baptist health school of nursing
advertisement

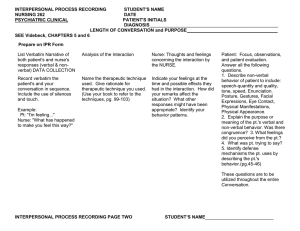
I1 BAPTIST HEALTH SCHOOL OF NURSING NSG 3036A: PSYCHIATRIC-MENTAL HEALTH THERAPEUTIC COMMUNICATION: THE PROFESSIONAL ROLE IN RELATIONSHIP DEVELOPMENT 2007 LECTURE OBJECTIVES: 1. Discuss the variables that affect the transmission of communication. 2. Identify types of preexisting conditions that influence the outcome of the communication process. 3. Define territoriality, density, and distance as components of the environment. 4. Evaluate the components of nonverbal expression. 5. Describe and implement therapeutic and non-therapeutic verbal communication techniques. 6. Describe the facilitating behaviors of active listening. 7. Discuss the elements that convey therapeutic feedback. VOCABULARY: territoriality density intimate distance social distance public distance paralanguage LECTURE OUTLINE: I. Introduction: II. Communication A. Interpersonal Communication - transaction between the sender and receiver. 1. Channels of Communication a. b. c. d. e. Sensor (fun) Comforter (nurturer) Requestive Directive Interruptive (emergency) I2 B. Communication Model 1. 2. 3. 4. Sender (encoder) Receiver (decoder) Message - unit of information Environment - private, social, public. a. b. 5. 6. 7. 8. 9. 10. 11. 12. III. Internal - feeling tired, cold, or discomfort External - temperature, noise level, smells, color and lighting Feedback - clarification of both verbal and nonverbal communication. Skill - ability to observe, listen, clarify and validate meaning. Noise - can impair accuracy Encoding - designing the message Decoding - interpretation of the message Media - style/channel of communication Setting - private, social, public Verbal and nonverbal Impact of Preexisting Condition A. Transactional Model of Communication 1. 2. 3. 4. 5. 6. 7. 8. 9. Personal values - dress, Attitudes - prejudices, negative stereotyping, negativity, anger Knowledge - vocabulary, interests, topic matter Culture - mores, norms, ideas and customs ( % hugging - Italian), words Religion - crosses, Star of David, signing,, praying, Gender - gestures, posture, messages, vocabulary Age- developmental level, generation, in-words (adolescents) Social status - hi status display of power, power dressing, eye contact, posture, height, hand gestures Environment a. b. c. Territoriality - innate tendency to own space (safety/secure) Density - number of people within the space. Distance - space communicates 1. 2. 3. 4. IV. Intimate Distance - closest distance a person will allow. (0" - 18") Personal distance - for close interaction. (In USA 18" - 40") Social distance - conversation between strangers/acquaintances. (4' -12') Public distance - speaking in public or yelling a distance. (In USA >12') Nonverbal Communication A. Physical Appearance and Dress - B. Body movement and posture - I3 C. Touch 1. 2. 3. 4. 5. V. D. Facial expressions E. Eye behavior - “windows of the soul”; W here, W hen, How, How long eye contact is made. F. Vocal cues or paralanguage - pitch, tone, and loudness; rate, how verbalized. Therapeutic Communication Techniques A. B. C. D. E. F. G. H. I. J. K. L. M. N. O. P. Q. R. S. T. VI. Functional-professional - impersonal, business-like. Social-polite - impersonal, but affirming. Friendship-warmth - strong liking of another. Love-intimacy -emotional attachment/attraction. Sexual arousal - expression of physical attraction. Silence - allows client to take control and allows the nurse to collect their thoughts. Accepting - acceptance at the client’s level. W hatever their strengths, weakness, needs or problems they may possess. Giving recognition - acknowledgment Offering self - making ones self available Broad openings - allows client to select topic. General leads - encouraging continuation Placement of event in time - clarifies the relationship of events in time. Making observations - verbalize observations and perceptions. Description of Perceptions - asking the client to verbalize their perception. Comparison - asking for comparing of similarities and differences in ideas, experiences, or interpersonal relationships. Restating - acknowledges that expressed statement has been understood. Reflecting - questions or feelings are directed back to the client for recognition and acceptance. Focusing - narrowing the topic to a single idea or a word. Exploring - further delving into a subject, idea, experience or relationship. Clarification and validation - searching for mutual understanding by clearing vague ideas. Reality orientation - clarify misconceptions that have been expressed. Voicing doubt - express uncertainty to the reality of a perception. Verbalizing the implied - putting words to what the client has implied. Translating words into feelings - indirectly putting into words the feelings that have been expressed. Formulating a plan of action - striving to prevent anger/anxiety from escalating to an unmanageable level the next time the stressor occurs. Nontherapeutic Communication Techniques A. B. C. D. E. F. G. Reassurance - discourages client from further expression of feelings. Rejection - refusing to consider the client’s ideas or behavior. Approval or disapproval - implies the nurse has the right to pass judgement or opinions of right and wrong. Agreeing/disagreeing - implies the nurse has the right to pass judgement. Giving advice - implies the nurse knows best and the client is incapable of self-direction. Probing - pushing for answers to issues that client does not wish to discuss. Client feels used and devalued. Defending - implies that client has no right to express ideas, opinions, or feelings. H. I. J. K. L. M. N. VII. I4 Requesting an explanation - asking “why?” Puts client on the defense. Indicating an external of power - encourages projection of blame for client’s thought or behaviors onto others. Belittling feelings expressed - cause feelings of insignificance or unimportance. Using stereotypical comments, cliches, and trite expressions - meaningless and have no value. Denial - blocks discussion and avoids identifying and exploring of areas of difficulty. Interpretation - nurse is telling patient the meaning of his/her experience. Introducing unrelated topic - cause nurse to take over the direction of conversation. Active Listening A. B. To Listen - attentive to what the client is saying, both verbally and nonverbally. Nonverbal Facilitating Behaviors 1. 2. 3. 4. 5. VIII. Sit squarely facing the patient. Observe an open posture. Lean forward toward the client. Establish eye contact. Relax Process Recording A. B. C. D. IX. SOLER- Goal directed conversations between the nurse and client. W ritten reports of verbal interactions with clients A tool for improving communication techniques. See Guideline for Interpersonal Process Recording Feedback A. As a technique to convey the following: 1. A descriptive versus evaluative statement which focuses on the behavior rather than on the client. 2. Be specific versus general. 3. Directed at behaviors that the client has the capacity to modify. 4. Imparts information rather than offering advice. 5. Be well timed. 5.23 BAPTIST HEALTH SCHOOL OF NURSING NSG 3036A: PSYCHIATRIC-MENTAL HEALTH INTERPERSONAL PROCESS RECORDING PATIENT INITIALS: STUDENT: AGE: INSTRUCTOR: DIAGNOSIS: DATE: PROBLEM/NURSING DIAGNOSIS EXPECTED OUTCOME OR GOAL STATEMENT PATIENT BEHAVIOR STUDENT NURSE BEHAVIOR TECHNIQUE & ANALYSIS 5.24 PATIENT BEHAVIOR Form Originated: September 1986 (C.C.) Content Approved: January 2006 (C.C.) STUDENT NURSE BEHAVIOR TECHNIQUE & ANALYSIS