the significance of the trendelenburg test
advertisement

THE
SIGNIFICANCE
OF
PHILIP
test
least
four methods
We examined
order to determine
enabled
method
The
responses
1897
a standard
hip abductor
that
method
of performing
function.
pitfalls
from
result
the patient,
and impingement
from the patient
using muscles
Friedrich
result
in misinterpretation,
Trendelenburg
of the
(Rang
1966).
only
two
described
other
hip
and
progressive
Trendelenburg’s
years
at a time
after
the discovery
the
physician
than
his
ears,
eyes,
in
most
textbooks
a test
major
methods
little
of
and
leg,
and
performing
among
the
our
Requests
and
pitfalls
test
its muscles
of the
should
1985 British
Editorial
0301
620X855150S2.00.
67 B. No.
pain,
lack
as a
of co-
False-negative
beyond
the hip
out
in
of the hip.
at least four dif-
Trendelenburg
it was seldom
Furthermore,
colleagues
test,
clear
there
how
was
the
per-
about
most
ofit
of
on
of this confusion
as to
of the test, we decided
to
were,
to the
first,
request
to
test
in order
as used
record
to stand
to assess
in current
FRACS.
Senior
Lecturer
in Orthopaedic
MD.
FRACS.
Professor
ofOrthopaedic
II Medical
Centre,
Nedlands.
Western
reprints
the test
is men-
Positive
Negative
Trendelenburg’s
the
on
These
drawings
tive and negative
and the alignment
( From
Mercer
Siga
5. NOVEMBER
he sent
Society
to Professor
of Bone
and
SUBJECTS
Surgery
Surgery
Australia
6009.
Surgery
--1985
volunteers.
A group
3 and 50 years were
of 50 normal
people
examined
to determine
happened
to their posture
when
they
Two
positions
of the non-stance
leg
the test was performed
with the hip
then it was repeated
with
son was asked
to maintain
S. M. L.Nade.
Joint
I
demonstrate
what
Trendelenburg
described
as a posisign.
Note
that both
hands
are held by an assistant
of the pelvis
with respect
to the ground
is observed.
Rang’s
Ani/zologt’
n/orthopaedics,
with permission).
the value
orthopaedic
Normal
between
for
are
Fig.
I
VOL.
responses,
between
the rib cage
and the iliac crest.
above and below the pelvis, and from leaning
and hence
to define
a standard
Trendelenburg
second,
to study people
with various
abnormali-
P. 1-1. 1-Iardcastle,
S. M. L. Nade.
Queen
Elizabeth
to interpret
physiotherapy
of the test, although
out their own version
aims
of this study
of normal
people
ties of the hip
and the
practice.
and
it.
The
responses
At
either the spine or the hip, in
to stand on one leg. This has
test,
or false-positive
available.
which
to be carried
dysfunction
we found
many
of their
patients.
Because
the #tic’t/iod, ineatting
and value
one
test;
the Trendelenburg
was
to diagnosis
The
and
manoeuvre
or interpretation
routinely
carried
investigate
radiology
I) appeared
aids
fingers.
vaguely,
and
be interpreted.
agreement
formance
them had
before
by Roentgen,
few
orthopaedic
as a diagnostic
usually
described
the test should
reported
atrophy
(Fig.
ofx-rays
had
the assessment
of function
and
In the standard
textbooks
ferent
first
Australia
ofhip
abducto congenital
muscular
report
when
tioned
was
NADE
side.
he found
useful
in determining
the integrity
tor muscle
function,
with specific
reference
dislocation
of Western
of the hip joint
major
on the standing
In
SYDNEY
TEST
of performing
it have since been described
in the literature.
50 normal
subjects
and 103 people with disorders
affecting
the different
responses
that occurred
when they were asked
us to define
of assessing
operation
tile University
of function
TRENDELENBURG
HARDCASTLE,
From
Trendelenburg’s
THE
stood
were
flexed
on one
studied:
to 30
the hip flexed
to 90
Each
the one-leg
stance
posture
.
aged
what
,
leg.
first
and
perfor
30seconds.
741
742
P. H. HARDCASTLE,
Volunteers
with
103
studied,
people
age range
They were
neuromusculoskeletal
12 had
of the
divided
with neurological
disorders
ofthe
bilateral
hip
disorders
hip or spine.
photography
were
used
and
those
Of
disorders.
103 patients
was from
into two major
groups
DATA
Clinical
videotapes
disorders.
6 to
(Table
with
S. M. L. NADE
Table
I. Classification
The
minimus,
tensor
were
82 years.
I): those
I . Neurological
2.
Mechanical
(a) Ofthe
with
regularly
subjects
matic
lata
and
with
the pelvis
adductor
the
in the different
and
positions
were
also
the
Medical
Research
(ii)
Three
to trau-
C
grading
of
Response
1. The
description
was
(Fig.
hip flexed
at 30
. Three
different
pat-
occurred
with
the
pelvis
rose on the non-stance
of a “negative
Trendelenburg
side,
the
test”;
Fig.
2
Fig.
103
3
Scoliosis
Ankylosing
Iliac crest
Ii
.5
9
spondylitis
defect
after
spinal
3
20
fusion
.5
.5
5
epiphysis
4
Fractured
neck of femur
After arthroplasty
Osteoarthritis
Avascular
necrosis
with
congenital
dislocation
a compensatory
ofthe
scoliosis
15
I5
S
4
hip (Fig.
convex
2. The
Response
with
.5
13)
to the
stance
2).
minimal
pelvis
remained
spinal
compensation
3. The
parallel
to the
(Fig. 3).
ground
pelvis dropped
on the non-stance
sic/c and
moved
downwards.
This was associ-
the
buttock
crease
ated
with
adduction
compensatory
terns
of pelvic
and spinal
movement
non-stance
hip flexed to 30
typical
side
one
Response
responses
With the non-stance
In adults
Including
there
the subject
ofthe
hip was
Council
ofthe
II
3
Congenital
dislocation
Subluxation
Coxa
vara
Perthes’
disease
Slipped
capital
femoral
found
RESULTS
Normal
(b) Ofthe
hip
(i) In children
sub-
studied.
With
disorders
Incomplete
paraplegia
Muscular
dystrophy
Nerve
root entrapment
Cerebral
palsy
Poliomyelitis
Hemiplegia
anterior
muscle
at rest
when
the test was performed.
with incomplete
paraplegia
due
fracture-dislocation
using
power.
magnus
subject
Assessment
of abductor
muscle
power.
lying on one side, the strength
ofabduction
assessed,
muscle
disorders
spine
and videotape.
Initially,
colour
in order
to study
the movement
fascia
to occur
walking
conditions
mechanical
ANALYSIS
recorded
sequently
neuromusculoskeletal
volunteers
patterns
by single-frame
analysis.
As we became
more
experienced,
the responses
were
recorded
on 35 mm
colour
projection
slides.
Electromyography.
This was performed
on three normal
volunteers.
Gluteus
maximus,
gluteus
medius,
gluteus
activities
ofthe
the
of
scoliosis
the
weight-bearing
convex
hip
to the non-stance
and
a
side,
as
seen
in the
classical
“positive
Trendelenburg
test”.
Balance
was achieved
by moving
the torso
and centre
of
gravity
directly
over the weight-bearing
hip (Fig. 4).
With
position
the
non-stance
the
pelvis
hip flexed
rose
Fig.
90
.
1. In
Response
on the non-stance
side
but
this
not
4
Three
different
responses
were seen in norma/
volunteers
when they were asked
to stand
on one
leg with the hip on the non-stance
side flexed
at about
30 . Figure
2-The
pelvis
on the nonstance
side rose above
the stance
side with the trunk
centred
over the stance
hip (a negative
response).
Figure
3-The
pelvis remained
parallel
to the ground.
Figure
4-The
pelvis
on the
non-stance
side dropped
below
the level ofthe
stance
side (a positive
Trendelenburg
sign).
THE
JOURNAL
OF
BONE
AND
JOINT
SURGERY
as
THE
high as when
was because
the non-stance
pelvic
rotation
to the rib cage
and
made
hip was
brought
spinal
SIGNIFICANCE
THE
OF
TRENDELENBURG
743
TEST
flexed only 30. This
the iliac crest closer
compensation
uncomfort-
able.
Response
2. The
There
was
90
-in
pelvis remained
parallel
to the ground.
no third
response
with
the hip flexed
subject
no
did
side.
Electromyographic
obtained
the third
or
fascia
tarily
the
pelvis
activity
2 with
With
was
the
It was
test)
gluteus
and adults
with
proved
difficult
subjects
before
patterns
in normal
standard
was that
way of performing
some
people
with
negative
Table
II. False
responses
of false
negatives
Use
ofsuprapelvic
Use
ofpsoas
activity
was present
in
on command,
volunside,
as during
Responses
I
a group
of
findings
a wide
at first.
we had
people,
the test.
pathological
test
.in
spectrum
Because
clarified
we had
What
(Table
false
could
this,
with
raise
first,
bearing
activity
Poor
Lack
of trunk
the hip as
negative
was
the pelvis
by moving
to
reducing
maintain
pelvis
side,
side,
above
also found
the centre
that
of
or
impingement
evident
in
whom
side. They
did
over
the weight-
amount
of abductor
this
posture
(Fig.
5).
of the shoulder
adductors,
and (possibly)
psoas major
weight-bearing
67- B. No.
Other
S. NOVEMBER
patients
1985
with
the
pelvis
hip
a painful
on
leaning
above
(Fig.
the
hip for only
non-stance
a very
short
side,
using
functioning
and gravity.
was performed
on three patients
non-stance
side of the pelvis
by
well over
the pelvis;
four
our
years
the hip
minimal
on
6). We
hip or spine
experience
could
the test
was
Trendelenburg
of
on the painful
muscles,
kinetic
energy
Electromyography
who could
elevate
the
It was
balance
ofco-operation
with quadratus
lumborum
on the
to raise the non-stance
side of the
of the
to stand
joint
or
electrical
using
muscle
activity
was
recorded
in the abductor
muscle
groups.
Thus,
simply
looking
at the final position
of the trans-iliac
line of the
pelvis gives no assessment
ofabductor
muscle
function.
positives
that people
with pain in the hip tended
to shift
of gravity
over the hip to decrease
the pull of
the abductors.
VOL.
clear
had a
the hand
on a table or wall on
were then able, by a combina-
muscle
contraction
latissimus
dorsi,
the non-stance
weight-bearing
the
able
either
groups
of false
many
on the non-stance
the torso
well
were
ing
a
II).
particularly
disorders,
Figure
5-A
false-negative
test can occur
if the trunk
shifts
excessively
to reduce
the abductor
muscle
force
necessary
to obtain
equilibrium:
note
the wasting
of the right
thigh
due to poliomyelitis.
Figure
6When
the trunk
is re-aligned
over
the stance
hip the pelvis
drops
rapidly
on the non-stance
side because
there
is not enough
muscle
power
available
to maintain
the elevated
position.
period.
In the absence
of significant
pain,
subjects
with
weak hip abductor
muscles
could
achieve
balance
by lift-
understanding
neurological
Secondly.
by supporting
the non-stance
side, they
tion of
especially
of different
we examined
the variable
not defined
Pain
femoris
hip, thereby
necessary
9#{216}c
test
muscles
This
at
became
disorders
Costo-pelvic
patients
a
same
Causes
Wide lateral
translocation
to allow balance
over
a fulcrum
was
hip
to Trendelenburg
rectus
there
non-stance
Trendelenburg
and
that with
no activity
was
medius,
gluteus
the
in abnormal
subjects
and
classifying
the
Ia/se
were
found
hip at 30.
children
conditions
abnormal
response
Causes
Electromyograms
hip abductor
muscle
activity,
when
the
first
response
was
was recorded
in adductor
magnus
the non-stance
Responses
Recording
non-stance
the
maximus.
abductor
on the
on the non-stance
increase
of
a maximum
no activity
gluteus
and
findings.
drop
adductor
magnus;
lata.
If the subject,
raised
gradual
reaching
achieved;
or
pelvis
from
three
volunteers.
response
(false-positive
in
gluteus
maximus,
present
minimus
tensor
the
not
performed.
test could
that
be
children
reliably
on the same
Delayed
Trendelenburg
an initial negative
with the non-stance
began
to fall and
This
sign;
time
at which
be
recorded.
In
fatigue
has been
Mitchell
the
pelvis
people
sign the gait
to walk quickly,
easily
and
a limp,
of the so-called
Trendelenburg
Two subjects
with severe
responses
fully;
unless
this was
and different
responses
at short
time inter-
because
sign.
Several
people
had
test. but after standing
for a short
time
side of the pelvis
raised,
it gradually
they were not able to maintain
their
initial
posture.
Trendelenburg
they
age
day.
positive
Trendelenburg
they are asked
the
however
In children
over
four,
the
be assessed
only if the children
could
understand
and co-operate
possible,
assessment
was invalid,
were seen at separate
examinations
vals
under
assessed,
of
called
(1973)
a delayed
suggested
began
with
a
positive
that the
to drop
delayed
should
positive
can be normal,
but
it becomes
apparent
with
all the characteristics
gait, becomes
scoliosis
had
impingement
when
that
between
obvious.
false-positive
the
lower
744
P. M. HARDCASTLE,
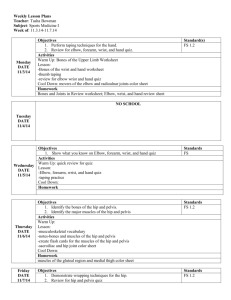
Fig.
7
Fig.
8
Fig.
S. M. L. NADE
9
Fig.
10
Fig.
II
Fig.
12
The suggested
method
ofperforming
the Trendelenburg
test: Figure
7-The
examiner
stands
behind
the patient.
Figure
8-The
patient
is asked
to
raise one leg off the ground
with the hip flexed
between
0 and 30 and to balance
herself.
Figure
9-The
patient
is asked
to raise the non-stance
side as high as possible.
Figure
lO-The
examiner
may support
the patient
by holding
the arm on the other
side. Figure
I I-The
examiner
may Pzot
support
the non-stance
arm as this may act as a fulcrum
for latissimus
dorsi.
quadratus
lumborum,
and the paraspinal
muscles.
Figure
1 2--If
there
is significant
trunk
shift to the stance
side this is corrected
by gently
aligning
the trunk
over the stance-side
hip and watching
the relation
of the
pelvis to the ground.
costal
margin
elevate
and
the
iliac
crest
A
STANDARD
if this
is used
.
response
to
and
be interpreted
perform
the
assessment
co-operation
ofthe
of the
joint
test;
not
being
neutral
and
be flexed
enough
ground
in order
test properly
does
demands
the full
patient.
tested,
30
the patient
and
(the line joining
7).
from
observes
the iliac
the ground
holding
the
of flexion.
The
hip
knee
to allow
the foot to be clear
to nullify
the effect
of the
examiner
(Fig.
3. Once
so
12).
balanced,
both shoulders
as to maintain
the
can be supported
balance
without
patient
is then
asked
II).
patient
examiner
leans
too
far
over
to
the
The
(a)
corrects
this
by
to bring the vertebra
the centre
of the hip
foot
(Fig.
I 2).
(b)
The
“positive”)
if
maximal.
at
(c) The
be lifted
that
position
by the
a stick
the
of
the
pelvis
ment,
response
this
where
the
the stance
can
should
of the
rectus
response
is NORMAL
(i.e.
the
test
is “nega-
side can be elevated
stance
side will allow,
be maintained
for 30
centred
over the hip
foot.
joint
to raise
side
the weight-bearing
tive”)
if the pelvis on the non-stance
as high as hip abduction
on the
and
providing
this posture
can
seconds
with the vertebra
prominens
responses
side above
non-stance
side
of the pelvis
as high
as possible
(Fig.
9). The examiner
may support
the patient
by
holding
the arm on the stance
side (Fig.
10; compare
withFig.
If the
and
the foot
femoris
muscle.
The position
of the pelvis
is again
noted
(Fig.
8). A supporting
stick
can be used
in
the hand
only on the side of the weight-bearing
hip;
alternatively.
the
Interpretation
in a clini-
and
the ground
(Fig.
is asked
to raise
side
between
hip,
a
to do the test
The examiner
stands
behind
the angle
between
the pelvis
crests)
and
2. The patient
4.
weight-bearing
TEST
we have formulated
the Trendelenburg
can
way. To
its accurate
understanding
1
attempted
TRENDELENBURG
the
meaningful
time, and
How
they
gentle
pressure
on the shoulders
prominens
approximately
over
As a result
of our observations,
standard
method
of performing
cally
take
when
the pelvis.
or of
because
(i.e. the test is
This
includes
pelvis
side,
is elevated
but where
on the non-stance
this elevation
is not
response
is also ABNORMAL
if the pelvis
on command,
but can not be maintained
in
for
30 seconds.
The
time
taken
before
starts
to fall is recorded.
By introducing
the Trendelenburg
test can be objectively
for
comparison
described
in (b)
test.
Non-valid
is ABNORMAL
be done.
cannot
purposes.
constitutes
responses.
In the
Obviously
a zero time
presence
the
response
Trendelenburg
of back
deformity.
or if the
patient
is
ofage
or mental
status,
inappropriate
the
a time elerecorded
or leg pain
uncooperative
responses
may
arise
(Table
II). An abnormal
response
(positive
test) in these circumstances
can be misleading.
However,
ifthe
test is negative
that is significant-it
means
that the
subject
does not have abnormal
hip mechanics.
THE
JOURNAL
OF BONE
AND
JOINT
SURGERY
THE
Significance
Neurological
disorders.
strength
was
subjects
whose
MRC
Grade
OF THE
5 abductor
responses
at
patients
in this
the
not
but
to the
full
times
group
extent.
good
at 5 seconds
rectus
(a delayed
femoris
two subjects
with
or SI had negative
muscle
isolated
responses.
nerve
importance
of
this
test).
He
had
helped.
entrapment
(‘oxa
vara.
a
of L5
of 90
The
after
not
by
size
by
bilateral
replacement
the
Arthritis
ofthe
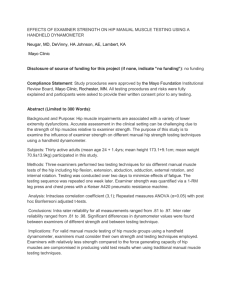
13
Fig.
14
radiograph
of a nine-year-old
boy with
Trendelenburg
response
was negative
seconds
he had a delayed
positive
test.
VOL.
5, NOVEMBER
67-B.
No.
1985
Variable
15
was
head
response.
inequality
qfter
(i.e.
normal
responses
would
in respect
tests
not
altered
if there
is
become
posi-
seen
in one
were
sub-
observed
be
expected
to reduction
but
hip arthroplastv.
to
alter
the
of time of
Two
patients
above
the intertrochanteric
had negative
Trendelenburg
responses).
of the greater
absence
of pain,
trochanter
qfter
the Trendelenburg
hip
arthroplastr.
test was par-
ticularly
osteotomy
valuable
some time after operation.
Where
gap was greater
than 2 cm the Trendelenburg
test
positive
was
in
examined
not vary in the same individual
times.
Obviously
pain or pro-
either
immediately
Fig.
a subluxating
but within
test
femoral
head.
However,
the test can
response
at 20
Trendelenburg
of the
delayed
positive
response.
Fractured
neck of/emur.
Patients
tion with Ender
or Zickel
nails
A 48-year-old
woman
with congenital
dislocation
of the hip showing
a positive
Trendelenburg
response
despite
supporting her body weight
with her hands.
Anteroposterior
hip. His initial
hip.
up to 2 cm ofshortening
after
hip replacement
In the
Fig.
positive
with
line
A i’ulsion
test
15).
of the disease
particularly
the normal
Leg length
a positive
The
rotation
type of response
did
studied
at different
gression
response,
at IS
depend-
femoral
neck and the subjects
responses
if they were painfree.
The Trendelenburg
test was
a delayed
acethips
one
or negative
had
epiphrsis.
by the
tive, and
ject(Fig.
when
osteotomy
of the femoral
or hinge abduction
incongruity
the
be positive
tests,
the
in
test
neck
angle
and
the presence
of
With femoral
neck angles
of up to
be normal.
One child with an angle
capital
altered
patient
treated
may
a varus
to the
negative
disease.
been
test
seconds.
Slippedjemoral
was
examined
deterioration
in adolescents
with
Our two patients
with subluxating
ing on the femoral
degenerative
changes.
100 the response
can
The
when
(1973)
has
described
(timed)
Trendelenburg
both had positive
(timed)
Trendelenburg
and one at 20 seconds
(Fig. 14).
considered
relation
all had
Perthes’
had
hips.
Mitchell
thedelayed
We
Mechanical
disorders.
Congenital
dislocation
of the hip.
The Trendelenburg
test was always
positive
in subjects
with
congenital
dislocation
of the hip (Fig.
13). One
who
respQnse
assessing
clinical
abular
dysplasia.
probably
root
had
a normal
after surgery.
between
0 and
25
were able to elevate
positive
which
745
TEST
Subluxating
to be a positive
Trendelenburg
test at 0 seconds.
One subject
who had Grade
5 strength
on clinical
testing
had a delayed
(or timed)
positive
Trendelenburg
test at 1 5 seconds.
Only
one subject
with Grade
3 hip
abductors
had an initial
negative
response
which
became
positive
TRENDELENBURG
arthroplasty
three years
muscle
required
to produce
a normal
response.
All
hip abductor
power
was Grade
4 or less
had
abnormal
seconds.
Some
pelvis,
SIGNIFICANCE
(zero
time)
the
or with
a
who had unstable
fixahad a positive
response
15
Anteroposterior
radiograph
ofa
10-year-old
boy with coxa magna
and
hip joint
incongruity
as a sequel
of Perthes’
disease.
He had a delayed
positive
test at 20 seconds.
746
P. H. HARDCASTLE,
until
the fracture
were
tested
was
had no
response,
pain at
which
also
positive
had
united
initially
8 to
radiologically.
10 weeks
the time of
was positive.
These
after
pelvis
people
operation
and
at 20 seconds
seconds
vented
on the
adequate
Spinal
disorders.
losing
spondylitis,
also
on the first
next day.
assessment.
other
patients
to elevate
or shifts
of the hip
and
at 25
pain
pre-
stiff spines,
as in ankythe test unless
there was
or gross
spinal
the
the
years
of age,
deformity.
non-weight-bearing
torso
well
called
noted
and
the
over
“trick
in some
test
side
the
of the
pel-
weight-bearing
side;
movements”.
patients
less
is of no value
Variable
than
seven
in children
under
four. Nevertheless,
if the Trendelenburg
test is carefully
performed,
it is an accurate
clinical
sign with prognostic
implications.
Inman
(1947)
measured
the torque
strength
about
the hip with the pelvis
in different
postures
with respect
to the ground.
Stiffliess.
Totally
did not affect
abnormality
examination,
In the
vis,
these
can
be
responses
were
their
initial
Trendelenburg
Two
nialunited
fractures
responses.
A vascular
necrosis
of the jemoral
head.
Hip pain
made
proper
assessment
of these
cases difficult.
However,
one
ofour
four patients
had only mild symptoms;
his test was
positive
S. M. L. NADE
Our
electromyographic
results
confirm
findings
necessary
that little
abductor
muscle
strength/activity
to maintain
a balanced
posture
with the
dropped
side. As
abductor
(as in Response
3) on the
the pelvis
rises on this side
muscle
activity
provided
his
is
pelvis
non-weight-bearing
there
is increase
that
the torso
over the hip.
Functional
assessment
of a joint
is important
clinical
assessment
of patients.
Observation
of
of
is
centred
probably
Fig.
16
This
43-year-old
lady’s
hip
abductors
had
normal
strength.
However,
she was
unable
to raise her pelvis on
the left above
the horizontal
because
of impingement
between the iliac crest and costal margin
as the result
of
severe scoliosis.
performed
of limitation
functional
valuable
less
of space.
assessment
clinical
often
than
is desirable
The Trendelenburg
in a confined
space,
sign
than
many
static
be easily recorded
on film or videotape.
It is our belief
that a patient
who
response
to the Trendelenburg
paper
has an inefficient
gait,
easily
With
fatigued.
a little
test
and
because
test allows
for
and is a more
tests.
It can
has
an abnormal
as described
therefore
practice,
in the
gait
is
the
test
also
in this
becomes
is not
diffi-
cult to perform
and interpret.
Timing
is an essential
part
of the test; it provides
an objective
measure
of improvement
or deterioration
in the neuromuscular
or mechanical function
of the hip.
Kyphosis
Deformiti’.
scoliosis,
lower
costal
positive
margin
Nerve
16).
root
but
results,
not affect the outcome.
Severe
lead to impingement
between
the
and the iliac crest and give a false-
may
(Fig.
test
Pain.
did
however,
irritation
back
lead
to
not lead
can
pain
itself
did
Trendelenburg’s
original
observations
and clear,
and his interpretations
accurate.
the need for meticulous
clinical
examination
provide
correct
the standardised
ment offunction
false-positive
to abnormal
were precise
We Support
in order
to
diagnosis
and we recommend
the use of
timed
Trendelenburg
test in the assessand malfunction
ofthe
hip.
responses.
DISCUSSION
When
routine
same
asked
to stand
hip
to ensure
side,
may
test
response
is
the
if the pelvis
drops
seconds
the Trendelenburg
indeed,
altered
is an
makes
either
lack
patient
can
cannot
be
negative
essential
tests
on
part
it an
hip mechanics.
However,
the
muscle
follow
a standard
contraction
to
the
response
on the
standardised
must
the non-stance
test is positive.
of the
objective
one
An
2.
occur,
be absolute,
test
side within
30
The use of a
Trendelenburg
measure
of
test,
severity
the test.
False-positive
3. The
tial,
mal”
and,
of
and
but
their
is properly
use
false-negative
interpretation
can
responses
may
be clarified
if the
performed.
of a timer
and allows
response.
when
performing
measurement
the
of
test
a “delayed
is essenabnor-
REFERENCES
presence
of pain,
of co-operation
or
lead to false-positive
properly
performed.
is that
and
respond
normal
and
timer
.
leg,
in one
of three
ways.
Only
the other
two are abnormal.
normal;
to assume
one
abductor
patients
Trendelenburg
ability
on
Conclusions
I The Trendelenburg
test is a useful
part
of clinical
examination
if performed
and interpreted
correctly.
We have described
a standard
method
for performing
the
subject
poor
and
balance
understanding
tests,
because
The
reason
for
uses
above
muscles
by
the
the
test
falsethe
Inman
VI. Functional
aspects
of the abductor
Bonefoint
Surg[Br] l947;29:607-19.
Mitchell
GP. The
291: 1113.
Rang
M. Antho/ogy
1966; 139-43.
delayed
of
Trendelenburg
orthopaedics.
THE JOURNAL
hip
muscles
test.
mt
Edinburgh:
OF BONE AND
of the
Congr
E&S
JOINT
Ser
hip.
1973;
Livingstone,
SURGERY
J