Page 1 of 6
View this article online at: patient.info/doctor/facial-nerve-palsy
Facial Nerve Palsy
Synonym: Bell's palsy (lower motor neurone facial palsy); idiopathic facial paralysis (IFP)
Damage to the facial nerve - either upper motor neurone (UMN) or lower motor neurone (LMN) - produces weak
muscles of facial expression.
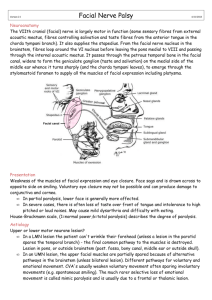
Neuroanatomy [1]
The VIIth cranial (facial) nerve is largely motor in function (some sensory fibres from external acoustic meatus,
fibres controlling salivation and taste fibres from the anterior tongue in the chorda tympani branch). It also
supplies the stapedius (so a complete nerve lesion will alter auditory acuity on the affected side). From the facial
nerve nucleus in the brainstem, fibres loop around the VI nucleus before leaving the pons medial to VIII and
passing through the internal acoustic meatus. It passes through the petrous temporal bone in the facial canal,
widens to form the geniculate ganglion (taste and salivation) on the medial side of the middle ear, whence it turns
sharply (and the chorda tympani leaves), to emerge through the stylomastoid foramen to supply all the muscles
of facial expression, including the platysma.
Presentation
Weakness of the muscles of facial expression and eye closure. The face sags and is drawn across to the
opposite side on smiling. Voluntary eye closure may not be possible and can produce damage to the conjunctiva
and cornea.
In partial paralysis, the lower face is generally more affected.
In severe cases, there is often demonstrable loss of taste over the anterior two thirds of the tongue
and intolerance to high-pitched or loud noises. It may cause mild dysarthria and difficulty with eating.
The most common system used for describing the degree of paralysis is the House-Brackmann scale, where 1
is normal power and 6 is total paralysis. [2]
It is important to identify whether the patient has an UMN or LMN lesion, to assist in identifying the cause.
In an LMN lesion, the patient can't wrinkle their forehead - the final common pathway to the muscles is
destroyed. The lesion must be either in the pons, or outside the brainstem (posterior fossa, bony
canal, middle ear or outside skull).
In a UMN lesion, the upper facial muscles are partially spared because of alternative pathways in the
brainstem, ie the patient can wrinkle their forehead (unless there is bilateral lesion) and the sagging of
the face seen with LMN palsies is not as prominent. There appear to be different pathways for
voluntary and emotional movement.
Cerebrovascular accidents usually weaken voluntary movement, often sparing involuntary movements (eg,
spontaneous smiling). The much rarer selective loss of emotional movement is called mimic paralysis and is
usually due to a frontal or thalamic lesion.
Page 2 of 6
Aetiology [3]
LMN
Idiopathic (Bell's palsy):
Pregnancy - 3x more common.
Diabetes mellitus.
Cerebrovascular disease (eg, brainstem stroke).
Iatrogenic:
Local anaesthetic for dental treatment.
Linezolid. [4]
Infective:
Herpesvirus (type 1).
Herpes zoster (Ramsay Hunt syndrome) - see below.
HIV.
Epstein-Barr virus.
Cytomegalovirus.
Lyme disease (more likely if bilateral when responsible for 36% of cases). [5]
Otitis media or cholesteatoma.
Trauma:
Fractures of the skull base.
Forceps delivery. [6]
Haematoma after acupuncture. [7]
Neurological:
Guillain-Barré syndrome.
Mononeuropathy - eg, due to diabetes mellitus, sarcoidosis or amyloidosis.
Neoplastic:
Posterior fossa tumours, primary and secondary.
Parotid gland tumours.
Hypertension in pregnancy and eclampsia.
Sarcoidosis. [5]
Sjögren's syndrome and rheumatoid arthritis. [8]
Melkersson-Rosenthal syndrome (recurrent facial palsy, chronic facial oedema of the face and lips,
and hypertrophy/fissuring of the tongue). [9]
UMN
Cerebrovascular disease.
Intracranial tumours, primary and secondary.
Multiple sclerosis.
Syphilis.
HIV. [10]
Vasculitides.
If bilateral, particularly consider immunosuppression (HIV), Guillain-Barré syndrome or Lyme disease.
If recurrent, particularly consider lymphoma, sarcoidosis and Lyme disease.
In children, particularly consider Lyme disease and middle ear disease.
Characteristic features
Page 3 of 6
Characteristic features
Acute LMN palsy
Acute LMN palsy can present at any age but is most frequently seen at age 15-60 years, affecting both sexes
equally. There is a rapid onset of unilateral facial paralysis:
Ask the patient to give a big grin showing their teeth.
Ask them to blow out their cheeks.
Ask them to screw up their eyes.
Ask them to raise their eyebrows (preserved in UMN lesion).
Aching pain below the ear or in the mastoid area is also common and may suggest middle ear or
herpetic cause.
There may be hyperacusis.
Patients with lesions proximal to the geniculate ganglion may be unable to produce tears and have
loss of taste.
Bell's palsy [3]
This, the most common cause of acute LMN facial palsy, was originally described by Sir Charles Bell in 1821.
Incidence is 11-40 per 100,000 with a lifetime risk of 1 in 60. [9]
Probably caused by ischaemic compression of the facial nerve within the facial canal, as a result of
inflammation, most likely due to a viral infection.
In the past no cause was found in the majority of cases of LMN facial nerve palsy and these were
labelled as idiopathic (ie Bell's palsy). Increasingly, various viral causes are being identified, particularly
herpes simplex type 1 or varicella (herpes) zoster.
Approximately 7% of patients have a recurrence.
There may be a familial component in recurrent cases, possibly due to anatomical abnormality of the
facial canal. [11]
The incidence is higher in people with diabetes than in those without diabetes.
Ramsay Hunt syndrome
LMN facial nerve palsy due specifically to varicella (herpes) zoster is Ramsay Hunt syndrome. Pain is often a
prominent feature and vesicles are seen in the ipsilateral ear, on the hard palate and/or on the anterior two thirds
of the tongue. It can include deafness and vertigo and other cranial nerves can be affected. When the rash is
absent it is known as zoster sine herpete; 2-23% of people with Bell's palsy actually have Ramsay Hunt
syndrome. [12] It should be suspected when pain is significant, especially in those aged over 60.
Immunodeficiency - for example, HIV - is a risk factor.
Investigations
Serology - Lyme, herpes and zoster (paired samples 4-6 weeks apart). It may not influence
management but may reveal aetiology.
Check blood pressure in children with Bell's palsy (two case reports of aortic coarctation presenting
with facial nerve palsy and hypertension). [13]
The following tests are rarely done but, combined with a good understanding of the neuroanatomy, can
determine the level of the palsy:
Schirmer's tear test (reveals a reduced flow of tears on the side of a palsy affecting the
greater palatine nerve).
Stapedial reflex (an audiological test, absent if the stapedius muscle is affected).
Electrodiagnostic studies (generally a research tool) reveal no changes in involved facial
muscles for the first three days but a steady decline of electrical activity often occurs over
the next week and will identify the 15% with axonal degeneration.
Management [14]
Except in the mildest cases, ideally this should be a multidisciplinary approach, encompassing ophthalmologists,
ENT surgeons, plastic surgeons, physiotherapists and psychologists. [15]
Page 4 of 6
General measures
Reassurance - the majority of cases resolve spontaneously - see 'Prognosis', below.
Eye care:
Ophthalmologists play an important role in preventing irreversible blindness from corneal
exposure. This may be successfully achieved by using lubricating drops hourly and eye
ointment at night ± an eye patch.
Botulinum toxin or surgery (upper lid weighting or tarsorrhaphy) may also be required
temporarily. [15]
After the cornea has been protected but recovery is thought to be unlikely, longer-term
management of eyelid and facial re-animation may be arranged.
Bell's palsy management
Steroids:
Steroids are effective in the treatment of facial nerve palsy. [16] Of the 29% that wouldn't be
expected to fully recover, a third to a half wil do so if given steroids. [3]
Prednisolone should be given to patients over the age of 16 presenting within 72 hours. The
optimum dosing regime is not known but the following are suggested:
25 mg bd for 10 days.
60 mg od for 5 days then reducing by 10 mg each day.
There is no evidence to support the use of steroids after 72 hours.
It is not known whether steroids in children are effective. [17]
There is moderate-quality evidence of benefit from adding antivirals to steroid therapy, with no
significant increase in adverse events. [18] This remains controversial. [19] It is currently not
recommended as treatment in the UK. [14]
Physiotherapy may be beneficial but there is no high-quality evidence to support significant benefit or
harm. [20]
Referral - will depend on clinical assessment. A patient may need immediate hospital referral - eg,
when there is any clinical suspicion of an underlying stroke: [14]
Refer urgently to neurology or to ENT if there is:
Any doubt regarding the diagnosis.
Recurrent Bell's palsy.
Bilateral Bell's palsy.
If the cornea remains exposed after attempting to close the eyelid, refer urgently to
ophthalmology.
If the paralysis shows no sign of improvement after one month, or there is suspicion of a
serious underlying diagnosis (eg, cholesteatoma, parotid tumour, malignant otitis externa),
refer urgently to ENT.
Surgery:
Surgical options for patients with facial palsy not responding to medical treatment include
facial nerve decompression.
If there is residual paralysis after 6-9 months, consider referral to a plastic surgeon with a
special interest in facial reconstructive surgery. The muscle targets remain viable for crossfacial nerve grafting for about 12-18 months. [3]
Where the nerve fails to regenerate, cosmetic surgery to elevate the mouth or anastomosis
of the hypoglossal nerve to the facial nerve may help.
Facial palsy in children
Facial palsy in children is often idiopathic but an underlying cause is increasingly being identified after
thorough investigations. [21]
Radiological investigation is required if there is a history of trauma. [22]
The prognosis is variable but usually good. [23]
Prognosis [14] [24]
Page 5 of 6
Prognosis
[14] [24]
85% improve spontaneously within three weeks of its onset.
71% recover fully.
16% have significant sequelae, 5% severe:
Facial asymmetry
Gustatory lacrimation
Inadequate lid closure
Brow ptosis
Drooling
Hemifacial spasms
Poor prognostic features:
Complete palsy or severe degeneration (electrophysiology).
No signs of recovery by three weeks.
Age >60 years.
Severe pain (suggests may be due to Ramsay Hunt syndrome).
Ramsay Hunt syndrome (herpes zoster virus).
Associated with either hypertension, diabetes, or pregnancy.
Those with axonal degeneration may not show any re-innervation for three months and recovery may be partial or
not at all. Synkinesis is often seen - eg, blinking causes the angle of the mouth to contract. Also aberrant
parasympathetic re-innervation may cause symptoms such as gustatory lacrimation ('crocodile tears').
Symptoms can be helped by subcutaneous or intramuscular injections of botulinum toxin. [25]
Further reading & references
1. Toulgoat F, Sarrazin JL, Benoudiba F, et al; Facial nerve: from anatomy to pathology. Diagn Interv Imaging. 2013
Oct;94(10):1033-42. doi: 10.1016/j.diii.2013.06.016. Epub 2013 Jul 25.
2. House JW, Brackman DE; House Brackman Facial Nerve Grading System 2010.
3. Glass GE, Tzafetta K; Bell's palsy: a summary of current evidence and referral algorithm. Fam Pract. 2014 Dec;31(6):63142. doi: 10.1093/fampra/cmu058. Epub 2014 Sep 10.
4. Thai XC, Bruno-Murtha LA; Bell's palsy associated with linezolid therapy: case report and review of neuropathic adverse
events. Pharmacotherapy. 2006 Aug;26(8):1183-9.
5. Jain V, Deshmukh A, Gollomp S; Bilateral facial paralysis: case presentation and discussion of differential diagnosis. J
Gen Intern Med. 2006 Jul;21(7):C7-10.
6. Duval M, Daniel SJ; Facial nerve palsy in neonates secondary to forceps use. Arch Otolaryngol Head Neck Surg. 2009
Jul;135(7):634-6. doi: 10.1001/archoto.2009.69.
7. Rosted P, Woolley DR; Bell's Palsy following acupuncture treatment - a case report. Acupunct Med. 2007 Jun;25(1-2):47-8.
8. Birnbaum J; Facial Weakness, Otalgia, and Hemifacial Spasm: ANovel Neurological Syndrome in a Case-Series of 3
Patients With Rheumatic Disease. Medicine (Baltimore). 2015 Oct;94(40):e1445. doi: 10.1097/MD.0000000000001445.
9. Cirpaciu D, Goanta CM, Cirpaciu MD; Recurrences of Bell's palsy. J Med Life. 2014;7 Spec No. 3:68-77.
10. Serrano P, Hernandez N, Arroyo JA, et al; Bilateral Bell palsy and acute HIV type 1 infection: report of 2 cases and review.
Clin Infect Dis. 2007 Mar 15;44(6):e57-61. Epub 2007 Feb 8.
11. Qin D, Ouyang Z, Luo W; Familial recurrent Bell's palsy. Neurol India. 2009 Nov-Dec;57(6):783-4.
12. Worme M, Chada R, Lavallee L; An unexpected case of Ramsay Hunt syndrome: case report and literature review. BMC
Res Notes. 2013 Aug 28;6:337. doi: 10.1186/1756-0500-6-337.
13. Margabanthu G, Brooks J, Barron D, et al; Facial palsy as a presenting feature of coarctation of aorta. Interact Cardiovasc
Thorac Surg. 2003 Mar;2(1):91-3.
14. Bell's palsy; NICE CKS, October 2012 (UK access only)
15. Rahman I, Sadiq SA; Ophthalmic management of facial nerve palsy: a review. Surv Ophthalmol. 2007 Mar-Apr;52(2):12144.
16. Salinas RA, Alvarez G, Daly F, et al; Corticosteroids for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst
Rev. 2010 Mar 17;(3):CD001942. doi: 10.1002/14651858.CD001942.pub4.
17. Ismail AQ, Alake O, Kallappa C; Do oral steroids aid recovery in children with Bell's palsy? J Child Neurol. 2014
Oct;29(10):NP96-7. doi: 10.1177/0883073813504624. Epub 2013 Oct 18.
18. Gagyor I, Madhok VB, Daly F, et al; Antiviral treatment for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst
Rev. 2015 Nov 9;11:CD001869. doi: 10.1002/14651858.CD001869.pub8.
19. Kang HM, Jung SY, Byun JY, et al; Steroid plus antiviral treatment for Bell's palsy. J Intern Med. 2015 May;277(5):532-9. doi:
10.1111/joim.12288. Epub 2014 Aug 1.
20. Teixeira LJ, Valbuza JS, Prado GF; Physical therapy for Bell's palsy (idiopathic facial paralysis). Cochrane Database Syst
Rev. 2011 Dec 7;(12):CD006283. doi: 10.1002/14651858.CD006283.pub3.
21. Shargorodsky J, Lin HW, Gopen Q; Facial Nerve Palsy in the Pediatric Population. Clin Pediatr (Phila). 2010 Feb 4.
22. Cha HE, Baek MK, Yoon JH, et al; Clinical features and management of facial nerve paralysis in children: analysis of 24
cases. J Laryngol Otol. 2009 Dec 22:1-5.
Page 6 of 6
23. Lorch M, Teach SJ; Facial nerve palsy: etiology and approach to diagnosis and treatment. Pediatr Emerg Care. 2010
Oct;26(10):763-9; quiz 770-3. doi: 10.1097/PEC.0b013e3181f3bd4a.
24. Finsterer J; Management of peripheral facial nerve palsy. Eur Arch Otorhinolaryngol. 2008 Jul;265(7):743-52. Epub 2008
Mar 27.
25. Filipo R, Spahiu I, Covelli E, et al; Botulinum toxin in the treatment of facial synkinesis and hyperkinesis. Laryngoscope.
2012 Feb;122(2):266-70. doi: 10.1002/lary.22404. Epub 2012 Jan 17.
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical
conditions. EMIS has used all reasonable care in compiling the information but make no warranty as to its
accuracy. Consult a doctor or other health care professional for diagnosis and treatment of medical conditions.
For details see our conditions.
Original Author:
Dr Huw Thomas
Current Version:
Dr Jacqueline Payne
Peer Reviewer:
Dr Laurence Knott
Document ID:
2130 (v25)
Last Checked:
02/02/2016
Next Review:
31/01/2021
View this article online at: patient.info/doctor/facial-nerve-palsy
Discuss Facial Nerve Palsy and find more trusted resources at Patient.
© EMIS Group plc - all rights reserved.