Case Studies of Lower Respiratory Tract Infections

Supplement issue
Case Studies of Lower Respiratory Tract Infections:
Community-Acquired Pneumonia
Thomas M. File, Jr., MD, MSc
Department of Internal Medicine and Infectious Disease Section, Northeastern Ohio Universities Colleges of Medicine and Pharmacy,
Rootstown, Ohio, USA; and Infectious Disease Service and Division of HIV Research, Summa Health System, Akron, Ohio, USA
ABSTRACT
Community-acquired pneumonia (CAP) is a common and potentially serious illness with significant human and economic costs to society. The recent collaborative statement from the Infectious Diseases Society of
America (IDSA) and the American Thoracic Society (ATS) represents the most up-to-date evidence-based guidelines from North America, incorporating important advances in the management of patients with
CAP. The cases presented in this review highlight many of the recent recommendations from the
IDSA/ATS guidelines.
© 2010 Elsevier Inc. All rights reserved.
• The American Journal of Medicine (2010) 123, S4 –S15
KEYWORDS: Community-acquired infection; Fluoroquinolone; Methicillin-resistant Staphylococcus aureus ; Respiratory disorders; Tuberculosis
Infectious Diseases Society of America (IDSA) and the
American Thoracic Society (ATS), which incorporates im-
portant advances in the management of patients with CAP.
The cases presented in this review highlight many of the recent recommendations from the IDSA/ATS guidelines.
Community-acquired pneumonia (CAP) is a common and potentially serious illness, particularly in elderly patients
and those with significant comorbidities.
In the United
States, CAP is the most frequent cause of death due to infectious disease and is the eighth leading cause of death
The mortality rate of patients treated on an outpatient basis is
⬍
1%; the rate for those who require admission to the hospital averages 12%, but it approaches 40% for patients with severe CAP who require admission to the
The annual estimated incidence of CAP requiring hospitalization is 267 individuals per
100,000 population and 1,014 individuals ⱖ
65 years of
More cases occur during the winter months. The estimated economic cost in the United States exceeds $12
In light of the impact of CAP, numerous professional societies have developed guidelines for management of
The primary purposes of these guidelines are to optimize care and, ultimately, improve outcome of patients. The most recent evidence-based guidelines from
North America are the collaborative statement from the
Statement of author disclosure: Please see the Author Disclosures section at the end of this article.
Requests for reprints should be addressed to Thomas M. File, Jr., MD,
MSc, Infectious Disease Service and Division of HIV Research, Summa
Health System, 75 Arch Street, Suite 506, Akron, Ohio, 44304.
E-mail address: filet@summa-health.org
.
0002-9343/$ -see front matter © 2010 Elsevier Inc. All rights reserved.
doi:10.1016/j.amjmed.2010.02.002
CASE 1
Presentation
A 66-year-old man presented to his primary care practitioner with a headache, fever, and cough for the previous 3 days, and recent bouts of confusion.
History and Physical Examination
The patient had smoked cigarettes (approximately 1 pack per day) since age 17, had had type 2 diabetes mellitus for
15 years, and had coronary artery bypass surgery 12 years ago. He was treated with a macrolide (azithromycin) for sinusitis 8 weeks before presentation. Vital signs were as follows: temperature, 100.8°F (38.2°C); pulse, 110 beats per minute, respiratory rate, 28 breaths per minute. Auscultation of his lungs revealed rhonchi in the right lower lobe. A blood test showed leukocytosis (white blood cell [WBC] count 20,000 per mm
3
(20
⫻
10
9
/L), and his blood glucose level was 180 mg/dL (1 mg/dL ⫽ 0.0555 mmol/L).
File Management of Lower Respiratory Infections: Case Studies S5
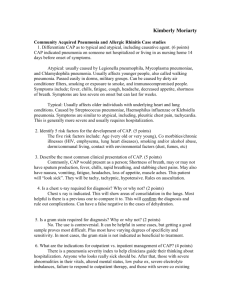
Figure 1 Plain chest radiograph showing presence of right lower lobe infiltrate.
Comment.
A patient presenting to a practitioner’s office with cough (either productive or nonproductive), pleuritic chest pain, shortness of breath, temperature
⬎
38°C, and crackles on auscultation shows the classic signs and symptoms of CAP. As seen with this patient, mental status changes may complement respiratory manifestations of the disease; gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea) also may be present. Leukocytosis (WBC count between
⬃
15,000/mm
3 and 30,000/mm
3
) with a leftward shift is the major blood test abnormality observed in patients with CAP. No clear constellation of symptoms and signs has been observed to universally and accurately predict the patient with pneumonia. A demonstrative infiltrate by imaging techniques and/or supporting microbiologic data also are necessary.
Diagnostic Testing
The presence of a right lower lobe infiltrate was detected on
a plain chest radiograph ( Figure 1 ). Although this patient’s
clinical picture does suggest CAP, clinical symptoms and signs alone are not specific for the definitive diagnosis, especially in elderly patients. A chest imaging study is
required for an accurate diagnosis.
The presence of a new infiltrate on a chest radiograph is considered the “gold standard” when clinical features are supportive, as in this patient. Radiologists are unable to reliably differentiate between bacterial and nonbacterial pneumonia based on radiographic appearance.
Diagnosis
The patient was diagnosed with CAP.
Determination of Site of Care
The patient was determined to have a class III Pneumonia
Severity Index (PSI) classification and a CURB-65 (confusion; urea
⬎
7 mmol/L; respiratory rate ⱖ
30/min; low systolic [
⬍
90 mm Hg] or diastolic [ ⱕ
60 mm Hg] blood pressure; age ⱖ
65 years) score of 2—a classification associated with a mortality rate of 8% to 9%. The patient was admitted to a local hospital for care.
Comment.
After establishment of the diagnosis, the next management decision is to determine the site of care. This determination has an impact on the intensity of diagnostic testing and options for empirical antimicrobial therapy. Advantages of outpatient therapy include preference by most patients (if considered safe), association with faster convalescence of illness, avoidance of potential nosocomial complications, and decreased cost. The general consensus in the medical care community is that the majority of patients with
CAP can indeed be treated safely as outpatients. However, selected patients (like the patient in this case study) should
S6 be hospitalized based on their risk for poor outcome, which may be mitigated by close observation, respiratory support, intravenous antibiotics, and management of comorbid illness. Deciding on whether to hospitalize a patient is based on such tools as the Pneumonia Prediction Rule and the
The Pneumonia Prediction Rule utilizes a combination of demographic variables, comorbidities, physical observations, and laboratory and radiographic vari-
ables to assign patients to 1 of 5 classes.
The classes are demarcated by distinct risks of mortality and consequent recommendations regarding site of care as shown in
scoring to determine class is shown in
Our current patient merits a class III status (PSI score 86 points [age 66 years
⫹ confusion 20]) with a risk of mortality of
⬍
5%, and is suggested for brief hospital observation. Although the Pneumonia Prediction Rule is effective in determining mortality risk, it is not “user-friendly” in the clinical setting, because it includes laboratory results that may not be available when a disposition decision must be made. The CURB-65 Rule is more useful at the bedside, because it uses a much less rigorous process in its clinical determination—measurements include confusion, urea concentration, respiratory rate, blood pressure, and age. The patient with CAP in this case study scored a 2 (age ⱖ
65 years
⫹ confusion), which also merits hospitalization. Despite its simplicity, however, the CURB-65 may be considered impractical because both a blood sample and laboratory analysis of blood urea often are required. As a result, the CRB-65 was devised; it eliminates the blood urea determination but is otherwise identical to the CURB-65 and, therefore, is optimally designed for the office setting (see
and
Figure 3 ). The performance of CRB-65 was
shown to be comparable to CURB-65 and PSI in a study by
Thus, once the diagnosis is established, the PSI or CURB-65 (or CRB-65) scores can support an initial site-of-care decision (i.e., hospital versus outpatient).
Diagnostic Testing for Etiology
A blood culture, sputum Gram stain, and urinary antigen test were performed. In recent guidelines most tests are considered optional, but I advocate performing blood cultures, sputum Gram stain and culture, and urinary antigen tests for Streptococcus pneumoniae and Legionella species for patients requiring admission to the hospital. However, obtaining these tests should never delay administration of antimicrobial therapy because timely administration is critical for good outcome. Positive blood cultures are observed in approximately 11% of high-risk patients with CAP, although falsepositive blood cultures can lead to prolonged hospital stays
with significantly greater use of vancomycin.
It may be difficult to obtain a good sputum sample, and validity of the Gram stain may be influenced by such factors as specimen collection, transport time to the microbiology laboratory, rapidity of sample processing, satisfactory use of cytologic criteria, absence of prior antibiotic therapy, and experience of the interpreter; however, when stringent cri-
The American Journal of Medicine, Vol 123, No 4A, April 2010
Table 1 Pneumonia prediction rule
Total Points Class Mortality (%) How to Treat ⱕ 70
71-90
91-130
⬎ 130
I
II
III
IV
V
0.1
0.6
0.9-2.8
8.2-9.3
27.0-29.2
Outpatient
Outpatient
Brief hospital observation
Inpatient
Inpatient ICU
ICU
⫽ intensive care unit. Adapted from
Table 2 Point scoring system for assignment to risk classes
II, III, IV, and V
Points Assigned Characteristic
Demographic Factor
Age
Men
Women
Nursing home resident
Coexisting illnesses
Neoplastic disease
Liver disease
Congestive heart failure
Cerebrovascular disease
Renal disease
Physical examination findings
Altered mental status
Respiratory rate ⱖ 30/min
Systolic blood pressure ⬍ 90 mm Hg
Temperature ⬍ 35°C or ⱖ 40°C
Pulse ⱖ 125 beats/min
Laboratory and radiographic findings
Arterial pH ⬍ 7.35
Blood urea nitrogen ⱖ 30 mg/dL
(11 mmol/L)
Sodium ⬍ 130 mmol/L
Glucose ⱖ 250 mg/dL (14 mmol/L)
Hematocrit ⬍ 30%
Partial pressure of arterial oxygen
⬍ 60 mm Hg
Pleural effusion
Adapted from
Age (yr)
Age (yr)
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
⫹
10
30
20
10
10
10
20
20
20
15
10
30
20
20
10
10
10
10
⫺ 10 teria are applied, specificity for pneumococcal pneumonia
Epidemiologic trends should be considered in deciding to perform additional diagnostic tests for less usual CAP pathogens, such as fungus or Mycobacteria species.
The urinary antigen test for S pneumoniae is 50% to
80% sensitive and ⱖ
In a prospective study of 269 patients with CAP and no identifiable pathogen, S pneumoniae urinary antigen was de-
tected in 69 (27.5%) of those patients.
The additional information on etiology may help narrow down choices of antibiotic therapy.
File Management of Lower Respiratory Infections: Case Studies S7
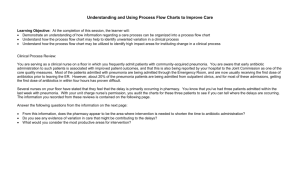
Figure 2 CRB-65 versus CURB-65 and Pneumonia Severity Index (PSI). CURB-65
⫽ confusion; urea ⬎ 7 mmol/L; respiratory rate ⱖ 30/min; low systolic ( ⬍ 90 mm Hg) or diastolic ( ⱕ 60 mm
Hg) blood pressure; age ⱖ
65 years; CRB-65
⫽ confusion; respiratory rate ⱖ
30/min; low systolic
( ⬍ 90 mm Hg) or diastolic ( ⱕ 60 mm Hg) blood pressure; age ⱖ 65 years. (Adapted from Eur
Respir J
Treatment
The patient was administered levofloxacin 750 mg once daily for 5 days. The patient was stabilized by the second day of therapy and was switched from intravenous to oral therapy.
For the majority of patients, an etiologic pathogenic agent will not be identified owing to the lack of rapid diagnostic methods. Consequently, an empirical approach to initial therapy is typically based on the likelihood that a key pathogen is responsible. For this patient (hospitalized, non-
ICU) the most common pathogens include S pneumoniae ,
Mycoplasma pneumoniae , Chlamydia pneumoniae , Haemophilus influenzae , or Legionella species.
Empirical treatment of CAP is nearly universal because pathogen identification, when possible, is generally not available when a treatment decision needs to be made, and the presenting clinical features are not specific enough to reliably predict the etiology of CAP. The recommended treatment option for an inpatient on the general ward is either combination therapy with a

-lactam, such as cefotaxime, ceftriaxone, ertapenem, or ampicillin-sulbactam, plus azithromycin, or monotherapy with a respiratory fluo-
roquinolone (levofloxacin, moxifloxacin, gemifloxacin).
Because the patient previously had been treated with a macrolide, levofloxacin 750 mg once daily was adminis-
A switch from intravenous to oral treatment is recommended once the patient is stable, typically by the second or third day of treatment in most cases even if S pneumoniae bacteremia is present. A treatment duration of
5 days is often adequate for either an outpatient or general ward patient with CAP, assuming the patient is doing well at 48 to 72 hours and in the absence of an unusual pathogen.
When deciding on initial therapy, the clinician should always ask the patient whether she or he has received antimicrobials within the last 3 months, because this is an important risk factor for antimicrobial resistance. In such cases, empirical therapy with a different antibiotic class is preferred.
Outcome
The patient’s fever was reduced within 3 days of therapy.
His cough and fatigue remained for several weeks. Despite an initial good response from antimicrobial therapy with resolution of fever and acute morbidity, it is very common for patients to experience prolonged cough and malaise. To increase their understanding of their illness and expected clinical course, patients should be informed that symptoms can last for a prolonged period.
Although this patient was treated successfully, up to 15% of patients may not respond appropriately to initial antibiotic treatment. The most common causes of treatment failure are lack of or delayed response by the host despite appropriate antibiotics or infection with an organism that is not covered by the initial antibiotic regimen. Other causes of treatment failure include a resistant pathogen, an unusual pathogen, a suppurative complication (e.g., empyema), or obstruction. It should be noted that a chest radiograph can
S8 The American Journal of Medicine, Vol 123, No 4A, April 2010
Figure 3 Calculation of CURB-65 (confusion; urea ⬎ 7 mmol/L; respiratory rate ⱖ
30/min; low systolic [
⬍
90 mm Hg] or diastolic [ ⱕ
60 mm Hg] blood pressure; age ⱖ 65 years). DBP ⫽ diastolic blood pressure; ICU ⫽ intensive care unit; SBP ⫽ systolic blood pressure. (For urea 7 mmol/L
⫽
20 mg/dL.) (Reprinted with permission from
Thorax
remain abnormal for weeks (even in the presence of successful treatment).
CASE 2
Presentation
A 79-year-old woman presented to her primary care practitioner with progressive weight loss, malaise, and a nonproductive cough that had developed over the past 3 weeks.
History
The patient had several comorbid conditions, including obesity, type 2 diabetes, and hypertension. The last time she recalled having a persistent cough (although less severe than what she was now experiencing) was 10 years prior, when she had been administered an angiotensin-converting enzyme (ACE) inhibitor to control her hypertension; the ACE inhibitor was discontinued and she remained on a daily regimen of an angiotensin receptor blocker with a diuretic.
Her greatest complaint in recent visits had been deteriorating vision related to macular degeneration. She had a stilted gait secondary to a hip fracture repair experienced 5 years ago. Her history also included a nonmalignant breast mass that had been biopsied approximately 10 years ago. She had a remote smoking history of approximately 2 packs of cigarettes per day, but she had quit in her late 40s.
Physical Examination
Physical examination revealed a fever (100.5°F [38.1°C]), elevated blood pressure 140/90 mm Hg, and a loss of 3 lb
(1.35 kg) since her last visit 4 months prior. The patient had shortness of breath and, upon auscultation of her lungs, rales were heard bilaterally. Blood analysis showed hemoglobin of 11.4 g/dL (114 g/L), WBC of 9.48
⫻
10
9
/L, and a platelet count of 349
⫻
10
9
/L. A chest radiograph performed in the office was interpreted as showing chronic fibrotic changes and probable small patchy infiltrates.
Treatment
The patient was treated with an oral fluoroquinolone for 5 days and was scheduled for a return to the office at the end of therapy. In such cases as this patient with several comorbidities, empirical antibiotic therapy for an outpatient with
CAP includes a respiratory fluoroquinolone. These agents
File Management of Lower Respiratory Infections: Case Studies S9
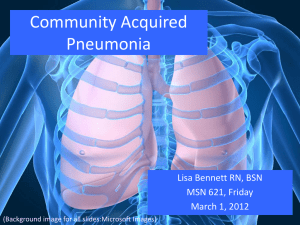
Figure 4 Chest radiograph showing progressive bilateral fibronodular diseases.
Table 3 When to suspect tuberculosis as a cause of community-acquired pneumonia
● Patients from endemic areas
● Chest x-ray: upper lobe infiltrate, cavitation, miliary pattern
● Hemoptysis or ⬎ 1 mo of any of the following: cough, fever, malaise, weakness, night sweats, or significant weight loss
● Nursing home patients, homeless, prison dweller, alcoholism
● Human immunodeficiency virus
● Exposure to tuberculosis
Adapted from
are widely chosen as empirical therapy for CAP owing to their broad-spectrum activity, high bioavailability, and convenient dosing schedules.
Posttreatment Assessment
The patient felt improved at the conclusion of therapy and canceled her follow-up appointment. The office receptionist placed her call through to the physician assistant, to whom the patient reported that her cough had dissipated somewhat and that she no longer had a fever.
Return Visit
The patient returned to the office 2 months later concerned that she had been “coughing up blood” over the previous 2 days. In addition to hemoptysis, the patient revealed that since her previous visit she had continued to feel malaise, was continuing to lose weight, and had been experiencing night sweats. The primary care physician suspected tuberculosis (TB) (the patient now recalled that a family member had once been diagnosed with TB) and had the patient transferred immediately for isolation in a local hospital.
A repeat chest radiograph revealed progressive bilateral fibronodular diseases with a “miliary” pattern (see
The hospitalist ordered a sputum culture and the culture was subsequently positive for Mycobacterium tuberculosis .
Diagnosis
The patient was diagnosed with TB. Although TB is frequently overlooked as a cause of CAP, it is responsible for
approximately 0.3% of cases in the United States.
This is far removed from the prevalence seen in the epicenter of the human immunodeficiency virus (HIV) pandemic in sub-
Saharan Africa. An indication of TB as a common cause of
CAP is illustrated by a prospective study of 266 patients admitted with a diagnosis of CAP in a hospital in Durban,
South Africa, between May 2000 and July 2001—a highprevalence HIV setting. A microbiologic diagnosis of 169 patients (64%) showed 44 with TB, 31 with Pneumocystis jirovecii
pneumonia, and 35 with bacterial pneumonia.
A retrospective review of patients with active TB shows how pulmonary TB was unsuspected in a 515-bed, university-affiliated, community teaching hospital located in Akron, Ohio. In patients with cultures for M tuberculosis (1983 to 1987), of 31 cases with active disease (admitted to 9 different services), TB was not suspected in 13 (42%). The patients with unsuspected TB were older, had a delay in isolation (1 vs. 6 days; P
⫽
0.002), had a longer hospitalization (16 vs. 11 days; P
⫽
0.02), and showed a higher mortality rate (46% vs. 11%; P ⫽ 0.07). Interestingly, most were admitted with a diagnosis of CAP as well as carcinoma of the lung and congestive heart failure, among the admitting diagnoses; of note, these patients did not belong to populations traditionally thought to be at risk. In the 13 patients with unsuspected TB, the chest radiograph findings were as follows: upper lobe infiltrate and/or cavitation (n
⫽
6), lower lobe infiltrate (n
⫽
2), bilateral diffuse infiltrate
(n ⫽ 2), pulmonary nodule (n ⫽ 1), pleural effusion (n ⫽ 1), and bilateral apical scarring (n
⫽
shows when to suspect TB as a cause of CAP,
S10 The American Journal of Medicine, Vol 123, No 4A, April 2010
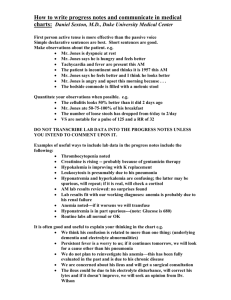
Figure 5 Cases of tuberculosis per 100,000 population (2000). (Courtesy of University of California at Santa Cruz.) and
shows worldwide endemic areas for TB. To avoid misdiagnosing TB as CAP, it is recommended that the following patients be considered suspect for TB: (1) patients with a chest radiograph showing upper lobe infiltrate, cavitation, and a miliary pattern; (2) patients with hemoptysis or
⬎
1 month of any cough, fever, malaise, weakness, night sweats, or significant weight loss; (3) patients failing or relapsing after empirical therapy; and (4) any patient with
HIV, regardless of CD4 count, with a known history of positive tuberculin skin test, previous TB, or recent expo-
sure to TB, who presents with CAP.
Fluoroquinolones should not be used as first-line therapy to treat CAP in areas of endemic TB or in the other conditions listed in
Table 2 . These drugs are likely to both mask
active TB and select for quinolone resistance in the infect-
Thus, clinicians should be aware of risk factors associated with TB pneumonia and avoid using a fluoroquinolone empirically in these patients owing to the risk of promoting fluoroquinolone resistance.
As observed in the present case, several studies have demonstrated delays in the treatment of TB in patients
treated empirically with fluoroquinolones.
In a retrospective study of 33 patients with culture-confirmed TB at
Johns Hopkins Hospital in Baltimore, Maryland, 16 (48%)
patients received fluoroquinolones for presumed CAP.
The median time between presentation to the hospital and initiation of TB treatment was 21 days in those patients treated with fluoroquinolones compared with 5 days in those patients who did not receive fluoroquinolone therapy ( P
⫽
0.04). This delay in treatment may be ascribed to partial symptom resolution, as observed in the present case. Although the patient in this case recovered fully, empirical treatment with fluoroquinolones with the consequent delay in treatment has been associated with poorer outcomes as compared with patients who do not receive fluoroquino-
Monotherapy with an empirical fluoroquinolone in patients with suspected CAP who have TB may be associated with an initial partial response, but it is followed by gradual worsening of symptoms leading to poorer outcomes.
In a study by Ginsburg and colleagues,
2 of 55 M tuberculosis isolates were found to have decreased susceptibility to fluoroquinolones, compared with 0 of 36 isolates from nonfluoroquinolone-treated patients. However, this was in a relatively small sample and more recent studies have questioned whether empirical treatment with fluoroquinolones is a concern in terms of increased M tuberculosis
For example, Huang and coworkers
found that fluoroquinolone resistance was restricted to multidrug resistant (MDR) strains and was a consequence of treating patients with MDR TB strains rather than empirical use in the community setting. In a study of 420 M tuberculosis isolates from January 2004 to December 2005 in endemic areas of Taiwan, it was found that neither previous use of fluoroquinolones nor duration of fluoroquinolone exposure was correlated with fluoroquinolone susceptibility of the
propose that increasing empirical use of fluoroquinolones to treat CAP may not necessarily lead to increased numbers of resistant M tuberculosis clones in the future. This supposition is based on the use of fluoroquinolones in combination therapy and by the use of
File Management of Lower Respiratory Infections: Case Studies fluoroquinolones at doses that exceed the resistance levels of spontaneous mutants to thereby prevent their amplification. In any event, fluoroquinolones should not be given as first-line empirical treatment when TB is suspected.
Treatment
The patient had confirmed miliary TB with positive sputum and bone marrow cultures. She was administered isoniazid, rifampin, pyrazinamide, and ethambutol for 7 days per week for 8 weeks, followed by isoniazid and rifampin 7 days per week for 24 weeks.
Outcome
The patient responded well to the drug regimen.
CASE 3
Presentation
On a late afternoon in mid-November, a 33-year-old corrections officer was brought by her husband to their primary care practitioner. The husband stated that his wife had come home from work late that morning not feeling well and developed a high fever and difficulty breathing over the course of the afternoon. She had been to visit the primary care practitioner 5 days prior for a respiratory virus and had been experiencing a lingering and severe cough that had been deteriorating over time.
History and Physical Examination
The patient was moderately overweight (body mass index,
28.5). She had smoked cigarettes since age 15 (approximately 2.5 packs per day) and drank beers liberally (
⬃
6 beers per night). Aside from her recent visit for flu-like symptoms, she had visited her primary care practitioner over the previous year for minor lacerations and a jobrelated shoulder separation. She had no history of chronic disease, but had a family history of hypertension and coronary artery disease. Her father had a fatal myocardial infarction at age 54.
Her vital signs were as follows: temperature, 101.3°F
(38.5°C); pulse, 135 beats per minute; and respiratory rate,
33 breaths per minute. On auscultation, bilateral coarse rhonchi could be heard in both the left and right lung fields.
The primary care practitioner was concerned about the condition of this patient based on the results of the examination. Although the patient had no history of methicillinresistant Staphylococcus aureus (MRSA) infections or colonizations, her job in the prison environment was a risk factor suggestive of community-acquired MRSA (CA-
MRSA) pneumonia—particularly as a potential secondary bacterial infection postinfluenza. As a consequence, the patient was referred immediately to the local university medical center emergency department (ED), where she was met by an attending pulmonologist colleague of her primary care practitioner.
S11
CA-MRSA as the causative pathogen in patients with
CAP is becoming more common, such that practitioners should be aware of local prevalence patterns and associated risk factors. Under such conditions, patients presenting with severe CAP should be urged by their primary care practitioner to seek immediate medical attention at a local ED. As in this patient, CA-MRSA pneumonia should be suspected in young, previously healthy adults who have had a flu-like illness—particularly those who participate in close-contact settings (sports participants [e.g., football players, wrestlers, fencers], prisoners in correctional facilities, children in day care and other institutional centers, military recruits), male homosexuals, and people in the general population who
Clinicians should determine from the patient (and caretaker, if necessary) social and family history, history of recurrent infections, any recent contact with healthcare facilities, or if any family members have a history of skin abscesses or cellulitis or are
The key to rapid diagnosis of CA-
MRSA is a high level of suspicion.
ED Visit (Diagnostic Testing)
Upon initial examination of the patient, the pulmonologist
ordered a chest radiograph ( Figure 6 ) and measurement of
arterial blood gases. Bilateral infiltrates were observed throughout both lung fields. Blood gas measurements (partial pressure of oxygen [Po
2
]
⫽
42 mm Hg) confirmed that the patient had severe hypoxia.
The patient in this case had bilateral infiltrates. Patients with CA-MRSA pneumonia characteristically exhibit bilateral consolidation and multilobular cavitating alveolar in-
filtrates, and possibly the presence of pleural effusion.
Cavitation possibly caused by the Panton-Valentine leukocidin toxin associated with CA-MRSA pneumonia may not show on a chest radiograph initially, but may develop rapidly. A computed tomography scan or magnetic resonance imaging are suggested for the optimal evaluation of the
Initial Treatment
As a consequence of the severe hypoxia, the patient was intubated and placed on a mechanical respirator. Prior to intubation, she was administered a third-generation cephalosporin and azithromycin. At the time of intubation a
Gram stain of endotracheal aspirate showed many polymorphonuclear leukocytes and many gram-positive cocci in clusters (see Gram stain under “Laboratory Testing” below). Intravenous vancomycin (15 mg/kg every 12 hours) was initiated.
The IDSA/ATS guidelines recommend the use of vancomycin or linezolid in cases of suspected CA-MRSA pneu-
Susceptibility data show that CA-MRSA isolates are becoming more resistant to multiple drugs/drug classes, including clindamycin, fluoroquinolones, mupirocin, and
Moreover, clindamycin and linezolid may act to reduce or suppress Panton-Valentine leukocidin produc-
tion through protein synthesis inhibition.
S12 The American Journal of Medicine, Vol 123, No 4A, April 2010
Figure 6 Chest radiograph showing bilateral pulmonary infiltrates.
Laboratory Testing
A Gram stain of endotracheal secretions ( Figure 7 ) revealed
gram-positive cocci in clusters typical of S aureus . According to the IDSA/ATS 2007 guidelines, a Gram stain should be obtained from patients at risk for CA-MRSA pneumo-
If the Gram stain and culture results of an adequate respiratory specimen are negative, these results alone should be adequate to withhold or stop treatment for CA-
MRSA pneumonia.
Diagnosis
The patient was diagnosed with CA-MRSA. Evidence supportive of the diagnosis in this patient included the patient’s preceding influenza-like illness, Gram stain evidence of gram-positive cocci clusters, chest radiograph with bilateral infiltrates, and laboratory findings.
Additional Treatment
Based on the results of the Gram stain, treatment with vancomycin was maintained. The patient’s WBC count was
4,100/
L (4.1
⫻
10
9
/L).
Outcome
Despite urgent care, the patient’s condition deteriorated and she died 12 hours after presentation to the hospital. There was evidence of multiple organ failure (abnormal coagulation studies, elevated liver function tests, and anuria). Endotracheal aspirate cultures exhibited heavy growth of MRSA. Follow-up typing of the pathogen led to its identification as the
Panton-Valentine leukocidin–positive USA300 MRSA strain indicative of CA-MRSA.
The patient died of virulent CA-MRSA pneumonia that carried the Panton-Valentine leukocidin gene and isolate banding patterns consistent with the USA300 pulsed-field
type as described by Francis and associates.
Recent reports of 2 case series of 50 patients in France and 51 patients in the United States show mortality to be
⬃
50% in
patients with CA-MRSA pneumonia.
A total of 14 of
20 patients with confirmed Panton-Valentine leukocidin– secreting CA-MRSA died despite being treated with appro-
The illness is typically characterized by severe respiratory symptoms, hemoptysis, high fever, leukopenia, and hypotension. Risk factors for mortality include influenza, requirement for intubation, need for inotropic
File Management of Lower Respiratory Infections: Case Studies S13
Figure 7 Gram stain showing gram-positive cocci.
support, acute respiratory distress syndrome, hemoptysis,
Although early reports of CA-MRSA pneumonia suggest a high association with necrotizing infection with high mortality, it is quite likely that less severe cases also occur.
Optimal antimicrobial therapy of CA-MRSA pneumonia is not well defined. The recent IDSA/ATS guidelines recommend vancomycin or linezolid for severe pneumonia. In our case, the patient rapidly deteriorated despite vancomycin therapy; however, it is unlikely that any alternative intervention in the ED in the context of her clinical condition would have resulted in survival. Therapeutic failures with vancomycin may be a result of the greater prevalence of S aureus infections with increasing minimal inhibitory
Other limitations associated with vancomycin that may lead to therapeutic failure include its
poor penetration into the epithelial lining fluid
and its slow bactericidal activity against high-MIC, yet susceptible,
Higher dosing of vancomycin (
⬎
4 g/day) to achieve higher trough serum concentrations may not be
feasible because vancomycin is potentially nephrotoxic.
Because of the lack of randomized controlled trials in
CA-MRSA pneumonia, guidelines are unable to provide strong recommendations beyond use of either vancomycin or linezolid, particularly because these agents are moderately recommended based on level III evidence. (Such evidence comes from case studies and expert opinion. In some instances therapy recommendations come from antibiotic
susceptibility data without clinical observations.
the IDSA/ATS guidelines acknowledge that vancomycin does not decrease Panton-Valentine leukocidin or other toxin production, suggesting the addition of clindamycin or linezolid may be more beneficial for the treatment of ne-
The Canadian guidelines suggest that linezolid may be preferred over empirical therapy with vancomycin based on clinical trial data of adults with healthcare-associated MRSA and improved penetration in
The United Kingdom guidelines acknowledge that “there is as yet no unequivocal clinical evidence to support combination” therapy for CA-MRSA pneumonia, yet they list the use of combination therapy with linezolid plus clindamycin and also acknowledge support
Investigational agents that may fulfill the promise of treating CA-MRSA pneumonia include the cephalosporins (ceftobiprole, ceftaroline fos-
45,46 and the lipoglycopeptides (telavancin).
The association of influenza and secondary CA-MRSA pneumonia is another reason to promote universal influenza vaccination.
(This illustrative case study is a variation of a case recently
reported in a CME-accredited MRSA monograph.
COMMENTARY
The case studies in this article—a typical case of CAP, a case of TB initially treated as CAP, and a severe case of
CA-MRSA— have been described to provide the primary care practitioner with some insight into case management beyond that available by being merely informed of current guideline recommendations. However, what must remain
S14 foremost in the mindset of the primary care practitioner is the prevention of lower respiratory tract infections. These avenues to improve outcome are well characterized; they include smoking cessation, timely administration of vaccines (both pneumococcal and influenza), reducing the effect of comorbidities (e.g., controlling congestive heart failure, hyperglycemia, reducing swallowing disorders [e.g.,
when brushing teeth]), and pandemic preparation.
Moving forward, continuing improvements in the delineation of performance measures will also be instrumental in improving care of patients with CAP. Deviation from performance measures can be deemed acceptable based on individual characteristics because “specific performance
measures cannot cover all host settings.”
Finally, measures should be evaluated for “unintended” consequences, as was observed with the overuse of vancomycin associated with requiring blood cultures for all patients with CAP who were admitted to the hospital (with a consequent high number of false-positive results), as well as forced timing of antimicrobial delivery that led to antibiotic overuse before a
The Centers for Medicare and
Medicaid Services provide performance measures for antibiotic treatment of CAP, underscoring the need for adequate blood culture collection, oxygenation assessment, influenza and pneumococcal immunization, and smoking cessation
ACKNOWLEDGMENTS
Medical writing support for the preparation of this article was provided by Ira Mills, PhD, and Craig Ornstein, PhD, of Embryon; LLC, A Division of Advanced Health Media,
LLC formerly Medesta Publications Group, A Business of
Advogent).
AUTHOR DISCLOSURES
The author of this article has disclosed the following industry relationships:
Thomas M. File, Jr., MD, MSc, has worked as a consultant to Advanced Life Sciences Inc., Astellas/Theravance,
Cerexa, Inc., Merck & Co., Inc., Nabriva Therapeutics
AG, Ortho-McNeil-Janssen Pharmaceuticals, Inc., Oscient
Pharmaceuticals, Pfizer Inc, Protez Pharmaceuticals,
Schering-Plough Corp., Targanta Therapeutics Corp., and Wyeth; has received honoraria from Advanced Life
Sciences Inc., Astellas/Theravance, Cerexa, Inc., Merck
& Co., Inc., Nabriva Therapeutics AG, Ortho-McNeil-
Janssen Pharmaceuticals, Inc., Oscient Pharmaceuticals,
Pfizer Inc, Protez Pharmaceuticals, Schering-Plough
Corp., Targanta Therapeutics Corp., and Wyeth; and has received research/grant support from Boehringer Ingelheim, Cerexa, Inc., Gilead, Ortho-McNeil-Janssen
Pharmaceuticals, Inc., Pfizer Inc, Protez Pharmaceuticals,
Rib-X Pharmaceuticals, Inc., and Tibotec Pharmaceuticals.
The American Journal of Medicine, Vol 123, No 4A, April 2010
References
1. Niederman MS, Mandell LA, Anzueto A, et al, for the American
Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia: diagnosis, assessment of severity, antimicrobial therapy, and prevention.
Am J Respir Crit Care Med.
2001;163:1730-1754.
2. File TM. Community-acquired pneumonia.
Lancet.
2003;362:1991-
2001.
3. File TM Jr, Tan JS. Pneumonia in older adults: reversing the trend.
JAMA.
2005;294:2760-2763.
4. DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National
Hospital Discharge Survey.
Natl Health Stat Rep.
2008;1-20.
5. Kung HC, Hoyert DL, Xu J, Murphy SL. Deaths: final data for 2005.
Natl Vital Stat Rep.
2008;56:1-120.
6. Marston BJ, Plouffe JF, File TM Jr, et al, for the Community-Based
Pneumonia Incidence Study Group. Incidence of community-acquired pneumonia requiring hospitalization: results of a population-based active surveillance study in Ohio.
Arch Intern Med.
1997;157:1709-
1718.
7. Colice GL, Morley MA, Asche C, Birnbaum HG. Treatment costs of community-acquired pneumonia in an employed population.
Chest.
2004;125:2140-2145.
8. Mandell LA, Wunderink RG, Anzueto A, et al, for the Infectious
Diseases Society of America and the American Thoracic Society.
Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults.
Clin Infect Dis.
2007;44(suppl 2):S27-S72.
9. Aujesky D, Fine MJ. The pneumonia severity index: a decade after the initial derivation and validation.
Clin Infect Dis.
2008;47(suppl 3):
S133-S139.
10. Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia.
N Engl J Med.
1997;336:243-250.
11. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study.
Thorax.
2003;58:377-382.
12. Capelastegui A, Espana PP, Quintana JM, et al. Validation of a predictive rule for the management of community-acquired pneumonia.
Eur Respir J.
2006;27:151-157.
13. Metersky ML, Ma A, Houck PM, Bratzler DW. Antibiotics for bacteremic pneumonia: improved outcomes with macrolides but not fluoroquinolones.
Chest.
2007;131:466-473.
14. Musher DM, Montoya R, Wanahita A. Diagnostic value of microscopic examination of Gram-stained sputum and sputum cultures in patients with bacteremic pneumococcal pneumonia.
Clin Infect Dis.
2004;39:165-169.
15. Gutierrez F, Masia M, Rodriguez JC, et al. Evaluation of the immunochromatographic Binax NOW assay for detection of Streptococcus pneumoniae urinary antigen in a prospective study of communityacquired pneumonia in Spain.
Clin Infect Dis.
2003;36:286-292.
16. Dunbar LM, Wunderink RG, Habib MP, et al. High-dose, short-course levofloxacin for community-acquired pneumonia: a new treatment paradigm.
Clin Infect Dis.
2003;37:752-760.
17. Kunimoto D, Long R. Tuberculosis: still overlooked as a cause of community-acquired pneumonia— how not to miss it.
Respir Care
Clin North Am.
2005;11:25-34.
18. Nyamande K, Lalloo UG. Serum procalcitonin distinguishes CAP due to bacteria, Mycobacterium tuberculosis and PJP.
Int J Tuberc Lung
Dis.
2006;10:510-515.
19. Counsell SR, Tan JS, Dittus RS. Unsuspected pulmonary tuberculosis in a community teaching hospital.
Arch Intern Med.
1989;149:1274-
1278.
20. Singh A. Fluoroquinolones should not be the first-line antibiotics to treat community-acquired pneumonia in areas of tuberculosis endemicity.
Clin Infect Dis.
2007;45:133-135.
File Management of Lower Respiratory Infections: Case Studies
21. Wang JY, Hsueh PR, Jan IS, et al. Empirical treatment with a fluoroquinolone delays the treatment for tuberculosis and is associated with a poor prognosis in endemic areas.
Thorax.
2006;61:903-908.
22. Ang D, Hsu AA, Tan BH. Fluoroquinolones may delay the diagnosis of tuberculosis.
Singapore Med J.
2006;47:747-751.
23. Yoon YS, Lee HJ, Yoon HI, et al. Impact of fluoroquinolones on the diagnosis of pulmonary tuberculosis initially treated as bacterial pneumonia.
Int J Tuberc Lung Dis.
2005;9:1215-1219.
24. Avnon LS, Jotkowitz A, Smoliakov A, Flusser D, Heimer D. Can the routine use of fluoroquinolones for community-acquired pneumonia delay the diagnosis of tuberculosis? A salutary case of diagnostic delay in a pilgrim returning from Mecca.
Eur J Intern Med.
2006;17:444-
446.
25. Grupper M, Potasman I. Fluoroquinolones in community-acquired pneumonia when tuberculosis is around: an instructive case.
Am J Med
Sci.
2008;335:141-144.
26. Dooley KE, Golub J, Goes FS, Merz WG, Sterling TR. Empiric treatment of community-acquired pneumonia with fluoroquinolones, and delays in the treatment of tuberculosis.
Clin Infect Dis.
2002;34:
1607-1612.
27. Ginsburg AS, Hooper N, Parrish N, et al. Fluoroquinolone resistance in patients with newly diagnosed tuberculosis.
Clin Infect Dis.
2003;
37:1448-1452.
28. Low DE. Fluoroquinolones for treatment of community-acquired pneumonia and tuberculosis: putting the risk of resistance into perspective.
Clin Infect Dis.
2009;48:1361-1363.
29. Huang TS, Kunin CM, Shin-Jung Lee S, Chen YS, Tu HZ, Liu YC.
Trends in fluoroquinolone resistance of Mycobacterium tuberculosis complex in a Taiwanese medical centre: 1995-2003.
J Antimicrob
Chemother.
2005;56:1058-1062.
30. Wang JY, Lee LN, Lai HC, et al. Fluoroquinolone resistance in
Mycobacterium tuberculosis isolates: associated genetic mutations and relationship to antimicrobial exposure.
J Antimicrob Chemother.
2007;
59:860-865.
31. Nathwani D, Morgan M, Masterton RG, et al, for the British Society for Antimicrobial Chemotherapy Working Party on Community-onset
MRSA Infections. Guidelines for UK practice for the diagnosis and management of methicillin-resistant Staphylococcus aureus (MRSA) infections presenting in the community.
J Antimicrob Chemother.
2008;61:976-994.
32. Gillet Y, Vanhems P, Lina G, et al. Factors predicting mortality in necrotizing community-acquired pneumonia caused by Staphylococcus aureus containing Panton-Valentine leukocidin.
Clin Infect Dis.
2007;45:315-321.
33. Nguyen ET, Kanne JP, Hoang LM, et al. Community-acquired methicillin-resistant Staphylococcus aureus pneumonia: radiographic and computed tomography findings.
J Thorac Imaging.
2008;23:13-19.
34. Diederen BM, Kluytmans JA. The emergence of infections with community-associated methicillin resistant Staphylococcus aureus .
J Infect.
2006;52:157-168.
35. Francis JS, Doherty MC, Lopatin U, et al. Severe community-onset pneumonia in healthy adults caused by methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes.
Clin
Infect Dis.
2005;40:100-107.
36. Kallen AJ, Brunkard J, Moore Z, et al.
Staphylococcus aureus community-acquired pneumonia during the 2006 to 2007 influenza season.
Ann Emerg Med.
2009;53:358-365.
S15
37. Wargo KA, Eiland EH III. Appropriate antimicrobial therapy for community-acquired methicillin-resistant Staphylococcus aureus carrying the Panton-Valentine leukocidin genes.
Clin Infect Dis.
2005;
40:1376-1378.
38. Wang G, Hindler JF, Ward KW, Bruckner DA. Increased vancomycin
MICs for Staphylococcus aureus clinical isolates from a university hospital during a 5-year period.
J Clin Microbiol.
2006;44:3883-3886.
39. Rubinstein E, Kollef MH, Nathwani D. Pneumonia caused by methicillin-resistant Staphylococcus aureus .
Clin Infect Dis.
2008;46(suppl
5):S378-S385.
40. Hidayat LK, Hsu DI, Quist R, Shriner KA, Wong-Beringer A. Highdose vancomycin therapy for methicillin-resistant Staphylococcus aureus infections: efficacy and toxicity.
Arch Intern Med.
2006;166:
2138-2144.
41. Tenover FC, Moellering RC Jr. The rationale for revising the Clinical and Laboratory Standards Institute vancomycin minimal inhibitory concentration interpretive criteria for Staphylococcus aureus .
Clin
Infect Dis.
2007;44:1208-1215.
42. American Thoracic Society, Infectious Diseases Society of America.
Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia.
Am J Respir
Crit Care Med.
2005;171:388-416.
43. Barton M, Hawkes M, Moore D, et al, for the Writing Group of the
Expert Panel of Canadian infectious Disease, Infection Prevention and
Control, and Public Health Specialists. Guidelines for the prevention and management of community-associated methicillin-resistant Staphylococcus aureus : a perspective for Canadian health care practitioners
[published correction appears in Can J Infect Dis Med Microbiol.
2006;
17:396].
Can J Infect Dis Med Microbiol.
2006;17(suppl SC):4C-24C.
44. Conte JE Jr, Golden JA, Kipps J, Zurlinden E. Intrapulmonary pharmacokinetics of linezolid.
Antimicrob Agents Chemother.
2002;46:
1475-1480.
45. Murthy B, Schmitt-Hoffmann A. Pharmacokinetics and pharmacodynamics of ceftobiprole, an anti-MRSA cephalosporin with broad-spectrum activity.
Clin Pharmacokinet.
2008;47:21-33.
46. Micek ST. Alternatives to vancomycin for the treatment of methicillinresistant Staphylococcus aureus infections.
Clin Infect Dis.
2007;
45(suppl 3):S184-S190.
47. Rubinstein E, Corey GR, Stryjewski ME, et al. Telavancin for hospital-acquired pneumonia, including ventilator-associated pneumonia: the ATTAIN studies. Presented at the 18th European Congress of
Clinical Microbiology and Infectious Diseases (ECCMID); April 19,
2008; Barcelona, Spain. Oral presentation O75.
48. Moellering RC Jr, Miller LG, Cosgrove SE, File TM, Corey GR.
Improving clinical practice: MRSA case studies.
MRSA.
2009;2-23.
49. US Department of Health and Human Services. Pandemic flu [HHS
Website.] Available at: http://www.hhs.gov/pandemicflu/.
Accessed
November 2, 2009.
50. File TM Jr, Gross PA. Performance measurement in communityacquired pneumonia: consequences intended and unintended.
Clin
Infect Dis.
2007;44:942-944.
51. Medicare Quality Improvement Community. Measures: pneumonia.
[MedQIC Website.] Available at: http://www.qualitynet.org/dcs/
ContentServer?level3
⫽
Measures&c
⫽
MQParents&pagename
⫽
Medqic%2FMeasure%2FMeasuresHome&cid
⫽
1089815967023& parentName
⫽
Topic.
Accessed November 10, 2009.