To View Sample 2 Internal Pages From The Muscular System Manual
advertisement

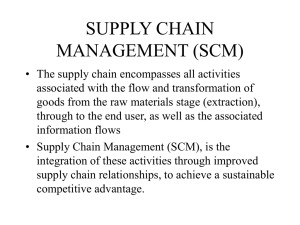
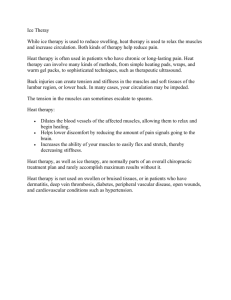
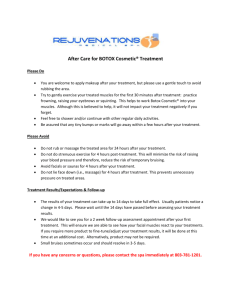
238 PART 2 The Skeletal Muscles of the Upper Extremity Thenar Eminence Group ■ ORGANIZATION OF THE THENAR MUSCLES ■ MISCELLANEOUS The thenar eminence is an eminence of soft tissue located on the radial side of the palm of the hand. There are three muscles in the thenar eminence group: the abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis. The ■ ATTACHMENTS All three thenar muscles attach proximally onto the flexor 9 retinaculum and carpal bones. All three thenar muscles attach distally onto the thumb. The abductor pollicis brevis and the flexor pollicis brevis attach onto the proximal phalanx of the thumb. The opponens pollicis attaches onto the metacarpal of the thumb. layering of the thenar muscles is approximately as follows: The abductor pollicis brevis is the most superficial of the three. The flexor pollicis brevis is intermediate. The opponens pollicis is the deepest of the three. There are three muscles located in the hypothenar eminence that are analogous to the thenar muscles. The three hypothenar muscles are the abductor digiti minimi manus, flexor digiti minimi manus, and opponens digiti minimi. The thenar muscles are located within the deep front arm line myofascial meridian. INNERVATION The three thenar muscles are innervated by the median nerve. (The ulnar nerve usually contributes to a small degree.) ARTERIAL SUPPLY ■ FUNCTIONS All three thenar muscles move the thumb. In each case, the name of the muscle indicates its major joint The three thenar muscles receive their arterial supply from the radial artery. action. Transverse carpal ligament (flexor retinaculum) Opponens pollicis Abductor pollicis brevis Flexor pollicis brevis A Figure 9-5 Anterior views of the right thenar group muscles. A, Superficial view. CHAPTER 9 Intrinsic Muscles of the Finger Joints Thenar Eminence Group—cont’d 239 APB (cut) FPB (cut) OP FPB (cut) APB (cut) 9 B Figure 9-5, cont’d B, Deep view. The abductor pollicis brevis and flexor pollicis brevis have been cut. APB, abductor pollicis brevis; FPB, flexor pollicis brevis; OP, opponens pollicis. CHAPTER 10 Muscles of the Spinal Joints 273 Anterior Views of the Muscles of the Trunk—Deep Views 6th rib 10 Internal intercostals Rectus abdominis External abdominal oblique (cut) Diaphragm Quadratus lumborum Psoas minor Internal abdominal oblique (cut) Psoas major Transversus abdominis Iliacus Anterior superior iliac spine (ASIS) Inguinal ligament Pyramidalis B Figure 10-2, cont’d B, Deep views with the posterior abdominal wall seen on the left. The muscles of the neck, arm, and thigh have been ghosted in. 310 PART 3 The Skeletal Muscles of the Axial Body NECK AND HEAD Sternocleidomastoid (SCM) The name, sternocleidomastoid, tells us that this muscle attaches to the sternum, the clavicle, and the mastoid process of the temporal bone. Derivation sterno: Pronunciation Gr. refers to the sternum. cleido: Gr. refers to the clavicle. mastoid: Gr. refers to the mastoid process. STER-no-KLI-do-MAS-toyd ■ ATTACHMENTS STERNAL HEAD: Manubrium of the Sternum the anterior superior surface Medial Clavicle Clavicular Head: the medial 1 3 to the 10 Mastoid Process of the Temporal Bone and the lateral 1 2 of the superior nuchal line of the occipi- Trapezius Sternal head Clavicular head tal bone ■ FUNCTIONS Concentric (Shortening) Mover Actions Standard Mover Actions 1. Flexes the lower neck at the spinal joints 2. Extends the upper neck and head at the spinal joints 3. Laterally flexes the neck and head at the spinal joints 4. Contralaterally rotates the neck and head at the spinal joints Reverse Mover Actions 1. Elevates the sternum and trapezius has been ghosted in. clavicle Figure 10-19 Lateral view of the right sternocleidomastoid. The 2. Ipsilaterally rotates the trunk at the spinal joints Standard Mover Action Notes • The sternocleidomastoid (SCM) crosses the joints of the lower neck anteriorly (with its fibers running vertically in the sagittal plane); therefore it flexes the lower neck at the cervical spinal joints. (action 1) • Because the SCM courses posteriorly as it ascends from the sternum/clavicle to the head, it crosses the joints of the upper neck posteriorly. Therefore, it extends the upper neck at the cervical spinal joints and extends the head at the atlanto-occipital joint (AOJ). (action 2) • The SCM is the only muscle that can flex one region of the neck and extend another region (every other muscle either flexes or extends the neck). Exactly where the dividing line is located is determined by the degree of curvature of the client’s neck. (actions 1, 2) • The SCM crosses the spinal joints laterally (with its fibers running vertically in the frontal plane); therefore it laterally flexes the neck at the cervical spinal joints and laterally flexes the head at the AOJ. (action 3) • The clavicular head is more active than the sternal head with lateral flexion of the neck and head. (action 3) • The SCM wraps around the neck from the sternum/clavicle anteriorly to the cranium more posteriorly (with its fibers running somewhat horizontally in the transverse plane). When the SCM contracts, it pulls on the cranium, causing the anterior surface of the neck and/or the head to face the opposite side of the body from the side to which it is attached. Therefore the SCM contralaterally rotates the neck at the cervical spinal joints and the head at the AOJ. (action 4) • The sternal head is more active than the clavicular head with contralateral rotation of the neck and head. (action 4) Reverse Mover Action Notes • If the cranial attachment of the SCM is fixed, the sternal/ clavicular attachment must move. Because the SCM has its fibers running vertically from the sternum/clavicle, the sternum and the clavicle would be elevated toward the cranial attachment. Elevating the sternum and clavicle can assist in lifting the rib cage during inspiration (breathing in). Therefore the SCM is an accessory muscle of respiration. (reverse action 1) CHAPTER 10 Muscles of the Spinal Joints 311 Sternocleidomastoid (SCM)—cont’d • With the cranial attachment of the SCM fixed, the sternal/ clavicular attachment will be pulled in the transverse plane such that the anterior surface of the trunk will come to face the same side of the body to which the SCM is attached. Therefore the SCM can ipsilaterally rotate the trunk at the spinal joints (the reverse action of contralateral rotation of the upper spine relative to the fixed lower spine is ipsilateral rotation of the lower spine relative to the fixed upper spine). This reverse action requires the cranial attachment to be sufficiently fixed so that the weight of the trunk is moved relative to it. (reverse action 2) Eccentric Antagonist Functions 1. Restrains/slows extension of the lower neck at the spinal joints 2. Restrains/slows flexion of the upper neck and head at the spinal joints 3. Restrains/slows opposite-side lateral flexion and ipsilateral rotation of the neck and head at the spinal joints 4. Restrains/slows depression of the sternum and clavicle 5. Restrains/slows ipsilateral rotation of the trunk Isometric Stabilization Functions 1. Stabilizes the cervical spinal joints and the sternoclavicular joint Isometric Stabilization Function Note • The SCM stabilizes the entire neck, including the head at the AOJ. By attaching to the sternum and clavicle, it also helps to stabilize the sternoclavicular joint. Additional Notes on Functions 1. Some sources state that the action of the SCM on the head at the AOJ can change from extension to flexion if the position of the head changes sufficiently, thus changing the line of pull of the SCM relative to the AOJ. This becomes more likely as a person ages and tends to posturally carry the head more anteriorly. 2. The SCM may also be able to weakly upwardly rotate the clavicle at the sternoclavicular joint. INNERVATION Spinal Accessory Nerve (CN XI) and C2, C3 ARTERIAL SUPPLY The Occipital and Posterior Auricular Arteries (branches of the External Carotid Artery) and the Superior Thyroid Artery (a branch of the External Carotid Artery) , PA LPA TI ON 1. Have the client supine with the neck and head rotated contralaterally. 2. Then have the client lift the head and neck up into the air and the SCM will visibly contract. 3. Palpate the SCM from attachment to attachment. ■ RELATIONSHIP TO OTHER STRUCTURES Except for the platysma (which is superficial to all anterior neck muscles), the SCM is superficial throughout its entire course. The following muscles are deep to the SCM (listed from inferior to superior): infrahyoids, scalenes, levator scapulae, digastric, and splenius capitis. The attachment of the SCM onto the mastoid process of the temporal bone and the superior nuchal line of the occipital bone is superficial to the splenius capitis and lateral to the trapezius. The SCM is located within the superficial front line and lateral line myofascial meridians. ■ MISCELLANEOUS 1. The SCM’s major superior attachment is the mastoid process attachment of the temporal bone. However, it also has a thin aponeurotic attachment to the occipital bone. 2. The carotid sinus of the common carotid artery lies directly deep and medial to the SCM, midway up the neck. Given the neurologic reflex that occurs to lower blood pressure when the carotid sinus is pressed, massage to this region must be done judiciously, especially with weak and/or elderly clients. 3. The SCM and the scalenes, are often injured as a result of car accidents. This trauma is usually called whiplash, wherein the head and neck are forcefully thrown anteriorly and posteriorly (like a whip being lashed). When the head and the neck are thrown posteriorly, the anterior cervical musculature may be torn; or the muscle spindle reflex may occur, causing the anterior cervical musculature to spasm. When the head and the neck are thrown anteriorly, the same trauma may occur to the posterior musculature. 4. The SCM is an excellent landmark for palpating other muscles of the neck. Locate the posterior (lateral) border of the SCM and the anterior border of the upper trapezius, and then palpate in the tall narrow triangular space that is located between them; this triangular area is called the posterior triangle of the neck. Locating the medial border of the SCM can be used as a landmark for palpating the longus colli and longus capitis (of the prevertebral group). 10 396 PART 3 The Skeletal Muscles of the Axial Body Views of the Major Muscles of Mastication Temporalis Masseter Figure 12-2 Right lateral view of the temporalis and masseter. The masseter has been ghosted in. 12 Lateral pterygoid plate of sphenoid Lateral pterygoid Mandibular condyle Superior head Superior head Inferior head Inferior head Maxilla Medial pterygoid Medial pterygoid Angle of mandible Mandible (cut) Mandible Figure 12-3 Views of the right lateral and medial pterygoids. A, Lateral view with the mandible partially cut away. B, Posterior view of the lateral and medial pterygoids with the cranial bones cut away. Lateral pterygoid 398 PART 3 The Skeletal Muscles of the Axial Body Temporalis The name, temporalis, tells us that this muscle attaches onto the temporal bone. Derivation Pronunciation temporalis: L. refers to the temple. tem-po-RA-lis ■ ATTACHMENTS Temporal Fossa the entire temporal fossa except the portion on the zygomatic bone to the Coronoid Process and the Ramus of the Mandible the anterior border, apex, posterior border, and internal surface of the coronoid process of the mandible, as well as the anterior border of the ramus of the mandible Figure 12-5 Lateral view of the right temporalis. The masseter has been ghosted in. ■ FUNCTIONS 12 Eccentric Antagonist Functions CONCENTRIC (SHORTENING) MOVER ACTIONS Standard Mover Actions 1. Elevates the mandible at the TMJs 2. Retracts the mandible at the TMJs Reverse Mover Actions 1. Moves the temporal bone inferiorly toward the mandible 2. Moves the temporal bone anteriorly toward the mandible TMJs = temporomandibular joints Standard Mover Action Notes • The anterior fibers of the temporalis are oriented vertically from the cranium superiorly, to the mandible inferiorly. When the temporalis contracts, it pulls the mandible superiorly toward the cranium. Therefore the temporalis elevates the mandible at the TMJs. (action 1) • The posterior fibers of the temporalis are oriented horizontally from the cranium posteriorly, to the mandible anteriorly. When the temporalis contracts, it pulls the mandible posteriorly toward the cranium. Therefore the temporalis retracts the mandible at the TMJs. (action 2) Reverse Mover Action Notes • Reverse actions of moving the temporal bone toward the mandible require the mandible to be fixed and the temporal bone and entire cranium to move toward the fixed mandible at the TMJs. These reverse actions do not commonly occur. When they do occur, they would be opposite in direction to the standard mover actions. Therefore, the cranium would be pulled inferiorly and anteriorly. (reverse actions 1, 2) 1. Restrains/slows depression and protraction of the mandible Isometric Stabilization Function 1. Stabilizes the mandible at the TMJs Additional Note on Functions 1. Some sources state that the temporalis also contributes to side-to-side grinding by doing ipsilateral deviation of the mandible at the TMJs. INNERVATION The Trigeminal Nerve (CN V) deep temporal branches of the anterior trunk of the mandibular division of the trigeminal nerve ARTERIAL SUPPLY The Maxillary and Superficial Temporal Arteries (branches of the External Carotid Artery) , PA LPA TI ON 1. With the client supine, place palpating fingers over the temporal fossa. 2. Have the client alternately clench and relax the teeth and feel for the contraction and relaxation of the temporalis. In this manner the majority of the temporalis superior to the zygomatic arch can be easily palpated. CHAPTER 12 Muscles of the Temporomandibular Joints 399 Temporalis—cont’d ■ RELATIONSHIP TO OTHER STRUCTURES The superior portion of the temporalis is superficial (except for the auriculares anterior and superior, which are superficial to it). The inferior portion of the temporalis runs deep to the zygomatic arch. Inferior to the zygomatic arch, the temporalis is deep to the masseter. Deep to the superior portion of the temporalis are the cranial bones (frontal, parietal, temporal, and sphenoid). Deep to the inferior portion of the temporalis are the lateral pterygoid, the superficial head of the medial pterygoid, and a small part of the buccinator. The temporalis is involved with the deep front line myofascial meridian. ■ MISCELLANEOUS 1. The temporalis muscle is deep to thick fibrous fascia called the temporalis fascia. 2. The more superficial fibers of the temporalis actually attach into the temporal fascia. 3. A tight temporalis may be involved with tension headaches and with dysfunction of the temporomandibular joint (TMJ syndrome). 4. The temporal fossa is a fossa (depression) that overlies not only the temporal bone but also the frontal, parietal, zygomatic, and sphenoid bones. 5. The superficial temporal artery is superficial to the temporalis muscle, and its pulse can be palpated. 6. The temporal fossa is much deeper in carnivores, allowing for a much thicker and stronger temporalis muscle. This contributes to the strength of a carnivore’s bite. 12 430 PART 3 The Skeletal Muscles of the Axial Body SCALP Occipitofrontalis (of Epicranius) The name, occipitofrontalis, tells us that this muscle lies over the occipital and frontal bones. Galea aponeurotica Frontalis Derivation Pronunciation occipitofrontalis: L. refers to the occiput and the frontal bone. ok-SIP-i-to-fron-TA-lis Occipitalis ■ ATTACHMENTS OCCIPITALIS: and the Temporal Bone Occipital Bone the lateral 2 3 of the highest nuchal line of the occipital bone and the mastoid area of the temporal bone Trapezius Sternocleidomastoid to the Galea Aponeurotica 13 FRONTALIS: Galea Aponeurotica to the A Fascia and Skin overlying the Frontal Bone ■ FUNCTIONS Concentric Mover Actions 1. Draws the Scalp Posteriorly (Elevation of the Eyebrow) 2. Draws the Scalp Anteriorly Mover Action Notes 1. The occipitofrontalis attaches from the occipital and temporal bones posteriorly, to the fascia and skin overlying the frontal bone anteriorly. The posterior attachment, which is bone, is more fixed than the anterior attachment, which is soft tissue. Therefore when the posterior attachment is fixed, and the occipitofrontalis contracts, it pulls the anterior attachment toward the posterior attachment. When this occurs, the entire scalp moves posteriorly. This pulls on the fascia and skin located superior to the eye, causing the eyebrow to elevate and the skin of the forehead to wrinkle. (action 1) 2. The frontalis belly of the occipitofrontalis attaches from the fascia and skin overlying the frontal bone to the galea aponeurotica posteriorly. When the anterior attachment is fixed and the frontalis contracts, it pulls the posterior attachment (the galea aponeurotica) toward the anterior attachment. Therefore the scalp is drawn anteriorly. When this occurs, the skin of the forehead may also wrinkle. (action 2) B Figure 13-5 The occipitofrontalis. A, Lateral view of the right occipitofrontalis. The trapezius and sternocleidomastoid have been ghosted in. B, Expression of elevating the eyebrows created by the bilateral contraction of the occipitofrontalis. CHAPTER 13 Muscles of Facial Expression 431 Occipitofrontalis (of Epicranius)—cont’d INNERVATION The Facial Nerve (CN VII) occipitalis: posterior auricular branch of the facial nerve frontalis: temporal branches of the facial nerve ARTERIAL SUPPLY Occipitalis: the Occipital and Posterior Auricular Arteries (branches of the External Carotid Artery) Frontalis: supraorbital and supratrochlear branches of the Ophthalmic Artery (a branch of the Internal Carotid Artery) , P A L PATION 1. With the client prone or supine, place palpating hand over the occipital bone and feel for the occipitalis, over the parietal bone and feel for the galea aponeurotica, and over the frontal bone and feel for the frontalis. 2. Ask the client to wrinkle the skin of the forehead, and feel for the contraction of the muscle. ■ RELATIONSHIP TO OTHER STRUCTURES The occipitalis is directly superior to the most superficial muscles of the neck that attach into the superior nuchal line and the mastoid process, namely, the trapezius and the sternocleidomastoid. The frontalis is superior to and even blends into the procerus, the corrugator supercilii, and the orbicularis oculi. Lateral to the frontalis and the galea aponeurotica is the temporoparietalis, and deep to that, the temporalis. The occipitofrontalis is located within the superficial back line myofascial meridian. ■ MISCELLANEOUS 1. The occipitofrontalis attaches into the galea aponeurotica; the temporoparietalis also attaches into the galea aponeurotica. The occipitofrontalis and the temporoparietalis together are known as the epicranius. (Note: The galea aponeurotica is also known as the epicranial aponeurosis.) 2. The occipitofrontalis can be considered to be two separate muscles: the occipitalis and the frontalis. 3. Elevation of the eyebrows often accompanies glancing upward. Elevation of the eyebrows is associated with the expressions of surprise, shock, horror, fright, or recognition. 4. The occipitofrontalis is located within the scalp. The scalp consists of five layers: the skin, subcutaneous tissue, the epicranius and its aponeurosis (the galea aponeurotica), loose connective tissue, and the pericranium. Of these layers, the skin, the subcutaneous tissue, and the galea aponeurotica are firmly connected to each other. 5. The left and right frontalis muscles blend into each other in the midline of the head. The left and right occipitalis muscles usually have a gap between them that is filled in with an extension of the galea aponeurotica. 6. The occipitofrontalis is often ignored or only worked lightly during bodywork. It is a muscle like any other in the body, and moderate or even deeper work may be done to benefit the client. Because tension headaches often involve the occipitofrontalis, this muscle should be evaluated in any client complaining of headaches, especially tension headaches. 13 CHAPTER 14 Muscles of the Hip Joint 475 Posterior Views of the Muscles of the Hip Joint—Superficial and Intermediate Views Iliac crest Gluteus medius Gluteus medius (deep to fascia) Sacrotuberous ligament Piriformis Tensor fasciae latae Superior gemellus Obturator internus Inferior gemellus Sciatic nerve Gluteus maximus Greater trochanter of femur Quadratus femoris Ischial tuberosity Adductor magnus Iliotibial band (ITB) Vastus lateralis Vastus lateralis Adductor magnus Gracilis 14 Long head Semitendinosus Biceps femoris Short head Biceps femoris Semimembranosus Popliteal artery and vein Tibial nerve Plantaris Common fibular nerve Sartorius A Figure 14-2 Posterior views of the muscles of the hip joint. A, Superficial view on the left and intermediate view on the right.