Joint Commission Resources
Quality & Safety Network
Resource Guide
Changes for 2013: Standards and
Survey Process
December 20, 2012
Joint Commission Resources
Changes for 2013: Standards and Survey Process
About Joint Commission Resources
Joint Commission Resources (JCR) is a client-focused, expert resource for healthcare organizations. It partners
with these organizations, providing consulting services, educational services and publications to assist in
improving the quality, safety and efficiency of healthcare services, and to assist in meeting the accreditation
standards of The Joint Commission. JCR is a subsidiary of The Joint Commission, but provides services
independently and confidentially, disclosing no information about its clients to The Joint Commission or others.
Visit our web site at: www.jcrinc.com.
Disclaimers
Joint Commission Resources educational programs and publications support, but are separate from, the
accreditation activities of The Joint Commission. Attendees at Joint Commission Resources educational
programs and purchasers of Joint Commission Resources publications receive no special consideration or
treatment in, or confidential information about, the accreditation process.
The information in this Resource Guide has been compiled for educational purposes only and does not constitute
any product, service, or process endorsement by The Joint Commission or organizations collaborating with The
Joint Commission in the content of these programs.
NOTE: Interactivation Health Networks is the distributor of the Joint Commission Resources Quality & Safety
Network series and has no influence on the content of the series.
©2012 Joint Commission Resources. The purchaser of this educational package is granted limited rights to
photocopy this Resource Guide for internal educational use only. All other rights reserved.
Requests for permission to make copies of this publication for any use not covered by these limited rights should
be made in writing to: Department of Education Programs, Joint Commission Resources, One Renaissance
Boulevard, Oakbrook Terrace, IL 60181.
© 2012 Joint Commission Resources
2 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
TABLE OF CONTENTS
Program Summary .................................................................................................................................................4
Continuing Education (CE) Credit ........................................................................................................................5
Program Outline.....................................................................................................................................................6
Accreditation Process Issues (Ms. Buturusis’ slides) ............................................................................................7
Challenging Clinical Standards and Hot Topics (Ms. Adamski’s slides)............................................................16
Top Standards Compliance Issues .......................................................................................................................25
Appendix A: Faculty Biographies ......................................................................................................................33
Appendix B: Post-Test ........................................................................................................................................35
Appendix C: Resources and Related Information ..............................................................................................37
Appendix D: Continuing Education Credit Information ....................................................................................38
Appendix E: Discipline Codes: Instructions .......................................................................................................39
Appendix F: JCR Quality & Safety Network Contact Information ....................................................................40
© 2012 Joint Commission Resources
3 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Program Summary
This page provides an overview of the program content and learning objectives. Please refer to the Table of
Contents and Program Outline for a detailed list of the topics covered. The information included in this Resource
Guide is intended to support but not duplicate the video presentation content. There may be additional
information available online for this topic.
Program Description
The arrival of 2013 means implementation of changes to the accreditation process, the standards, and elements of
performance (EPs). It is critical for hospital leaders and accreditation managers to stay up-to-date with these
changes.
In this program, experts help you assess your organization's compliance with these new standards and
requirements. This program also focuses on key changes in The Joint Commission's accreditation process, as
well as updated and revised details on new survey activities.
This 60-minute activity features Joint Commission experts who share the new and revised standards, as well as
the accreditation process – with practical, up-to-date information to help all levels of hospital staff to maintain a
state of constant survey readiness.
NOTE: Life Safety (LS) and Environment of Care (EC) standards and issues will not be topics in this program.
LS and EC standards were covered in the October 2012 JCRQSN broadcast and will be program topics
again in 2013.
Program Objectives
After completing this activity, the participant should be able to:
1. Describe new and revised standards.
2. Discuss how to meet new or changed standards.
3. List strategies to meet those standards identified as challenging.
4. Identify changes in the survey process for 2013.
Target Audience
This activity is relevant to organization leaders, medical staff, managers, supervisors, and staff responsible for
accreditation, performance improvement, patient safety, and risk management initiatives.
© 2012 Joint Commission Resources
4 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Continuing Education (CE) Credit
After viewing the JCR Quality & Safety Network presentation and reading this Resource Guide, please complete
the required online CE/CME credit activities (test and feedback form). The test measures knowledge gained
and/or provides a means of self-assessment on a specific topic. The feedback form provides us with valuable
information regarding your thoughts on the activity’s quality and effectiveness.
NOTE: Effective April 1, 2012, the Learning Management System web site URL changed as noted below.
Prior to the Program Presentation Day
1. Login to the JCRQSN Learning Management System web site at http://twnlms.com/
2. Enroll yourself into the program
Note: Your administrator may have already enrolled you in the program
• Select All Courses from the courses menu.
• Select the course category for the current year, 2012 Programs.
• Select the course for this program, Changes for 2013: Standards and Survey Process
• When prompted, choose Yes to confirm that you would like to enroll yourself.
3. Display and print the desire documents (Resource Guide, etc.).
Online Process for CE/CME Credit
1. Read the course materials and view the entire presentation.
2. Login to the JCRQSN Learning Management System web site at http://twnlms.com/
3. Select Changes for 2013: Standards and Survey Process from the courses menu block.
Note: This assumes you have already been enrolled in the program as described above.
4. If you didn’t view the broadcast video presentation, view it online.
5. Complete the online post test.
• You have up to three attempts to successfully complete the test with a minimum passing score of 80%.
• Physicians must take the post test to obtain credit.
6. Complete the program feedback form.
7. On the top right corner of the main course page, you will see your completion status in the Status block.
8. Select Print Certificate from within the Status block to print your completion certificate.
Process for VA Knowledge Network Participants
1. Read the program’s Resource Guide and view the entire video presentation (speak with your administrator
for broadcasting times – do NOT log in to view the program).
2. Complete the Viewer Response form (speak with your administrator to obtain a paper copy that will be
completed manually – do NOT log in to take the online test).
3. Complete the Program Evaluation.
4. Record the answers to the post test where indicated on the Viewer Response form.
5. Return the Viewer Response form by the program due date listed in the upper left corner of the page.
Forms received after this due date will not be eligible for CE credit.
6. Please allow 6 weeks for processing your Viewer Response Form.
* If you have any questions, please contact Lloyd Parish at (562) 826-5505, extension 3856.
© 2012 Joint Commission Resources
5 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Program Outline
Changes for 2013: Standards and Survey Process
December 20, 2012
I.
Introduction
A. Program Content
B. Objectives
C. Faculty
II. Accreditation Process Issues
III. Challenging Clinical Standards and Hot Topics
IV. Survey Process Update
V. Conclusion
VI. Post-Program Live Question and Answer Session
A. Audio only telephone seminar with program faculty – for 30 minutes following the program.
B. Call 1-888-206-0090; enter conference code: 7925428.
Or e-mail your questions or comments to: Questions@jcrqsn.com
Program Broadcast Time
Eastern:
Central:
Mountain:
Pacific:
2:00 p.m. to 3:00 p.m.
1:00 p.m. to 2:00 p.m.
12:00 p.m. to 1:00 p.m.
11:00 a.m. to 12:00 p.m.
During the live airing of this program on December 20, 2012, you may be able to talk directly with the faculty
when prompted by the program’s host. After this date, your message will be forwarded to the appropriate
personnel.
Immediately following the program, we invite you to join in a live discussion with the program presenters. Call
1-888-206-0090 and enter Conference Code: 7925428 to be included in the teleconference.
To submit your question ahead of time or for additional details, please send an e-mail to questions@jcrqsn.com.
If you submit your questions after this date, your message will be forwarded to the appropriate personnel.
You can also receive answers to your questions by calling The Joint Commission’s Standards Interpretation
Hotline at 630-792-5900, option 6.
© 2012 Joint Commission Resources
6 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Accreditation Process Issues (Ms. Buturusis’ slides)
Agenda
•
Value of Accreditation
•
Transitions of Care
•
Primary Care Medical Home
•
Baldrige
•
ISO
•
Intracycle Monitoring (ICM)
Value of Accreditation
How The Joint Commission Helps Shift Your Performance Curve to the Right
© 2012 Joint Commission Resources
7 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Value of Accreditation
Focus
Pay-4-Performance
Joint Commission Enabler
Outcome
• Core Measures: AMI, CHF,
Pneumonia, SCIP
• CTH solutions
• Core Measures Solutions
• Leading Practices Library
• Increase reimbursement
• Reduce risk
Decrease preventable hospital
re-admissions
• CHF core measures
• Standards related to discharge
planning, transitions of care
• CTH solutions, Certification
• Decrease payment denials
• Increase in commercial payer
differentiation
Decrease in HAIs
•
•
•
•
•
• Decrease in risk payment and
denials
• Increase in P4P
• Increase in commercial payer
differentiation
HCAHPs
• Standards on patient rights
• Standards on patient-centered
communication and cultural
competency
New standard on immunization
Standards on Infection Control
CTH hand hygiene project
Leading Practices Library
HAI portal, CLABSI analysis
• Higher HCAHPs scores
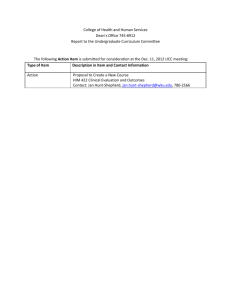
Joint Commission Accredited Hospitals Do Much Better
ORIGINAL RESEARCH
Hospital Performance Trends on National Quality Measures and the
Association With Joint Commission Accreditation
Stephen P. Schmalz, MPH, PhD, Scott C. Williams, PsyD, Mark R. Chassin, MD, MPP, MPH,
Jerod M. Loeb, PhD, Robert M. Wachter, MD
RESULTS: Hospitals accredited by The Joint Commission tended to have better
baseline performance in 2004 than non-accredited hospitals. Accredited hospitals
had larger gains over time, and were significantly more likely to have high
performance in 2008 on 13 out of 16 standardized clinical performance measures
and all summary scores.
JHM October 2011; 6:454-61
© 2012 Joint Commission Resources
8 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Transitions of Care
Organizations with Successful Transitions of Care Have…
•
Multidisciplinary communication, collaboration and coordination – including patient/caregiver education –
from admission through transition.
•
Clinician involvement and shared accountability during all points of transition.
•
Comprehensive planning and risk assessment throughout hospital stay.
•
Standardized transition plans, procedures, and forms.
•
Standardized training.
•
Timely follow-up, support, and coordination after the patient leaves a care setting
Transitions of Care (ToC) Portal
A valuable resource of information
from The Joint Commission
enterprise, related to the topic of
transitions of care (the movement
of patients between various health
care settings).
© 2012 Joint Commission Resources
9 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Primary Care
Medical Home
Agency for Healthcare Research and Quality (AHRQ) Definition of
Medical Home
•
AHRQ believes that the primary care medical home, also referred to as the patient-centered medical home
(PCMH), advanced primary care, and the healthcare home, is a promising model for transforming the
organization and delivery of prompt care.
•
A medical home is not simply a place but a model of primary care that delivers the care that:
– Patient-Centered
– Comprehensive
– Coordinated
– Accessible
– Continuously improved through a systems-based approach to quality and safety
•
AHRQ believes that Health IT, workforce development, and payment reform are critical to achieving the
potential of the medical home.
Joint Commission Hospital Accreditation Plus Option:
Primary Care Medical Home (PCMH)
Baldrige
Baldrige and Joint Commission on Leadership
•
Baldrige centers on the roles and effectiveness of senior leaders.
•
The Joint Commission sharpens that focus by advocating leadership functions that promote patient safety and
quality health care.
•
The ultimate goal for both organizations is helping health care organizations provide better care for patients.
© 2012 Joint Commission Resources
10 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Both Organizations Reach for Excellence Beyond Mandates
Leadership concepts from both organizations that are not in CoPs:
•
Mission, values, goals
•
Ethical behavior and conflict of interest
•
Culture of safety
•
Focus on systems
•
Leadership performance
•
Organization-wide communication
•
Organization-wide strategic planning
ISO 9001:2008/Joint Commission
Focus
•
Joint Commission focuses on quality and safety, systems for providing care, treatment, and services.
•
ISO 9001:2008 standards focus on Quality Management Systems.
What Is an Integrated Approach?
•
A program offering that would combine:
– The Joint Commission’s contemporary health care quality and safety standards, survey process, and
accountability performance measures
– with an ISO 9001: 2008 quality management system audit.
•
The program is in pilot stages now.
•
More to come in 2013.
Components of the Proposed Integrated Survey Model
•
On-site evaluation by surveyors with a blended expertise.
•
Evaluation of The Joint Commission standards compliance.
•
Evaluation of ISO 9001:2008 QMS conformance.
•
Use Joint Commission equivalent standards to evaluate
compliance with Medicare requirements (CoPs).
© 2012 Joint Commission Resources
Evaluation
of common
requirements
11 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Why Are We Piloting It?
Provides a synergistic linking of Joint Commission accreditation and ISO certification with the potential to
enhance quality and safety through greater emphasis on areas such as:
•
Document and records control
•
Systems engineering
•
Medical device calibration and maintenance
•
Environmental management
•
Information security
•
Employee safety
•
Value stream production/efficiency
Intracycle Monitoring
Two Touch Points in the Intracycle Monitoring Process
ICM Goals
•
•
Improve and add value to the periodic performance review.
– To make significant improvements in the current process and
assessment tool (PPR).
– To design a process that is valued, relevant, and efficient for both
customers and The Joint Commission.
Risk
• Proximity to patient
• Probability of harm
• Severity of harm
• Number of patients at risk
Identify risk and proactively manage risk.
– To focus activities on identifying risk points in health care
organizations to help manage risk throughout the accreditation cycle.
– To provide health care organizations with tools/resources/solutions for addressing their risk points.
© 2012 Joint Commission Resources
12 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
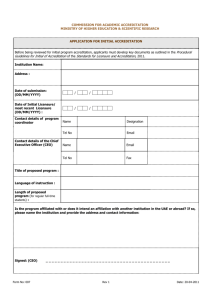
Did We Meet Our Pilot Goals? Feedback from the ICM Pilot (Feb-July 2011)
YES
Are the risk areas identified by The Joint Commission the most important ones for your
organization?
73%
Were you able to identify Accreditation Program risk areas that were previously unknown to your
organization?
72%
Do you think the new Intracycle Monitoring Profile is easy to use?
100%
Is the FSA an improvement over the PPR?
100%
Did you gain new knowledge or insight from participating in the Intracycle Monitoring
Touchpoint call?
96%
Current State (PPR)
PPR Tool – Periodic Performance Review
Future State (CM/FSA)
FSA Tool – Focused Standards Assessment
• Displays all applicable standards for an organization
• Incorporates the “R” risk icon to easily
based upon program and service selections in the
identify standards related to risk areas.
electronic application (eApp).
• Risk areas: all NPSGs, program-specific risk
• All standards must be scored in order to accomplish a
area related standards, selected direct/indirect
“Full PPR” submission.
impact standards, all current cycle survey
RFIs).
• The “R” standards make up the minimum
subset of standards required to be scored in
order to accomplish a “Full FSA”
submission.
• All applicable standards continue to be
displayed and may be included in a “Full
FSA” submission.
Submission Options (PPR Tool)
• Full (all standards must be scored).
• Option 1 (attestation).
• Option 2 Survey (findings documented).
• Option 3 Survey (findings not documented).
© 2012 Joint Commission Resources
Submission Options (ICM Profile/FSA Tool)
• Full (required subset of standards must
be scored).
• Option 1 (attestation).
• Option 2 Survey (findings documented).
• Option 3 Survey (findings not documented).
13 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Current State (PPR)
Future State (CM/FSA)
• ICM Profile – comprehensive extranet work
area.
• Simplified navigation to valuable tools,
resources, and proven solutions.
• Joint Commission identified risk areas with
associated standards for each accreditation
program.
• Ability to self-identify organization-specific
risk areas to be discussed during the
educational conference call.
• Measurement data review included in
conference call.
Risk Icon
•
•
•
Integrated into the Manuals, E-dition, AMP, and FSA Tool.
All products will display a single icon at the EP level for three risk-focused categories:
– National Patient Safety Goals
– Accreditation program-specific risk area standards
– Selected direct/indirect impact standards
In addition, the FSA Tool will use the R icon to identify RFI standards from current cycle survey events.
The ICM Profile
© 2012 Joint Commission Resources
14 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
The ICM Profile
ICM Implementation Timeline
•
Submission function is disabled for the remainder of 2012 to allow organizations to become familiar with the
ICM Profile and FSA tool.
•
Organizations with:
– 2012 submission due dates in Nov. and Dec. 2012 will be granted a 2012 submission extension to
2/11/2013.
– 2013 submission due dates in Jan. and early Feb. 2013 will be granted a 2013 submission extension to
02/11/2013 following the 2013 standards edition update.
Summary
Strategic Direction: The Next Five Years
•
Continue to have an focus on Joint Commission’s mission of “evaluating and inspiring.”
– Value of accreditation, Reimaging Accreditation.
•
Through the Center for Transforming Healthcare, identify solutions to serious patient safety and
quality issues.
– Transitions of care, Primary Care Medical Home, ICM.
•
Help to create solutions to move healthcare toward becoming a high reliability industry.
– Baldrige, ISO.
•
Continue to advocate to CMS and policymakers on behalf of the healthcare field and our
customers’ interests.
©Copyright,
© 2012 Joint Commission Resources
The Joint Commission
15 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Challenging Clinical Standards and Hot Topics (Ms. Adamski’s slides)
Agenda
•
What’s new for 2012/2013?
•
CMS Conditions of Participation Final Rule
•
Most Challenging Standards for 2011/2012
What’s New for 2012/2013?
Catheter-Associated Urinary Tract Infections (CAUTI)
•
NPSG.07.06.01: Implement evidence-based practices to prevent indwelling catheter-associated urinary tract
infections:
– Not applicable to peds population.
– Evidence-based guidelines for CAUTI located at:
http://www.shea-online.org/GuidelinesResources/CompendiumofStrategiestoPreventHAIs.aspx
http://www.cdc.gov/hicpac/cauti/001_cauti.html
– EP 1: During 2012, plan for the full implementation of this NPSG by January 1, 2013.
– EP 2: Insert indwelling urinary catheters according to established evidence-based guidelines that address
the following:
Limiting use and duration to situations necessary for patient care.
Using aseptic techniques for site preparation, equipment, and supplies.
– EP 3: Manage indwelling urinary catheters according to established evidence-based guidelines that
address the following:
Securing catheters for unobstructed urine flow and drainage.
Maintaining the sterility of the urine collection system.
Replacing the urine collection system when required.
Collecting urine samples.
– EP 4: Measure and monitor catheter-associated urinary tract infection prevention processes and outcomes
in high-volume areas by doing the following:
Selecting measures using evidence-based guidelines or best practices.
Monitoring compliance with evidence-based guidelines or best practices.
Evaluating the effectiveness of prevention efforts.
Surveillance may be targeted to areas with high volume (as identified through risk assessment—
IC.01.03.01 EP 2).
© 2012 Joint Commission Resources
16 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Patient Flow
Patient Flow
•
Revisions approved in June of 2012.
– Most become effective January 2013.
– Two EPs become effective January 2014.
•
Standards impacted:
– LD.04.03.11: The hospital manages the flow of patients throughout the hospital.
– PC.01.01.01: The hospital accepts the patient for care, treatment, and services based on its ability to meet
the patient’s needs.
•
2012 Update 2 for the CAMH scheduled for publication Fall 2012 will have the revisions.
•
See Perspectives, July 2012.
•
R3 document coming.
•
LD.04.03.11 Revisions address the following:
– Leadership use of data and measures to identify, mitigate, and manage issues affecting patient flow
throughout the hospital (effective January 2014).
– The management of ED throughput as a system-wide issue.
– Safety for boarded patients.
– Leadership communication with behavioral health providers and authorities to enhance coordination of
care (effective January 2014).
Patient Flow LD.04.03.11
•
Considerations:
– Patient flow throughout the organization including boarding.
Not just the ED
Monitoring
Managing
Anticipating/Mitigating
Cyclical trends
– Clear goals and accountability for improvement.
Goals should consider patient acuity and best practices.
Patient Flow
•
PC.01.01.01 Revision addresses safety for boarded patients who have behavioral health emergencies in the
following areas:
– Environment of Care
– Staffing
– Assessment, reassessment, and the care provided
© 2012 Joint Commission Resources
17 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Patient Flow PC.01.01.01
•
Considerations:
– Behavioral patients boarded for extended periods of time tend to not receive safe, quality care needed for
their needs.
– Staff may not be prepared to deal with this vulnerable but challenging population.
– Environment may not be suited to the needs of the population.
– Policies/practices in the community may add complexity to the issue.
Most Challenging Clinical Standards
2011 Non Compliance
2012 Non Compliance
(1st 6 months)
RC.01.01.01
66%
61%
IC.02.02.01
36%
39%
PC.01.02.03
33%
28%
MM.03.01.01
33%
36%
RC.02.03.07
32%
27%
MM.04.01.01
24%
26%
PC.01.03.01
22%
25%
PC.01.02.07
21%
16%
MS.01.01.01
21%
21%
PC.03.01.03
20%
20%
Standard/NPSG
RC.01.01.01
The hospital maintains complete and accurate medical records for each individual patient.
•
CoP 482.24 Medical Records 482.24(c)(1)
•
Problematic EPs:
– EP 19: all entries are timed.
– EP 11: all entries are dated.
– EP 6: information needed to justify the patient’s care, treatment, services.
•
Issues:
– Stamps
– Buy-in
© 2012 Joint Commission Resources
18 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
IC.02.02.01
The hospital reduces the risk of infections associated with medical equipment, devices, and supplies.
•
CoP Infection Control 482.42
•
CoP Surgical Services 482.51(b)
•
Implements infection prevention and control activities.
– EP 2: when performing intermediate and high-level disinfection and sterilization of medical equipment,
devices, and supplies (EC.02.04.03, EP 4).
Scopes, contamination issues.
– EP 4: when storing medical equipment, devices, and supplies.
– Also consider EP 1: cleaning and performing low level disinfection.
PC.01.02.03
The hospital assesses and reassesses the patient and his or her condition according to defined time frames.
•
Problematic EPs:
– EP 2: initial patient assessments are performed within defined time frame.
– EP 4: the patient receives a medical history and physical examination no more than 30 days prior to, or
within 24 hours after registration or inpatient admission but prior to surgery or procedure requiring
anesthesia services (MS.01.01.01).
– EP 5: update to the H&P documenting any changes is done within 24 hours after admission
(MS.01.01.01).
– CoPs require documentation of the examination and any changes.
Medical Staff: 482.22(c)(5)(ii)
Medical Records: 482.24(c)(2)(i)(b)
Surgical Services: 482.51(b)(1)(ii)
MM.03.01.01
The hospital safely stores medications.
•
CoP Pharmaceutical Services 482.25(a), 482.25 (b)
•
Problematic EPs:
– EP 2: medications are stored according to manufacturer’s recommendations.
– EP 3: all medications and biologicals are stored in secure area to prevent diversion and locked when
necessary, in accordance with law and regulation.
– EP 6: the hospital prevents unauthorized individuals from obtaining medications in accordance with law
and regulation.
– EP 7: stored meds and components used are labeled with contents, expiration date and applicable
warnings.
FAQs published July 2010.
– EP 8: removes expired, damaged, and/or contaminated meds/stores separately.
© 2012 Joint Commission Resources
19 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
RC.02.03.07
Qualified staff receive and record verbal orders.
•
CoP Medical Records 482.24(c)(1)(i, ii, iii)
•
Allowance for partners to sign.
•
Problematic EP:
– EP 4: verbal orders are authenticated within the time frame defined by law and regulation.
MM.04.01.01
Medication orders are clear and accurate.
•
CoP Nursing Services 482.23(c)(2)
•
Problematic EPs:
– EP 13: the hospital implements its policies for medication orders.
– EP 7: the hospital reviews and updates preprinted order sheets within the time frames it identifies or
sooner if necessary based on current evidence and practice.
PC.01.03.01
The hospital plans the patient’s care.
•
Problematic EPs:
– EP 1: hospital plans the patient’s care based on needs identified by the patient’s assessment, reassessment,
and results.
– EP 2: written plan of care is based on patient’s goals and time frames required to meet goals.
– EP 22: based on goals established, staff evaluate patient progress.
– EP 23: revises plans and goals based on patient’s needs.
•
CoP 482.23(b)(4) Nursing Services
PC.01.02.07
The hospital assesses and manages the patient’s pain.
•
Problematic EPs:
– EP 1: conducts comprehensive pain assessment.
– EP 3: reassesses and responds to the patient’s pain based on its reassessment criteria.
– Consider that overmedicating is as much of a problem as undermedicating.
MS.01.01.01
Medical staff bylaws address self-governance and accountability to the governing body.
•
Problematic EPs:
– EP 3: the requirements in EPs 12-36 have been addressed.
– EP16: for deemed status—requirements for completing the H&P are in the bylaws (PC.01.02.03
EPs 4 and 5).
© 2012 Joint Commission Resources
20 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
PC.03.01.03
The hospital provides the patient with care before initiating operative or other high-risk procedures, including
those that require the administration of moderate or deep sedation or anesthesia.
•
Problematic EPs:
– EP 1: presedation/preanesthesia patient assessment.
– EP 8: immediate reassessment.
Medicare Conditions of Participation Final Rule
Medicare Final Rule
Revised hospital and critical access hospital requirements published May 16, 2012 in the Federal Register.
•
Effective July 16, 2012.
•
Interpretive Guidelines will be published when they have been completed.
•
Revisions to Joint Commission standards/EPs have been approved and are effective September 1, 2012.
Medicare CoP Changes
•
Now allows for a single Governing Body overseeing multiple hospitals in a multi-hospital system.
•
New requirement for one or more members of the medical staff to be included on the hospital’s
Governing Body.
•
Surveyors have stopped surveying for a single Governing Body for each CCN.
•
CMS instructed us not to survey for this as the requirement is still under review.
•
Role of other practitioners on the medical staff.
– Concept of medical staff broadened to include other practitioners.
– These practitioners can perform all functions within their scope of practice.
– Must still function under the rules of the medical staff.
•
No change to Joint Commission requirements or survey process.
•
Single medical staff required for each CCN.
– This is being challenged due to the language in the preamble of the proposed rule contradicting the final
rule language.
•
Joint Commission has been surveying for a single medical staff for each CCN for a few years.
– Ability for system MEC to continue if the meetings clearly address each facility (CCN) separately and the
minutes reflect the discussion and decisions for each CCN.
– Practitioners are privileged at each facility they practice at.
© 2012 Joint Commission Resources
21 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Medicare CoP Changes (cont.)
•
Reporting restraint-related deaths.
– For patient deaths that occur while a patient is in soft, two-point wrist restraints the hospital must record
these deaths in a log or other system within seven days and the log must be made available to CMS
immediately upon request.
•
Joint Commission will continue to survey for reporting restraint-related deaths to CMS but with this new
caveat.
– PC.03.05.19 EPs 1 and 2 revised and EP 3 added.
•
Medical Staff Leadership:
– Podiatrists are now allowed to be responsible for the organization and conduct of the medical staff.
•
Joint Commission now allows for podiatrists to lead the medical staff.
– LD.01.05.01 EP 7 has been revised.
•
Nursing Care Plan:
– Now allows for a stand alone nursing care plan or an interdisciplinary plan of care that addresses nursing
and other disciplines.
•
Joint Commission standards have allowed this practice for many years.
•
Administration of blood transfusions and intravenous medications:
– Eliminated the requirement for non-physician personnel to have special training in the administration of
blood products and IV medications.
•
The requirement at HR.01.02.01 EP 19 has been removed and surveyors instructed not to survey for this.
•
Administration of medications:
– Allows for the self-administration of medication.
•
CoPs now consistent with Joint Commission standards (MM.06.01.03).
•
Orders by other practitioners.
– Allows other practitioners, such as APRNs and PAs, to write orders for medications and for others to
administer the medications in accordance with state law and regulation.
•
No change to Joint Commission processes.
– PC.02.01.03 EP 1 has been modified.
•
Standing orders:
– Allows the use of nurse-initiated standing orders.
– Added requirement for medical staff, nursing, and pharmacy to approve written and electronic standing
orders, order sets, and protocols.
– Are to be based on nationally-recognized and evidence-based guidelines and recommendations.
– PI process for review of standing orders.
•
Joint Commission has been surveying to this level for several years.
– New EP has been developed: MM.04.01.01 EP 15.
© 2012 Joint Commission Resources
22 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Standing Orders/Protocols (cont.)
EP 15: For hospitals that use Joint Commission accreditation for deemed status purposes: Processes for the use
of pre-printed and electronic standing orders, order sets, and protocols for medication orders include the
following:
•
Review and approval of standing orders and protocols by the medical staff and the hospital’s nursing and
pharmacy leadership.
•
Evaluation of established standing orders and protocols for consistency with nationally recognized and
evidence-based guidelines.
•
Regular review of such standing orders and protocols by the medical staff and the hospital’s nursing and
pharmacy leadership to determine the continuing usefulness and safety of the standing orders and protocols.
•
Dating, timing, and authenticating of standing orders and protocols by the ordering practitioner or another
practitioner responsible for the patient’s care in accordance with professional standards of practice; law and
regulation; hospital policies; and medical staff bylaws, rules, and regulations.
Medicare CoP Changes (cont.)
•
Verbal orders:
– Removed the requirement for authentication within 48 hours.
– Authentication timeframe should be based on state law and regulation.
•
Surveyors will not be scoring authentication that has not occurred within 48 hours (unless required by state
law and reg).
– They will be asking about your policy.
– Recommend that your policy be based on state law and regulation.
– If your policy is more stringent than state law and regulation and surveyors find non compliance, you may
receive score at LD.04.01.07.
– RC.02.03.07 EP 4 has been revised.
•
Authentication of orders:
– Have made permanent the ability of another practitioner responsible for the care of the patient to
authenticate the verbal order of another practitioner.
•
No change to our survey process.
– RC.02.03.07 EP 4 has been revised to remove the “Notes.”
•
Infection Control Log
– Removed the requirement for an infection control log.
•
No change to our survey process.
•
Outpatient Services Director:
– Requirement for a single director of outpatient services has been removed.
•
Ours surveyors have not been surveying for this since publication of the rule.
– LD.04.01.05 EP 8 has been revised.
© 2012 Joint Commission Resources
23 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Medicare CoP Changes (cont.)
•
Critical Access Hospitals:
– Provision of services.
– Requirement that CAHs must directly furnish diagnostic and therapeutic services, laboratory services,
radiology services, and emergency procedures has been eliminated.
– They can be provided under arrangement.
•
LD.04.03.01 EPs 8, 9, 10, and 11 have been revised (see appendix).
•
Surveyors have been instructed.
•
Some minor editorial changes.
– Adding “quality assessment” to performance improvement to reflect CMS’ QAPI language.
©
© 2012 Joint Commission Resources
Copyright, The Joint Commission
24 of 40
The Official Newsletter of The Joint Commission
October 2012 Volume 32 Number 10
●
●
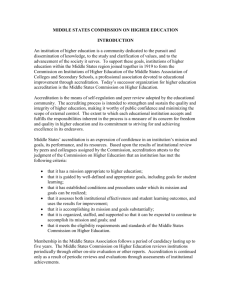
Top Standards Compliance
Issues for First Half of 2012
The Joint Commission has aggregated standards compliance data for accredited
organizations and certified programs surveyed or reviewed during the first half of
2012. These data help The Joint Commission recognize trends and tailor education
around challenging standards; National Patient Safety Goals (NPSGs); the
Universal Protocol for Preventing Wrong Site, Wrong Procedure, and Wrong
Person SurgeryTM; and Accreditation or Certification Participation Requirements
(APRs or CPRs). These data also help The Joint Commission identify risk areas to
highlight in the Focused Standards Assessment process (see the article on page 10 of
this issue).
The bar graphs on pages 14 to 19 identify, for each accreditation and certification program, the standards, NPSG and Universal Protocol requirements, and
APRs or CPRs identified most frequently as “not compliant” during surveys and
reviews from January 1, 2012, through June 30, 2012. While the text of the
requirement also appears in the bar graph, the full text of each (including elements
of performance and scoring information) is published in the applicable accreditation or certification manual.
The graphs display the 10 most frequently cited requirements in decreasing frequency for each program. The percentage shown at the beginning of each row represents the percentage (rounded to the nearest whole point) of organizations that
received Requirements for
Improvement (RFIs) for that particular
requirement. More than 10 standards
may be cited if two or more standards
in a program were tied in their percentage of RFIs.
Perspectives publishes these compliance data to allow accredited organizations and certified programs to evaluate
their own performance against that of
others. Organizations may also find
Continued on page 13
http://www.jointcommission.org
Contents
1
Top Standards Compliance
Issues for First Half of 2012
2
In Sight
3
4
4
6
8
ACCEPTED: Changes to
Requirements for Deemed
Status ASCs
ACCEPTED: New and
Revised Requirements to
Align with CMS CoPs
ACCEPTED: Changes to
Requirements for CA
Organizations Performing CT
Scans
The Joint Commission
Launches New
Comprehensive Stroke
Certification Program
APPROVED: Revised
Behavioral Health Care
Requirements to Eliminate
Redundancy
9
MAILED: Accreditation Manual
10
Joint Commission to Launch
New Intracycle Monitoring
Process
11
CLARIFICATIONS AND
EXPECTATIONS: Super Suites
Updates
Super Suites (continued)
Continued from page 12
According to the 2000 edition of the Life Safety Code, sleeping suites must not exceed 5,000 square feet in size. Later editions of the Life Safety Code allow them to be up to 7,500
square feet, provided that the area is protected by an approved
automatic sprinkler system and meets the requirements for separation between the suite and the corridor. The 2012 edition of
the Life Safety Code allows a size of up to 10,000 square feet for
sleeping suites, with certain provisions. If the building complies
with the requirements of later editions of the Life Safety Code,
the suite may be eligible for a traditional equivalency (pending
approval, including field verification from either a registered
architect, a fire protection professional, or the local fire marshal
responsible for the building’s fire safety).**
More Suite Advantages
Many believe that the greatest advantage of suites is that the
8-foot-wide space typically designated as an exit corridor is
instead designated as an intervening room. This intervening
room does not have the restrictions of a corridor. The doors
in this space are not corridor doors, because the space is not a
corridor. Those areas designated as hazardous, such as clean
or soiled utility rooms, must have doors with self-closing and
self-latching devices. Also, nonrated doors within the suite
are not required to have positive latches or be smoke resistant. The intervening room can be treated as circulating space,
which means that items can be placed in it as long as they do
not block egress or create a hazard if there are too many combustibles in the defined space.
Nonsleeping Suites
Nonsleeping suites might be found in the surgical depart** See last month’s column for more details on submitting a traditional
equivalency.
ment, laboratory, emergency department, and radiology
department. The boundaries are calculated the same for
sleeping and nonsleeping suites. Both types of suites must
have at least two separate and remote means of egress when
they exceed 2,500 square feet. The size of a nonsleeping suite
is limited to 10,000 square feet. In the suite, if travel distance
to an exit access door is 100 feet or less, one intervening
room is allowed. If the travel distance within the suite is less
than 50 feet to the exit access door, a second intervening
room is allowed.
The “Life Safety” Chapter and Suites
The Joint Commission’s “Life Safety” (LS) chapter requires
all organizations to keep their electronic Statement of
Conditions™ (E-SOC) current, including required Life
Safety Code drawings. In 2011, 52% of all Joint
Commission–accredited hospitals did not comply with
Standard LS.01.01.01, Element of Performance 2, because of
inaccurate Life Safety Code drawings, including the boundaries and suite sizes. The Life Safety Code drawings must
clearly display certain information, as shown in “What to
Include in Life Safety Code Drawings” on the preceding page.
The Joint Commission does not specify where Life Safety
Code drawings should be kept; however, the Basic Building
Information (BBI) in the E-SOC does require this information in the Additional Comments text field. Converting Life
Safety Code drawings to a Web-based system can provide significant support in maintaining current drawings as well as
size restrictions of suites.
This month’s column discusses the role of suites in fire safety.
Next month’s column will continue to focus on the importance of
maintaining various life safety features by discussing the documentation of compliance with important requirements. P
Top Standards Compliance Issues for First Half of 2012 (continued)
Continued from page 1
this information helpful in assessing their own compliance in
these areas and planning any necessary improvement efforts.
Remember: Surveyors review compliance with all standards in
an accreditation or certification manual. This list is provided
only to help organizations pinpoint potential trouble spots.
If you have questions about these requirements, please
review the Standards Frequently Asked Questions at
http://www.jointcommission.org
http://www.jointcommission.org/Standards/FAQs. Questions
not addressed on this site may be directed to the Standards
Interpretation Group through its online question form
(http://www.jointcommission.org/Standards/OnlineQuestion
Form) or by calling 630-792-5900. P
October 2012
Continued on page 14
The Joint Commission Perspectives
13
Top Standards Compliance Issues for First Half of 2012
Ambulatory Care
50% HR.02.01.03
The organization grants initial, renewed, or revised clinical privileges to individuals who are permitted by
law and the organization to practice independently.
39% MM.03.01.01
The organization safely stores medications.
34% IC.02.02.01
The organization reduces the risk of infections associated with medical equipment, devices, and supplies.
21% IC.01.03.01
The organization identifies risks for acquiring and transmitting infections.
21% EC.02.02.01
The organization manages risks related to hazardous materials and waste.
18% MM.01.02.01
The organization addresses the safe use of look-alike/sound-alike medications.
17% MM.01.01.03
The organization safely manages high-alert and hazardous medications.
16% NPSG.07.01.01
Comply with either the current Centers for Disease Control and Prevention (CDC) hand hygiene
guidelines or the current World Health Organization (WHO) hand hygiene guidelines.
16% EC.04.01.01
The organization collects information to monitor conditions in the environment.
15% UP.01.03.01
A time-out is performed before the procedure.
Top Standards Compliance Issues for First Half of 2012
Behavioral Health Care
34% CTS.03.01.03
The organization has a plan for care, treatment, or services that reflects the assessed needs, strengths,
preferences, and goals of the individual served.
20% HR.02.01.03
The organization assigns initial, renewed, or revised clinical responsibilities to staff who are permitted by
law and the organization to practice independently.
15% HR.01.02.05
The organization verifies staff qualifications.
15% EC.02.06.01
The organization establishes and maintains a safe, functional environment.
14% CTS.04.03.33
For organizations providing food services: The organization has a process for preparing and/or
distributing food and nutrition products.
14% HR.01.06.01
Staff are competent to perform their responsibilities.
13% CTS.02.01.05
The organization implements a written process requiring a physical health screening to determine the
individual’s need for a medical history and physical examination in [non–24-hour settings].
13% NPSG.15.01.01 Identify individuals at risk for suicide.
13% MM.03.01.01
The organization safely stores medications.
13% EC.02.01.05
For foster care: The agency places individuals in foster care in physically safe environments.
14
The Joint Commission Perspectives
October 2012
http://www.jointcommission.org
Top Standards Compliance Issues for First Half of 2012
Critical Access Hospitals
50% EC.02.03.05
The critical access hospital maintains fire safety equipment and fire safety building features.
45% LS.02.01.10
Building and fire protection features are designed and maintained to minimize the effects of fire, smoke,
and heat.
38% EC.02.05.01
The critical access hospital manages risks associated with its utility systems.
36% LS.02.01.20
The critical access hospital maintains the integrity of the means of egress.
31% EC.02.06.01
The critical access hospital establishes and maintains a safe, functional environment.
31% IC.02.02.01
The critical access hospital reduces the risk of infections associated with medical equipment, devices,
and supplies.
31% LS.02.01.35
The critical access hospital provides and maintains systems for extinguishing fires.
29% EC.02.05.07
The critical access hospital inspects, tests, and maintains emergency power systems.
29% LS.02.01.30
The critical access hospital provides and maintains building features to protect individuals from the
hazards of fire and smoke.
29% RC.01.01.01
The critical access hospital maintains complete and accurate medical records for each individual patient.
Top Standards Compliance Issues for First Half of 2012
Disease-Specific Care Certification
21% DSDF.2
The program develops a standardized process originating in clinical practice guidelines (CPGs) or evidencebased practice to deliver or facilitate the delivery of clinical care.
13% DSDF.3 The program is designed to meet the participant’s needs.
13% DSCT.5 The program initiates, maintains, and makes accessible a health or medical record for every participant.
9% DSSE.3 The program addresses participants’ education needs.
5% DSDF.1 Practitioners are qualified and competent.
5% DSPM.6 The program evaluates participant perception of the quality of care.
3% DSPR.1 The program defines its leadership roles.
2% DSCT.4
The program shares information with any relevant practitioner or setting about the participant’s disease or
condition across the continuum of care.
2% DSPM.3 The program maintains data quality and integrity.
2% DSPM.2 The program uses measurement data to evaluate processes and outcomes.
http://www.jointcommission.org
October 2012
The Joint Commission Perspectives
15
Top Standards Compliance Issues for First Half of 2012
Health Care Staffing Services Certification
10% HSHR.1 The HCSS firm confirms that a person’s qualifications are consistent with his or her assignment(s).
7% HSHR.6 The HCSS firm evaluates the performance of clinical staff.
6% HSLD.5 The services contracted for by the HCSS firm are provided to customers.
4% HSHR.3 The HCSS firm provides orientation to clinical staff regarding initial job training and information.
4% HSPM.4 The HCSS firm analyzes its data.
3% HSHR.4 The HCSS firm assesses and reassesses the competence of clinical staff and clinical staff supervisors.
2% CPR 5
The staffing firm submits performance measurement data to The Joint Commission on a routine basis.
2% HSLD.9 The HCSS firm addresses emergency management.
Note: The remaining standards for the Health Care Staffing Services Certification program had a noncompliance rate of less than
1% or were fully compliant during the first half of 2012.
Top Standards Compliance Issues for First Half of 2012
Home Care
36% PC.02.01.03
The organization provides care, treatment, or services in accordance with orders or prescriptions, as
required by law and regulation.
27% NPSG.07.01.01
Comply with either the current Centers for Disease Control and Prevention (CDC) hand hygiene
guidelines or the current World Health Organization (WHO) hand hygiene guidelines.
24% EM.03.01.03
The organization evaluates the effectiveness of its Emergency Operations Plan.
24% HR.01.06.01
Staff are competent to perform their responsibilities.
23% HR.01.02.05
The organization verifies staff qualifications.
20% RC.02.01.01
The patient record contains information that reflects the patient’s care, treatment, or services.
19% PI.02.01.01
The organization compiles and analyzes data.
17% PI.01.01.01
The organization collects data to monitor its performance.
17% PC.01.03.01
The organization plans the patient’s care.
16% IC.01.03.01
The organization identifies risks for acquiring and spreading infections.
16
The Joint Commission Perspectives
October 2012
http://www.jointcommission.org
Top Standards Compliance Issues for First Half of 2012
Hospitals
61% RC.01.01.01
The hospital maintains complete and accurate medical records for each individual patient.
52% LS.02.01.20
The hospital maintains the integrity of the means of egress.
47% LS.02.01.10
Building and fire protection features are designed and maintained to minimize the effects of fire, smoke,
and heat.
40% EC.02.03.05
The hospital maintains fire safety equipment and fire safety building features.
39% IC.02.02.01
The hospital reduces the risk of infections associated with medical equipment, devices, and supplies.
37% LS.02.01.30
The hospital provides and maintains building features to protect individuals from the hazards of fire and
smoke.
36% MM.03.01.01
The hospital safely stores medications.
34% LS.02.01.35
The hospital provides and maintains systems for extinguishing fires.
33% EC.02.06.01
The hospital establishes and maintains a safe, functional environment.
29% EC.02.02.01
The hospital manages risks related to hazardous materials and waste.
Top Standards Compliance Issues for First Half of 2012
Laboratory and Point-of-Care Testing
67% QSA.01.01.01
The laboratory participates in Centers for Medicare & Medicaid Services (CMS)–approved proficiency
testing programs for all regulated analytes.
38% HR.01.06.01
Staff are competent to perform their responsibilities.
35% QSA.02.03.01
The laboratory performs calibration verification.
35% DC.02.03.01
The laboratory report is complete and is in the patient’s clinical record.
26% QSA.01.02.01
The laboratory maintains records of its participation in a proficiency testing program.
25% QSA.02.04.01
The laboratory evaluates instrument-based testing with electronic or internal systems prior to using them
for routine quality control.
24% QSA.02.08.01
The laboratory performs correlations to evaluate the results of the same test performed with different
methodologies or instruments or at different locations.
23% TS.03.01.01
The organization uses standardized procedures for managing tissues.
20% WT.05.01.01
The organization maintains records for waived testing.
20% QSA.01.03.01
The laboratory has a process for handling and testing proficiency testing samples.
http://www.jointcommission.org
October 2012
The Joint Commission Perspectives
17
Top Standards Compliance Issues for First Half of 2012
Long Term Care
39% HR.02.01.04
The organization permits licensed independent practitioners to provide care, treatment, and services.
26% NPSG.07.01.01 Comply with either the current CDC hand hygiene guidelines or the current WHO hand hygiene guidelines.
24% WT.04.01.01
The organization performs quality control checks for waived testing on each procedure.
21% IM.02.02.01
The organization effectively manages the collection of health information.
18% PC.01.02.03
The organization assesses and reassesses the resident and his or her condition according to defined time frames.
16% PC.02.03.01
The organization provides resident education and training based on each resident’s needs and abilities.
15% EC.04.01.01
The organization collects information to monitor conditions in the environment.
14% MM.03.01.01
The organization safely stores medications.
14% WT.03.01.01
Staff and licensed independent practitioners performing waived tests are competent.
13% PC.01.02.07
The organization assesses and manages the resident’s pain.
13% PC.01.03.01
The organization plans the resident’s care.
13% RC.02.01.21
Clinical record documentation includes resident education.
Top Standards Compliance Issues for First Half of 2012
Medicare/Medicaid Certification–Based Long Term Care
44% HR.02.01.04
The organization permits licensed independent practitioners to provide care, treatment, and services.
26% WT.03.01.01
Staff and licensed independent practitioners performing waived tests are competent.
25% RC.02.01.21
Clinical record documentation includes resident education.
22% EM.03.01.01
The organization evaluates the effectiveness of its emergency management planning activities.
21% EC.04.01.01
The organization collects information to monitor conditions in the environment.
21% IM.02.02.01
The organization effectively manages the collection of health information.
16% LD.04.04.05
The organization has an organization-wide, integrated resident safety program.
15% NPSG.07.01.01
Comply with either the current Centers for Disease Control and Prevention (CDC) hand hygiene
guidelines or the current World Health Organization (WHO) hand hygiene guidelines.
14% HR.02.02.01
The organization provides orientation to licensed independent practitioners.
14% PC.01.02.07
The organization assesses and manages the resident’s pain.
18
The Joint Commission Perspectives
October 2012
http://www.jointcommission.org
Top Standards Compliance Issues for First Half of 2012
Office-Based Surgery Practices
45% HR.02.01.03
The practice grants initial, renewed, or revised clinical privileges to individuals who are permitted by law
and the organization to practice independently.
31% IC.02.02.01
The practice reduces the risk of infections associated with medical equipment, devices, and supplies.
24% MM.03.01.01
The practice safely stores medications.
14% IC.01.03.01
The practice identifies risks for acquiring and transmitting infections.
14% NPSG.07.01.01
Comply with either the current Centers for Disease Control and Prevention (CDC) hand hygiene
guidelines or the current World Health Organization (WHO) hand hygiene guidelines.
13% PI.02.01.01
The practice compiles and analyzes data.
13% WT.05.01.01
The practice maintains records for waived testing.
10% HR.01.02.05
The practice verifies staff qualifications.
10% HR.01.06.01
Staff are competent to perform their responsibilities.
10% NPSG.03.04.01
Label all medications, medication containers, and other solutions on and off the sterile field in
perioperative and other procedural settings.
Top Standards Compliance Issues for First Half of 2012
Advanced Certification for Palliative Care
60% PCPC.4 The interdisciplinary program team assesses and reassesses the patient’s needs.
13% PCPC.5 The program provides care, treatment, and services according to the plan of care.
13% PCPI.2 The program collects data to monitor its performance.
7% PCPC.3 The program tailors care, treatment, and services to meet the patient’s lifestyle, needs, and values.
7% PCPI.3 The program analyzes and uses its data.
7% PCPM.6 Program leaders are responsible for selecting, orienting, educating, retaining, and providing incentives for staff.
7% PCPM.7
The program has an interdisciplinary team which includes individuals with expertise in and/or knowledge about
the program’s specialized care, treatment, and services.
Note: The remaining standards for the Advanced Certification for Palliative Care program were in full compliance during the first
half of 2012.
http://www.jointcommission.org
October 2012
The Joint Commission Perspectives
19
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix A: Faculty Biographies
NOTE: These presenters do not have any financial arrangements or affiliations with corporate organizations that
either provide educational grants to this program or may be referenced in this activity. These presenters
have also attested that their discussions will not include any unapproved or off-label use of products.
Patricia Adamski, RN, MS, MBA
Director of Standards Interpretation
Division of Healthcare Improvement
The Joint Commission
As Director of Standards Interpretation, Ms. Adamski is responsible for operational oversight for the standards
interpretation functions, including: Periodic Performance Review process, response to over 40,000 inquiries per
year, review of survey reports and post survey processes, and support of the surveyor cadre. Prior to assuming
her director responsibilities, Ms. Adamski was the Senior Associate Director of the Standards Interpretation
Group. Ms. Adamski serves as faculty for surveyor and other educational programs and is a certified nurse
surveyor in the Hospital program.
Prior to joining The Joint Commission, Ms. Adamski held various positions in the Chicago area including most
recently the Director of Professional Development, Administrative and Support Services, and Privacy Officer at
Elmhurst Memorial Hospital. She is affiliated with the American Organization of Nurse Executives (AONE),
and the American College of Healthcare Executives (ACHE). Ms. Adamski has over 35 years of healthcare
management and nursing experience in the acute care setting and an extensive background in oncology nursing
and pain management.
Ms. Adamski received a diploma from Wesley-Passavant School of Nursing in Chicago, Illinois. She also
received her Bachelor of Science and Master of Science degrees in Nursing and a Master of Business
Administration degree from St. Xavier University in Chicago, Illinois.
© 2012 Joint Commission Resources
33 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Barbara Buturusis, RN, MSN
Director of Survey Management and Support
Accreditation and Certification Operations
The Joint Commission
Ms. Buturusis is The Joint Commission's Director of Survey Management and Support. In this role, she oversees
the activities of the accreditation and certification field directors and over 500 field staff. Ms. Buturusis also
oversees orientation and education for the Division of Accreditation and Certification Operation, Intracycle
Monitoring, Survey Technology, and Divisional Operations Excellence.
Previously, Ms. Buturusis worked for Loyola University Medical Center as the Executive Director of Cancer
Services responsible for inpatient, outpatient, cancer programs, and medical affiliations with community
providers. She also oversaw the Neurosciences Service Line including Neurodiagnostics, Intraoperative
Neuromonitoring, Audiology, Epilepsy Monitoring, inpatient neuroscience units, and the Primary Stroke Center.
She has experience in implementation of the electronic medical record (EMR) for oncology inpatient and
outpatient care. At Loyola, Ms. Buturusis also oversaw home care, hospice, academic ambulatory practices,
outpatient rehabilitation services, and cardiac rehabilitation.
Ms. Buturusis worked for Ernst and Young LLP in their Health Care Transformation practice working on
national engagements for post merger integration, strategic repositioning, and system redesign. She has worked
at Children's Memorial Hospital and in the home care, hospice, and community hospital setting in critical care,
ambulatory surgery, and ambulatory care settings.
Ms. Buturusis has a Master, Bachelor, and Associate Degree in Nursing. She has a certificate in Health Care
Leadership from the Harvard School of Public Health and is a member of Sigma Theta Tau, the national honor
society for nurses.
Judy Homa-Lowry, RN, MS, CPHQ
Consultant
Joint Commission Resources, Inc.
As a Consultant for Joint Commission Resources, Ms. Homa-Lowry has extensive experience consulting with
hospital administrative and medical staffs to improve quality systems and patient care outcomes. Ms. HomaLowry performs JCR operational assessments for acute care, critical access hospitals, behavioral health,
long-term care, home health, and hospital-owned ambulatory clinics. She also designs systems and processes for
healthcare organizations to improve clinical operations and financial outcomes.
Ms. Homa-Lowry has an extensive background in healthcare data and analysis. She worked for a healthcare
database company for approximately seven years where she was responsible for product development,
consulting, and account management. She has held quality positions in healthcare organizations. She also has
consulted and has experience in utilization management, case management, and risk management.
Ms. Homa-Lowry is the past President of the National Association for Healthcare Quality. She also served on the
Board of the International Society for Quality Health Care, Inc. She was President of the Michigan Association
for Healthcare Quality for two terms. She served as the Chairman of the Healthcare Education Foundation for the
National Association for Healthcare Quality. She also served on a Quality and Utilization Committee for the
American Hospital Association.
Ms. Homa-Lowry has published several articles and book chapters related to quality improvement. She is a
member of a number of healthcare professional organizations, including the American Society for Quality. She is
a member of the editorial review board for Hospital Peer Review, Healthcare Benchmarks and Quality
Improvement, and Hospital Case Management. She is certified in Health Care Quality and the Systems
Approach to Quality. She is an RN and obtained her MS in Business Administration with a major in quality and
operations management from Madonna University. She was also a Malcolm Baldridge Examiner for three years.
© 2012 Joint Commission Resources
34 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix B: Post-Test
Changes for 2013: Standards and Survey Process
To be eligible for CE credit, you MUST view the video presentation and read the Resource Guide first. Then
complete the post-test at http://twnlms.com/ by the due date listed online.
1. One of The Joint Commission's enablers for improving healthcare outcomes is _____.
a. HAI portal
b. core measures
c. leading practices library
d. All of the above.
2. According to the AHRQ definition, a Medical Home is not simply a place, but a model of primary care.
a. True
b. False
3. The Joint Commission is piloting a linking of Joint Commission accreditation and _____.
a. OSHA compliance
b. ISO certification
c. state regulation
d. NFPA certification
4. Touch Point 2 occurs _____ to _____ months after the triennial survey in the Intracycle Monitoring process.
a. 10; 12
b. 12; 18
c. 18; 24
d. 24; 30
5. One of the goals of the Intracycle Monitoring Process is to identify and proactively manage risk.
a. True
b. False
6. For standard RC.01.01.01 - the hospital maintains complete and accurate medical records for each
individual patient - problematic EP 19 requires that all entries are _____.
a. dated
b. signed
c. timed
d. None of the above.
7. Which Joint Commission Standard requires that hospitals reduce the risk of infections associated with
medical equipment, devices, and supplies?
a. IC.01.01.01
b. IC.01.01.02
c. IC.02.01.02
d. IC.02.02.01
8. The Joint Commission's NPSG.07.06.01 relating to catheter-associated urinary tract infections has been
eliminated.
a. True
b. False
© 2012 Joint Commission Resources
35 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
9. Which Joint Commission Standard requires that hospitals safely store medications?
a. PC.03.01.01
b. PC.03.03.03
c. MM.03.01.01
d. MM.03.03.03
10. Revisions to Leadership Standard LD.04.03.11, which are effective in 2013, relate to _____.
a. medical staff relations
b. patient flow
c. credentialing and privileging
d. None of the above.
© 2012 Joint Commission Resources
36 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix C: Resources and Related Information
Electronic Resources
The Joint Commission: http://www.jointcommission.org
Joint Commission Resources: http://www.jcrinc.com/
NOTE: The Internet is an ever-evolving environment and links are subject to change without notice.
© 2012 Joint Commission Resources
37 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix D: Continuing Education Credit Information
Accreditation Council for Continuing Medical Education
Joint Commission Resources (JCR) is accredited by the Accreditation Council for Continuing Medical
Education to provide continuing medical education for physicians. JCR takes responsibility for the content,
quality, and scientific integrity of this CME activity. JCR designates this educational activity for the listed
contact hours of AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with
the extent of their participation in the activity.
American Nurses Credentialing Center's Commission on Accreditation
JCR is also accredited as a provider of continuing nursing education by the American Nurses Credentialing
Center's Commission on Accreditation. JCR designates this continuing nursing education activity for the listed
contact hours.
JCR is a provider approved by the California Board of Registered Nursing, provider number CEP 6381 for the
listed contact hours.
American College of Healthcare Executives
Joint Commission Resources is authorized to award the listed contact hours of pre-approved ACHE Qualified
Education credit for this program toward advancement, or re-certification in the American College of Healthcare
Executives. Participants in this program wishing to have the continuing education hours applied toward ACHE
Qualified Education credit should indicate their attendance when submitting application to the American College
of Healthcare Executives for advancement or re-certification.
National Association for Healthcare Quality
This activity has been approved by the National Association for Healthcare Quality (NAHQ) for 1.0 Certified
Professional Healthcare Quality (CPHQ) CE credit.
Successful completion of this CE activity includes the following:
• View the presentation and read the accompanying Resource Guide.
• Complete the online Evaluation Form and Post Test.
• A CE certificate/statement of credit can be printed online following successful completion of the Post Test
and the Evaluation Form.
NOTE: This information applies to The Joint Commission Resources Quality & Safety Network program titled,
Changes for 2013: Standards and Survey Process, originally presented on Thursday, December 20, 2012
from 2:00 - 3:00 p.m. ET.
There is no individual participant fee for this educational activity.
© 2012 Joint Commission Resources
38 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix E: Discipline Codes: Instructions
Some of our programs are accredited for more than one discipline. To ensure that we issue each participant a certificate by
the appropriate accrediting body, we ask that you supply us with the following information:
1. The two-digit discipline code
2. Followed by the position code
Example: For a medical doctor, use: 10 MD
Discipline
Physician
(CME)
Discipline Position
Code
Code
10
MD
MDFP
12
MD-Psychiatrist
MD-Public Health Certificate
MDPP
MD-Public Psychiatry Certificate
MDAC
MD-Area Clinical Needs
Dietary
Dietary
Manager
Counseling
Laboratory
Physical
Therapy
Occupational
Therapy
13
14
15
16
17
18
Respiratory
Therapy
Medical
Records
Discipline Position
Code
Code
20
21
RT
Position
Respiratory Therapist, Registered
RTC
Respiratory Therapist, Certified
RPNC
Resp. Practitioner, Non-Critical
Care
RPCC
Resp. Practitioner, Critical Care
RHA
Health Information Administrator
RHT
Health Information Technician
MD-Medical Faculty Certificate
CCS
Coding Specialist
MD-Medical Staff Physician
CCP
Coding Specialist, Physician-Based
Radiologic Technologist
MD-Limited License
Radiology
22
RAD
DO
Doctor of Osteopathy
Sonography
23
MS
Medical Sonographer
PHA
Physician Assistant
24
AT
Athletic Trainer
DDS
Doctor of Dental Science
Athletic
Training
HC Quality
25
HQP
Healthcare Quality Professional
Activity
Professional
26
ADP
Profession Activity Director
ADC
Activity Director
AAC
Activity Assistant
OP
Other Medical Professional
HA
Hospital Administrator
LTC Administrator
OA
Other Administrator
PH
Pharmacist (PharmD)
PHN
Pharmacist, Nuclear
PHC
Pharmacist, Consultant
PA
Pharmacy Technician
RD
Registered Dietitian/Nutritionist
NC
Nutrition Counselor
DTR
Dietetic Technician
DOD
MHC
Dietary Manager
Mental Health Counselor,
Licensed
ACC
Nurse
(CNE)
30
RN
ARNP
NP
Psychology
33
Activity Consultant
Registered Nurse
Advanced RN Practitioner
Nurse Practitioner
LPN
Licensed Practical Nurse (or LVN)
ON
Other Nursing Professional
PSY
Psychologist (non-MD)
PSYL
Psychologist, Limited License
Case Mgmt
35
CCM
Certified Case Manager
Nursing
Assistant
45
CNA
Certified Nursing Assistant
SW
Social Worker, Licensed
RA
Restorative Care Aide
OCT
Other Counselor/Therapist
HSA
Health Support Aide
MFT
Marriage/Family Therapist,
Licensed
Laboratory Technologist/
Professional
NA
LTG
LT
Laboratory Technician
LS
Laboratory Supervisor
LD
Laboratory Director
PT
Physical Therapist
PTA
19
Discipline
MDLL
ADM
Pharmacy
MD-Family Practice
MDPS
MSP
Administration
Medical Doctor
MDPH
MDMF
40
Position
OT
OTA
© 2012 Joint Commission Resources
Physical Therapy Assistant
Occupational Therapist
Occupational Therapy Assistant
Emergency
Medical
Services
46
Nursing Technician
CFR
First Responder
EMTB
EMT, Basic Level/EMT1
EMTI
EMT, Intermediate
Level/EMT2/EMT3
EMTP
EMT, Paramedic Level/EMT4
OTH
Health Unit
Coor
Other
Nurse Aide, Non-certified
NT
55
CHUC
27
OTH
Other
Health Unit Coordinator, Certified
Other
39 of 40
Joint Commission Resources
Changes for 2013: Standards and Survey Process
Appendix F: JCR Quality & Safety Network Contact Information
General information, customer service issues, or program reception problems?
If you have questions or need technical assistance,
please contact the JCRQSN Customer Service Team
via e-mail at support@jcrqsn.com or call toll-free
1-888-219-4678
To provide feedback or comment on JCRQSN educational programming
Please contact:
George Riccio
Associate Director of Video and Satellite Service
Joint Commission Resources
630-792-5428
Continuing education questions?
Please contact:
JCRQSN Continuing Education Support Team
support@jcrqsn.com
1-888-219-4678
Questions about standards?
Standards Interpretation Group
630-792-5900
Questions about JCR education or other resources?
JCR Customer Service Center
877-223-6866
VA Knowledge Network Questions?
Contact Lloyd Parish
© 2012 Joint Commission Resources
562-826-5505, extension 3856
40 of 40