Comparing Three Experimental Protocols for the Determination of
advertisement

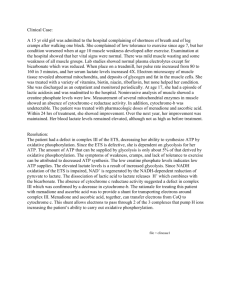
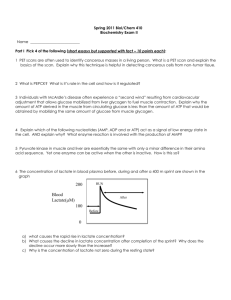
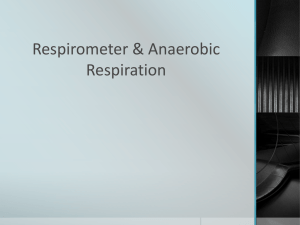
Comparing Three Experimental Protocols for the Determination of Blood Lactate Values by Rachel White A thesis submitted in partial satisfaction of the requirements of an undergraduate program in Biology for the degree of Bachelor of Arts May 1, 2007 Willamette University 2 ACKNOWLEDGEMENTS: I would like to thank Professor Stasinos Stavrianeas for his contribution and guidance in every aspect of this study, as well as Daniel Yaeger for his involvement with subject testing and data analysis. I would also like to thank the Willamette University Science Collaborative Research Program, M.J. Murdock Charitable Trust, Mary Stuart Rogers Foundation, and the National Science Foundation for their support in funding this project. I would also like to recognize Professor Janeba (Department of Mathematics) and Professor Stewart (Department of Psychology) for their constructive feedback on the statistical design of our study. ABSTRACT: Introduction: The measurement of blood lactate has long been used as marker of exercise intensity and training status. The abundance of methodologies for the determination of blood lactate levels during exercise renders comparisons of lactate values between studies difficult, often resulting in confusion over the meaning of such values. Purpose: We sought to compare a unique combination of three methods for determination of blood lactate levels, a necessary step in the interpretation of findings. Methods: We compared three commercially available products: two spectrophotometric methods, one using hydrogen peroxidase (HPO) and the other lactate dehydrogenase (LDH) as catalysts, and one lactate analyzer. We established the ideal combinations of sample volume, lysing agent, enzyme concentrations and total solution through a series of calibration curves over physiological range of lactate values (1-15 mmol/l). Capillary blood samples (25 µl) were analyzed from aerobically trained participants (n=4) who repeatedly performed a series of exercise bouts of varying intensities on a cycle ergometer, and the data were analyzed using an ANOVA (!=0.05). Results: Calibration curves for all three methods had almost perfect correlations over the physiological range tested: HPO (R2 = 0.9958), LDH (R2 = 0.9873), and the lactate analyzer (R2 = 0.9983). Although all three experimental protocols yielded similarly-shaped lactate curves, the actual values for the LDH method was significantly lower than the HPO and the lactate analyzer at every intensity level. For example, blood lactate levels at Maximum Lactate Steady State ranged from 2.82 mmol/l (HPO) to 2.52 mmol/l (analyzer), to 1.98 mmol/l (LDH). Conclusion: We were successful in comparing the three methods of lactate determination, and we provide a quantification of the differences between them. We conclude that all three methods can provide useful within-subject curves, and that the HPO method and the analyzer provide more consistent results than the LDH method. Finally, based on the lower operating costs and greater ease of use, we recommend the use of the lactate analyzer for work with blood lactate. 3 INTRODUCTION: LACTATE: Determination of blood lactate concentration is widely used to indicate exercise intensity in research with athletes and health status in critical care patients. Lactate is produced in regions of the body that have high rates of glycolysis including skeletal muscle, intestines, brain, skin, and red blood cells (Tofflaletti 1991). Glycolysis is the first phase of cellular metabolism and involves the breakdown of glucose into two pyruvic acid molecules. Some of the energy from the broken chemical bonds of glucose is used to convert two ADP into two ATP per glucose molecule that is processed in the ten step reaction of glycolysis (Sherwood 2004). In the presence of oxygen pyruvate will enter the Krebs cycle as it proceeds towards the process of cellular respiration. However, in the absence of oxygen, the pyruvate will be converted to lactic acid. Lactic acid is a strong organic acid (pKa 3.9) that dissociates into a proton (H+) and a lactate ion at a physiological pH, forming a salt called lactate. The terms lactic acid and lactate, therefore, are used interchangeably (Billat et al 2003). Although no ATP is produced when pyruvate is converted to lactate, this reaction is important because pyruvate is removed and NAD+ (rate limiting factor) is produced, promoting glycolysis (Tofflaletti 1991). Eventually, lactate that is produced in muscle cells is shuttled out of the cells and into the blood and transported to other tissues to be processed. Although there is a strong correlation between muscle and blood lactate concentrations during exercise, it is important to note that blood lactate accumulation reflects the difference between the release of lactate from muscle cells into the blood and the uptake of blood lactate by muscle and other tissue cells. This means that the majority of blood lactate produced is not a measure of lactate formed in muscle, but rather a net release of lactate. The heart, liver, and skeletal muscle are the primary sites for lactate removal from the blood and are responsible for using lactate as a substrate for gluconeogenesis and for glycogen synthesis, respectively (Weltman 1995). Billat, et al. (2003) advocate the lactate shuttle theory between and within cells as being supported by systematic lactate flux and whole body oxidation data. They maintain that the lactate shuttle across the interstitial and vascular areas supplies a 4 significant source of carbon for oxidation and gluconeogenesis at rest and during exercise. Lactate turnover is high at rest and increases in direct proportion to exercise intensity and metabolic demands. The intracellular shuttle allows glycolysis to produce lactate in the cytosol and transport it to the mitochondria within the cell of production for oxidative removal. The transport of lactate between muscle cells and blood is dependent on two barriers: the sarcolemma and the capillary membrane. The sarcolemma is a barrier for both the influx and efflux of muscle lactate, which is facilitated by a protein attached to the sarcoplasmic membrane (Billat et al. 2003). Richardson, et al. (1998) conducted a study on the role of the intracellular partial pressure of oxygen in lactate efflux from exercising skeletal muscle; their results indicate that increasing work rates causing lactate efflux is unrelated to muscle cytoplasmic partial pressure of oxygen. They did find, however, that lactate efflux is positively correlated with hypoxia and suggest that whether lactate formation during incremental exercise is due to muscle hypoxia remains controversial. These authors propose two contrasting models for lactate efflux, which include a saturable lactate-proton cotransporter, and the idea that efflux is linearly dependent on intracellular pH. These authors suggest that their data support the physiological model of lactate efflux that is dependent on intracellular pH, as they are linearly related without evidence of a transporter. APPLICATIONS: There are many practical applications of blood lactate measurements, which can be used in critical care settings and research in athletic performance. The blood lactate concentrations of critical patients can be monitored to determine if they are experiencing circulatory shock and need medical intervention. Tofflaletti (1991) reviewed the causes and treatments of hemodynamic deficits that lead to lactic acidosis, and the use of measurements in critical care monitoring—including the use of whole blood analyzers. There are many clinical considerations for the causes of hemodynamic deficits that lead to lactic acidosis, such as abnormal increase in blood hydrogen ion concentration, i.e. arterial pH below 7.35 (Powers & Howley 2004). Lactic acidosis is caused by circulatory shock whose primary characteristic is acute perfusion failure that impairs aerobic metabolism by decreased oxygen availability, or hypoxia to the tissues. Tofflaletti 5 suggests that the clinical causes of excess lactate are also due to vigorous muscle activity that stimulates an enhanced rate of glycogen metabolism. Arterial lactate concentrations can be used as a systemic indication of circulatory shock and can be measured by taking arterial whole blood samples from patients. The extracellular concentration of lactate is usually about 1 mmol/L, with a basal rate of lactate production at 1.0 mmol/kg/h (Tofflaletti 1991). Many protocols have been developed to analyze blood lactate, including enzymatic methods that are based on the reaction of lactate and NAD to form pyruvate and NADH. NADH can then be detected by either kinetic or end-point spectrophotometry at " = 340 nm. There are also automated lactate analyzers that use electrochemical sensors to measure lactate in whole blood samples within a few seconds, in a manner similar to the measurement of blood glucose levels for diabetics. These methods can be used to monitor a patient’s blood lactate levels while in critical care (Tofflaletti 1991). Toffaletti also recognizes that sports physiology lactate measurements can be useful for developing training schedules for athletes. Lactate levels can be analyzed at a specific exercise intensity, and training protocols can then be developed for the athlete to maintain a certain pace to achieve a target blood lactate concentration within a specific range. For example, lactate concentrations up to 4 mmol/L were historically used to indicate aerobic exercise, while ranges of 4-8 mmol/L were used to indicate anaerobic exercise (Tofflaletti 1991). LACTATE & EXERCISE: Blood lactate levels have a strong relationship with exercise intensity: as the intensity rises during incremental exercise, blood lactate accumulates in proportion to the number of muscle fibers recruited and the intensity of activation. For example, during the early stages of incremental exercise, slow-twitch muscle fibers are primarily recruited and produce minimal amounts of lactic acid. Slow-twitch muscle fibers are highly fatigue-resistant because they have a large number of oxidative enzymes, which gives them a high capacity for aerobic metabolism (Powers & Howley 2004). As exercise intensities increase, more fast-twitch muscle fibers—which have high amounts of glycolytic enzymes and, thus, a large anaerobic capacity—are recruited and undergo 6 glycolysis to meet the demands of ATP production. This increases muscle lactate production as well as blood lactate accumulation, which is curvilinear and becomes exponential as work and oxygen consumption increase (Weltman 1995). The blood lactate response to exercise is a widely used indicator of aerobic fitness, and is related to the rate of lactic acid production and blood lactate clearance. The energy consumption of skeletal muscle can increase up to 100-fold from rest when engaging in high intensity exercise causing a notable shift from aerobic respiration to glycolysis. When oxygen delivery or oxidative phosphorylation cannot meet the demands for ATP production during increasing exercise intensities, muscle fibers must rely primarily on anaerobic glycolysis to generate ATP (Sherwood 2004). Lactate accumulation denotes glycogen depletion as not all pyruvate can be converted into acetyl coenzyme A in the mitochondria to undergo oxidative phosphorylation (Billat et al. 2003). According to data presented by Katz and Sahlin (1990), lactate production during submaximal exercise is largely due to hypoxia, or a low partial pressure of oxygen available to mitochondria for aerobic respiration. They propose that a lack of available oxygen causes an increase in mitochondrial adenosine diphosphate (ADP), inorganic phosphate (Pi), and NADH, which stimulates glycolytic metabolism. This results in an increased cytosolic production of NADH that when combined with increased mitochondrial NADH induces a shift in lactate dehydrogenase (LDH) equilibrium towards a rise in lactate production (Weltman 1995). There are many other hypotheses that explain the mechanisms and reasons that muscle cells produce lactate. Sainsby and Brooks (1990) propose that although hypoxia plays a role in muscle lactate production, the #-adrenergic receptor system is the major factor that affects blood lactate. They suggest that #-adrenergic stimulation of skeletal muscle accelerates the rate of glycogenolysis, regardless of muscle activity. They advocate that other factors such as contraction pattern and duration, substrate availability, and hypoxia are all also vital in lactic acid production (Weltman 1995). Shulman (2005) performed a study on the formation of lactate from glycogen turnover during exercise, and he found that lactate can shuttle energy to from its location of synthesis (white fibers of skeletal muscle, brain) to other locations (red muscle fibers 7 or synaptic neurons) for oxidation. Shulman asserts that lactate is not a metabolic byproduct; it is synthesized to meet physiological demands by using its residual reductive capacity to provide energy in other organs of the body. He also proposes the glycogenshunt hypothesis, which maintains that glycogen produces ATP and lactate rapidly via anaerobic metabolism during exercise with net glycogenesis increasing to produce a dynamic steady state of glycogen concentration (Shulman 2005). 8 Blood lactate concentration (mmol/L) 7 6 5 4 MLSS 3 2 1 0 90 100 110 120 130 140 150 160 170 180 190 Exercise Intensity (Watts) Figure 1. Sample lactate curve: blood lactate concentrations are at a dynamic equilibrium at exercise intensities below MLSS, however, they increase exponentially at intensities above MLSS. One useful tool for athletes is the determination of their lactate threshold, since the blood lactate response to exercise is a consistent indicator of endurance performance. The deflection point on the lactate curve of Figure 1 indicates an individual’s maximal lactate steady state (MLSS), or the anaerobic threshold at which blood lactate accumulation is at a dynamic equilibrium with lactate clearance. At rest and at low intensities of exercise, the rate of lactate production and clearance is at an equilibrium—also called turnover (Billat et al. 2003). Increasing exercise intensities beyond this point results in a sharp rise in blood lactate accumulation because the rate of lactate loading into the bloodstream as a result of muscle activity surpasses the clearance rate (Weltman 1995). The metabolic clearance rate (MCR) is equal to lactate turnover divided by blood lactate concentration. Lactate disappearance is concentration dependent and is linearly related to arterial blood concentration during incremental exercise. During exercise, lactate removal via oxidation accounts for 75% of lactate clearance. NADH can 8 also be re-oxidized in the mitochondria by LDH during the transformation of lactate into pyruvate. At exercise intensities above maximal lactate steady state (lactate threshold), lactate accumulates in the blood as a result of lactic acid production exceeding its removal. It is the accumulation of protons, rather than lactate ions, that causes the pH of blood and skeletal muscles to drop (Billat et al. 2003). This phenomenon has been implicated in muscle soreness during intense exercise such as sprinting. This combined with the depletion of glycogen energy reserves causes the onset of muscle fatigue during anaerobic exercise (Sherwood 2004). In order to determine an individual’s MLSS, their blood lactate concentrations must be measured. MEASURING LACTATE: Following the notion that lactate accumulates in skeletal muscle and the blood during exercise, lactate concentrations can be measured by performing muscle biopsies or obtaining blood samples. Muscle biopsies are invasive procedures, and because the subjects in our study performed a continuous exercise protocol, this method was not a feasible option. Blood sampling was a much more practical method, as we could easily obtain venous blood samples through the finger tips of subjects during exercise tests. There are several techniques by which blood lactate can be measured. Historically, the spectrophotometer was the first method developed in the 1960’s to enzymatically analyze blood lactate levels. Then, in the 1980’s, automated analyzers were developed to increase the speed of blood lactate analysis at lower operating costs. Finally, in the 1990’s, portable hand held units were developed to make blood lactate analysis feasible in the field setting for research with athletes. Given the fact that there are so many ways to measure lactate, there has been a need to compare these methods in order to know how accurate they are. Most protocols involve obtaining blood samples and analyze lactate concentrations using two of the previously mentioned techniques. These studies have revealed a varying degree of accuracy and repeatability. One interesting finding is that the authors caution against comparing data obtained from different techniques. For example, one would not want to compare data from Lactate Pro hand held unit to data from a Sigma Diagnostics spectrophotometric technique. Some have even created algorithms to convert data from 9 one device to another to allow for comparisons of data across different methods (Pinnington & Dawson 2001). We sought to compare three different methods for the determination of blood lactate levels. Our objective was to determine which of the three methods is best to have a standard for data comparisons across literature analyzing lactate values. We will use the most accurate and reliable method for further studies on the metabolic effects of cardiovascular drift. METHOD: We compared blood lactate levels using two commercially available spectrophotometric methods, one of which has not been compared to other methods in the literature, and an automated lactate analyzer. Our procedures were based on existing literature and our protocols were identical to commonly accepted standards of measurement. EXERCISE PROTOCOL: This study was conducted in tandem with an MLSS determination study, in which study participants attended five separate exercise sessions where they rode a Monark 838E cycle ergometer at prescribed intensities controlled by a computerized motor system (Robobike). The first session was a maximal oxygen consumption (VO2max) test, followed by a submaximal bout of specific intensity (around MLSS), and three prolonged bouts of 45 minutes at maximal lactate steady state (MLSS), 95% MLSS, and 105% MLSS. In this way, out study differs from previous studies because we were able to measure blood lactate levels several times at each of several intensities to increase the consistency of our results. Simply put, we had multiple samples for each intensity at which our subjects exercised. For the first two tests, subjects performed exercise bouts in two-minute stages, with each stage increasing in intensity by 10-50 watts. In order to establish a protocol for the determination of MLSS, subjects were fitted with a gas mask that was attached to a ParvoMedics TrueOne metabolic gas analyzer, and ventilatory data were collected including minute ventilation (VE), O2 and CO2 concentrations and volumes, and heart 10 rate. The gas analyzer was calibrated using a known volume of gas before each exercise test, and the flowmeter was calibrated using a 3 L syringe. We obtained two capillary blood samples from each subject’s finger at the end of each stage: one whole blood sample of 25 µL was injected into an automated YSI 1500L Sport unit; and one whole blood sample of 50 µL was injected into an eppendorf tube containing 100 µL of 7% perchloric acid (PCA) cell lysing agent, which was then vortexed, centrifuged, and the supernatant was extracted and stored on ice for later spectrophotometric analysis. LACTATE ANALYSIS: We performed a comparative analysis of lactate values using three methods including spectrophotometric protocols of Sigma Diagnostics and Trinity Biotech (not found in literature), as well as an automated analyzer, YSI 1500L Sport. Sigma Diagnostics: The lactic acid levels of the blood samples were measured enzymatically according to the following reaction: Lactic acid + NAD+ ––LDH! pyruvic acid + NADH Pyruvate + hydrazine ! pyruvate hydrazone We used a blank consisting of 1 mL of lactate reagent and 25 µL de-ionized water, and we made new 25 mL batch of reagent cocktail daily (8 mL of 1 M glycine, 0.4 mL of ~400U/mL lactate dehydrogenase (LDH), 0.6 mL of 0.1 mM NAD, 0.4 mL of 20 M (100%) hydrazine, and 15 mL de-ionized water) to ensure chemicals were fresh and untainted. First, we created a standard calibration curve using standards of known concentrations (" = 340 nm). Lactate standards of concentrations ranging from 5-120 mg/dL were created from dilutions of 20, 80, and 120 mg/dL stock standards, and 25 µL of each standard was added to 1 mL lactate reagent in separate 1 mL cuvettes. All samples were compared against the calibration curve. Each standard dilution was analyzed in duplicate and incubated for a total of one hour; absorbance values were recorded every ten minutes. Duplicate absorbance values were averaged and then used to 11 calculate lactate values. Standard calibration curves were then generated to determine their correlation over the physiological range (0-15 mmol/L). We used disposable 1 mL cuvettes and mixed 1 mL lactate reagent with 25 µL supernatant fluid of centrifuged blood samples diluted three-fold with 7% PCA (all samples analyzed in duplicate). The cuvettes were incubated for one hour and we recorded their absorbance values every 10 minutes. From the standard curve that was established, we created a regression curve, which we used to determine the lactate concentrations of unknown samples. Trinity Biotech: The lactate levels of the blood samples were measure enzymatically according to the following reaction: Lactate + lactate oxidase ! pyruvate + H2O2 Presence of H2O2: peroxidase –-catalyzes! oxidative condensation of chromogen precursors ! color change (Solution becomes purple: degree of color saturation is lactate concentration dependent) We used a blank consisting of 1 mL of lactate reagent and 10 µL de-ionized water, and lactate reagent was reconstituted from reagent powder (400 µ/l lactate oxidase, 2400 µL/l peroxidase, chromogen precursors (as required), and buffer (pH 7.2)) and 10 mL deionized water. We performed a Trinity spectrophotometric analysis using similar methods. We ran calibrations at " = 540 nm, and created appropriate standard dilutions from 20, 80, and 120 mg/dL standards by mixing 10 µL of each standard with 1 mL Trinity lactate reagent in separate 1 mL cuvettes. The cuvettes were incubated for a total of fifteen minutes; absorbance values were recorded every five minutes. We then generated correlations of the standard values to validate the protocol. The increase in absorbance was directly related to the concentration of lactate in the cuvette sample. We used 1 mL cuvettes and mixed 1 mL lactate reagent with 25 µL supernatant fluid of centrifuged blood samples diluted three-fold with 7% PCA (all samples run in duplicate). The cuvettes were incubated for fifteen minutes and their absorbance values were recorded every five minutes. We then analyzed results by regression analysis to determine the lactate concentrations of unknown samples. 12 YSI 1500L Sport: Lactate levels were measured enzymatically according to the following reaction that took place in the sample chamber between the whole blood sample and the trilayered enzyme membrane and probe: Lactate + lactate oxidase ! hydrogen peroxide Hydrogen peroxide + platinum anode ! electron current Prior to data collection, we performed calibrations and linearity checks with standard lactate solutions in concentrations ranging from 1-30 mM diluted from 5 mM and 30 mM standard stock solutions. We also performed calibration procedures before each exercise test, using the 5 mM standard as recommended by the manufacturer. After calibrating the instrument, whole blood samples of 25 µL were injected into the sample chamber using a calibrated syringe pipette, and the blood lactate concentration of the sample was analyzed within one minute. The probe inside the buffer-filled sample chamber is fitted with a three-layer enzyme membrane containing layers of polycarbonate, lactate oxidase, and cellulose acetate that is in direct contact with the silver-platinum probe. When a sample is injected into the chamber, lactate oxidase rapidly oxidizes the substrate to produce hydrogen peroxide, which is then oxidized at the platinum anode to produce an electron current. When the rate of hydrogen peroxide production equals the rate of clearance from the enzyme layer a dynamic equilibrium is achieved, therefore, the flow of electrons is linearly proportional to the constant hydrogen peroxide concentration, as well as the lactate concentration (User’s Manual YSI 1500 Sport L-Lactate Analyzer: Section 5-1 2003). STATISTICS In all measurements we compared the blood lactate concentrations obtained at the same time and analyzed with different instruments. We ran an ANOVA analysis (!=0.05) to determine whether there were significant differences between the mean values of the three different methods. We also compared standard curves and lactate trends from methods of the same instrument (Sigma vs. Trinity), as well as between instruments (spectrophotometry vs. YSI). 13 RESULTS: 3.0 y = 0.2512x - 0.0467 R2 = 0.9873 Absorbance 2.5 Trinity Biotech Sigma Diagnostics 2.0 1.5 y = 0.1767x - 0.0376 R2 = 0.9958 1.0 0.5 0.0 0 3 6 9 12 15 Concentration of Standard (mmol/l) Figure 1. Spectrophotometric calibration curves for the Sigma Diagnostics and Trinity Biotech methods. The standard curves were created by reading known lactate concentrations at their specific wavelength. All different volume calibrations yielded high correlations including the ones we used in our study: Trinity (R2 = 0.9958), Sigma (R2 = 0.9873). These high correlations over the physiological range gave us confidence that our Measured Concentrations (mmol/l) instruments would give us reliable data. 10 9 8 R2 = 0.9983 7 6 5 4 3 2 1 0 0 2 4 6 8 10 12 Standard Concentrations (mmol/l) Figure 2. Standard calibration curve for the YSI 1500L Sport analyzer. 14 Standard calibrations for the YSI method also yielded high correlations over the physiological range (R2 = 0.9983). Sample Lactate Graph Using 3 Different Methods 10 Blood Lactate Concentration (mmol/L) 9 8 YSI Sigma Trinity 7 6 5 4 3 2 1 0 50 75 100 125 150 175 200 225 Exercise Stage (Watts) Figure 3. Sample lactate curve using the three different methods of blood lactate analysis. Although all three experimental protocols yielded similarly shaped lactate curves (R2 = 0.989-0.995), the values obtained from the Sigma method were significantly lower from the Trinity and the YSI at every intensity level (p<0.05). Even though all three techniques identified the specific intensity of MLSS, all three methods yielded different lactate values for MLSS, ranging from 2.82 mmol/l (Trinity) to 2.52 mmol/l (YSI), to 1.98 mmol/l (Sigma), with the results of the Trinity and YSI protocols were more similar than the Sigma protocol. DISCUSSION: The purpose of our study was to compare three different methods for the determination of blood lactate levels to conclude which one we will use in future studies. We were successful in comparing the three methods of lactate determination, and provided a quantification of the differences between them. We concluded that all three 15 methods can provide useful lactate curves within each subject, and that the Trinity and YSI methods provide more similar results than the Sigma method. Finally, since all methods can consistently track changes in blood lactate for future studies working with blood lactate, we recommend the use of the YSI analyzer to give valid measurements because it has the lowest operating cost and it is easiest method to implement. PROTOCOL VERIFICATION: In order to verify our methodology, we tested different ratios of the Sigma reagent to lactate standard/sample including 25 µL /1 mL, 15 µL /500 ml, 5 µL /1 mL, 50 µL /1 mL, and 25 µL /500 ml. We chose to use the recommended ratio of 25 µL /1 mL because it gave us the most consistently high correlations with the standard calibrations. We also measured effects of time, and found that one hour caused no changes in absorbance values. We tested different ratios of Trinity reagent to lactate standard/sample including 5 µL /500 ml, 5 µL /1 mL, 15 µL /500 ml, 10 µL /1 mL and 50 µL /1 mL to determine if percent error of micropipetting could be reduced with larger sample volumes. We decided to use to recommended ratio of 10 µL /1 mL for data collection. We also compared water and reagent blanks (1.015 mL), and found that values were slightly lower (0.01-0.02 abs) with the reagent blank. We chose to use the reagent blank (1 mL reagent and 15 µL de-ionized water) for data collection to ensure our samples would be accurately measured. In order to ensure the accuracy of our lactate values, we verified our spectrophotometric methodology with the following tests. In one test, we experimented with blood volumes in the cuvette solution ranging from 10-50 µL. We also tested PCA dilution factors including 25 µL blood in 100 µL of 7% PCA (1:5), 25 µL blood in 200 µL PCA (1:9), and 50 µL blood in 100 µL PCA (1:3). We also compared 7% PCA to 3% PCA, and found the 3% PCA to give slightly higher lactate values, so we decided to use recommended concentration of 7% PCA. We also ran calibrations of standards mixed with 7% PCA to simulate sample tests and compared it against a calibration of standards diluted with water. We found that the absorbance values were very similar, therefore, we could safely conclude that the PCA did not interfere with LDH in reagent. We also ran 16 calibrations with standard concentrations ranging from 5-120 mg/dL to verify a linear relationship (correlation) over the physiological range. For the spectrophotometric calibrations, we made standard dilutions with 20, 80, and 120 mg/dL standards as well as only 120 mg/dL to eliminate fluctuations and create a more linear correlation. We found these different calibrations had similar absorbance values, therefore, the dilutions were accurate. In addition, we compared the precision of 1mL cuvettes to 0.5 mL cuvettes, and found that if we made even a 1 µL micropipette error, our results would be much less precise when using a 0.5 mL solution as compared to a 1 mL solution. We decided to use 1 mL to decrease percent error of our data. We decided to use the 1 mL cuvettes in order to reduce the percent error of micropipetting. We compared three methods to verify lactate standard values using the Trinity equation, Sigma equation, and standard calibration curves. We chose to use standard curves to calculate lactate values for both the Sigma and the Trinity. All three of the standard curves indicated high precision of the instruments. Bishop et al. (1992) conducted a study comparing the Yellow Springs Instruments (YSI), and Boehringer Mannheim (BMM) methods of lactate analysis, as well as the influence of the lysing agent Triton X-100 (TX) on lactate concentrations of the YSI analyzer. They found that the YSI with TX buffer had higher values that differed significantly by < 3% from the YSI with non-TX buffer. They also found significant differences in lactate values between the BMM with YSI-nonTX, but not between the BMM and YSI-TX instruments, which were highly correlated (R2 = 0.99). The BMM method uses LDH as a catalyst for the formation of pyruvate and NADH from lactate and NAD+, and the NADH is measured spectrophotometrically at 340 nm. This method is identical to the Sigma method used in our own study, as was the non-TX YSI method. The results from this study are consistent with the data from our experiments as their YSI values were also statistically different from the Sigma values. Their YSI values were lower than the Sigma values, but this may have resulted from using a different buffer solution for the blood sample used in spectrophotometric analysis. In their experiments, they added 17.5 mg sodium fluoride and 14 mg potassium oxalate to their blood sample and stored it on ice for later analysis, while we added 100 µL 7% PCA to our blood samples and chilled them as well. These authors also note that is it important to 17 recognize that mean differences are applicable to group data, but do not necessarily reflect errors made in any specific measurement. In a study conducted by Medbo et al. (2000) comparing the imprecision of four different lactate analyzers including two types of YSI instruments (YSI 23L and YSI 1500) and three less expensive analyzers, they found that most of the different instruments had values that were systematically too high or too low (10-25% deviation). These differences are important because they may distort an athlete’s lactate threshold by 2-5%. They even observed different values between the two YSI 1500 instruments. When comparing all of these methods to their reference method of standard enzymatic photofluorometry, the authors determined that the YSI instruments were superior to most of the other lower-cost methods (except for the Lactate Pro that was as good as the YSI instruments). Their enzymatic photofluorometry method involved the use of a PCA red blood cell lysing agent, as well as a LDH reaction that initiates NADH formation with the use of Sigma reagent chemicals. This method is similar to the one used in our own research, and their results support our data in which the YSI values of non-hemolyzed blood differed by 20-25% than those of the Sigma method because the lactate produced by red blood cells was not measured. This particular study also found YSI values to be consistently lower than the Sigma values, which may be because they used a different concentration of PCA for their Sigma samples: these authors used 500 !L of 0.4 mmol/L PCA, while we used 100 !L of 7% PCA. Buckley, et al. (2003) conducted a study evaluating three different automated lactate analyzers (Accusport, Lactate Pro, and YSI 1500 Sport) while testing subjects at their respective MLSS. They determined that the use of difference analyzers did not have an effect on MLSS. The YSI instrument yielded blood lactate values that were 1.1 +/1.0 mmol/L lower than Accusport values and 1.6 +/- 1.6 mmol/L lower than Lactate Pro values at all stages of testing. The authors also noted that differences between analyzers were minimized at low blood lactate concentrations, and increased as blood lactate concentrations rose, which was consistent with our data trends. These authors conclude that MLSS should be determined based on relative changes in blood lactate concentrations because an athlete’s threshold is not affected significantly by different values provided by different analyzers. 18 A study performed by Pyne et al. (2000) comparing the accuracy and reliability of the Lactate Pro analyzer in relation to three other analyzers (ABL 700 Series Acid-Base, Accusport Lactate Meter, and YSI 2300 Stat) found that the Lactate Pro was highly correlated with all three methods (r > 0.96). The YSI 2300 Stat is similar to the YSI 1500L Sport we used in our study, with the additional capacity of blood glucose analysis. (These authors, however, used hemolyzed blood samples, while we used non-hemolyzed blood samples.) The authors concluded that Lactate Pro is accurate and reliable, therefore, since it also exhibits a high correlation with the YSI 2300 Stat, then YSI instruments must be reliable as well. These authors used the “limits of agreement” analysis as a measure of absolute reliability to overcome the limitations concerned with standard errors of the mean (SEM) and coefficient of variation (CV). The results of their evaluation show Lactate Pro data to be homeoscedastic. In other words, there is no obvious relationship between the degree of disparity between analyzers and level of lactate measured. Noordally et al. performed a study to determine the reliability of three different methods including the Chiron M865, YSI mode 2300, and Hitachi 911, and found that all methods were highly correlated (R2 > 0.98). They determined that the Chiron M865 lactate analyzer is reliable for whole blood sample measurements, and since the YSI mode 2300 had a high degree of agreement with the Chiron M865, we can infer that the YSI 1500L Sport instrument yields consistent results as well and will be a reliable source for future studies using blood lactate analysis. While these studies provide valid comparisons between the different methods of blood lactate analysis, the authors argue that these are only relative value comparisons because it is impossible to discern absolute values of lactate. In the case of our study, we found that the Trinity and YSI methods gave the most similar data values, and since the YSI gives faster results at a lower cost we will use this analyzer in future studies with blood lactate. POSSIBILITIES FOR IMPROVEMENT: The major difficulty in this study was the collection of multiple blood samples in a very short time. Although the timing of the blood collection was very close, 19 occasionally some of the samples did not correspond very closely. It was especially problematic when a subject’s blood clotted at the sampling site, forcing us to puncture their finger multiple times. This could have resulted in the blood samples taken farther apart than the average time of 30 seconds, resulting in different lactate values. For example, difficulties in obtaining the two blood samples taken for the YSI and spectrophotometer may have caused the second sample to have a higher lactate concentration because it was taken a 1-2 minutes later. Some of the blood samples may have also been diluted by interstitial fluid from squeezing a subject’s finger too hard or too long, resulting in a lower lactate value. It is also possible that some batches of the spectrophotometric chemicals were tainted when we reconstituted the Trinity reagent, or made the Sigma reagent cocktail. There is an especially high chance for error in creating the Sigma reagent since we made a new batch of 25 mL everyday, increasing the chances of variability in the reagent composition. REFERENCES: 2003. User’s Manual YSI 1500 Sport L-Lactate Analyzer. Yellow Springs (OH): YSI Incorporated 97 p. Beneke R. 2003. Methodological aspects of maximal lactate steady state—implications for performance testing. European Journal of Applied Physiology 89: 95-99. Billat VL, Sirvent P, Py G, Koralsztein J-P, Mercier J. 2003. The concept of maximal lactate steady state. Sports Medicine 33(6): 407-426. Bishop PA, Smith JF, Kime JC, Mayo JM, Tin YH. 1992. Comparison of a manual and an automated enzymatic technique for determining blood lactate concentration. International Journal of Sports Medicine 13(1): 36-39. Buckley JD, Bourdon PC, Woolford SM. 2003. Effect of measuring blood lactate concentrations using different automated lactate analysers on blood lactate transition thresholds. Journal of Science and Medicine in Sport 6(4): 408-421. Davison RC, Coleman D, Balmer J, Nunn M, Theakston S, Burrows M, Bird S. 2000. Assessment of blood lactate: practical evaluation of the Biosen 5030 lactate analyzer. Medicine & Science in Sport & Exercise 243-247. Detry B, Nullens W, Cao ML, Frans A, Robert A, Clerbaux T. 1998. Assessment of the lactate biosensor methodology. European Respiratory Journal 11: 183-187. 20 Medbo JI, Mamen A, Olsen OH, Evertsen F. 2000. Examination of four different instruments for measuring blood lactate concentration. Scandinavian Journal of Clinical Laboratory Investigations 60: 367-380. Myers J., Ashley E. 1997. Dangerous curves. A perspective on exercise, lactate and the anaerobic threshold. Chest 111:787-795. Noordally O, Vincent J-L. 1999. Evaluation of a new, rapid lactate analyzer in critical care. Intensive Care Medicine 25: 508-513. Pinnington H, Dawson B. 2001. Examination of the validity and reliability of the Accusport blood lactate analyzer. Journal of Science and Medicine in Sport 4(1): 129138. Powers SK, Howley ET. 2004. Exercise Physiology: Theory and Application to Fitness and Performance, 5th Ed. Boston: McGraw/Hill. 519 p. Pyne DB, Boston T, Martin DT, Logan A. 2000. Evaluation of the Lactate Pro blood lactate analyzer. European Journal of Applied Physiology 82: 112-116. Richardson RS, Moyszewski EA, Leigh JS, Wagner PD. 1998. Lactate efflux from exercising human skeletal muscle: role of intracellular PO2. Journal of Applied Physiology 627-634. Sherwood L. 2004. Human Physiology, From Cells to Systems. 5th Ed. United States: Thomson & Brooks/Cole. 629 p. Shulman RG. 2005. Glycogen Turnover Forms Lactate during Exercise. Exercise and Sport Science Reviews 33(4): 157-162. Suga A. 1990. Ventricular Energetics. Physiological Reviews 70(2): 247-277. Toffaletti JG. 1991. Blood Lactate; biochemistry, laboratory methods, and clinical interpretation. Critical Reviews in Clinical Laboratory Sciences 28(4): 253-268. Weltman A. 1995. The Blood Lactate Response to Exercise. Current Issues in Exercise Science: Monograph Number 4. Human Kinetics. 21