Oxytocin Basics 101
advertisement

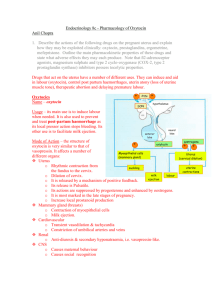
Oxytocin Basics 101 Oxytocin Pharmacology During the first stage of spontaneous labor, maternal circulating concentrations of endogenous oxytocin are approximately that of a continuous infusion of exogenous oxytocin at 2 to 4 milliunits/minute. During labor, the fetus is thought to secrete about 3 milliunits/minute of oxytocin. Thus, the maternal plus fetal contribution of maternal plasma oxytocin concentration is equivalent to a range of 5 to 7 milliunits/minute. The biologic ½ life of oxytocin is 10 to 12 minutes. The uterine response to oxytocin usually occurs within 3 to 5 minutes of IV administration. There is an inverse relationship between the duration and dosage of oxytocin and the number of oxytocin receptor sites available for oxytocin uptake throughout labor. Continued increases in oxytocin rates over a prolonged period of time can result in oxytocin receptor desensitization (down regulation). This makes oxytocin less effective in producing normal uterine contractions resulting in the opposite of the intended effect. Abnormal uterine activity such as persistent coupling or tripling of contractions, or uterine tachysystole may be the end result of continued increases in oxytocin rates. Normal Contraction Pattern 90% of pregnant women at term will have labor successfully induced with 6 milliunits/ minute or less of oxytocin. Adequate uterine activity has been identified as contractions that occur approximately every 2 to 4.5 minutes and measure 24 to 75 mm Hg in intensity. Resting tone of the uterus between contractions should be 15 to 20 mm Hg with the uterus being soft when palpated. (It is important to assure that resting tone is calibrated.) The duration of contractions should be approximately 60 to 90 seconds in length. Oxytocin Titration At least a 30 minute interval is recommended between oxytocin dosage increases (HCA recommendation) because the full effect of oxytocin on the uterine response to increase dosage cannot be evaluated until steady-state concentration has been achieved. Increasing the infusion rate before steady-state concentrations are achieved results in laboring women receiving higher than necessary dosages of oxytocin. Higher doses and shorter dose intervals lead to more uterine tachysystole and abnormal FHR patterns, and do not result in a clinically significant decrease in length of labor. Once active labor is established in women undergoing induction, oxytocin may often be discontinued, and may avoid receptor down regulation. This is especially true in cases of active labor after rupture of membranes. Impact of Uterine Activity on Fetal Status The more time there is between contractions, the more time there is to maximally perfuse the placenta and deliver oxygen to the fetus. Fetal Sp02 decreases during contractions, reaching the lowest level 92 seconds after the peak of the contraction. Approximately 90 seconds is required for fetal Sp02 to return to normal levels. When contractions are occurring every 2 minutes or more often, recovery of fetal Sp02 to previous baseline levels is incomplete. Contraction intervals of less than 2-3 minutes are less favorable on fetal cerebral oxygen saturation when compared with longer contraction intervals. Contractions occurring repeatedly more frequently than every 2 to 3 minutes are likely to result in progressive fetal cerebral desaturation. Tachysystole over the last hour of the second stage of labor is significantly associated with a higher incidence of fetal academia at birth when compared with less frequent contractions. When the FHR is abnormal, the oxytocin should be decreased or discontinued. It makes little sense to give oxygen for fetal indications and at the same time continue the oxytocin infusion unchanged. Resumption of Oxytocin after Resolution of Tachysystole Resumption of the oxytocin infusion should be delayed until uterine activity returns to normal and the FHR tracing is normal. If oxytocin has been discontinued for less than 20-30 minutes, the FHR is reassuring, and contraction frequency, intensity, and duration are normal, then resume oxytocin at no more than half the rate that caused the hyperstimulation and gradually increase the rate as appropriate based on hospital protocol and maternal-fetal status. If the oxytocin is discontinued for more than 30-40 minutes, resume oxytocin at the initial dose ordered. (These are AWHONN recommendations) Points to Remember: Titrate the oxytocin to the maternal-fetal status and in accordance with the oxytocin checklist criteria. Complete the checklist at the bedside as you are doing the assessment, promptly, every 30 minutes. Administer oxytocin only with an interpretable EFM tracing. Inductions with the patient on the birthing ball or walking the hallway are fine if the strip is interpretable and normal. FHR monitoring by auscultation only is not appropriate with oxytocin infusing. The patient must be continuously monitored for oxytocin to continue. Stop oxytocin during: Prolonged decelerations Epidural administration if you cannot monitor the baby Oxygen administration if oxygen is thought necessary The time waiting for an OR for a C-section or waiting for a C-section Nursing Responsibilities during Oxytocin Infusion: Carefully titrate the drug to the maternal-fetal response. The titration process includes decreasing the dosage or discontinuing the medication when contractions are too frequent, discontinuing the medication when the fetal status is non-reassuring and increasing the dosage when uterine activity and labor progress are inadequate. Document interventions and patient response. Communicate patient’s status both verbally and in writing to appropriate members of the healthcare team. Written and verbal communication includes: Baseline, Variability, Accelerations, Decelerations, Episodic or periodic baseline changes, Trends *Recent research data by the Hospital Corporation of America (HCA) has now established the use of the oxytocin administration checklists as the standard of care for their large hospital system. Non-compliance clearly showed increased adverse fetal outcomes. Source: “Oxytocin Strategies for Improving Maternal and Neonatal Outcomes”, HealthStream online perinatal courses