Cranial Nerve Examination - OSCE-Aid
advertisement

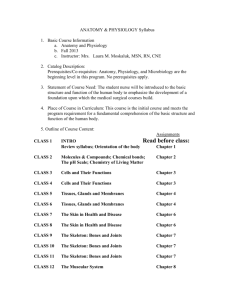
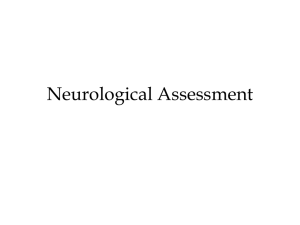
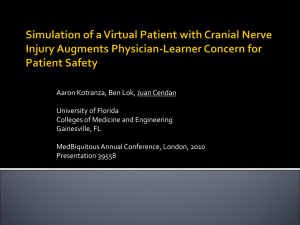
OSCE-Aid Revision Workshops: Cranial Nerves Cranial Nerve Examination Overview: This is a role-play exercise based on a typical short OSCE examination station. In this scenario, the student will be given ten minutes to examine a patient’s cranial nerves. In any OSCE, a student may be asked to examine all or part of the cranial nerves I – XII in this time. Format of the exercise: Ask one student to be the actor and one to be the OSCE finalist. Provide the actor with their brief and the student with the scenario instructions (both overleaf). Ask the student to read the instructions to the group. Check for questions. The student should proceed to manage the actor – allow 8 minutes for examination and 2 minutes to summarise/ask questions below The examiner should only volunteer answers to specific questions as detailed below and should provide examination and investigation findings when specifically asked by the student. Afterwards, gather feedback. Start with the student then open it up to the group. Then provide your own feedback to the student. Finally, discuss key learning points. Suggestions for questions to ask the group, a recommended ‘model answer’ and key discussion points are included overleaf. © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves Student instructions To be read out loud by the student to the group Please examine this patient’s cranial nerves. Do not take a history. Offer to do all aspects of the examination; the examiner will tell you to move on if not needed and answer your questions with findings. You have 9 minutes to examine the patient and 1 minute to discuss with the examiner at the end. © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves Actor’s brief On examination: there are no abnormalities. Only volunteer specific information about symptoms and your past medical history when asked the relevant and specific questions by the student. If any questions cannot be answered with the above information, please answer “no” or “don’t know”. © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves Model examination/instructions for examiner ◦ ◦ ◦ ◦ ◦ Wash your hands Introduce yourself Tell the patient that you would like to examine the nerves in their head and neck Ask if they are happy to do this Reposition the patient sitting down I – Olfactory – offer to do this, move student on II – Optic ◦ Visual acuity – offer to do this, move student on ◦ Colour recognition – offer to do this, move student on ◦ Fundoscopy – offer to do this, move student on ◦ Pupillary reflexes – A) LIGHT - check for pupil symmetry - check for ipsilateral (same side) and contralateral (opposite side) pupil constriction - Test for relative afferent pupillary defect (RAPD) B) ACCOMODATION - ask the patient to focus on a distant spot, then change focus to your finger (15cm in front of their face). Their pupil should constrict to focus. ◦ Convergence - "look at a distant object, now look at my finger" ◦ Visual fields: A) Visual neglect: ask the patient to keep both eyes open. Hold your hands at the periphery of their vision and wave each hand in turn each time asking the patient to state which hand is waving. Then wave both hands. B) Cover one of your own eyes and ask the patient to cover the mirror eye and fix their gaze on your nose, keeping their head still. Hold one of your fingers in the upper outer quadrant of their visual field and move it towards the centre asking the patient to identify the point at which they first see the finger/pin. Repeat this for the other 3 quadrants and then repeat with the other eye. C) Offer to assess blind spot – move on III – Oculomotor/ IV – Trochlear/ VI - Abducens Test all three nerves together: move finger in a large 'H' shape across the patient's field of vision and ask patient to follow finger whilst keeping their head still. Ask if patient can see double or if vision is blurred at any point during the test Test for nystagmus: ask the patient to focus on the tip of your finger. Hold your finger at the left lateral edge of their visual field, and move it rapidly to the right lateral edge of their visual field and hold it there. 2-3 beats is acceptable; more than this indicates pathology. Carry out the reverse (right to left) movement. V – Trigeminal ◦ Sensation: - Test sensation on the sternum with cotton wool first - Press (don't rub) the cotton wool in the distribution of the ophthalmic (forehead), maxillary (cheek) and mandibular (jaw) divisions - Test like for like bilaterally and ask them if it feels the same on both sides © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves ◦ Motor: - Corneal reflex - offer to do this, move student on - Jaw jerk reflex - offer to do this, move student on - Ask patient to clench their jaw - feel temporalis and masseter muscles for contraction - Open jaw to resistance (try to push their jaw up). VII – Facial - Inspect: comment on facial symmetry/appearance - Assess taste - move student on - Raise their eyebrows - Close their eyes tightly - Hold their lips together and blow out their cheeks VIII – Vestibulocochlear - Rub fingers together by one ear, and whisper a two-digit number (e.g. 72) by the other - Offer to carry out specific tests Weber's Test and Rinne's Test - move student on IX – Glossopharyngeal/ X - Vagus - Ask the patient to open their mouth and say 'ahh' - look at uvula Examine the gag reflex (with an orange stick) – offer to do this, move student on Assess the patient's swallow - offer to do this, move student on XI – Accessory - Ask the patient to shrug their shoulders + resist your attempts to push their shoulders down - Put your flat palm on one side of the patient's face and ask them to turn their head against your hand. Feel for sternocleidomastoid strength XII – Hypoglossal - Inspect the tongue for fasciculations at rest Ask the patient to stick out their tongue straight and check for deviation Ask the patient to move their tongue from side to side Questions to ask student 1. Please summarise your findings - normal findings 2. How would you complete your examination? – assess speech, swallow, take a full history, full neurological examination, fundoscopy 3. What investigations/tests you would you like to order – consider CT head or MRI brain, bloods © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves Key learning points for students on cranial nerve palsies: Group discussion around common cranial nerve pathologies (this should be useful for osces but also for writtens) – images on pages below Questions for group: CRN 3 PALSY – show students PICTURE A 1. What abnormality on the left of the page? 2. Where is the site of the lesion? Partial or total? Consider using clip board for this 3. Causes for 3rd nerve palsy? 4. This is a partial nerve palsy - would you expect this finding in all causes of 3rd nerve palsy? 5. What questions would you want to ask patient? Tell student that patient is a type 1 diabetic – what other neurological findings would you expect? VISUAL FIELD DEFECTS – show students PICTURE C 1. Where are the sites of lesions? 2. Revision of optic pathway 3. Causes of lesions along pathway (see below) – encourage students to write in causes as go through handout and sites of lesions BELL’S PALSY – show students PICTURE B 1. What is this? 2. How do you distinguish between this and an UMN lesion? BULBAR PALSY 1. What is this? 2. How do you distinguish between this and an UMN (pseudobulbar) lesion? © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves Answers for group/general points: Questions to consider in cranial nerves examination: 1. Single cranial nerve or groups of cranial nerves? 2. Where is the site of the lesion? In brainstem or outside brainstem? Common pathologies: Please review with above questions 1. Crn 3 palsy: Findings: 1. Partial or full ptosis 2. Eye down and out 3. Pupils may be equal and reactive to light or fixed and dilated one affected side 4. Convergence will be impaired Causes: 1. ‘Medical’ causes: diabetes, atherosclerosis, inflammation, infection, demyelinating disease egg multiple sclerosis usually partial 3rd nerve palsy 2. ‘Surgical’ causes: aneurysms egg posterior communicating artery, SOLs/tumours, trauma, cavernous sinus thrombosis usually total 3rd nerve palsy Other neurological findings if patient was a type 1 diabetic: 1. Diabetic feet e.g.: peripheral neuropathy, charcot joint, ulcers 2. Diabetic gastroparesis/other autonomic neuropathy 3. Fundoscopy – proliferative or non-proliferative diabetic retinopathy Causes of ptosis: Bilateral: myasthenia gravis, myotonic dystrophy Unilateral: 3rd nerve palsy, horner’s syndrome 2. Visual field defects: a. Bitemporal hemianopia – loss of temporal fields bilaterally, all other fields intact. Causes: compression at optic chiasm e.g.: pituitary adenoma, craniopharyngioma, internal carotid artery aneurysm b. Monocular blindness – lesion at eye or optic nerve. Causes: eye pathology, MS, GCA c. Homonymous hemianopia or quadrantanopia – loss of L or R-sided fields or quadrants contralateral to lesion in each eye. Lesion beyond optic chiasm, at level of tracts, radiation, or occipital cortex. Causes: stroke, SOL, abscess, inflammatory process e.g.: abscess 3. Facial nerve palsy: a. LMN: unilateral flaccid facial weakness, unable to raise eyebrows. Causes: Bell’s palsy, skull fracture, CPA tumours, Lyme disease, Ramsay Hunt syndrome, sarcoidosis, diabetes b. UMN: spares forehead, able to raise eyebrows. Causes: stroke, tumour 4. Lower cranial nerve findings: a. Bulbar palsy: diseases of nuclei of cranial nerves IX-XII in medulla - LMN. i. Signs: flaccid, fasciculating tongue, jaw jerk absent, speech is quiet/hoarse/nasal. ii. Causes: MND, GBS, polio, myasthenia gravis, syringobulbia, brainstem tumours, central pontine myelinolysis b. Pseudobulbar palsy: UMN lesion due to lesions of corticobulbar tracts © 2015 www.osce-aid.co.uk OSCE-Aid Revision Workshops: Cranial Nerves i. Signs: slow tongue movements, slow speech, hyperreflexic jaw jerk, emotional lability ii. Causes: MS, MND, stroke, central pontine myelinolysis 5. Groupings of cranial nerves: a. V, VI, VIII, IX, X: CPA lesions/tumours egg acoustic neuroma b. V, VI: lesion at apex of petrous temporal bone egg complication of otitis media c. III, IV, VI: stroke, tumours, Wernicke’s encephalopathy, aneurysms, MS d. III, IV, Va, VI: cavernous sinus thrombosis, superior orbital fissure lesions e. IX, X, XI: jugular foramen lesion Please note: these resources are copyright of the authors and OSCE-Aid unless otherwise stated. Please refer to our website terms & conditions at: http://www.osceaid.co.uk/terms&conditions.php . All resources can be printed and shared for personal use only. No amendment or alteration to these resources is allowed, unless otherwise agreed by the OSCE-Aid team. For any queries, please contact the team at: contact@osce-aid.co.uk © 2015 www.osce-aid.co.uk