Practitioner Version
EMT / P / AP
EMT / P / AP
EMS Flashcards ‐ Practitioner Version 3rd Ed ‐ March 2012
Author: Alan Batt DipEMT NQEMT‐P
alan@emsflashcards.com www.emsflashcards.com
Copyright © 2012 Alan Batt. All rights reserved.
The information in this publication is considered to be correct at time of publishing. No responsibility whatsoever is or will be accepted by the author(s) for any misuse of these flashcards, or any errors contained within these flashcards.The author(s) cannot and do not guarantee the accuracy of information contained within this publication. As such the user accepts use of this guide i t th i
is at their own risk. These are designed to be used by trained i k Th
d i dt b
db t i d
personnel only. Medication dosages and details etc. should always be confirmed with an official publication. Always practice within your scope of practice, and follow the current CPGs and Medication Formulary relevant to your qualification and approved for use by your service provider. This edition supersedes all previous editions. If you discover any errors in these cards email info@emsflashcards.com. Donations welcome at www emsflashcards com
at www.emsflashcards.com.
This publication is not affiliated with nor endorsed by the
PHECC, HSE NAS, DFB or any other stautory, auxiliary,
voluntary or private entity involved in the provision of prehospital care in Ireland.
Acknowledgements: S.Deasy, J.Flahavan, D.Grennan, R.White, S.Knox, g
y
R.Mannion, J.Holland, J.Ward, L.O'Callaghan, N.O'Leary
Patient Assessment
EMS Priority Dispatch Protocols
1. Abdo Pain/Problems
2. Allergies/Envenomnations
3. Animal bites/attack
4. Assualt/sexual assault
5. Back pain (non‐trauma)
6. Breathing problems
7.Burns/Scalds
8. CO Inhalation/HazChem
9. Cardiac or Respiratory Arrest/Death
/
10. Chest pain (non‐trauma)
11. Choking
12. Convulsions/fitting
13. Diabetic problems
14. Drowning (near) /diving
15. Electrocution/lightning
16. Eye problem/injury
17. Falls
18 H d h
18. Headache
19. Heart problems/AICD
20. Heat/cold exposure
21. Haemorrhage/laceration
22. Inaccessible incident (non‐
vehicular)
23.Overdose/Poisoning
24. Pregnancy/ Childbirth/ Miscarriage
25 Psychiatric/Abnormal
25. Psychiatric/Abnormal Behaviour / Suicide attempt
26. Sick person (specific dx)
27. Stab/Gunshot/Penetrating trauma
28. Stroke (CVA)
29. Traffic/Transportation Incident
30. Traumatic Injuries (specific)
31.Unconscious/fainting (near)
32. Unknown problem (collapse 3rd party)
33. Transfer/Interfacility/ /
/
Palliative Care
34. ACN (Automatic Crash Notification)
35. Health Care Professional Admission
36. Influenza Pandemic
37. Interfacility Transfer
N t
Note:
Bravo, Charlie, Delta & Echo Calls: respond to scene with lights & siren
Alpha & Omega Calls: respond to scene in normal traffic (no lights/siren)
Primary Survey ‐ Adult
Scene safety survey & situation
Scene safety, survey & situation
Universal Precautions
Control catastrophic haemorrhage
Response ‐ shake & shout
No response ‐ OPA, call for ALS
Airway ‐ maintain patent
C‐Spine manual immobilisation if trauma
Breathing? adequate?
Auscultate/palpate/inspect/percuss
Oxygen therapy
Check circulation & pulse
Colour & temp of skin, Cap refill
Cardiac & SpO2 monitoring
Collar application if trauma
Disability
AVPU, PEARRL?
Expose & Examine
Cli i l St t D i i
Clinical Status Decision
SAMPLE
Signs & Symptoms
Signs
& Symptoms
Allergies
Medications
Pertinent past medical
Last Oral Intake
Events leading to illness/injury
OPQRST‐A
Onset?
Provokes/Relieves?
Quality
li
Radiation? Referral?
Severity?
Time? How long?
Associated symptoms?
Associated
symptoms?
e.g. nausea, dizziness
AVPU
Alert ‐ awake & interacting with environment
awake & interacting with environment
Voice ‐ responds to verbal commands
Pain ‐ only responds to painful stimuli
Unresponsive ‐ no response any stimuli
Baseline Vitals
Pulse (rate,rhythm,strength)
Breathing (rate, rhythm, effort, auscultation, palpate, inspect)
BP (Palp or Auscultation)
ECG (rate & rhythm)
BGL
SpO2%
Pain score (0‐10)
Skin colour, temp, cap ref
Pupils
AVPU/GCS
Temperature
Normal Vital Signs ‐ Adult
Pulse: 60‐100bpm, regular
Resp: 12‐20 rpm, regular
BP: 120/80 mmHg
BGL: 4‐7mmol/l
Pupils: PEARRL
Skin colour: pink
Skin condition: warm
Temperature: 37.0°C
ECG: NSR
Auscultation: bilateral breath sounds, no audible wheeze
dibl h
SpO2%: >95%
AVPU: Alert, oriented x 3
Cap refill: <2 secs
GCS: 15/15
Physical Exam
DCAP ‐ BTLS
Deformities
Contusions
Abrasions
Punctures
Burns
Tenderness
Lacerations
Swelling
lli
CSM
Circulation
Sensation
Motor function
Motor function
Spinal Injury Decision
1 Any dangerous mechanism?
1. Any dangerous mechanism?
Fall ≥1m/5 steps, Axial load to head, MC >100km/h, Rollover or ejection, Bicycle/ ATV collision, Pedestrian v vehicle
IF YES TO ANY ‐ IMMOBILISE
2. Ensure patient is low risk
Simple rear‐end MVC (excludes push into oncoming traffic or hit by bus/truck), No neck/back pain, Absence of midline c‐spine or back tenderness
IF NOT ‐ IMMOBILISE
3. Ensure all factors for rule out present
GCS = 15, communication effective, no dangerous mechanism or distracting injury, no numbness/tingling, no midline pain/tenderness, able to rotate neck 45° left & right & walk pain free
left & right & walk pain free
IF NOT ‐ IMMOBILISE
Estimating Blood Pressure
Average BP: 120/80mmHg
General rule: 100 + age for systolic BP
Radial pulse present = Sys BP at least 80mmHg
Femoral pulse present = Sys BP at least 70mmHg
Carotid pulse present = Sys BP at least 60mmHg
Tachycardia: >100bpm
Tachycardia:
>100bpm
Bradycardia: <60bpm
Airway Management
Blood pressure
Suction
Yankeur cathether:
Keep tip in sight when suctioning
Soft cath:
Measure as per OPA, mark with finger, p
,
g ,
suction as far as this mark
General principles:
Pre‐oxygenate patient
Suction on way out
No more than 10 secs
h
Don't forget to take Universal Precautions!
EasyCap™ ETCO2 Detector
Colour change
from purple to
gold
when CO2 detected
Special clinical considerations for
advanced airway
advanced airway
GCS = 3
SpO2 < 92%
RR ≤ 9
BVM ineffective
(All of the above must be present)
Laryngeal Mask Airway
Size 3 = Small adult
Size 4 = Regular
Size 5 = Large adult
LMA Equipment
BVM
OPA
Stethoscope
Suction
Yankeur
Bacterial Filter
LMA
Oxygen
Cath mount / CO2 detector
KY Gell
Securing device
BOSSY BLOCKS
i‐Gel® Airway
iGel Size Max ET tube size
iGel Size
Max ET tube size
1 3.0mm
1.5 4.0mm
2 5.0mm
2.5 5.0mm
3 6.0mm
4 7.0mm
5 8.0mm
1 Neonate 2‐5kg
1.5 Infant 5‐12kg
f
k
2 Small paediatric 10‐25kg
2.5 Large paediatric 25‐35kg
3 Small adult 30‐60kg
4 Medium adult 50‐90kg
5
5 Large adult 90+kg
Large adult
90+kg
i‐Gel® Airway
Recommended insertion technique
Place patient in sniffing position
Grasp lubricated iGel by bite block
Introduce soft tip towards hard palate
d
f
d h d l
Glide down & back until firm resistance is felt
Ensure teeth at horizontal mark on bite block
Tape down maxilla to maxilla
Confirm placement (breath sounds, ETCO2, chest rise)
© 2010 Intersurgical Ltd
King LT Airway
Lt Size Patient Height Cuff Vol
Lt Size Patient Height Cuff Vol
2 35‐45in 25‐35ml
2.5 41‐51in 30‐40ml
3 4‐5ft 45‐60ml
4 5‐6ft 60‐80ml
5 >6ft 70‐90ml
King LT Airway
Recommended insertion technique
Place patient in sniffing position
Grasp lubricated LT by connector
Introduce tip past base of tongue from right d
b
f
f
h
corner of mouth
As it passes base of tongue, rotate back to midline (blue orientation line facing chin)
Advance until base of connector is in line with teeth/gums
Inflate to recommended volume
Confirm placement (breath sounds, ETCO2, chest rise)
© 2009 King Systems Ltd.
ET Intubation Equipment
10ml syringe
10ml
syringe
Suction
Oxygen
Cath mount / CO2 detector
KY Gel
Stethoscope
Stylet/bougie, securing device
Magills Forceps
ET Tube
Laryngoscope handle with bulb
Laryngoscope blade
BVM
OPA
Yankeur
10 SOCKS SMELL BOY!
10 SOCKS SMELL BOY!
ET Tube Troubleshooting
Displaced: oesophagus, right mainstem, back of throat, etc
Obstructed: secretions, blood, mucus plug, kink, etc
Pneumothorax
Equipment: malfunctions, O2, ETT, BVM, ventilator, monitor
You: your approach, technique: missing something?
DOPEY!
O
© The Walt Disney Company
Resuscitation & ECG
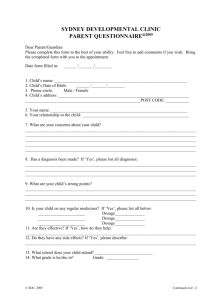
Determining ECG rate
Find a QRS complex that begins on a heavy line on ECG paper. The heavy lines following this become 300, 150, 100, 75, 60, 50, 43. Wherever the next QRS occurs between, this will indicate the rate
Example above rate = 60
Reading an ECG
Paper runs at 25mm/sec
Paper runs at 25mm/sec
One small box = 0.04/sec
One large box = 0.2/sec
Five large boxes = 1 sec
PR Interval = 3‐5 small sq
QRS = 2‐3 small squares
3 Lead ECG
Ride Your Green Bike
12 Lead ECG
V1 ‐ 4th intercostal space, right costal margin
V2 ‐ 4th intercostal space, left
costal margin
V3 ‐ between V2 & V4
V4 ‐ 5th intercostal space, mid‐clavicular
V5 ‐ anterior axiliary line, in line
with V4
V6 ‐ mid axillary line, in line with V4
Blood pressure
12 Lead ECG
12 Lead ECG Lead Views
Reading an ECG
Quality? Any artefact?
Quality? Any artefact?
Is aVR negative? Are all leads present?
1. Rhythm?
Is it regular or irregular?
2. Rate
Is it tachy or brady?
3. Is there a P wave before every QRS?
4. Is there a QRS after every P wave?
5. Is it isoelectric?
6. Is there ST elevation or ST depression in any lead?
Causes of ST elevation
Electrolytes
LBBB
Early repolarization
Ventricular hypertrophy
Aneurysm
Treatment (eg pericardiocentesis)
Injury (AMI, contusion)
Osborne waves (hypothermia)
Non‐occlusive vasospasm
ELEVATION
ECG Rhythms
Normal Sinus
Sinus Tachycardia
Sinus Bradycardia
Asystole
Ventricular Tachycardia
Ventricular Fibrillation
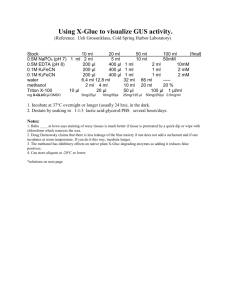
Recognising Left Bundle Branch Block
1 Rhythm must be supraventricular
1. Rhythm must be supraventricular
2. QRS duration ≥120 ms
3. QS or rS complex in V1
4. RsR' wave in V6
The T wave should be deflected opposite
the terminal deflection of the QRS. A
concordant T wave may indicate
ischaemia or AMI.
GNU Free Documentation Licence
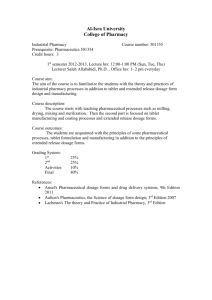
Recognising Atrial Fibrillation
1 Rhythm must be supraventricular
1. Rhythm must be supraventricular
(i.e. QRS complexes must be narrow)
2. Absence of P waves
3. Chaotic baseline in place of P waves
4. Irregular R‐R interval
Wide QRS complexes are generally indicative of ventricular tachycardia, however these may be present in some
cases of AFib with a rapid ventricular
response.
GNU Free Documentation Licence
Drugs causing Torsades de Pointes
Amiodarone
Procainamide
Arsenium
Cisapride
Haloperidol
p
Eritromycin
APACHE
GNU Free Documentation Licence
Cardiac Arrest Algorithm
ADULT
Scene Safety
Standard Precautions
Response ‐ shake & shout
No response ‐ OPA, ALS
Airway ‐ consider advanced ‐ LMA/ETT
Check breathing: Not breathing
Provide 2 x ventilations via BVM
p
Check circulation & pulse
Not present
Witnessed arrest: attach AED pads
Unwitnessed arrest: start CPR
30 compressions: 2 ventilations
Rate of 100 per min
Continue as per CPG
Continue as per CPG
Causes of PEA
6 Hs
Hydrogen ions (acidosis)
Hypokalaemia
Hyperkalaemia
Hypovolaemia
Hypoxia
Hypothermia
6 Ts
Tamponade
Toxicity
i i
Tension pneumothorax
Trauma
Thrombosis ‐ pulmonary
Thrombosis ‐ coronary
Ceasing Resuscitation
Patient is not
‐ Hypothermic
‐ Cold water drowning ‐ Poisoning
‐ Overdose
‐ Pregnant
‐ <18 years
NB: Witnessed arrest with CPR prior to arrival ‐ at least 20 mins resuscitation in asystole
Confirm asystolic cardiac arrest
‐ Unresponsive
‐ No signs of life, pulseless, apnoea
‐ Asystole on monitor
Confirm 2 mins CPR & "No Shock Advised" x 3 completed
If still pulseless, apnoeic, asystole
CEASE RESUSCITATION
Recognition of Death
Inappropriate to commence resuscitation when:
1. Death confirmed by Doctor
or
2. Any of the following present:
‐ Decomposition
‐ Rigor Mortis
‐ Incineration
‐ Decapitation
‐ Pooling
‐ Unwitnessed traumatic cardiac arrest following blunt trauma (5/6.4.13)
‐ Other injuries totally incompatible with life
Document with 2 x 10 second rhythm Mnemonics & Calculators
NATO Phoenetic Alphabet
Alpha
Bravo
Charlie
Delta
Echo
Foxtrot
Golf
Hotel
India
Juliet
Kilo
Lima
Mike
1 – Wun
2 – Too
3 – Thuh-ree
4 – Fower
5 – Fi-yiv
November
Oscar
Papa
Quebec
Romeo
Sierra
Tango
Uniform
Victor
Whiskey
X-Ray
Yankee
Zulu
6 – Six
7 – Se-ven
8 – Ate
9 – Niner
0 – Zero
ASHICE Radio Report to ED
Age of the patient
Age of the patient
Sex of the patient
History ‐ briefly what happened
Injuries/Illnesses
Condition ‐ vitals, drug admin
ETA
Arterial Tourniquet Application
1. Leave uncovered
2. Document time of application
3. Report application and time to ED
4. The letter T and time of application should be written in marker clearly visible h ld b
i
i
k l l i ibl
on the patient’s forehead.
IV Fluid Equipment
Giving set
Giving
set
IV Cannula
Tourniquet
Bag of fluids
IV Dressing
Tape
Steriwipe
GIT BITS
Organophosphate Poisoning
Diarrhoea
Urination
Mi i
Miosis
Bradycardia
Bronchospasm
Emesis
Lacrimation
Salivation
DUMBBELS
Oxygen Cylinder Capacity
D Size Oxygen = 340L
D
Size Oxygen = 340L
@15lpm = 22mins
@10lpm = 34mins
@6lpm = 56min
@2lpm = 2hr 50min
CD Size Oxygen = 460L
@15lpm = 30min
@10lpm = 46min
@6lpm = 1hr 16min
@2lpm = 3hr 48min
F Size Oxygen = 1360L
@15lpm = 1hr 30min
@10lpm = 2hr 15min
@6lpm = 3hr 40min
@2lpm = 11hr 20min
@2lpm = 11hr 20min
FAST Assessment
F - Facial droop?
A - Arm drift/weakness?
S - Speech slurred?
T - Time to activate EMS
If any of the above are present,
patient is
considered to be FAST positive!
Hospital. Pre‐alert ED if symptoms <4 hours. t
4h
Glasgow Coma Scale (Adult)
Eyes
Spontaneous = 4
To voice = 3
To pain = 2
None =1
Verbal
Orientated = 5
d
Confused = 4
Inapp. Words = 3
Incomp/ sounds = 2
None = 1
Motor
Obeys command = 6
Localises pain = 5
Flexion to pain = 4
Abnormal flexion = 3
Extension to pain = 2
None = 1
None = 1
Total GCS = /15
Causes of Seizures
Temperature (fever)
Head Injury
Epilepsy
Stroke
Hypoxia
Eclampsia
Drug/alcohol poisoning
Tricyclic Poisoning
Insulin (hypo/hyperglycaemia)
li (h
/h
l
i )
Meningitis
THE SHED TIM
Causes of Unconsciousness
Fainting
Infantile Convulsions
Shock
Hypoxia
Stroke
Hypothermia, Hypotension, Heart Attack
Anaphylaxis, Asthma, Arrest
Poisoning
Epilpetic Convulsion
il i
li
Diabetes
FISH SHAPED
FISH SHAPED
Causes of confusion
Convulsion [post ictal]
Oxygen [hypoxia, hypercarbia]
Nociception [pain]
Full bladder
Uremia
Sugar [hypo/hyperglycemia]
Infection
Opiates
Natremia [hypo/hyper]
CONFUSION
Cranial Nerves
I Olfactory S
I ‐ Olfactory ‐ S
II ‐ Optic ‐ S
III ‐ Oculomotor ‐ M
IV ‐ Trochlear ‐ M
V ‐ Trigeminal ‐ M/S
VI Abducens M
VI ‐ Abducens ‐ M
VII ‐ Facial ‐ M/S
VIII ‐ Auditory / vestibulocochlear ‐ S
IX ‐ Glossopharyngeal ‐ M/S
X ‐ Vagus ‐ M/S
XI ‐ Accessory ‐ M
XII ‐ Hypoglossal ‐ M
S = Sensory
M = Motor
B= Both
B= Both
Spinal Injury
Dangerous Mechanisms
Fall >1m / 5 steps
Axial load to head
MC >100km/h
Rollover or ejection
Bicycle/ATV collision
Pedestrian v vehicle
Low risk factors
Simple rear‐end MVC
(excludes push into oncoming traffic or hit by bus/truck)
No neck/back pain
Absence of midline c‐spine or
Absence of midline c‐spine or
back tenderness
Spinal Innervation
Markers of multi system trauma
GCS < 13
SBP <90mmHg
Resp rate <10 or >29
Pulse >120
RTS <12
MOI
Markers of acutely unwell patient
Cardiac chest pain
MEWS Score of ≥ 5
f
Acute pain > 5
MEWS Sco
core of 5 or more
e requires immed
diate transport.
Revised Trauma Score
Bones of the skull (frontal)
Bones of the skull (lateral)
Rule of Nines/TBSA % (Adult)
FACE
HANDS
FEET
FLEXION
POINTS
PERINEUM
Don'tt forget FHFFP!
Don
forget FHFFP!
Back of trunk =18%
PEFR ‐ Male
PEFR ‐ Female
Weight Conversion
Weight Conversion PCR Abbreviations
O/A On arrival
O/A ‐ On arrival
O/E ‐ On examination
C/O ‐ complained of
PMH ‐ past medical history
Sx ‐ Social History
Rx Treatment
Rx ‐ Treatment
Δ ‐ Diagnosis
< ‐ less than
> ‐ greater than
\ ‐ therefore
CCF ‐ congestive cardiac failure
LVF ‐ left ventricular failure
RVF ‐ right ventricular failure
BBA ‐ born before arrival
DSH ‐ deliberate self harm
PPH ‐ post partum haemorrhage
PERRL ‐ Pupils equal round
PERRL ‐ Pupils equal, round,
reacting to light
PCR Abbreviations
°C ‐ degrees celsius
°C degrees celsius
x° ‐ x equals number of hours
x/7 ‐ x equals number of days
x/52 ‐ x equals number of weeks
x/12 ‐ x equals number of months
NSR normal sinus rhythm
NSR ‐ normal sinus rhythm
SB ‐ sinus bradycardia
ST ‐ sinus tachycardia
PAC ‐ premature atrial contraction
PVC ‐ premature ventricular contr.
VT ‐ ventricular tachycardia
JR ‐ junctional rhythm
SVT ‐ supraventricular tachycardia
AF ‐ atrial fibrillation
AFL ‐ atrial flutter
FHB ‐ first degree AV block
SHBT1 ‐ second degree AV block T1
SHBT1 ‐ second degree AV block T1
SBHT2 ‐ second degree AV block T2
PCR Abbreviations
THB third degree AV block
THB ‐ third degree AV block
ASY ‐ asystole
IDO ‐ idioventricular
PEA ‐ pulsesless electrical activity
‐ with
? query
? ‐ query
# ‐ fracture
C ‐ cold/cool (in temp obs box)
N ‐ normal (in temp obs box)
H ‐ hot (in temp obs box)
P ‐ palpation (in BP obs box)
R ‐ regular (in pulse obs box)
I ‐ irregular (in pulse obs box)
U ‐ unknown (for any unknown details on PCR)
NOK ‐ next of kin
Principles of Safe Lifting
1. Assess TILE
Task
Load
Individual Capacity
Environment
2. Bend knees
3. Broad stable base
4. Back straight
5. Firm palmer grip
6. Arms in line with trunk
7. Load close to centre of gravity
d l
f
i
8. Pivot feet in direction
HSE Ambulance Control
Dublin
016709111 / 016709444
Mid West
061482215 / 061228177
Midlands
0579358165
North East
0469066749
North West
0719851888
South
0214921125
South East
189049919
West
0949021122
DFB Control
DFB Control
016778221
Basic Anatomical Positioning
Anterior front
Anterior ‐ front
Posterior ‐ back
Lateral ‐ side
Medial ‐ centre
Proximal ‐ near to body, close to point of attachment
Distal ‐ away from body, furthest from point of attachment
Palmer ‐ anterior of hand, palm
Dorsal ‐ back of hand
Retro ‐ behind
Supra ‐ above
otomy ‐ to cut
stomy ‐ surgically created opening
ectomy ‐ removal of
Normal Lab Values
Arterial Blood Gases
pH: 7 35 7 45
pH: 7.35‐7.45
H+: 35‐45 nmol/L
PaO2: 75‐100 mmHg (11.1‐14.4 kPa)
PaCO2: 35‐45 mmHg (4.6‐6.4 kPa)
HCO3‐: 22‐28 mmol/L
Base excess: 0
Base excess: 0
SpO2%: 90‐100%
U&E
Urea: 2.5‐8.5 mmol/L
BUN: 1.2‐3.0 mmol/L
/
Plasma Glucose: 3.8‐6.0 mmol/L
Creatinine: M 25‐90/ F 10‐70 μmol/L
+
Na : 135‐145 mmol/L
+
K : 3.5‐5.0 mmol/L
Cardiac Enzymes
CK: M 20‐200 / F 20‐180 U/L
CK‐MB: 0‐12 U/L
Normal Lab Values
Troponin 12 hours after onset of pain
Troponin, 12 hours after onset of pain
14 ng/mL +: AMI likely
FBC
Hb: M 13.5‐18.0 / F 12.1‐15.1 g/dL
Hct: M 41‐50% / F 36‐44%
RBC: M 4.5‐5.5 / F 4.0‐4.9 (x 10
RBC:
M 4.5‐5.5 / F 4.0‐4.9 (x 1012/L)
WBC: 3.2‐10.6 (x109/L)
Coag Screen
INR: 0.9‐1.2
APTT: 22‐43
Plt: 140 450 (x109/L)
Plt: 140‐450 (x10
LFT
Albumin: 35‐50g/L
ALP: 35‐100 U/L
ALT & AST: 0‐40 U/L
Bilrubin (total): 2‐17μmol/L
GGT: 0‐58 U/L
/
Amylase: 25‐125
Paediatrics
Blood pressure
Neonatal resuscitation
Term?
Clear amniotic fluid?
Breathing/crying?
Good muscle tone?
Y
Warm
Clear airway
Dry
Assess colour
N
Warm
Clear airway
Clear airway
Dry, stimulate, reposition
A
Breathing, HR>100, Pink
RR, HR, Colour
Observe
Apnoea or HR<100
B
Pink
PPV
HR
<60
C
D
Breathing, HR>100 Cyanosed
HR>100, Cyanosed
Cyanosed
Supplemental O2
HR >60
PPV, Chest compressions 3:1
HR 60
HR<60
E i
Epinephrine
hi
Visual Analogue Pain Scale
WETFAG
Weight (kg) = (Age x 3) + 7
Energy (J) =
4J/kg
Tracheal tube diameter (mm) = Tracheal tube diameter (mm) (Age/4) + 4
Fluid bolus = 20ml/kg NaCl
Adrenaline = 0.1ml/kg of 1:10,000
Glucose = l
5ml/kg of 10% Dextrose
Neonate: fluid bolus of 10ml/kg
Estimating Paediatric weight
(Age x 3) + 7 = approx weight in kg
e.g. 10 year old child
(10 x 3) + 7 = weight in kg
(10 x 3) + 7 weight in kg
(30) + 7 = weight in kg
Approx weight in kg = 37kgs
e.g. 7 year old child
((7 x 3) + 7 = weight in kg
)
i h i k
(21) + 7 = weight in kg
Approx weight in kg = 28kg
Rule of Nines/TBSA % (Paediatric)
FACE
HANDS
FEET
FLEXION
POINTS
PERINEUM
Don't forget FHFFP!
Glasgow Coma Scale (Paediatric)
Eyes
Spontaneous = 4
To voice = 3
To pain = 2
None =1
Verbal
Coos or babbles = 5
Irritable, continually cries = 4
Cries to pain = 3
Moans to pain = 2
None = 1
Motor
Moves spontaneously/purposefully = 6
Withdraws from touch = 5
Withdraws from pain = 4
Abnormal flexion to pain for infant = 3
Extension to pain = 2
None = 1
T t l GCS /15
Total GCS = /15
Apgar Score
7‐10
0: Supportive care
e
4‐6: Mo
Moderate depressi
sion
1‐3: Agggressive resuscitaation
Major Emergency
Blood pressure
Triage Sieve
Triage Sort
Triage Sort
METHANE Message
Major Emergency declared
Exact Location of incident
Type of incident
Hazards present
Access/Egress to site
Number of casualties (approx)
b
f
li (
)
Emergency services required
Role of 1st Practitioner
Wear PPE & helmet
Park safely at scene
Leave blue lights on ‐ vehicle acts
as Forward Control Point
Confirm arrival at scene with Amb
Control, provide initial report
Maintain comms with Practitioner 2
Leave keys in ignition, remain with
vehicle at all times
Carry out role of Communications
Officer until relieved.
ffi
il li d
First crew do not provide treatment or transport to patients
transport to patients
Role of 2nd Practitioner
Wear PPE & helmet
Carry out scene survey
Give situation report to Amb Control
using METHANE message
Carry out role of HSE Controller of
Operations until relieved
Liaise with Garda & Local Authority
Controllers of Operations
Select location for holding area
Set up key areas
Site Control Point
i
l i
Casualty Clearing Station
First crew do not provide treatment or transport to patients
transport to patients
Controllers of Operations
Irish National Grid
Example: S 237 128
Sheet: S
East: 237
North: 128
Read across then up
Read across then up
"In the door and up the stairs"
Major Emergency
Major Emergency
Major Emergency
Major Emergency
Helicopter safety
Only approach after the pilot has given a clear signal!
has given a clear signal!
Helicopter safety
If the rotors are turning or are
If the rotors are turning, or are about to turn:
‐ always approach in pilots visual
field
‐ approach a helicopter walking
approach a helicopter walking
uphill or crouching if level
‐ never approach a helicopter
walking downhill (main rotor)
‐ never approach a helicopter
from the rear (tail rotor)
‐ hold on to all lightweight items
as they may be blown away
‐ if an item gets blown away do
not chase it ‐ it's not worth your
life
Medication Formulary
Medication Administration
RIGHT
RIGHT medication at the di ti
t th
RIGHT dose through the
RIGHT route to the
RIGHT patient at the RIGHT time and
WRITE it down
Patient has RIGHT to refuse
Always consider
indications
contraindications
side effects
adverse effects
Always check
expiry date on carton
expiry date on vial/syringe
clarity of medication/fluid
Drug dosage calculation
Dose req (mgs) x Vol of dilutent (mls)
Dose avail (mgs) 1
= dose to be administered in mls
e.g. req 2.5mg from 5mg in 10ml
2.5mg x 10ml
5mg 1
= 5ml to be administered
e.g. req 0.05mg from 1mg in 1ml
0.05mg x 1ml
1mg 1
= 0.05ml to be administered
= 0 05ml to be administered
Drop/min calculation
Vol of infusion x Drop factor
Time of infusion x 60 1
= drops per minute
e.g. admin 2500mls in 24 hours
2500 x 20drops/ml (as per giving set)
24 x 60 1
= 34 drops/min (1 drop/2 sec)
e.g. admin 1000mls in 2 hours
1000 x 20drops/ml (as per giving set)
2 x 60 1
= 166 drops/min (2 drops/1.5 sec)
= 166 drops/min (2 drops/1 5 sec)
Amiodarone
Indications
VF, Pulseless VT
Dosage & Route (Adult)
VF/VT: 5mg/kg IV/IO. Loading dose 300mg, supplemental dose 150mg
Dosage & Route (Paed)
5mg/kg IV/IO
Contra‐Indications
KSAR, iodine hypersensitivity
Side Effects
Inflammation of peripheral veins, b
d
di AV
d i
b
li i
bradycardia, AV conduction abnormalities
Additional Info
If diluted mix with Dextrose 5%. May
be flushed with NaCl.
Aspirin
Indications
Cardiac Chest Pain, Suspected AMI
Dosage & Route (Adult)
300mg PO chew/soluble
Dosage & Route (Paed)
Not indicated
Contra‐Indications
Active symptomatic GI ulcer/bleed, bleeding disorder, KSAR, <16yrs old
Side Effects
Epigastric pain/discomfort, bronchospasm, GI bleed, GI irritation, skin reaction, increased bleeding time
Additional Info & Clinical Directive
Admin even if pt already on anticoagulant or Aspirin. If enteric coated Aspirin taken p
g
(swallowed not chewed), pt should be regarded as not having taken Aspirin. Ref CD 03/2011
Atropine
Indications
Sympt Brady, Organophosphate Poisoning
Dosage & Route (Adult)
Symptom. Brady: 0.5mg IV/IO
Rpt 3‐5mins up to max 2mg
Organophosphate Poisoning:
1mg IV/IO. Rpt 3‐5mins to ensure minimal salivary excretions
Dosage & Route (Paed)
Not indicated
Contra‐Indications
KSAR
Side Effects
Tachycardia,dry mouth,dilated pupils
Additional Info
Accidental expsoure to eyes causes
blurred vision
blurred vision
Benzylpenicillin
Indications
Suspected or confirmed meningococcal sepsis
Dosage (Adult) >8yrs
1200mg IV/IO/IM
Dosage (Paed) <8yrs
1‐8 yrs: 600mg IV/IO or IM
<1 yr: 300mg IV/IO or IM
Contra‐Indications
KSAR
Side Effects
GI disturbances, hypersensitivity reactions
d
b
h
Clopidogrel
Indications
Identification of STEMI
Dosage (Adult)
600mg PO
>75 yrs: 75mg PO
Dosage (Paed)
Not indicated
Contra‐Indications
KSAR, active pathological bleeding, severe liver impairment
Side Effects
Abdominal pain, dyspepsia, diarrhoea
Cyclizine
Indications
Managing, preventing and treating nausea/vomiting
Dosage & Route (Adult)
50mg slow IV/IO
Dosage & Route (Paed)
Not indicated
Contra‐Indications
KSAR
Side Effects
Tachycardia, dry mouth, sedation
Dextrose 10% solution
Indications
Blood Glucose < 4mmol/L
Dosage (Adult)
250ml IV/IO infusion. Repeat x 1 prn
Dosage (Paed)
5ml/kg IV/IO. Repeat x 1 prn
Contra‐Indications
KSAR
Side Effects
Necrosis of tissue around IV access site ‐ patency will reduce this
Additional Info
Use as large a vein as possible
Clinical Directive
Pts with good clinical evidence of hypoglycaemia & BGL 4‐5mmol/L or glucometer fail, should be treated for hypoglycaemia Ref CD 07/2011
for hypoglycaemia. Ref CD 07/2011
Diazepam Injection
Indications
Seizure
Dosage & Route (Adult)
5 mg IV/IO. Rpt prn to max 10mg
Dosage & Route (Paed)
0.1mg IV/IO. Rpt prn to max 0.4mg/kg or 10mg
Contra‐Indications
KSAR, respiratory depression
Side Effects
Hypotension, respiratory depression, drowsiness, light‐headedness
Additional Info
Diazepam IV/IO should be titrated to
effect. Max dose includes admin prior
to Practitioner arrival.
Clinical Directive
Clinical Directive
Midazolam is preferred medication. Ref CD 02/2012
Diazepam PR
Indications
Seizures
Dosage (Adult)
≥8 yrs: 10mg PR
Dosage (Paed)
<3 yrs: 2.5mg PR
3‐7 yrs: 5mg PR.
Contra‐Indications
KSAR, respiratory depression
Side Effects
Hypotension, respiratory depression, drowsiness, light‐headedness
Additional Info
Be aware of modesty, admin in presence
of 2nd person. Max dose includes admin prior to Practitioner arrival.
Clinical Directive
Clinical Directive
Midazolam is preferred medication. Ref CD 02/2012
Enoxaparin Sodium Solution
Indications
STEMI immediately following
admin of a thrombolytic agent
Dosage (Adult)
30mg IV bolus
Dosage (Paed)
Not indicated
Contra‐Indications
Active major bleeding disorders, conditions with high risk of bleeding, recent hemorrhagic stroke or subdural h
j
di
i
i
haematoma; jaundice; active gastric or duodenal ulcer; hiatal ulceration; threatened abortion, retinopathy
Side Effects
Pain, haematoma
Epinephrine 1:10,000
NB: Double check concentration!!
NB: Double check concentration!!
Indications
Adult: Cardiac arrest
Paed: Cardiac arrest, bradycardia
Dosage & Route (Adult)
1mg IV/IO, Rpt 3
5mins.
1mg IV/IO, Rpt 3‐5mins.
Dosage & Route (Paed)
0.01mg/kg IV/IO. Rpt 3‐5mins
Contra‐Indications
KSAR
Side Effects
None in cardiac arrest
Epinephrine 1:1,000
NB: Double check concentration!!
NB: Double check concentration!!
Indications
Severe anaphylaxis
Dosage & Route (Adult)
0.5mg IM x 5 mins prn
E: Auto injector 0.3mg x 5 mins prn
Dosage & Route (Paed)
< 6m: 0.05mg (0.05ml) IM
6m‐5y: 0.125mg (0.13ml) IM
6y‐8y: 0.25mg (0.25ml) IM
E: 6m ‐ <10yrs: Epi‐Pen Jr ‐ 0.15mg
E: >10 yrs: Auto Injector ‐ 0.3mg
Contra‐Indications
None known
Side Effects
Palpitations, tachycardia, hypertension, angina‐like symptoms
angina‐like symptoms
Furosemide
Indications
Pulmonary Oedema
Dosage (Adult)
40mg IV
Dosage (Paed)
Not indicated
Contra‐Indications
Pregnancy, hypokalaemia, KSAR
Side Effects
Headache, dizziness, hypotension, arrhythmias, deafness, diarrhoea, N&V
Additional Info
Protect from light
Glucagon
Indications
Hypoglycaemia, BGL <4mmol/L in pts
unable to take oral glucose or gain IV
Dosage & Route (Adult)
1mg IM
Dosage & Route (Paed)
≤8 yrs: 0.5mg IM
>8yrs: 1mg IM
Contra‐Indications
KSAR, phaechromocytoma
Side Effects
Hypotension, dizziness, headache, N&V
Additional Info
May be ineffective in pts with low stores
of glycogen or if admin <24hrs. Clinical Directive
Pts with good clinical evidence of hypoglycaemia & BGL 4‐5mmol/L or glucometer fail, should be treated for hypoglycaemia. Ref CD 07/2011
Glucose Gel
Indications
BGL < 4mmol/L
Dosage & Route (Adult)
10‐20g buccal
Dosage & Route (Paed)
≤8yrs: 5 10g buccal
≤8yrs: 5‐10g buccal
>8 yrs: 10‐20g buccal
Contra‐Indications
KSAR
Side Effects
Vomiting in <5y if admin too quickly
Additional Info
Will maintain glucose levels once raised but should be used 2° to Dextrose or Glucagon to reverse hypoglycaemia.
Clinical Directive
Pts with good clinical evidence of hypoglycaemia & BGL 4‐5mmol/L or glucometer fail, should be treated for hypoglycaemia. Ref CD 07/2011
Glyceryl Trinitrate
Indications
Angina, Suspected AMI
P & AP only : Pulmonary Oedema
Dosage & Route (Adult)
ACS: 0.4mg SL every 5 mins up to 1.2mg
u o a y Oede a 0 8 g S pt
p
Pulmonary Oedema: 0.8mg SL.Rpt x 1 prn
Dosage & Route (Paed)
Not indicated
Contra‐Indications
SBP <90mmHg, sildenafil or other use <24hr, KSAR
Sid ff
Side Effects
Headache, hypotension, flushing, dizziness
Additional Info
Release first spray into air if new or not
used for more than 1 week.
used for more than 1 week.
Hartmann's Solution
Indications
When NaCl unavailable, except for crush injuries, burns, renal failure & hyperglycaemia.
Dosage (Adult)
See NaCl
Dosage (Paed)
See NaCl
Contra‐Indications
KSAR
Side Effects
May cause oedema
Additional Info
Warm fluids if possible
Hydrocortisone
Indications
Severe/recurrent anaphylaxis, Asthmatic pts following anaphylaxis, Exac. COPD
Dosage (Adult)
200mg IM or slow IV (1 to 10 mins)
Dosage (Paed)
<1 y: 25mg IM or slow IV (1 to 10 mins)
1‐5y: 50mg IM or slow IV (1 to 10 mins)
6‐12y: 100mg IM or slow IV (1 to 10 mins)
>12y: 130mg IM or slow IV (1 to 10 mins)
Contra‐Indications
Nil
Side Effects
CCF, HTN, adbo distension, vertigo, headache, nausea, malaise, hiccups
Additional Info
IM avoid deltoid Infusion mix w 100ml
IM avoid deltoid. Infusion mix w 100ml
NaCl. Dosage not less than 25mg.
Ibuprofen
Indications
Mild to moderate pain Dosage (Adult)
400mg PO
Dosage (Paed)
10mg/kg PO
Contra‐Indications
Other NSAIDs within past 8 hrs, children < 3mths, asthma exacerbated by aspirin & pregnancy
Side Effects
Skin rash, GI intolerance, GI bleeding
Additional Info
Adjust dose downward to max of 10mg/kg if admin <6hrs.
Ipratropium Bromide
Indications
Acute severe asthma not responding to initial two salbutamol dose, Exac COPD
Dosage (Adult)
0.5mg NEB
Dosage (Paed)
0.25mg NEB
Contra‐Indications
KSAR
Side Effects
Dry mouth, blurred vision, tachycardia and headache.
Lidocaine
Indications
When amiodarone is unavailable
Dosage (Adult)
1 ‐ 1.5mg/kg IV/IO. Max 3mg/kg
Dosage (Paed)
Not indicated
Contra‐Indications
Nil
Side Effects
Drowsiness, dizziness, twitching, convulsions, bradycardia, unconsciousness, resp depression
Additional Info
May not be administered if Amiodarone
has been administered
Lorazepam
Indications
Combative with hallucinations or paranoia & risk to self or others.
Dosage (Adult)
2mg PO
Dosage (Paed)
Not indicated
Contra‐Indications
Sensitivity to benzodiazepines, severe hepatic or pulmonary insufficiency, suspected signifcant alcohol/sedative intake, KSAR
Side Effects
Drowsiness, confusion, headache, dizziness, blurred vision, nausea/vomiting. Magnesium Suphate
Indications
Torsades de pointes, persistent bronchospasm (life threatening asthma)
Dosage (Adult)
Torsades de pointes: 2g IV/IO (15mins)
Bronchospasm: 1.5g IV/IO (20mins)
Dosage (Paed)
Not indicated
Contra‐Indications
KSAR
Side Effects
Decreased deep tendon reflexes, resp depression, bradycardia, hypothermia
Additional Information
Dilute in 100ml NaCl for infusion
Midazolam Solution
Indications
Seizures. AP only: psychostimulant overdose, hallucinations or paranoia.
Dosage (Adult)
Seizure: 2.5mg IV or 5mg IM or 10mg buccal or 5mg intranasal. Rpt x 1 prn
OD:2.5 mg IV or 5mg IM. Rpt x 2 prn Hallucinations/paranoia: 5mg IV/IM.
Dosage (Paed)
0.5mg/kg buccal or 0.2mg/kg intranasal or 0.1mg/kg IV/IO. Rpt x 1 prn
Contra‐Indications
Shock, depressed vitals, ALOC (2° alcohol)
Side Effects
Resp dep,headache,hypotension,drowsy
Additional info
Titrate to effect (IV) Dilute to 1mg/1ml for
Titrate to effect (IV). Dilute to 1mg/1ml for adult IV. MAD add 0.1ml dead space.
Morphine
Indications
Severe pain
Dosage (Adult)
2mg IV/IO. Rpt not <2 min intervals. MAX 10mg IV/IO. MAX 16mg musculoskeletal pain. Up to 10mg IM if no chest pain & no IV access
Dosage (Paed)
0.05mg/kg IV/IO. Rpt not <2 min intervals
to MAX 0.1mg/kg IV/IO
0.3mg/kg PO. MAX 10mg
Contra‐Indications
PO < 1yr, KSAR, brain injury, labour pain, acute resp depression, SBP<90mmHg, migraine
Side Effects
Resp depression, drowsiness, N&V, Resp
depression drowsiness N&V
constipation
Naloxone
Indications
Resp rate <10 secondary to known
or suspected narcotic overdose
Dosage (Adult)
0.4mg IV/IO/IM or SC. Rpt x 1 prn
AP: Rpt to max 2mg
Dosage (Paed)
0.01mg/kg IV/IO/IM/SC. Rpt x 1prn
AP: Rpt to max 0.1mg/kg or 2mg
Contra‐Indications
KSAR
Side Effects
Nausea/vomiting, agitation, seizures, aggressive/violent due to withdrawal
Additional Info
Caution in pregnancy. First adult dose IM for IVDUs. Prepare to deal with aggressive for
IVDUs Prepare to deal with aggressive
pts. Nifedipine
Indications
Prolapsed cord
Dosage (Adult)
20mg PO
Dosage (Paed)
Not indicated
Contra‐Indications
Hypotension, KSAR
Side Effects
Hypotension, headache, N&V,
bradycardia
Additional Info
Close monitoring of maternal pulse & BP & continuous foetal monitoring if possible.
Nitrous Oxide 50% & Oxygen 50% Indications
Pain relief
Dosage (Adult)
Self administered
Dosage (Paed)
Self administered
Contra‐Indications
Altered LOC, chest injury, shock, pneumothorax, recent scuba dive, decompression sickness, intestinal obstr, inhalation injury, CO poisoning, KSAR
Side Effects
Disinhibition, lowered LOC, lightheadedness
Additional Information
APs may use discretion with minor chest injuries Has addictive properties
injuries. Has addictive properties.
Ondansetron
Indications
Managing, preventing and treating nausea/vomiting
Dosage (Adult)
4mg slow IV
Dosage (Paed)
0.1mg/kg slow IV to max 4mg
Contra‐Indications
KSAR
Side Effects
Headache, flushing, sensation of warmth, hiccups
Oxygen
Indications
SpO2 < 94% adult & <96% paed; SpO2 <92% (COPD), inadequate/absent ventilation
Dosage (Adult)
Titrate to SpO2 94 98%
Titrate to SpO2 94‐98%
Dosage (Paed)
Titrate to SpO2 96‐98%
Dosage (COPD)
Titrate to SpO2 92% or as per COPD card
Contra‐Indications
Paraquat poisoning
Bleomycin lung injury
Side Effects
Prolonged O2 in COPD may reduce vent. Stimulus
Additional info
Additional info
SpO2 on PCR should specify if on supp O2
Paracetamol
Indications
Minor/moderate pain, pyrexia following seizure (paed)
Dosage (Adult)
1g PO
Dosage (Paed)
20mg/kg PO
AP: <1 yr: 60mg PR
AP: 1‐3yrs: 180mg PR
AP: 4‐8yrs: 360mg PR
AP: Pt pyrexial, hx of febrile convulsions
Contra‐Indications
KSAR
Side Effects
None
Additional Info
Adjust dose downward to max 20mg/kg if Adjust
dose downward to max 20mg/kg if
admin <4 hrs.
Salbutamol
Indications
Bronchospasm, Exac COPD, Resp distress following submersion
Dosage (Adult)
E: 0.1mg metered aerosol spray x 2
P: 5mg NEB; Rpt x 1 x 5min prn
AP: 5mg NEB; Rpt x 3 x every 5min prn
Dosage (Paed)
E: 0.1mg metered aerosol spray x 2
<5y: 2.5mg NEB >5y: 5mg NEB
P: Rpt x 1 x 5min prn
AP: Rpt x 3 x every 5min prn
Contra‐Indications
KSAR
Side Effects
Tachycardia, tachyarrythmias, tremors
Additional Info
Additional Info
Max 6lpm O2 for NEB for COPD pts.
Sodium Bicarbonate
Indications
Wide complex QRS arrhythmias, seizures or cardiac arrest following Tricyclic
(TCA) overdose.
Dosage (Adult)
1 mEq/Kg (1mL/Kg 8.4% solution).
Dosage (Paed)
Not indicated
Contra‐Indications
KSAR
Side Effects
Nil
Addintional Information
Anti‐cholinergic S&S: dry eyes, dilated
pupils, dry mouth, dry flushed skin, urinary retention, ALOC
Sodium Chloride 0.9%
Indications
Fluid for prehospital emergency care
Dosage & Route (Adult) IV or IO
Anaphylaxis: 1000ml. Rpt x 1
Burns: >10% TBSA consider 500ml.
>25% TBSA & 1hr incident to ED: 1000ml
Crush injury: 20ml/kg
Decompression illness: 500ml
Glycaemic emergency: 1000ml
Hypothermia: 250ml @ 40°C
ROSC: 500ml @ 4°C. Maintain SBP >90
Shock: 500ml, aliq of 250ml maintain SBP
90‐100mmHg (no trauma, GCS >8)
120mmHg (head injury, GCS ≤8)
Dosage & Route (Paed) IV or IO
Anaphylaxis, glycaemic, hypothermia (@40°C)
(@40
C), crush, ROSC, shock:20ml/kg. crush ROSC shock:20ml/kg
Neonate or haemorrhagic shock: 10ml/kg
Syntometrine
Indications
Control of post partum haemorrhage
Dosage (Adult)
1ml IM
Dosage (Paed)
Not indicated
Contra‐Indications
Severe kidney, liver or cardiac dysfunction, sepsis, KSAR
Side Effects
N&V, abdo pain, headache, dizziness
Additional Info
Ensure that a second foetus is not in the uterus prior to admin.
Tenectaplase
Indications
Conscious, coherent, understands, consents. Under 75 years old. Symp < 3 hrs. Confirmed STEMI (ST elev in 2 or more contiguous leads ; 2mm in V2 & V3, or 1mm in any other lead) or new onset LBBB. Time to PCI >90 mins of STEMI confirmation. No contraindications.
Dosage (Adult)
<60kg: 30mg (6ml)
≥60 < 70kg: 35mg (7ml)
≥70 < 80kg: 40mg (8ml)
≥80 < 90kg: 45mg (9ml)
≥90: 50mg (10ml)
Special Instructions
<20 mins to ED: do not thrombolyse
>30 mins: thrombolyse transport to PCI
>30 mins: thrombolyse, transport to PCI
20‐30 min: thrombolyse if delay, then PCI
Tenectaplase
Contra Indications
Contra‐Indications
Haemorrhagic CVA or CVA of unknown origin at any time. Ischemic CVA in previous 6mths, CNS damage or neoplasms. Recent trauma/surgery/head injury (<3wks). GI bleeding within the last mth active peptic
bleeding within the last mth, active peptic ulcer, known bleeding disorder. Oral anticoagulant therapy, aortic dissection, TIA in preceding 6mths, pregnancy and within 1wk post partum. Non‐compressible punctures, traumatic resus, refractory hypertension (Sys BP > 180 mmHg). Advanced liver disease, infective endocarditis.
Side Effects
CVA, bleeding at site, ecchymoses
Dosage (Paed)
Dosage (Paed)
Not indicated
IM Injections ‐ deltoid
2 fingers down from acromial process,
form triangle inject into centre
form triangle, inject into centre
IM Injections ‐ vastus lateralis
2 hand widths below greater trochanter
of femur hand widths above patella
of femur, hand widths above patella
inject into centre
IM Injections ‐ dorsogluteal
Imagine line between greater trochanter
of femur and iliac crest inject into
of femur and iliac crest, inject into
upper outer quadrant
Age Per Page Reference
Age: Neonate <4 weeks
dose (mg)
Weight
3.5
mls
kg
Energy
14
Tube
3
Age/4+4
Fluids
10ml/kg
35.0
Adrenaline
0.04
0.4
Glucose 10%
5ml/kg
17.5
Amiodarone
17.5
0.6
<1 yr, 300mg
Benzylpen
NaCl ‐ neonate dose
Diazepam
35.0
0.4
0.1
Diazepam PR
<3 yrs, 2.5mg PR (1.25ml)
Epi 1:1,000
<6mths, 0.05mg (0.05ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
25mg
Ibuprofen
0.5
0.5ml
nil<3 months
Age: Neonate <4 weeks
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
1.75
0.2
Midazolam IN
0.7
0.2
Midazolam IV
0.4
0.1
Morphine PO
contraindicated
Morphine IV
0.18
Naloxone
0.04
0.1
Ondansetron
0.35
0.2
Paracetamol
70
2.9
Para PR
<1 yr, 60mg PR
Salbutamol
Pulse
2.5mg
100‐160
SBP
87
Resp rate
LMA ‐ 1
0.2
30‐60
iGel ‐ 1
bpm
mmHg
resp/min
LT ‐ 0
Max Morphine IV (mls)
0.35
Max Naloxone (mls)
0.9
Age: 6 months
dose (mg)
Weight
6
mls
kg
Energy
24
Tube
3.5
Age/4+4
Fluids
20ml/kg
120
0.06
0.6
Glucose 10%
5ml/kg
30
Amiodarone
30
1.0
Adrenaline
<1 yr, 300mg
Benzylpen
NaCl ‐ haemorrhagic shock
60.0
Diazepam
0.1
0.6
Diazepam PR
<3 yrs, 2.5mg PR (1.25ml)
Epi 1:1,000
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
25mg
0.5ml
60
3.0
Ibuprofen
0.5
Age: 6 months
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
3.0
0.3
Midazolam IN
1.2
0.3
Midazolam IV
0.6
0.1
Morphine PO
contraindicated
Morphine IV
0.3
Naloxone
0.06
0.2
Ondansetron
0.6
0.3
Paracetamol
120
5.0
Para PR
<1 yr, 60mg PR
Salbutamol
Pulse
2.5mg
100‐160
SBP
92
Resp rate
LMA ‐ 1.5
0.3
30‐60
iGel ‐ 1.5
bpm
mmHg
resp/min
LT ‐ 1
Max Morphine IV (mls)
0.6
Max Naloxone (mls)
1.5
Age: 1 year
dose (mg)
Weight
10
Energy
mls
kg
40
Tube
4
Age/4+4
Fluids
20ml/kg
200
0.1
1.0
Glucose 10%
5ml/kg
50
Amiodarone
50
1.7
Adrenaline
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
1.0
100.0
0.2
Diazepam PR
<3 yrs, 2.5mg PR (1.25ml)
Epi 1:1,000
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
50mg
1
100
5.0
Ibuprofen
0.5
Age: 1 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
5.0
0.5
Midazolam IN
2.0
0.5
Midazolam IV
1.0
0.2
Morphine PO
3.0
1.5
Morphine IV
0.5
0.5
Naloxone
0.10
0.3
Ondansetron
1
0.5
Paracetamol
200
8.3
Para PR
1y‐3y, 180mg PR
Salbutamol
Pulse
2.5mg
100‐160
SBP
100
Resp rate
LMA ‐ 2
30‐60
iGel ‐ 1.5
bpm
mmHg
resp/min
LT ‐ 1
Max Morphine IV (mls)
1.0
Max Naloxone (mls)
2.5
Age: 2 year
dose (mg)
Weight
13
Energy
mls
kg
52
Tube
4.5
Age/4+4
Fluids
20ml/kg
260
0.13
1.3
Glucose 10%
5ml/kg
65
Amiodarone
65
2.2
Adrenaline
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
1.3
130.0
0.3
Diazepam PR
<3 yrs, 2.5mg PR (1.25ml)
Epi 1:1,000
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
50mg
1
130
6.5
Ibuprofen
0.5
Age: 2 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
6.5
0.6
Midazolam IN
2.6
0.6
Midazolam IV
1.3
0.3
Morphine PO
3.9
2.0
Morphine IV
0.65
0.7
Naloxone
0.12
0.3
Ondansetron
1.3
0.7
Paracetamol
260
10.8
Para PR
1y‐3y, 180mg PR
Salbutamol
Pulse
2.5mg
100‐160
SBP
104
Resp rate
LMA ‐ 2
30‐60
iGel ‐ 1.5
bpm
mmHg
resp/min
LT ‐ 1
Max Morphine IV (mls)
1.3
Max Naloxone (mls)
3.3
Age: 3 year
dose (mg)
Weight
16
Energy
mls
kg
64
Tube
4.5
Age/4+4
Fluids
20ml/kg
320
0.16
1.6
Glucose 10%
5ml/kg
80
Amiodarone
80
2.7
Adrenaline
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
Epi 1:1,000
1.6
160.0
0.3
3y‐7y, 5mg PR
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
50mg
1
160
8
Ibuprofen
0.5
Age: 3 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
8.0
0.8
Midazolam IN
3.2
0.7
Midazolam IV
1.6
0.3
Morphine PO
4.8
2.4
Morphine IV
0.80
0.8
Naloxone
0.14
0.4
Ondansetron
1.6
0.8
Paracetamol
320
13.3
Para PR
1y‐3y, 180mg PR
Salbutamol
2.5mg
Pulse
90‐150
SBP
108
Resp rate
LMA ‐ 2
24‐40
iGel ‐ 2
bpm
mmHg
resp/min
LT ‐ 2
Max Morphine IV (mls)
1.6
Max Naloxone (mls)
4.0
Age: 4 year
dose (mg)
Weight
19
Energy
mls
kg
76
Tube
5
Age/4+4
Fluids
20ml/kg
380
0.19
1.9
Glucose 10%
5ml/kg
95
Amiodarone
95
3.2
Adrenaline
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
Epi 1:1,000
1.9
190.0
0.4
3y‐7y, 5mg PR
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
50mg
1
190
9.5
Ibuprofen
0.5
Age: 4 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
9.5
1.0
Midazolam IN
3.8
0.9
Midazolam IV
1.9
0.4
Morphine PO
5.7
2.9
Morphine IV
0.95
1.0
Naloxone
0.16
0.4
Ondansetron
1.9
1
Paracetamol
380
15.8
Para PR
4y‐8y, 360mg PR
Salbutamol
2.5mg
Pulse
80‐140
SBP
112
Resp rate
LMA ‐ 2
22‐34
iGel ‐ 2
bpm
mmHg
resp/min
LT ‐ 2
Max Morphine IV (mls)
1.9
Max Naloxone (mls)
4.8
Age: 5 year
dose (mg)
Weight
22
Energy
mls
kg
88
Tube
5
Age/4+4
Fluids
20ml/kg
440
Adrenaline
0.22
2.2
Glucose 10%
5ml/kg
110
Amiodarone
110
3.7
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
Epi 1:1,000
2.2
220.0
0.4
3y‐7y, 5mg PR
6m‐5y, 0.125mg (0.125ml)
Glucagon
0.5mg
Glucose gel
5‐10g
Hydrocortisone
50mg
1
220
11
Ibuprofen
0.5
Age: 5 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
4.4
1.0
Midazolam IV
2.2
0.4
Morphine PO
6.6
3.3
Morphine IV
1.10
1.1
Naloxone
0.18
0.5
Ondansetron
2.2
1.1
Paracetamol
440
18.3
Para PR
4y‐8y, 360mg PR
Salbutamol
Pulse
5mg
80‐140
SBP
116
Resp rate
LMA ‐ 2
22‐34
iGel ‐ 2
bpm
mmHg
resp/min
LT ‐ 2
Max Morphine IV (mls)
2.2
Max Naloxone (mls)
5.0
Age: 6 year
dose (mg)
Weight
25
Energy
mls
kg
100
Tube
5.5
Age/4+4
Fluids
20ml/kg
500
Adrenaline
0.25
2.5
Glucose 10%
5ml/kg
125
Amiodarone
125
4.2
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
2.5
250.0
0.5
3y‐7y, 5mg PR
Epi 1:1,000
6y‐8y, 0.25mg (0.25ml)
Glucagon
0.5mg
Glucose gel
5‐10g
0.5
Hydrocortisone
100
2
Ibuprofen
250
12.5
Age: 6 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5.0
1.1
Midazolam IV
2.5
0.5
Morphine PO
7.5
3.8
Morphine IV
1.25
1.3
Naloxone
0.20
0.5
Ondansetron
2.5
1.3
Paracetamol
500
20.8
Para PR
4y‐8y, 360mg PR
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 2.5
iGel ‐ 2
LT ‐ 2
Max Morphine IV (mls)
2.5
Max Naloxone (mls)
5.0
Age: 7 year
dose (mg)
Weight
28
Energy
mls
kg
112
Tube
5.5
Age/4+4
Fluids
20ml/kg
560
Adrenaline
0.28
2.8
Glucose 10%
5ml/kg
140
Amiodarone
140
4.7
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
2.8
280.0
0.6
3y‐7y, 5mg PR
Epi 1:1,000
6y‐8y, 0.25mg (0.25ml)
Glucagon
0.5mg
Glucose gel
5‐10g
0.5
Hydrocortisone
100
2
Ibuprofen
280
14
Age: 7 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
8.4
4.2
Morphine IV
1.40
1.4
Naloxone
0.22
0.6
Ondansetron
2.8
1.4
560
23.3
Paracetamol
Para PR
4y‐8y, 360mg PR
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 2.5
iGel ‐ 2
LT ‐ 2
Max Morphine IV (mls)
2.8
Max Naloxone (mls)
5.0
Age: 8 year
dose (mg)
Weight
31
Energy
kg
150
Tube
6
Fluids
20ml/kg
Adrenaline
mls
620
0.31
3.1
Glucose 10%
5ml/kg
155
Amiodarone
155
5.2
Benzylpen
1y‐8y, 600mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
3.1
310.0
0.6
>7y, 10mg PR
Epi 1:1,000
6y‐8y, 0.25mg (0.25ml)
Glucagon
0.5mg
Glucose gel
5‐10g
0.5
Hydrocortisone
100
2
Ibuprofen
310
15.5
Age: 8 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
9.3
4.7
Morphine IV
1.55
1.6
Naloxone
0.24
0.6
Ondansetron
3.1
1.6
Paracetamol
620
25.8
Para PR
4y‐8y, 360mg PR
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 2.5
iGel ‐ 2
LT ‐ 2
Max Morphine IV (mls)
3.1
Max Naloxone (mls)
5.0
Age: 9 year
dose (mg)
Weight
34
kg
Energy
150
Tube
6
Fluids
20ml/kg
Adrenaline
mls
680
0.34
3.4
Glucose 10%
5ml/kg
170
Amiodarone
170
5.7
Benzylpen
>8y, 1200mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
3.4
340.0
0.7
>7y, 10mg PR
Epi 1:1,000
>8y, 0.5mg (0.5ml)
Glucagon
1mg
Glucose gel
1
10‐20g
Hydrocortisone
100
2
Ibuprofen
340
17
Age: 9 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
10.0
5.0
Morphine IV
1.70
1.7
Naloxone
0.26
0.7
Ondansetron
3.4
1.7
680
28.3
Paracetamol
Para PR
nil >8yrs
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 2.5
iGel ‐ 2.5
LT ‐ 2.5
Max Morphine IV (mls)
3.4
Max Naloxone (mls)
5.0
Age: 10 year
dose (mg)
Weight
37
kg
Energy
150
Tube
6.5
Fluids
20ml/kg
Adrenaline
mls
740
0.37
3.7
Glucose 10%
5ml/kg
185
Amiodarone
185
6.2
Benzylpen
>8y, 1200mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
3.7
370.0
0.7
>7y, 10mg PR
Epi 1:1,000
>8y, 0.5mg (0.5ml)
Glucagon
1mg
Glucose gel
1
10‐20g
Hydrocortisone
100
2
Ibuprofen
370
18.5
Age: 10 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
10.0
5.0
Morphine IV
1.85
1.9
Naloxone
0.28
0.7
Ondansetron
3.7
1.9
740
30.8
Paracetamol
Para PR
nil >8yrs
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 2.5
iGel ‐ 2.5
LT ‐ 2.5
Max Morphine IV (mls)
3.7
Max Naloxone (mls)
5.0
Age: 11 year
dose (mg)
Weight
40
kg
Energy
150
Tube
6.5
Fluids
20ml/kg
Adrenaline
mls
800
0.4
4
Glucose 10%
5ml/kg
200
Amiodarone
200
6.7
Benzylpen
>8y, 1200mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
4.0
400.0
0.8
>7y, 10mg PR
Epi 1:1,000
>8y, 0.5mg (0.5ml)
Glucagon
1mg
Glucose gel
1
10‐20g
Hydrocortisone
100
2
Ibuprofen
400
20
Age: 11 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
10.0
5.0
Morphine IV
2.00
2.0
Naloxone
0.30
0.8
Ondansetron
4.0
2.0
800
33.3
Paracetamol
Para PR
nil >8yrs
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 3
iGel ‐ 3
LT ‐ 2.5
Max Morphine IV (mls)
4.0
Max Naloxone (mls)
5.0
Age: 12 year
dose (mg)
Weight
43
kg
Energy
150
Tube
7
Fluids
20ml/kg
Adrenaline
mls
860
0.43
4.3
Glucose 10%
5ml/kg
215
Amiodarone
215
7.2
Benzylpen
>8y, 1200mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
4.3
430.0
0.9
>7y, 10mg PR
Epi 1:1,000
>8y, 0.5mg (0.5ml)
Glucagon
1mg
Glucose gel
1
10‐20g
Hydrocortisone
100
2
Ibuprofen
400
20
Age: 12 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
10.0
5.0
Morphine IV
2.00
2.0
Naloxone
0.32
0.8
Ondansetron
4.0
2.0
860
35.8
Paracetamol
Para PR
nil >8yrs
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 3
iGel ‐ 3
LT ‐ 2.5
Max Morphine IV (mls)
4.3
Max Naloxone (mls)
5.0
Age: 13 year
dose (mg)
Weight
46
kg
Energy
150
Tube
7
Fluids
20ml/kg
Adrenaline
mls
920
0.46
4.6
Glucose 10%
5ml/kg
230
Amiodarone
230
7.7
Benzylpen
>8y, 1200mg
NaCl ‐ haemorrhagic shock
Diazepam
Diazepam PR
4.6
460.0
0.9
>7y, 10mg PR
Epi 1:1,000
>8y, 0.5mg (0.5ml)
Glucagon
1mg
Glucose gel
1
10‐20g
Hydrocortisone
130
2.6
Ibuprofen
400
20
Age: 13 year
Ipratropium
dose (mg)
mls
0.25mg
1ml
Midazolam BU
10
1.0
Midazolam IN
5
1.1
Midazolam IV
2.5
0.5
Morphine PO
10.0
5.0
Morphine IV
2.00
2.0
Naloxone
0.34
0.9
Ondansetron
4.0
2.0
920
38.3
Paracetamol
Para PR
nil >8yrs
Salbutamol
5mg
Pulse
70‐120
bpm
SBP
75‐120
mmHg
Resp rate
18‐30
resp/min
LMA ‐ 3
iGel ‐ 3
LT ‐ 2.5
Max Morphine IV (mls)
4.6
Max Naloxone (mls)
5.0