Objectives 35
advertisement

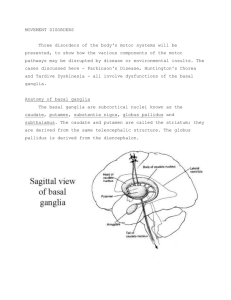
BASAL GANGLIA - major component of motor system; relationship to movement; Parkinson, Huntington’s disease 1. Basal ganglia structures include: Caudate nucleus Putamen Globus Pallidus (pallidum) – external segment (GPe) and internal segment (GPi) - Putamen and globus pallidus make up lenticular nucleus Substantia Nigra Subthalamic nucleus Nucleus Accumbens –related to caudate and putamen - caudate nucleus, putamen, and nucleus accumbens have similar but parallel connections striatum; internal capsule grows between these structures leaving bridges of gray matter - putamen and globus pallidus have different connections, but are physically attached 2. General connections - basal ganglia have few projections downstream to brainstem and spinal cord - instead, they affect movement by modulating cortical functions - input portion is striatum; output portion is globus pallidus - major direct circuit through basal ganglia involves a loop that starts in large areas of the cerebral cortex projects to striatum projects to globus pallidus output travels through lenticular fasciculus and ansa lenticularis to thalamus projection back to cerebral cortex - the above pathway is mostly uncrossed so damage on one side causes a movement problem on contralateral side of body Physiological effects of connections - striatum sends inhibitory (GABA) fibers to globus pallidus (GPe and GPi); GPi forms output from basal ganglia to ventrolateral thalamus (VL) and is inhibitory -when globus pallidus is excited, it generates more inhibition of the thalamus and less excitation of thalamocortical targets - when globus pallidus is inhibited, thalamus is less inhibited more excitation to thalamocortical targets - this can ultimately select a particular motor behavior out of a multitude of choices 3. Identify: head, body and tail of caudate nucleus, putamen, nucleus accumbens, globus pallidus (GPe and GPi), subthalamic nucleus, substantia nigra (reticular and compact) parts, ansa lenticularis, lenticular fasciculus, thalamic fasciculus 4. Substantia nigra -substantia nigra is like two separate neural structures laminated together - Reticular part (SNr) is adjacent to the cerebral peduncle and does not contain pigmented dopaminergic neurons; instead it contains GABAergic neurons to thalamus and is connected up like a displaced piece of globus pallidus - Compact part (SNc) contained pigmented neurons project to striatum release dopamine and modulate level of excitability of both direct and indirect pathways; reduction of dopamine levels decreases activity in direct pathway and increases activity indirect pathway both result in increased pallidal inhibition of thalamus - Striatum to reticular part is inhibitory 5 Subthalamic nucleus (indirect pathway) - subthalamic nucleus gets inputs from external segment of globus pallidus and sends excitatory (glutamate) projections to internal segment of globus pallidus (indirect path through basal ganglia) - fibers interconnecting subthalamic nucleus and globus pallidus pass across internal capsule called subthalamic fasciculus - activating subthalamic nucleus more inhibition of thalamus by globus pallidus; damaging subthalamic nucleus results in less of this inhibition - Globus pallidus to subthalamic nucleus is inhibitory 6. Parallel pathways in basal ganglia - motor loop that uses putamen as input to the basal ganglia and not the caudate nucleus - somatosensory and motor areas of cortex project to the putamen projects to globus pallidus projects to thalamus output to supplementary motor areas projects to motor cortex; motor programs selected by basal ganglia and relayed to motor cortex for elaboration and execution - loop involved in cognition uses caudate nucleus as input to basal ganglia - association areas of cerebral cortex project to caudate nucleus project to globus pallidus projects to thalamus project to prefrontal association areas; this loop mediates ideation of the desired movement (integrates motivation and ideas about responses) - all basal ganglia disorders affect cognitive or emotion function to varying degrees; depression, dementia (Huntington’s) and cognitive changes (Parkinson’s) - a limbic loop exists through basal ganglia; limbic structures project to ventral part of striatum where head of caudate and putamen merge with each other nucleus accumbens projects to globus pallidus underneath anterior commissure (ventral pallidum) projects to thalamus Chemical anatomy of basal ganglia - NTs in basal ganglia include dopamine, GABA, and Ach; pharmacological treatments for disorders of basal ganglia - many neurons have peptide NTs that are co-localized with those mentioned above - Dopamine from SNc is 1) inhibitory on striatal neurons of indirect pathway and 2) excitatory on striatal neurons in direct pathway - output neurons of striatum are inhibitory on neurons of globus pallidus (GPe and GPi) via GABA - Subthalamic neurons are excitatory on globus pallidus internal neurons via glutamate - Globus pallidus internal neurons are inhibitory on thalamic neurons 7. Disorders - positive signs include involuntary muscle contractions in various patterns - negative signs include lack of muscle contraction - Parkinson’s: positive signs include resting tremor in hands and increase in muscle tone (rigidity); negative signs include slow movements (bradykinesia) an few movements (hypokinesia); strength or reflex unchanged; differs from spasticity, increased reflexes caused by UMN damage - Three categories of involuntary movements associated with basal ganglia disorders: rapid movements called chorea, slow, writhing movements called athetosis, and flailing movements of entire limb called ballism Hypokinetic disorders – destruction of substantia nigra compact part - Dopamine loss decrease in excitatory drive onto striatal output neurons in direct pathway decreased inhibition of globus pallidus increased globus pallidus activity increased inhibition of thalamic neurons reduced drive onto motor cortex neurons - Dopamine loss loss of inhibition on striatal neurons in indirect pathway increased activity of striatal neurons increase inhibition of neurons in GPe decreased GPe activity decreased inhibition and increased activity in subthalamic nucleus increase excitatory drive on neurons of GPi - net effect of dopamine loss associated with Parkinson’s disease is increased neuronal activity in GPi (direct and indirect) increased inhibition of thalamus decreased drive to motor cortex loss or slowing of movement Hyperkinetic disorders - decreased activity in GPi - lesions in striatum or subthalamic nucleus - loss of striatal neurons in direct pathway decreased inhibition and increased activity on GPi hypokinetic syndrome - destruction of striatal neurons into indirect pathway loss of inhibitory input to GPe (increased activity) increased inhibition of and decreased activity in subthalamic nucleus decrease drive onto GPi neurons decreased inhibition of and increased activity in thalamus neurons increase activity to motor cortex increased involuntary movements (hyperkinetic) -lesions of subthalamic nucleus cause involuntary movements termed ballismus – brisk ballistic limb movement