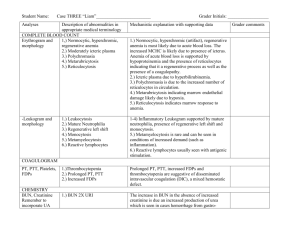
Lab Test Interpretation Table

Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Lab Test Interpretation Table
Normal Range Interpretation Tips
Hematology
White Blood Cell Count (WBC)
& Differential
Leukocytes/WBC 4.5-10.5 x 10
9
/L
Neutrophils
-
Absolute Neutrophil Count (ANC) =
3 - 7 x 10
9
/L
-
Calculated ANC =
WBC x (segs+bands) / 100
Band neutrophils: < 0.7 x 10
9
/L
Basophils < 0.10 x 10
9
/L
Eosinophils < 0.45 x 10
9
/L
Lymphocytes 1.5-3.4 x 10
9
/L
Monocytes 0.14-0.86 x 10
9
/L
Increased Counts
-
Leukocytosis and neutrophilia can be caused by many factors including infection, myeloproliferative disorders, inflammation, and medications. In cancer patients, support medications such as corticosteroids and colony stimulating factors can cause elevated counts.
No treatment is required unless they are associated with bone pain, which may improve with analgesic therapy.
-
When leukocytosis is accompanied by increased immature neutrophils (bands) and fever, infection is a likely cause. Band neutrophils often increase in numbers to fight infections (also called “a shift to the left”).
-
For patients receiving riTUXimab, lymphocyte counts above 25-30 x 10
9
/L increase the risk of cytokine-release syndrome. Consult protocol and/or tumor group chair for recommendations.
Decreased Counts
-
Leukocytopenia and neutropenia can result from nutritional deficiency, autoimmune disease, bone marrow infiltration (i.e., leukemia or myelodysplastic syndrome), radiation, and medications (including many chemotherapy drugs).
-
Many chemotherapy protocols require dose adjustments or the addition of colony stimulating factors (e.g., filgrastim) if ANC drops below 1.5 x 10
9
/L. Some protocols may tolerate even lower levels.
Platelets (Thrombocytes)
150 –450 x 10 9
/L
-
Febrile neutropenia is defined as the presence of neutropenia plus concurrent fever (single oral temperature of > 38.3 o
C orally or > 38 o
C over 1 h). It is a medical emergency that requires treatment with antibiotics +/- support medications.
Increased Counts
In patients with myeloproliferative disorders, thrombocytosis or thrombocythemia is
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
1
Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Normal Range Interpretation Tips generally caused by the malignancy.
In cancer patients without a myeloproliferative disorder, it is prudent to notify the ordering physician if thrombocytosis occurs. It does not generally require treatment unless the patient is symptomatic.
Prothrombin Time (PT)
10-13 sec
Decreased Counts
-
Many chemotherapy protocols require a dose reduction or delay if the platelet count is < 100 x 10
9
/L.
Erythrocytes (RBCs)
Females: 3.5-5 x 10
Males: 4.3-5.9 x 10
12
12
/L
/L
Hemoglobin (Hgb)
Increased Counts
Erythrocytosis and hemoglobinemia can occur in a variety of medical conditions such as congenital heart disease, polycythemia vera, dehydration and high altitudes.
Decreased Counts Females: 120-160 g/L
Males: 140 –180 g/L
Albumin
35-50 g/L
Decreased Hgb and RBCs can result from chronic anemia, cancer, hemorrhage, hemolysis, nutritional deficiency or medications
(including many cancer drugs).
Liver: Tests that Reflect the Liver’s Synthetic Ability
Albumin is synthesized by the liver and can be an indicator of the liver’s synthetic ability.
However, because it has a half-life of 20-30 days, it is not useful in assessing acute hepatic injury as levels often remain normal in acute disease.
-
Low albumin levels can occur in chronic diseases such as cirrhosis, cancer and malnutrition.
-
The liver is responsible for synthesizing a number of clotting factors. Liver damage can significantly prolong PT and increase the risk of bleeding.
Unlike albumin, PT is a good reflection of acute changes in liver function because of the short half-life of specific clotting factors. However, vitamin K deficiency must be ruled out because it is an essential cofactor in the clotting cascade. Other factors that can prolong PT include warfarin therapy and inherited clotting factor deficiencies.
-
PT may rise to 50 sec or greater in acute liver
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
2
Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Normal Range Interpretation Tips failure.
PT is usually 2-5 times the upper limit of normal
(ULN) in cirrhosis.
Liver: Tests for Hepatocellular Injury
Alanine aminotransferase (ALT) -
ALT is primarily located in hepatocytes, but
[Formerly Serum Glutamic Pyruvic also be found in the skeletal muscle, heart and
Transaminase, (SGPT)] kidneys.
7-53 units/L (varies with assay)
-
ALT is usually < 300 units/L in alcoholic hepatitis.
Aspartate Aminotransferase (AST)
[Formerly Serum Glutamic Oxaloacetic
Transaminase, (SGOT)]
11-47 units/L (varies with assay)
Very high ALT levels (1000 units/L) are most commonly due to viral hepatitis, ischemic hepatitis, or liver injury due to drug or toxin.
-
AST is a less specific indicator of hepatic injury than ALT because it is found in the liver, heart, skeletal muscle, kidneys, brain, lung and pancreas.
AST elevation generally indicates liver damage if ALT, bilirubin and ALP are also elevated.
Very high AST levels (1000 units/L) are most commonly due to viral hepatitis, ischemic hepatitis or liver injury due to drug or toxin.
AST/ALT Ratio
0.8
-
Isolated AST elevation (without ALT elevation) may indicate cardiac or muscle disease. This is often accompanied by an elevated serum creatine kinase.
A ratio < 1 can occur with non-alcoholic hepatitis or fatty liver disease.
A ratio > 1 can occur with cirrhosis, liver metastases or congestion from antineoplastic agents.
-
A ratio > 2 occurs in 70% of patients with alcoholic liver disease, where the AST is generally at least twice the ALT, and the ALT is rarely > 300 units/L.
Lactate Dehydrogenase (LDH)
Normal levels 160-450 IU/L (varies with assay)
-
A ratio > 3 can occur immediately after muscle injury.
-
LDH is present in most tissues, particularly the heart, kidneys, liver and skeletal muscle. There are 5 isoenzymes of LDH. LDH-5 is associated with the liver.
LDH is used in oncology to monitor tumor progression for some tumors and as a
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
3
Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Normal Range Interpretation Tips prognostic factor in lymphoma.
Liver: Tests for Cholestasis
Alkaline Phosphatase (Alk Phos, ALP) -
ALP is found in the liver, bone, intestinal tract, placenta, kidneys and leukocytes.
20-130 units/L (varies with assay)
-
Bile accumulation increases liver synthesis of
ALP; levels tend to normalize within 2-4 weeks after the cholestasis is resolved.
-
Levels > 3 times ULN are generally associated with cholestasis.
Levels < 3 times ULN in the presence of other elevated LFTs are generally indicates a hepatocellular source.
-
Levels < 3 times ULN in the absence of other elevated liver function tests generally indicate non-hepatic causes.
Total Bilirubin
2-18 umol/L
Very high ALP levels (>1000 units/L) often occur with indicate hepatic infiltration.
Some tumors (i.e., osteosarcomas, lung, gastric head and neck, renal, ovarian, uterine and Hodgkin lymphoma) can secrete ALP or cause it to leak into the serum.
-
80% of bilirubin is derived from metabolism of hemoglobin that is released from destroyed red blood cells. The remaining 20% is derived from other heme proteins.
-
Total serum bilirubin levels may be normal in the presence of liver injury. The liver has a reserve capacity to remove at least twice the normal daily bilirubin load.
Gamma Glutamyl Transpeptidase (GGT,
GGTP or GTP)
Male 9-50 units/L
Female 8-40 units/L
High levels, when accompanied by elevation in aminotransferases, generally indicate hepatitis or cirrhosis.
-
High levels, when accompanied by elevations in ALP and GGT, suggest a cholestatic disorder.
-
GGT is considered the most sensitive test for cholestatic disorders. However, it lacks specificity since it can be found in many tissues including the liver, kidneys, pancreas, spleen, heart, brain and seminal vesicles.
-
Because GGT is not found in the bone, it is useful in determining whether ALP elevations
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
4
Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Normal Range Interpretation Tips are secondary to liver or bone pathology. If both ALP and GGT are elevated, the source is likely the liver.
Serum Creatinine (SCr)
Female
62 –115 micromol/L
Male 80 –124 micromol/L
Blood Urea Nitrogen (BUN)
2.1
–7.9 mmoL/L
-
A twofold increase in GGT is suggestive of alcoholic liver disease when it is accompanied by an AST/ALT ratio > 2.
A GGT/ALP ratio > 2.5 suggests alcohol abuse.
Renal Function Tests
-
Creatinine is a product of muscle breakdown.
SCr alone is not very useful as many variables
(i.e., nutritional status, muscle mass, ingestion of meat) can affect the levels.
BUN:SCr Ratio (both values in mg/dL)
10:1 –15:1
Conversion to mg/dL:
BUN mg/dL = BUN mmol/L x 2.8
Scr mg/dL = Scr micromol/L x 0.01131
-
SCr is more useful when compared to BUN
(see BUN:SCr Ratio below).
Urea is a toxic nitrogen waste product of protein and amino acid metabolism. Increased levels can be caused by kidney disease, increased protein intake or increased protein breakdown from muscle damage or upper GI bleeds.
Normal ratio (10:1-15:1) may occur with:
Intrinsic renal disease
Reduced protein intake or liver disease accompanied by volume depletion
Elevated ratio (> 15:1) may occur with:
-
Prerenal causes (i.e., reduced delivery of blood to the kidneys from dehydration, blood loss or shock)
Postrenal causes (i.e., obstruction of urine flow from kidneys)
Although an elevated ratio is considered to be
> 15:1, prerenal and postrenal disease usually cause ratio’s > 20:1
-
Non-renal causes (i.e., tissue breakdown, loss of muscle mass or corticosteroid administration)
A ratio > 20.1 is not clinically significant if both the BUN and SCr are within normal limits
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
5
Clinical Pharmacy Guide: Chemotherapy Assessment and Review 4th Edition
Normal Range Interpretation Tips
Reduced ratio (<10:1) may occur with:
Hepatic dysfunction
Reduced protein intake
-
The most accurate method of assessing GFR is to measure it by nuclear renogram.
Creatinine Clearance (CrCl), Glomerular
Filtration Rate (GFR)
75 –125 mL/min
Lab Test Interpretation Table
Activated: September 2014 Revision Date: April 2, 2015
6