Medication Dosage - Para Meadows School
advertisement

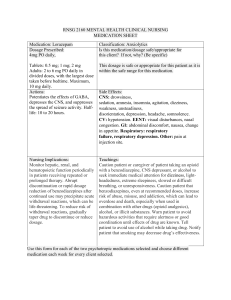
MEDICATION, DOSAGE & TIME GIVEN: **HOME: *SCHOOL: __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Signed: ………………………………………………..Dated …/…/… **This information is required should your child require emergency admission to hospital during school hours. MEDICATION, DOSAGE & TIME GIVEN: **HOME: *SCHOOL: __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Signed: ………………………………………………..Dated …/…/… **This information is required should your child require emergency admission to hospital during school hours. MEDICATION, DOSAGE & TIME GIVEN: **HOME: *SCHOOL: __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ __________________________________________________________________________________________ Signed: ………………………………………………..Dated …/…/… **This information is required should your child require emergency admission to hospital during school hours.