“Permissive Hypoventilation” in a Swine Model of Hemorrhagic Shock

“Permissive Hypoventilation” in a
Swine Model of Hemorrhagic Shock
Sharven Taghavi MD, MPH, Lucas Ferrer MD, Senthil Jayarajan
MD, Halley Vora BS, Conor McKee BS, Rich Milner BS, John
Gaughan PhD, Jay Dujon MD, Lars Sjoholm MD, Abhijit Pathak
MD, Joseph Rappold MD, Thomas Santora MD, Steven Houser
PhD, Amy Goldberg MD
Temple University Hospital
Department of Surgery
October 24, 2013
No Disclosures
Background
Most penetrating trauma patients in severe hemorrhagic shock receive positive pressure ventilation (PPV) upon transport to definitive care
Intubation and manual ventilation
Bag-valve mask (BVM) ventilation
Intubation clearly shown to have detrimental effects for penetrating trauma patients in urban locations
Background
Whether BVM ventilation improves outcomes in severe shock-state has not been studied
Previous study showing detrimental effects of BVM 1
New ACLS guidelines prioritizing uninterrupted chest compressions over advanced airway
Backed by animal and clinical studies
Consideration should be given to immediate transportation without airway intervention
1 - Taghavi et al. Examining Prehospital Intubation for Penetrating Trauma in a Swine Hemorrhagic Shock Model.
Journal of Trauma. 2012. 74 (5): 1246-51.
Goals
Test the idea of “permissive hypoventilation” – where manual breaths are not given and 100% oxygen is administered passively via facemask
Hypothesis
In severe low-flow states, PPV would have harmful physiological effects and that “permissive hypoventilation” would result in better outcomes
Methods
Yorkshire swine weighing 30.0 kg
Started on a propofol drip
Three groups of animals
1)
2)
3)
Intubation and manual ventilation (n=6)
BVM ventilation with ambu-bag (n=7)
Permissive hypoventilation with face mask (n=6)
Methods
Placement of Swan-Ganz catheter through central venous introducer
Femoral arterial line placed
14-gauge catheter with stopcock in carotid artery for exsanguination
Baseline arterial blood gas (ABG), laboratory values, and hemodynamic parameters
Outcomes
Stopcock opened and animal was exsanguinated
Hemodynamic and laboratory values measured at 10 minute intervals
Primary outcome was time until death
Secondary Outcomes
Hemodynamic Parameters – cardiac index, CVP
Metabolic values – pH, lactic acid, O
2
End-organ damage – creatinine
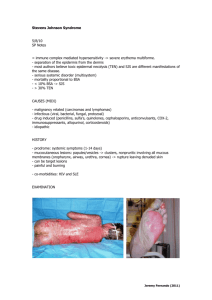
Survival
150
100
50
0
0 20 40
Minutes
60 80
Intubated
Bag-Valve Mask
Facemask
Mean Survival:
Intubated: 51.1 mins
Bag-Valve Mask: 48.5 mins
Facemask: 50.0 mins p = 0.84
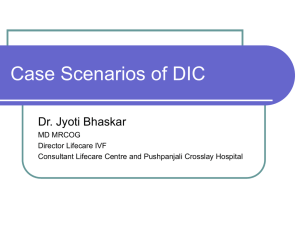
Thermoregulation and
Hemodynamics
Body Temperature
38.5
38.0
37.5
37.0
36.5
36.0
35.5
35.0
34.5
34.0
33.5
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated and BVM group at all time points
50
Intubated
Bag-valve
Facemask
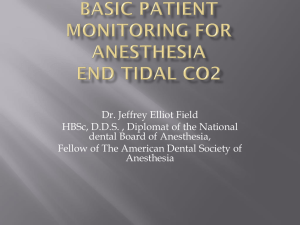
Systolic Blood Pressure
160
140
120
100
80
60
40
20
0
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated group at all time points
50
Intubated
Bag-valve
Facemask
Central Venous Pressure
12
10
8
6
4
2
0
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated group at 10 minutes
50
Intubated
Bag-valve
Facemask
Cardiac Output
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated and BVM group at all time points
50
Intubated
Bag-valve
Facemask
Acid-Base Status and
Gas Exchange
pH
7.80
7.60
7.40
7.20
7.00
6.80
6.60
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated and BVM group at all time points
50
Intubated
Bag-valve
Facemask
Carbon Dioxide
160
140
120
100
80
60
40
20
0
0 10 20 30
Time (minutes)
40
✖ p<0.001 when compared to intubated and BVM at all time points
50
Intubated
Bag-valve
Facemask
PaO
2
Level
600
500
400
300
200
100
0
0 10 20 30
Time (minutes)
40 50
Intubated
Bag-valve
Facemask
Bicarbonate Levels
40
35
30
25
20
15
10
5
0
0 10 20 30
Time (minutes)
40 50
✖ p<0.001 when compared to intubated and BVM group at all time points
Intubated
Bag-valve
Facemask
Metabolic Changes and End-Organ
Damage
Base Deficit
-8
-10
-12
-14
-2
-4
-6
6
4
2
0
0 10 20 30
Time (minutes)
40 50
Intubated
Bag-valve
Facemask
Lactic Acid
14
12
10
8
6
4
2
0
0 10 20
Time (minutes)
30
✖ p<0.001 when compared to intubated at all time points
★ p<0.05 when compared to BVM at 30 and 50 minutes
40 50
Intubated
Bag-valve
Facemask
Creatinine Levels
2.0
1.8
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0
0 10 20
Time (minutes)
30
✖ p<0.05 when compared to BVM at all time points
★ p<0.05 when compared to intubated at 40 minutes
40 50
Intubated
Bag-valve
Facemask
Creatinine Levels by Weight
0.07
0.06
0.05
0.04
0.03
0.02
0.01
0
0 10 20 30
Time (minutes)
40
✖ p<0.05 when compared to intubated and BVM at all time points
50
Intubated
Bag-valve
Facemask
Conclusions
Positive pressure ventilation, whether by endotracheal tube or BVM, does not result in a survival advantage
Worse thermoregulation
Hemodynamic compromise
Worse perfusion vital organs
Higher lactic acid levels
Worse increase in creatinine
Conclusions
“Permissive Hypoventilation” leads to decreased
CO
2 elimination
More profound respiratory acidosis
Evidence of protective effects of hypercapnia
Profound alkalosis with positive pressure ventilation
Conclusions
Consideration should be given to immediate transportation without airway intervention
Similar to change with ACLS guidelines, prospective, randomized trials are needed to determine best mode of ventilation for penetrating trauma patients in urban locations
Limitations
Small sample size
Use of propofol – hemodynamic depression
Ideal for large animal studies
Examined only physiological changes
Inflammatory markers