II.5.2 Benzalkonium chlorides
advertisement

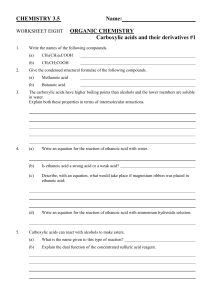
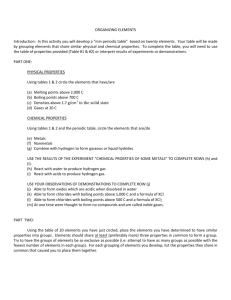
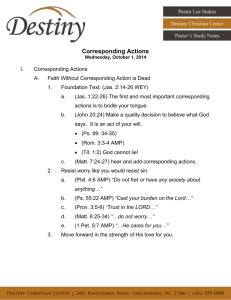
5.2 II.5.2 Benzalkonium chlorides by Kazuhiro Koyama and Yoko Shimazu Introduction Surfactants can be classified into cationic, anionic and nonionic ones. Benzalkonium chlorides are cationic surfectants and being widely used as a disinfectant and germicide using their strong protein-denaturing action. Especially in hospitals, 10 % solution of benzalkonium chloride mixture is being usually used; it is diluted to 0.05–0.1 % solution to be used for various types of disinfection. The drugs are contained in gargles and preservative solutions for contact lenses. Fatal benzalkonium chloride poisoning cases, in which the 10 % solution had been ingested, were reported [1, 2]; it can be regarded as one of the most important poisons in daily necessities. As poisoning symptoms, a pungent sense of the oral mucous membranes, sore throat, cyanosis, convulsion and coma can be mentioned [3, 4]. Benzalkonium chlorides are the mixture of multiple analogous compounds. To measure the concentration, it is necessary to combine concentrations of each component. The quaternary ammonium salt benzalkonium chlorides can be expressed as [C6H5CH2N(CH3)2R]Cl, where R is the mixture of C8H17-C18H37. In most cases, the major R’s are C12H25(C12), C14H29(C14) and C16H33(C16); especially according to the National Formulary XVI, C12, C14 and C12 + C14 count more than 40, 20 and 70 %, respectively [5]. Therefore, upon analysis of benzalkonium chlorides, it seems necessary to measure at least the C12 and C14 compounds ( > Figure 2.1). ⊡ Figure 2.1 Structures of main components of benzalkonium chlorides. Benzalkonium chlorides are a mixture of quaternary ammonium salts showing the structures of [C6H5CH2N(CH3)2R]Cl, where R is a mixture of C8H17–C18H37. However, main structures of R are C12H25(C12), C14H29(C14) and C16H33(C16); C12 40%, C14 20 %, and C12 plus C14 70 % [5]. © Springer-Verlag Berlin Heidelberg 2005 408 Benzalkonium chlorides In this chapter, a method for wide-bore capillary GC/MS analysis of benzalkonium chlorides is described and an HPLC method is also mentioned briefly. GC/MS analysis Reagents and their preparation • • • A 1-mg aliquot each of benzyldimethyldodecylammonium (C12) bromide, benzyldimethyltetradecylammonium (C14) chloride and benzyldimethylhexadecylammonium (C16) chloride (all from Sigma, St. Louis, MO, USA) is dissolved in 100 mL methanol in a 100-mL volmetric flask to prepare 10 µg/mL solution separately. A 4.3-g aliquot of NaOH is dissolved in distilled water to prepare 100 mL solution (1 M NaOH) in a 100-mL volmetric flask. A 1-mg aliquot of promazine hydrochloride (Sigma) is dissolved in distilled water to prepare 100 mL solution (10 µg/mL promazine, internal standard IS) in a 100-mL volmetric flask. GC/MS conditions GC column: SGE BPX35a (30 m × 0.53 mm i. d., film thickness 1.0 µm, Shimadzu GLC Center, Tokyo, Japan). GC/MS conditions; instrument: GCMS-QP 5050 Ancw (Shimadzu Corp., Kyoto, Japan); column (oven) temperature: 100 °C (1.5 min) → 7 °C/min → 200 °C → 5 °C/min → 330 °C (7 min); interface temperature: 280 °C; injection: PTVb splitless high pressure injectionc, initial injection temperature 50 °C (0.01 min) → 250 °C/min → 330 °C (10 min); initial pressure of injection: 200 kPa, 1.5 min; injection volume: 10 µL; split ratio: 10 ; sampling time: 1.9 min; column flow rate: 15 mL/min; MS ionization: EI; scan range ( > Figure 2.2): m/z 50–509; scan interval: 0.5 s [6]. ⊡ Figure 2.2 Total ion chromatogram (TIC) for the authentic benzalkonium chlorides. C12: benzyldimethyldodecylammonium; C14: benzyldimethyltetradecylammonium; C16: benzyldimethylhexadecylammonium. GC/MS analysis Procedures i. Liquid-liquid extraction i. ii. iii. iv. v. vi. A 50-µL volume each of C12, C14 and C16 methanolic solutions is placed in a small test tube, and evaporated to dryness under a stream of nitrogen with warming at 50 °C. To the combined residue, 500 µL blank serum is added and mixed well to prepare 1 µg/mL standard solutiond for C12, C 14 and C16 compounds of benzalkonium chlorides. A 500-µL volume each of specimens (serum, gastric juice or urine) and a 500-µL volume of the above standard solution are placed in separate test tubes, followed by the addition of 2 mL ethyl acetate, 500 µL distilled water, 50 µL of 1 M NaOH solution and 50 µL IS solution, respectively. After voltex-mixing (or shaking) for 3 min, each tube is centrifuged at 3,000 rpm for 5 min. The upper organic phase is transferred to a vial. The phase is evaporated to dryness under a stream of nitrogen with warming at 50 °C. The residue is dissolved in 100 µL ethyl acetate; a 10-µL aliquot is injected into GC/MS. The measurements are made in the scan mode ( > Figure 2.3); quantitation is made by ion chromatography using ions at m/z 134 for C12, C14 and C16 compounds of benzalkonium chlorides and at m/z 58 for promazine (IS). ⊡ Figure 2.3 Mass spectra of benzalkonium chlorides. 409 410 Benzalkonium chlorides ii. Extraction with Extrelut® i. ii. iii. iv. v. vi. The standard solutionsd for the C12, C14 and C16 compounds of benzalkonium chlorides are prepared according to the above i) step of the liquid-liquid extraction. A 500-µL volume each of specimens (serum, gastric juice or urine) and a 500-µL volume of the above standard solution are placed in separate test tubes, followed by the addition of 500 µL distilled water, 50 µL of 1 M NaOH solution and 50 µL IS solution, respectively. Each mixture is poured into Extrelut NTI® (Merck, Darmstadt, Germany) and left for 20 min. The target compounds are eluted with 4 mL ethyl acetate. The eluate is evaporated to dryness under a stream of nitrogen with warming at 50 °C and reconstituted in 100 µL ethyl acetate. After centrifugatione at 3,500 rpm for 5 min, a 10-µL aliquot of the supernatant fraction is injected into GC/MS. The GC/MS detection method is the same as described at the step vi. of the above liquidliquid extraction. Assessment of the method The detection limits by this method required for library research of a compound in the scan mode were 1–2 µg/mL; those for quantitation by mass chromatography were about 10 ng/mL ( > Figure 2.4). If higher sensitivity is required, the measurements in the SIM mode become necessary. In the present analytical system, the sensitivity is being increased by large-volume injection f using a wide-bore capillary column and the PTV sample injection device; but usual capillary GC/MS can be used without great differences, though the sensitivity becomes lower to some extent. The lower sensitivity can be overcome by using the SIM mode and/or derivatization g of the analytes. In this section, both liquid-liquid and Extrelut extractions are described. According to the experience of the authors, the Extrelut extraction is superior to the liquid-liquid extraction in view of stability and reproducibility. ⊡ Figure 2.4 TIC and mass chromatograms for an extract of plasma, into which benzalkonium chlorides had been spiked. C12: benzyldimethyldodecyl-ammonium; C14: benzyldimethyltetradecylammonium; C16: benzyldimethyl-hexadecylammonium. The concentration of each compound spiked was 1 µg/mL; GC/MS analysis was made after liquid-liquid extraction. Poisoning case, and toxic and fatal concentrations HPLC analysis Benzalkoniums in plasma can be extracted by solid-phase extraction with a C18 column, and analyzed by HPLC using a CN separation column, acetonitrile/propionate buffer solution (0.161 M, pH 5.4) (90:10) as a mobile phase and a UV detector [7]. In another method [8], dimethyldodecylammonium chloride (DDMAC) was used as IS; benzalkoniums and IS were analyzed by HPLC using a CN-NH2 column, chloroform/methanol (80:20) as a mobile phase and a post-column fluorescence detector with 9,10-dimethoxy-2-anthracene sulfonate (DMAS) as a fluorogenic reagent with excitation at 383 nm and emission at 459 nm. Poisoning case, and toxic and fatal concentrations Poisoning case A 22-year-old male attempted suicide by taking 20–100 mL of 10 % benzalkonium chloride solution, which had been mixed with coffee, by eating a quarter of a cigarette and then by slitting his left wrist (about 4 cm long injury). His consciousness was clear and he walked to an emergency room of a hospital by himself. Upon admission to the hospital, his physical findings were: blood pressure 120/60 mmHg; heart beat rate 94/min; body temperature 36.4 °C; respiration rate 16/min; consciousness, clear (O/JCS, E4V5M6/GCS); light reaction, positive; pupils, equally 3.5 mm; wound, cut injury in the left wrist of about 4 cm length; X-ray photographs, no finding in the chest and intestinal gas observable in the abdomen. After admission, gastrolavage and administration of activated charcoal and Niflec® (a mixture solution of NaCl, KCl, NaHCO3 and Na2SO4) were made. During his admission, no poisoning symptoms due to benzalkonium chlorides could be found; he was discharged on the next day. Serum concentrations upon admission were: benzalkonium chlorides, 52 ng/mL in total (C12: 52 ng/mL, C14: < 10 ng/mL, C16: < 10 ng/mL); nicotine h: < 10 ng/mL. However, the concentrations in gastric juice were: benzalkonium chlorides 54.4 µg/mL (C12: 50.7 µg/mL, C14: 3.6 µg/mL, C16: 0.06 µg/mL); nicotine h 5.75 µg/mL. Toxic and fatal concentrations In fatal benzalkonium chloride poisoning cases, solution products, containing not less than 10 % benzalkonium chlorides, were ingested. Human oral fatal doses are 100–400 mg/kg. In cases of non-oral administrations (i.v. and i.m. injections or intrauterine injection) its toxicity is much enhanced; the fatal doses were reported to be 5–15 mg/kg [1, 2]. However, the number of reports describing blood concentrations of benzalkoniums in poisoning cases are very limited. Hitosugi et al. [2] reported a fatal poisoning case, in which a 84-year-old female had taken 50 mL (96.2 mg/kg) of 10 % benzalkonium chloride solution and died 3 h later; her serum benzalkonium chloride concentration was reported to be 1.15 mg/ mL. In the above survived case described in the (1) section, the serum benzalkonium chloride concentration upon admission was 52 ng/mL, which is much lower than that in the fatal case. 411 412 Benzalkonium chlorides The survived patient might have ingested only a small amount of coffee containing the compounds; and/or the dilution of the benzalkonium solution with coffee might have resulted in no protein-denaturing action. Notes a) Any other column of slightly or intermediately polar types seems usable. In this chapter, a wide-bore capillary column was used. The column has a large capacity for loading of specimens, and the leading phenomenon does not appear, even when a trace amount of a drug in serum is measured, followed by the measurement of a large amount of the compound present in stomach contents. However, the wide-bore capillary column shows lower resolution (separation) ability. Since this type of column has a large capacity; an analyst sometimes injects a large volume of a specimen extract, resulting in the carry-over of many residual or impurity peaks during subsequent measurements. b) In the usual split/splitless injection mode, a sample solution is injected into an insert at a high temperature to vaporize it immediately. In contrast, the programed temperature vaporizing (PTV) device enables the injection of a liquid sample without immediate evaporation; gradual elevation of its temperature for mild evaporation. This is useful for more sensitive analysis of thermolabile compounds without heat decomposition to some extent [9]. In this respect, the PTV device seems very useful in clinical analysis cases, in which many thermolabile compounds are dealt with. The glass insert and silica wool to be used should be silanized to prevent drugs from their decomposition [10]. c) The high pressure injection is used for suppressing the broadening of a peak due to the large volume injection. d) In this method, semiquantitative measurements with one point standard are being used, because of too limited times available for analysis at a critical care medical center. For accurate quantitation, a calibration curve made of not less than 3 plots at different concentrations becomes necessary. e) When the Extrelut NT1® is used for extraction, clogging of a pre-filter for HPLC usually takes place in a relatively early stage; the movement of a plunger of a syringe for autoinjector of GC also becomes not smooth. To prevent these phenomena, insoluble components should be removed by centrifugation. f) In this method, large volume injection is being used to enhance the sensitivity for enabling identification of a trace amount of a drug being contained in a biomedical specimen. Our system can also quantitate a drug at the levels of > 10 ng/mL. The large volume injection together with PTV seems to be a powerful tool for analysis of samples obtained from drugpoisoned patients at a very busy critical care medical center, while it requires a time-consuming labor for its maintenance; when a large number of samples are analyzed, the washing of the ion source is necessary several times a week. g) Benzalkonium chlorides can be derivatized with 100 mg of potassium tert-butoxide in the presence of benzene/dimethyl sulfoxide (DMSO) by its reaction at room temperature for 10 min [11]. They cannot be converted into t- BDMS or TMS derivatives in their unchanged forms. h) Nicotine can be analyzed by HPLC as follows. A 500-µL volume of a specimen solution (serum, gastric juice or urine), 2 mL diethyl ether, 500 µL of 5 M NaOH solution, 50 µL of Poisoning case, and toxic and fatal concentrations chlordiazepoxide solution (10 µg/mL, IS) are shaken for 3 min and centrifuged. The upper organic (diethyl ether) phase is mixed with 50 µL of 5 M HCl solution, shaken for backextraction and centrifuged. The lower aqueous phase is evaporated to dryness under a stream of nitrogen with warming at 50 °C. The residue is dissolved in 100 µL of a mobile phase; a 20-µL aliquot is injected into HPLC [12]. HPLC conditions are: column: Shimpack CLC-ODS (M) (25 cm × 4.6 mm i.d., Shimadzu Corp.); mobile phase: 10 mM NaH2PO4/10 mM Na2HPO4/methanol (20:20:60); flow rate: 1 mL/min; column (oven) temperature: 40 °C; detection: UV. References 1) Akutsu I, Motojima S, Ogata H et al. (1989) A case of benzalkonium chloride poisoning. J Jpn Soc Intern Med 78: 1613–1614 (in Japanese) 2) Hitosugi M, Maruyama K, Takatsu A (1998) A case of fatal benzalkonium chloride poisoning. Int J Legal Med 111: 265–266 3) Kotaki M, Fujimura N, Omote T (1996) A case of asphyxia by severe oropharyngeal edema and erosion with 10 % benzalkonium chloride (Osvan®) ingestion. Jpn J Toxicol 9:427–429 (in Japanese with an English abstract) 4) Berkel MV, Wolff AD (1988) Survival after acute benzalkonium chloride poisoning. Hum Toxicol 7:191–193 5) Suzuki I, Inoue T, Fukuda H (1991) Benzalkonium chloride. In: Manual of the 12th Edition of Japanese Pharmacopoeia. Hirokawa Publishing Co., Tokyo, pp c366–c369 (in Japanese) 6) Cybulski ZR (1984) Determination of benzalkonium chloride by gas chromatography. J Pharm Sci 73: 1700– 1702 7) Bleau G, Desaulniers M (1989) High-performance liquid chromatographic assay of benzalkonium in plasma. J Chromatogr 487:221–227 8) Kummerer K, Eitel A, Braun U et al. (1997) Analysis of benzalkonium chloride in the effluent from European hospitals by solid-phase extraction and high-performance liquid chromatography with post-column ionpairing and fluorescence detection. J Chromatogr A 774: 281–286 9) Study group of Gas chromatography of Japanese Society of Analytical Chemistry (translation) (1999) PTV splitless injection. In: Guidebook of Sample Introduction Techniques in CGC. Maruzen, Tokyo, pp 256–266 (in Japanese) 10) Study Group of Gas chromatography of Japanese Society of Analytical Chemistry (translation) (1989) Inactivation of the insert and packing materials. In: Guidebook of Sample Introduction Techniques in CGC. Maruzen, Tokyo, pp 49–54 (in Japanese) 11) Suzuki S, Nakamura Y, Kaneko M et al. (1989) Analysis of benzalkonium chlorides by gas chromatography. J Chromatogr 463:188–191 12) Saito M, Tamura Z (ed and translation) (1982) Nicotine. In: Drug Level Monitoring. Hirokawa Publishing Co., Tokyo, pp 254–258 (in Japanese) 413