(POEM) and Laparoscopic Heller Myotomy
advertisement
 and Laparoscopic Heller Myotomy")
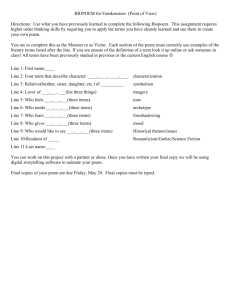
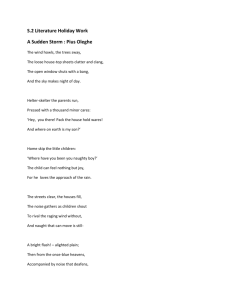
J Gastrointest Surg DOI 10.1007/s11605-012-2030-3 2012 SSAT QUICK SHOT PRESENTATION Comparison of Perioperative Outcomes Between Peroral Esophageal Myotomy (POEM) and Laparoscopic Heller Myotomy Eric S. Hungness & Ezra N. Teitelbaum & Byron F. Santos & Fahd O. Arafat & John E. Pandolfino & Peter J. Kahrilas & Nathaniel J. Soper Received: 24 July 2012 / Accepted: 27 August 2012 # 2012 The Society for Surgery of the Alimentary Tract Abstract Background Peroral esophageal myotomy (POEM) is a novel endoscopic operation for the treatment of achalasia. Few POEM outcome data exist, and no study has compared POEM with the surgical standard, laparoscopic Heller myotomy (LHM). Methods Perioperative outcomes were compared between POEM and LHM performed in a nonrandomized fashion. Patients in both groups met the following eligibility criteria: diagnosis of achalasia, age 18–85, and absence of prior achalasia treatment. Results Eighteen patients underwent POEM, and 55 patients underwent LHM. Operative times were shorter for POEM (113 vs. 125 min, p<.05), and estimated blood loss was less (≤10 ml in all cases vs. 50 ml, p<.001). Myotomy lengths, complication rates, and length of stay were similar. Pain scores were similar upon post-anesthesia care unit arrival and on postoperative day 1 but were higher at 2 h for POEM patients (3.5 vs. 2, p0.03). Narcotic requirements were similar, although fewer POEM patients received ketorolac. POEM patients’ Eckardt scores decreased (median 1 postop vs. 7 preop, p<.001), and 16 (89 %) patients had a treatment success (score ≤3) at median 6-month follow-up. Six weeks after POEM, routine follow-up manometry and esophagram showed normalization of esophagogastric junction pressures and contrast column heights. Conclusions POEM and LHM appear to have similar perioperative outcomes. Further investigation is needed regarding long-term results after POEM. Keywords Achalasia . Peroral endoscopic myotomy . Laparoscopic Heller myotomy . Natural orifice transluminal endoscopic surgery This study was presented at DDW: SSAT Quick Shots Session I on May 21, 2012. E. S. Hungness (*) : E. N. Teitelbaum : B. F. Santos : F. O. Arafat : N. J. Soper Department of Surgery, Northwestern University Feinberg School of Medicine, 676 North Saint Clair Street, Suite 650, Chicago, IL 60611, USA e-mail: ehungnes@nmh.org E. N. Teitelbaum Department of Surgery, George Washington University, Washington, DC, USA J. E. Pandolfino : P. J. Kahrilas Division of Gastroenterology and Hepatology, Northwestern University Feinberg School of Medicine, Chicago, IL, USA Introduction Achalasia is an idiopathic disease of esophageal physiology, characterized by the manometric findings of absent peristalsis and a failure of esophagogastric junction (EGJ) relaxation upon swallowing. Achalasia results in progressively severe dysphagia for solids and liquids, and can additionally cause regurgitation, aspiration, chest pain, weight loss, and eventually an irreversible dilatation of the esophageal body.1 Current primary treatment options include surgical myotomy across the EGJ [laparoscopic Heller myotomy (LHM)] and endoscopic pneumatic dilation of the EGJ, with a recent randomized trial suggesting similar efficacy between the two procedures at 2-year follow-up.2 However, substantial evidence suggests that LHM provides the most durable symptom relief, without the need for repeat interventions, as is often necessary with endoscopic dilation.3–5 Peroral esophageal myotomy (POEM) has recently been introduced as a novel endoscopic operation for the treatment J Gastrointest Surg of achalasia. POEM incorporates concepts of natural orifice transluminal endoscopic surgery6 and expands upon techniques used in endoscopic submucosal dissection7 in order to achieve a division of the esophageal circular muscle fibers across the EGJ and onto the stomach. As a result, POEM incorporates the theoretical advantages of both endoscopic dilation (no skin incisions, decreased pain, and less blood loss) and LHM (durable surgical myotomy and single procedure). A submucosal esophageal myotomy was first described in an animal model by Pasricha and colleagues,8 and POEM was first translated into clinical practice by Dr. Haru Inoue, reported with colleagues in their landmark paper in 2010.9 Since that time, several small, single-institution POEM case series have shown perioperative safety and excellent shortterm outcomes in terms of symptom resolution and improvement in EGJ physiology.10–12 However to date, no study has directly compared POEM with the surgical standard of care, LHM. In this study, we compare perioperative outcomes between POEM and LHM performed at a single institution in a nonrandomized fashion. Additionally, we present shortterm symptom and physiologic outcomes from our initial POEM experience. Methods Patient Eligibility and Preoperative Evaluation POEM procedures were performed at a single institution under a Northwestern Institutional Review Board (IRB)approved study protocol. Patients referred for treatment of achalasia were counseled regarding the existing treatment options (endoscopic botulinum toxin injection, endoscopic pneumatic dilation, LHM, and POEM) and elected to undergo POEM. Patients undergoing POEM in this study met the following eligibility criteria: diagnosis of achalasia confirmed by manometry, age 18–85, absence of prior treatment (either endoscopic or surgical) for achalasia, and absence of sigmoid esophagus. POEM procedures were performed conjointly by the primary and senior authors. All POEM cases performed up until the time of data analysis were included, so this series represents the initial learning curve of the authors. All patients signed a written consent for the procedure and outcomes data collection. The control group for this study was comprised of patients who had undergone LHM at the same institution by the same two surgeons, and who had enrolled in a prospective outcomes database begun in 2004 under an IRB-approved study protocol. Only LHM patients meeting the same eligibility criteria preoperatively as the POEM patients (diagnosis of achalasia, age 18–85, no prior achalasia treatment, and absence of sigmoid esophagus) were included for comparison. Preoperatively, patients in both groups were evaluated with a history and physical examination, upper endoscopy, timed barium esophagram (TBE), and high-resolution manometry (HRM). TBE was performed using a 200-ml oral bolus of low-density barium, with radiographs taken at 1, 2, and 5 min after swallowing. HRM was performed using a previously described technique13 and interpreted according to the Chicago Classification of esophageal pressure topography.14 The following patient demographics were also recorded prospectively: age, body mass index (BMI), and American Society of Anesthesiologists (ASA) Physical Classification status. An Eckardt symptom score15 (which measures frequency of dysphagia, regurgitation and chest pain, and amount of weight loss, each on a scale of 0–3 resulting in a total scale of 0–12 with higher scores indicating more severe disease) was recorded preoperatively for POEM patients, but was not included in the symptom surveys given to LHM patients. POEM Operative Technique POEM was performed in a fashion similar to that described by Inoue and colleagues.9 Patients are kept on a clear liquid diet for 48 h preoperatively and complete a 5-day course of oral liquid nystatin for candida prophylaxis (added to our protocol starting with patient #9). POEM is performed under general anesthesia with endotracheal intubation and muscle paralysis. Patients are positioned supine with the left arm tucked at the side and the right arm abducted. The patient’s systolic blood pressure is kept below 100 mmHg throughout the procedure if possible. An initial upper endoscopy is performed using a singlechannel, high-definition flexible gastroscope (GIF-H180 gastroscope; Olympus America, Inc., Center Valley, PA) with carbon dioxide (CO2) insufflation. The esophagus and stomach are aspirated of any residual fluid, and the stomach is desufflated. The endoscope is then fitted with a transparent oblique dissecting cap, and the distance from the incisors to EGJ is measured on the scope shaft. Approximately 10 ml of solution containing indigo carmine (0.2 mg/ ml), epinephrine (5 mcg/ml), and 0.9 % saline is then injected into the anterior esophageal wall 14 cm proximal to the EGJ to form a submucosal bleb. A triangle-tip (TT) endoscopic cautery knife (Triangle Tip Knife; Olympus) is used to make a longitudinal mucosotomy over the site of the fluid bleb, and the scope is maneuvered into the submucosal space. A combination of blunt dissection and electrocautery with the TT knife is then used to create an anterior submucosal tunnel extending at least 3 cm caudal to the EGJ. Additional indigo carmine solution is sequentially injected to mark progression of the tunnel, as well as to aid in hydrodissection and hemostasis. Once the submucosal tunnel is completed, the endoscope is withdrawn from the J Gastrointest Surg tunnel and advanced into the gastric lumen to ensure that indigo carmine dye is visible in the stomach submucosa, at least 3 cm distal to the EGJ. If it is not, the submucosal dissection is extended caudally. A selective myotomy of only the inner, circular muscle layer is then begun using the TT knife to lift and divide individual fibers. A starting point is chosen several centimeters distal to the caudal extent of the mucosotomy, and the myotomy is carried past the EGJ to the distal end of the submucosal tunnel. After completing the myotomy, the scope is reintroduced into the true esophageal lumen to evaluate the effect of the myotomy on EGJ patency. After the myotomy is deemed to be satisfactory, the submucosal tunnel is irrigated with bacitracin solution, and the mucosotomy is closed with endoscopic clips (QuickClip; Olympus). Postoperatively, patients are extubated and transferred to the post-anesthesia care unit (PACU). Patients are kept nil per os (NPO) on the night of surgery and receive standing intravenous (IV) antiemetics and pain medication as needed. On the morning of postoperative day (POD) 1, patients undergo a contrast esophagram. If there is no evidence of leak and adequate passage of contrast past the EGJ, patients are started on a clear liquid diet for breakfast and, if tolerated, advanced to full liquids for lunch. If progressing as expected, patients are discharged home on the afternoon of POD #1. A full liquid diet is maintained for 2 weeks and then gradually liberalized to include soft and solid foods. LHM Operative Technique Our technique for LHM has previously been described in detail.16 Briefly, after establishing a pneumoperitoneum, five trocars are placed. The phrenoesophageal ligament is divided, and the diaphragmatic crura are opened. The anterior mediastinal esophagus is dissected free from the surrounding structures, and the short gastric vessels are divided to mobilize the fundus. The anterior gastric fat pad and anterior vagus nerve are dissected free from the stomach and esophagus, and a myotomy of both muscle layers is performed using a combination of blunt and electrocautery dissection to at least 6 cm proximal and 2 cm distal to the EGJ. After endoscopic visualization of the EGJ to confirm adequacy of the myotomy and check for leak, an antireflux procedure is performed. We prefer a posterior Toupet fundoplication, unless an excessive anterior angulation of the EGJ results or if there is concern for esophageal perforation, in which case an anterior Dor fundoplication is performed. Postoperatively, patients are given standing IV antiemetics and pain medication as needed. They are allowed clear liquids on the day of surgery and advanced to soft diet the morning after if progressing as expected. An esophagram is not routinely performed, and patients are typically discharged home on the afternoon of POD #1 and maintained on a soft diet for 2 weeks. Perioperative Data Collection For both groups, the following intraoperative data were collected prospectively: operative time (from initial endoscope insertion to final endoscope withdrawal for POEM, and initial skin incision to final skin closure for LHM), estimated blood loss (EBL), myotomy length, and complications. POEM myotomy lengths were measured by subtracting the length on the endoscope shaft from the incisors to the proximal myotomy edge from the shaft length from incisors to the distal myotomy edge. LMH myotomy lengths were measured using the distance between the open jaws of a Hunter grasper (2.5 cm) as a ruler. Postoperatively, hospital length of stay and 30-day mortality and complications were recorded prospectively. Pain scores (scale 0–10) at PACU arrival, 2-h postoperatively, and on the morning (8 am) of POD #1 were obtained from nursing assessment records. Narcotic administration was derived from the medication administration record and converted into IV morphine equivalents for comparison. Follow-up Physiologic Studies and Symptom Scores At 6 weeks postoperatively, POEM patients underwent perprotocol HRM and TBE. Follow-up upper endoscopy was performed at the discretion of each patient’s gastroenterologist at variable time intervals, or as indicated by postoperative symptoms. POEM patients were contacted via telephone every 3 months postoperatively to assess for complications and to obtain a current Eckardt score. An Eckardt score ≤3 was considered a therapeutic success.2 Symptomatic gastroesophageal reflux (GER) was assessed in POEM patients every 3 months postoperatively using the GerdQ questionnaire.17 A score ≥7 (scale 0–18) was considered positive for GER, in line with established usage of the questionnaire. LHM patients did not have routine shortterm physiologic follow-up studies, postoperative Eckardt, or GerdQ scores. Statistical Analysis SPSS software (version 20; IBM, Armonk, NY) was used for data analysis. Continuous and ordinal variables were compared between groups using a Mann–Whitney U test. Paired variables in the same patient before and after surgery were compared using a Wilcoxon signed-rank test. Categorical variables were compared using a Fisher exact test. A two-tailed p value <.05 was considered statistically significant in all cases. Data are presented throughout as median (minimum– maximum). J Gastrointest Surg Results From August 2010 to May 2012, 18 patients underwent POEM and from March 2004 to May 2012, 55 patients meeting the same eligibility criteria underwent LHM (60 patients who underwent LHM during the same time period were excluded because they had received prior treatment, had a sigmoid esophagus, or were <18 or >85 years old). Gender distribution, BMI, ASA classification, and duration of symptoms were all similar between groups (Table 1). POEM patients were younger [38 (22–69) vs. 49 (22–79) years, p0.03]. On preoperative HRM, 4-s integrated relaxation pressures (IRP), nadir relaxation pressures, and achalasia subtype distribution were similar between groups, but POEM patients had lower expiratory EGJ resting pressures [19 (7–51) vs. 30 (8–60), p0.02]. Operative times were slightly shorter for POEM [113 (88–220) vs. 125 (90–195)min, p<.05), and EBL was less [≤10 ml in all cases vs. 50 (10–250)ml, p<.001). Myotomy lengths were similar between groups (Table 2). In the POEM cases, nine (7–17) clips were required to close the mucosotomy, and Veress needle decompression of the pneumoperitoneum was required intraoperatively in seven (39 %) cases. Two POEM cases were initially aborted after endoscopy revealed esophageal candidiasis. These patients completed a course of oral nystatin and had a subsequent upper endoscopy to confirm resolution of candidiasis prior to undergoing POEM. No mortalities and one major complication (Clavien– Dindo18 grade IIIb) occurred in both groups. A POEM patient had a contained perforation at the level of the EGJ. Table 1 Preoperative patient demographics Number Female Median (range) age BMI (kg/m2) ASA classification I II The bolded value represents statistical significance III Duration of symptoms (years) Preoperative HRM Basal expiratory pressure (mmHg) 4-s IRP (mmHg) Nadir relaxation pressure (mmHg) Achalasia subtype I II III The patient was non-compliant with NPO orders and ate solid food on the night of her operation. She developed retching and abdominal pain on postoperative day 1, and an esophagram revealed a contained perforation at the EGJ. She was taken back to the operating room where endoscopy and laparoscopy failed to demonstrate a discrete esophageal defect, and drains were placed. She initially recovered well, but went on to develop recurrent dysphagia over the next several months, potentially due to scarring as a result of the perforation. A LHM patient had an esophageal perforation that required bilateral thoractomy for drainage and repair. He complained of dyspnea on POD #2, and a CT scan of the chest showed a right lung consolidation and pneumomediastinum but no esophageal leak. He was treated for presumed aspiration pneumonia, but his symptoms persisted, and a repeat CT scan revealed extravasation of contrast from the distal esophagus and large right-sided pleural effusion. The patient was taken to the operating room, and a right-sided thoracotomy was performed to debride the right chest and repair the leak. However, an anterior perforation was found that was not entirely accessible from the right chest, so a left thoracotomy was then performed for primary esophageal repair with a reinforcing intercostal muscle flap. The patient recovered after a 19-day hospitalization. Three (17 %) minor complications (Clavien–Dindo grade I) occurred in the POEM group and seven (13 %) in the LHM group (p0ns; listed in Table 2). The median length of stay was 1 day in both groups. Pain scores were similar upon PACU arrival and on the morning of POD #1 but were higher at 2 h in POEM patients [3.5 (0–8) vs. 2 (0–10), scale 0–10, p 0.03). Narcotic POEM LHM 18 5 (28 %) 38 (22–69) 25 (19–45) 55 26 (47 %) 49 (22–79) 27 (17–48) 2 (11 %) 12 (67 %) 4 (7 %) 39 (71 %) 4 (22 %) 1 (0.13–30) 12 (22 %) 1.25 (0.25–15) 19 (7–51) 23 (10–59) 19 (9–52) 30 (8–60) 26 (10–70) 19 (9–62) 33 % 61 % 6% 20 % 77 % 3% p value .18 .03 .86 .95 .54 .02 .84 .87 .48 J Gastrointest Surg Table 2 Perioperative outcomes Median (range) operative time (min) Myotomy length (cm) EBL (ml) Clips required to close mucosotomy Veress needle decompression of pneumoperitoneum Major complications (grade IIIb) Minor complications (grade I) The bolded value represents statistical significance Length of stay (days) requirements were similar between groups, although fewer POEM patients received IV ketorolac (28 vs. 80 %, p<.001; Table 3). Sixteen POEM patients had per-protocol HRM at 6 weeks postoperatively. Resting expiratory EGJ pressures decreased to normal median values [pre 19 (7–51)mmHg vs. post 9 (0–23)mmHg, p<.001) as did IRP [pre 21 (10–59)mmHg vs. post 12 (6–18)mmHg, p<.001; Fig. 1]. Thirteen POEM patients completed follow-up TBE at 6 weeks, with significantly decreased column heights at 1, 2, and 5 min on their postoperative studies [pre 17 (9–31), 16 (9–31), and 14 (0–31) cm vs. post 7 (0–15), 5 (0–13), and 0 (0–9) cm, p≤.001; Fig. 2]. Postoperative upper endoscopy was performed on 15 POEM patients at a median follow-up interval of 1.5 (1.5–12)months. Esophagitis was present in five (33 %) patients (Los Angeles class A, 2; B, 2; C, 1). Among POEM patients, Eckardt scores (scale 0–12) decreased from 7 (5–12) preoperatively to 1 (0–9; p<.001) at median 6 (range, 1–18) month follow-up. Symptomatic recurrence (defined as an Eckardt score ≥4 at any time point) occurred in two (11 %) POEM patients: the patient in whom the contained leak occurred and the first patient in POEM LHM p value 113 (88–220) 9 (6–14) ≤10 in all cases 9 (7–17) 7 (39 %) 125 (90–195) 8.5 (7–10) 50 (10–250) – – <.05 .18 <.001 1 (6 %) - Esophageal perforation 3 (17 %) - Subcutaneous emphysema - Atrial fibrillation - Urinary retention 1 (2 %) - Esophageal perforation 7 (13 %) - Anterior vagus nerve division - Splenic capsule tear - Aspiration - Atrial fibrillation - Urinary retention ×2 - Readmission for chest pain 1 (1–19) 1 (1–13) .71 .63 our series. Both patients were subsequently successfully salvaged with a LHM. Four (22 %) POEM patients had a GerdQ score ≥7, indicating symptomatic GER, at the same follow-up interval. Seven (39 %) patients had either esophagitis on endoscopy or a GerdQ score ≥7: two patients had both esophagitis on EGD and a GerdQ ≥7, two patients had a GerdQ ≥7 but EGDs negative for esophagitis, and three patients were asymptomatic (i.e., GerdQ06) but had esophagitis on EGD. Discussion This study adds to the existing evidence that POEM is a feasible and safe procedure for creating an endoscopic myotomy in patients with treatment-naïve achalasia. Additionally, POEM appears to have perioperative outcomes on par with those of the surgical standard of care, LHM. During this, our initial learning curve, the POEM procedure created myotomies of similar length with slightly shorter operative times when compared with LHM. Shorter operative times, along with markedly reduced EBL and the absence of skin Table 3 Postoperative pain scores and pain medication usage The bolded value represents statistical significance .45 Median (range) pain score on PACU arrival (scale 0–10) Pain score at 2 h Pain score on POD #1 Narcotics on day of surgery (mg morphine equivalents) Narcotics on POD #1 Number of patients receiving ketorolac POEM LHM p value 2.5 (0–9) 3.5 (0–8) 1.5 (0–8) 8.5 (0–36) 2.5 (0–21) 5 (28 %) 2 2 2 6.7 3.3 44 .76 .03 .71 .18 .85 <.001 (0–9) (0–10) (0–10) (0–31.4) (0–18) (80 %) J Gastrointest Surg Fig. 1 POEM patients’ pre- and 6-week postoperative high-resolution manometry results (n016) incisions, all reinforce the concept that POEM is a less invasive procedure than LMH. However, the advantages of POEM in terms of operative time and EBL were small, and it is unknown whether these differences will translate into any concrete clinical benefits for patients. We found similar intra- and perioperative complication rates between the two procedures, providing initial evidence Fig. 2 POEM patients’ pre- and 6-week postoperative timed barium esophagram results (n013) that POEM has a safety profile comparable with LHM. One contained esophageal perforation occurred at the level of the EGJ in a patient who was non-compliant with NPO orders and ate solid food on the night of her operation. It is unclear whether this perforation was the result of food impaction or if it would have manifested radiographically and/or clinically regardless of adherence to postoperative protocol. Although we have had no radiographic or clinically apparent leaks at the site of the mucosotomy clip closure, we are still extremely cautious when advancing a patient’s diet after POEM. All patients are kept strictly NPO on the night of surgery and are only given liquids after a contrast esophagram is negative for leak. While postoperative care of these patients may liberalize after a large enough collective experience demonstrates the security of mucosotomy clip closure, at present, we do not envision POEM being safely performed as an outpatient, or “same-day,” procedure. One other complication specific to POEM occurred in a patient who developed subcutaneous emphysema postoperatively. This resolved spontaneously without sequelae, but the patient required an additional day of hospitalization for pain control and observation. Although the aim during POEM is to leave the layer of longitudinal muscle fibers intact, some degree of pneumomediastinum, and potentially pneumoperitoneum, pneumothorax, and/or subcutaneous emphysema, will likely result regardless of technique. The largest published POEM series to date, by Ren and colleagues, highlights some of these POEM-specific complications.19 In their series of 119 cases, 23 % of patients developed subcutaneous emphysema intraoperatively and an additional 56 % postoperatively. Three of these patients required treatment with subcutaneous needle decompression. Additionally, 3 % of their patients developed a pneumothorax intraoperatively and another 25 % postoperatively. A routine chest CT scan was performed on POD #1 which may have detected some clinically insignificant pneumothoraces; however, 17 patients (14 % of the total series) required chest tube decompression, bilaterally in 4 cases. These data underscore the points that CO2 (as opposed to room air) scope insufflation should be used throughout POEM and that any intra- or postoperative hemodynamic decompensation should be treated as a tension pneumothorax until proven otherwise. Interestingly, no patients in the above series required intraoperative decompression for pneumoperitoneum, as opposed to our experience in which seven (39 %) patients required abdominal Veress needle placement, but no pneumothoraces occurred at any time point. We hypothesize that this may be due to the fact that Ren et. al. perform their submucosal dissection in the posterior wall of the esophagus, which may predispose to pneumothorax, whereas an anterior tunnel (our approach) may result in a relatively increased incidence of pneumoperitoneum. J Gastrointest Surg In the immediate postoperative period, POEM appears to result in levels of pain comparable with LHM. In fact, pain scores were slightly higher in POEM patients at the 2-h time point. Inpatient narcotic usage was similar on both the day of surgery and POD #1, although fewer POEM patients received ketorolac postoperatively (28 vs. 80 %, p<.001) due to concern for bleeding in the submucosal tunnel. We hypothesize that this discrepancy was partially responsible for their higher 2-h pain scores. The first several patients in our series were given standing ketorolac, but we discontinued its usage in subsequent patients after encountering bleeding during submucosal dissection in early cases and based on an anecdotal report from another institution that a submucosal hematoma had caused dysphagia in a POEM patient postoperatively. The safety of postoperative ketorolac in POEM patients has yet to be conclusively determined. In terms of symptomatic efficacy, POEM patients had significantly decreased Eckardt scores to a median score of 1, and our therapeutic success rate (i.e., Eckardt score ≤3) was 89 % at median 6-month follow-up. This is in line with previously published POEM outcomes,9,10,12 as well as historic data from well-designed LHM trials.2,20 The two patients with symptomatic recurrences both underwent subsequent LHM. During these operations, an anterior myotomy was performed, in a similar fashion to which we would approach a reoperation after a failed Heller myotomy. In both cases, some mild adhesions were encountered when initially establishing the plane between esophageal muscularis and submucosa. However, there was no mediastinal inflammation, and once the correct plane was entered, the myotomies proceeded as normal. Both of these reoperations resulted in symptom resolution, providing initial evidence that LHM can be used as a salvage procedure in patients who develop recurrent dysphagia after POEM. Successful endoscopic dilation after failed POEM has also been reported10 and may serve as an alternative treatment modality to salvage these patients. On short-term follow-up HRM, POEM appears to result in a normalization of EGJ pressures. Both IRP and resting expiratory EGJ pressures were significantly reduced at 6 weeks postoperatively (Fig. 1). This mirrors the findings of prior series, which have shown significant improvements in EGJ physiology after POEM.9,10,12 TBE contrast column heights also normalized on postoperative studies, further supporting the concept that POEM results in improved functional bolus passage through the EGJ (Fig. 2). As opposed to LHM, POEM does not include an antireflux procedure, which could potentially result in increased rates of GER postoperatively. Conversely, preservation of the longitudinal muscle fibers and avoidance of dissection and repair of the diaphragmatic crura may help prevent GER after POEM. In our series, 33 % of patients who had postoperative upper endoscopies had evidence of esophagitis; however, only four patients (22 % of the overall series) had symptomatic GER, as defined by a GerdQ score ≥7. All were started on a proton pump inhibitor (PPI), and their long-term outcomes in terms of symptoms, resolution of esophagitis, and PPI dependence have yet to be determined. The LMH literature is extremely variable in terms of postoperative GER, with incidences of abnormal acid exposure on 24-h pH studies ranging from 3 to 42 %,2,20–22 which may be a function of differences in fundoplication construction and operator experience. An important research objective in our, and other, POEM series going forward will be the systematic administration of 24-h pH studies at longer follow-up intervals as no such data after POEM have been published to date. Our study has several limitations. Most importantly, patients were not randomized to treatment modality. This may have resulted in differences in baseline characteristics between groups, as is evidenced by the fact that LHM were older and had higher baseline resting expiratory EGJ pressures on preoperative HRM. Beginning in August 2010, all patients who met the eligibility criteria were offered pneumatic dilation, LHM, or POEM as treatment options. LHM was described to patients as the surgical standard of care and POEM as a novel procedure under investigation with limited outcomes data. Anecdotally, approximately 75 % of patients who qualified for both operations chose POEM. As a result, patient selection bias may have created additional unrecognized differences between the treatment groups. Additionally, PACU and ward nurses were not blinded to treatment group, which could potentially introduce bias into recorded pain scores and the amount of pain medication administered “as needed.” All patients in this series were treatment naïve, and although POEM after endoscopic therapy (botulinum toxin injection and/or dilation) has been described,10–12,19 further investigation is needed regarding the effects of prior treatment on POEM safety and efficacy. Additionally, this study represents our initial experience with POEM in a clinical setting, and post-learning curve results may differ significantly. Ideally, a multi-institution randomized trial comparing POEM and LHM should be conducted to more conclusively address these research questions. In conclusion, this study adds to the existing evidence that POEM is a feasible and safe procedure for primary treatment of achalasia. POEM results in an equally long myotomy as LHM, but with slightly shorter operative times and lower EBL. POEM does not appear to result in less pain postoperatively than LHM, and narcotic requirements are similar. At short-term follow-up, POEM results in significant improvement of EGJ physiologic function as measured by HRM and TBE. Further data are required regarding longterm symptomatic and physiologic outcomes in terms of both esophageal function and GER after POEM. J Gastrointest Surg Acknowledgments The authors would like to acknowledge Remedios Manuel, R.N., Colleen Krantz, R.N., and Meghan Thompson for their help coordinating the clinical aspects of the study. Disclosures Olympus America, Inc. granted instruments used during the POEM procedures, but was not involved in the study design, data collection, analysis, or manuscript preparation. John E. Pandolfino has consulting agreements with Given Imaging and Crospon. Nathaniel J. Soper is on the scientific advisory boards of TransEnterix and Miret Surgical. Eric S. Hungness, Ezra N. Teitelbaum, Byron S. Santos, Fahd O. Arafat, and Peter J. Kahrilas have no conflicts of interest or financial ties to disclose. References 1. Francis DL, Katzka DA. Achalasia: update on the disease and its treatment. Gastroenterology 2010;139:369–74. 2. Boeckxstaens GE, Annese V, des Varannes SB, et al. Pneumatic dilation versus laparoscopic Heller’s myotomy for idiopathic achalasia. The New England journal of medicine 2011;364:1807–16. 3. Patti MG, Pellegrini CA. Esophageal achalasia 2011: pneumatic dilatation or laparoscopic myotomy? Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 2012;16:870–3. 4. Kostic S, Kjellin A, Ruth M, et al. Pneumatic dilatation or laparoscopic cardiomyotomy in the management of newly diagnosed idiopathic achalasia. Results of a randomized controlled trial. World journal of surgery 2007;31:470–8. 5. Campos GM, Vittinghoff E, Rabl C, et al. Endoscopic and surgical treatments for achalasia: a systematic review and meta-analysis. Annals of surgery 2009;249:45–57. 6. Rattner D, Kalloo A, Group ASW. ASGE/SAGES Working Group on Natural Orifice Translumenal Endoscopic Surgery. October 2005. Surgical endoscopy 2006;20:329–33. 7. Othman MO, Wallace MB. Endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) in 2011, a Western perspective. Clinics and research in hepatology and gastroenterology 2011;35:288–94. 8. Pasricha PJ, Hawari R, Ahmed I, et al. Submucosal endoscopic esophageal myotomy: a novel experimental approach for the treatment of achalasia. Endoscopy 2007;39:761–4. 9. Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy (POEM) for esophageal achalasia. Endoscopy 2010;42:265–71. 10. von Renteln D, Inoue H, Minami H, et al. Peroral endoscopic myotomy for the treatment of achalasia: a prospective single center study. The American journal of gastroenterology 2012;107:411–7. 11. Swanstrom LL, Rieder E, Dunst CM. A stepwise approach and early clinical experience in peroral endoscopic myotomy for the treatment of achalasia and esophageal motility disorders. Journal of the American College of Surgeons 2011;213:751–6. 12. Costamagna G, Marchese M, Familiari P, Tringali A, Inoue H, Perri V. Peroral endoscopic myotomy (POEM) for oesophageal achalasia: Preliminary results in humans. Digestive and Liver Disease 2012;44(10):827-32. 13. Pandolfino JE, Kwiatek MA, Nealis T, Bulsiewicz W, Post J, Kahrilas PJ. Achalasia: a new clinically relevant classification by high-resolution manometry. Gastroenterology 2008;135:1526–33. 14. Bredenoord AJ, Fox M, Kahrilas PJ, et al. Chicago classification criteria of esophageal motility disorders defined in high resolution esophageal pressure topography. Neurogastroenterology and motility : the official journal of the European Gastrointestinal Motility Society 2012;24 Suppl 1:57–65. 15. Eckardt VF. Clinical presentations and complications of achalasia. Gastrointestinal Endoscopy Clinics of North America 2001; 11: 281–92, vi. 16. Vaziri K, Soper NJ. Laparoscopic Heller myotomy: technical aspects and operative pitfalls. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 2008;12:1586–91. 17. Jones R, Junghard O, Dent J, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Alimentary pharmacology & therapeutics 2009;30:1030–8. 18. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Annals of surgery 2004;240:205–13. 19. Ren Z, Zhong Y, Zhou P, et al. Perioperative management and treatment for complications during and after peroral endoscopic myotomy (POEM) for esophageal achalasia (EA) (data from 119 cases). Surgical Endoscopy 2012. doi:10.1007/ s00464-012-2336-y 20. Rawlings A, Soper NJ, Oelschlager B, et al. Laparoscopic Dor versus Toupet fundoplication following Heller myotomy for achalasia: results of a multicenter, prospective, randomized-controlled trial. Surgical endoscopy 2012;26:18–26. 21. Rebecchi F, Giaccone C, Farinella E, Campaci R, Morino M. Randomized controlled trial of laparoscopic Heller myotomy plus Dor fundoplication versus Nissen fundoplication for achalasia: long-term results. Annals of surgery 2008;248:1023–30. 22. Novais PA, Lemme EM. 24-h pH monitoring patterns and clinical response after achalasia treatment with pneumatic dilation or laparoscopic Heller myotomy. Alimentary pharmacology & therapeutics 2010;32:1257–65.