. Arch Iranian Med 5:136, 2002
35. Simforoosh N, Bassiri A, Amiransari B, et al: Livingunrelated renal transplantation. Transplant Proc 24:2421, 1992
36. Porooshani A, Porooshani F, Ghods AJ: Results of 1020
renal transplants single-center experience. Transplant Proc 33:
2644, 2001