New Developments in PSA Testing:
The Importance of the Median PSA Level
Key Points
• Most patients with Ca prostate have PSA
levels within the reference interval or RI
(normal range).
• The Median PSA level (rather than the PSA
reference interval) is useful for the sensitive
detection of Ca prostate.
• Free PSA testing reduces the false positive
rate in patients with PSA above the median
but below 10ug/L.
• Recent Medicare changes reflect these
findings.
C
linicians have been aware for some time that a
significant proportion of patients with PSA within
the “normal” reference range may, in fact, have
early prostate cancer or are at high risk of developing prostate
cancer. For example, only 20% of all patients with prostate
cancer will be detected, if a PSA cut-off of 4 ng/L is used1. Put
another way, 80% of patients with prostate cancer will have
a PSA of less than or equal to 4 ng/L and the higher the PSA
level within this “normal” range, the higher the risk of cancer.
About 15% of patients over 60 years old with PSA of less than
4 ng/L have Ca prostate.2
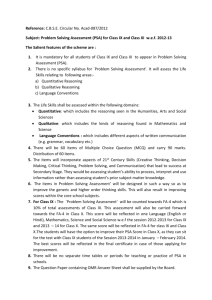
The distribution of PSA levels in the population is skewed
with the median value (value that separates the upper from
the lower 50% of values) being surprisingly low relative to the
upper reference limit; for example for males aged 55-60 years
the reference interval is 0.3-3.5 ug/L but the median is only
1.1 ug/L. This age-appropriate median is an effective tool to
separate patients with “normal” PSA values into low risk and
higher risk categories.
Diagram 1 shows the distribution of PSA results in healthy
males aged 55-60 years and illustrates this phenomenon.
Long term prospective follow-up of patients with “normal”
PSA levels has shown that the relative risk of having cancer
diagnosed is about 10 times higher (in men aged 50-59) if PSA
was within the RI but above the median than in those where
PSA was below the median.3 A low percentage free/total PSA,
which is an independent risk predictor of malignancy, is useful
to further risk stratify this second group of patients. Patients
with a PSA that falls above the age-related median should thus
be followed up more frequently with repeat PSA testing and
%free/total PSA measurement to increase sensitivity
and specificity of PSA testing.
The recent Medicare rule changes to PSA testing (below)
reflect these findings, and Clinipath Pathology is now routinely
reporting the age and method specific median PSA level
on PSA reports when the PSA falls within the age-related
reference interval.
Page 1 of 2
Diagram 1. PSA Distribution for 55-60 years
Men aged
55-60
years
Low
Risk
0.3
Higher
Risk
1.1
3.5
Median
PSA reference interval for 55-60 year age group
Medicare Changes to PSA Testing
As of 1st May 2009, new conditions apply in the Medicare
Benefits Schedule to the measurement of free PSA.
The changes that have been made are as follows:
• Amendment of the Medicare item (66659): The amended
version of the item allows a measurement of free PSA to be
performed if the total PSA value is above the age-related
median and below, or equal to, the age-related upper
reference limit – 1 episode in a 12 month period.
• A new Medicare item (66660), allowing up to 4 episodes of
testing for free PSA in a 12 month period, if the total PSA is
above the age-related upper reference limit, but below 10 ug/L.
Who Qualifies for Medicare Funded
% Free/Total PSA Testing?
A patient who is not known to have prostatic cancer and
whose total PSA is above the median and less than 10 ug/L,
is eligible for measurement of % free/total PSA.
How To Request % Free/Total PSA
To obtain a valid measurement of the free PSA, it is
important to ensure that a patient’s specimen is analysed
without delay (within 24 hours), otherwise collection of a further
specimen is necessary.
To avoid the need for a recollect, we suggest you request
“Total PSA” together with “Free PSA if indicated”. We will
perform the free PSA provided the patient is eligible by
Medicare rules.
Laboratory Testing and Reporting of Results
With the Medicare changes, Clinipath Pathology has
developed protocols to enhance testing and reporting of PSA
that include the following:
• We will specify the method (Abbott Architect®) used in our
laboratory for PSA and %free/total PSA measurement.
This is because different methods may give different
results on the same patient.
New Developments in PSA Testing:
The Importance of the Median PSA Level continued
Laboratory Testing and Reporting of Results
continued
• Reporting of total PSA results will be to 2 decimal places
below 1 ug/L e.g. 0.16 ug/L and to 2 significant figures for
results at or above 1 ug/L e.g. 9.9 ug/L.
• Ultra-sensitive PSA (down to 0.01ug/L) will be available on
request for early detection of recurrence of prostatic cancer.
• The previous age-related reference limits, which were based
on overseas data with 10-year increments, will be replaced
with method specific age-related reference limits, derived
from an extensive analysis of Australian population data.
This will enable 5-year increments to be used for men in the
40 to 79 year age group (see Table 1).
• An age-related median value will be provided for patients
whose total PSA level falls within their age related reference
interval (see Table 1).
• In terms of the %free/total PSA, a method-specific (Abbott
Architect®) reference interval of 10-60% and a median value
of 25% will be applied to all age groups tested.
• A range of new interpretative comments will be added to
reports, concerning the patient’s risk of prostatic cancer with
suggested follow-up depending on the total and % free/total
PSA values obtained.
• PSA measurement will utilise ‘delta checking’ whereby
repeat specimen testing is performed if there is a marked
difference noted between successive PSA results.
• Although a free PSA may be requested, it will not be
measured and reported routinely if the patient has a history
of (treated) prostatic neoplasia or if the total PSA is at or
below the age-related median level, or greater than or equal
to 10 ug/L (as Medicare does not fund these situations).
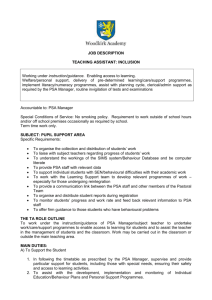
Age-Related Reference Limits and Median
Values for Total PSA
The age-related reference limits and median values that
apply to total PSA testing of Australian men using the Abbott
Architect® method are as follows:
Table 1.
Age (yrs)
Reference (ug/L)
Median (ug/L)
20 - 29
0.20 - 2.0
0.70
30 - 39
0.20 - 2.1
0.75
40 - 44
0.25 - 2.2
0.80
45 - 49
0.25 - 2.5
0.85
50 - 54
0.25 - 3.0
0.95
55 - 59
0.30 - 3.5
1.1
60 - 64
0.30 - 4.5
1.2
65 - 69
0.30 - 5.5
1.3
70 - 74
0.30 - 6.5
1.4
75 - 79
0.30 - 7.5
1.5
80+
0.25 - 9.0
1.6
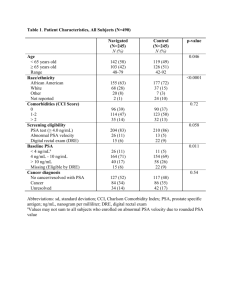
Whether to Screen Using PSA or not
Ultimately the value of screening is determined not by the
percentage of tumours detected, but by the improvement in
patient outcomes that screening delivers. This is of course an
entirely different issue to the one I have discussed in the above
article and may now have been answered by the European
Randomised Study of Screening for Prostate Cancer 4. This trial
which followed over 160,000 men found that there was a small
absolute reduction of 0.7 prostate cancer deaths per 1000 men
screened over 9 years, but at the cost of substantial increased
morbidity from biopsies and subsequent surgery. The decision
as to whether or not to screen remains a difficult one for both
doctors and patients.
References
1. Thompson, JAMA 2005;294:66-70
2. Thompson, N Engl J Med
2004;350:2239-46
3. Loeb, Urology 2006 Feb;67(2):316-20
4. Schroder NEJM 2009;360: 1320-1328
Dr Sydney Sacks
Chemical Pathologist
T:9476 5211
E: ssacks@clinipath.net
Page 2 of 2
 0
0