Hepatic Intra arterial Brachytherapy Pre Procedure
advertisement

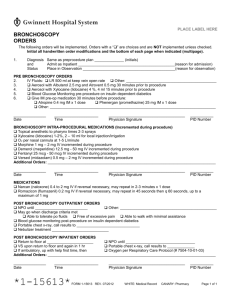
PLACE LABEL HERE HEPATIC INTRA-ARTERIAL BRACHYTHERAPY PRE-PROCEDURE ORDERS The following orders will be implemented. Orders with a “” are choices and are NOT implemented unless checked. Initial all handwritten order modifications and the bottom of each page when indicated (multipage). 1. Diagnosis Admit as Inpatient _____________________________________(reason for admission) and Status: Place in Outpatient ______________________________________________(diagnosis) 2. Unit: ICU IMCU/PCU Telemetry Floor Any Floor Telemetry Any Floor (No Telemetry) 3. Allergies: __________________________________________________________________________ If patient is allergic to contrast, notify the radiologist for possible pre-treatment orders. Radiologist will need to know the type of reaction, previous treatment, test that induced reaction and approximate date of last reaction. 4. Diet: 5. Insert Foley catheter; bedside gravity drainage 6. CBC, CMP, PT, PTT on chart (within 2 weeks) 7. Clip hair from both groins to midline of abdomen 8. Baseline vital signs: Temperature, pulse, respirations, BP and pulse oximeter 9. IV Fluids: NPO after 12 MN, except for AM medications NPO 4 hrs prior to procedure D5 ½ NS at __________ ml/hr ½ NS at __________ ml/hr (diabetic patients) Pepcid (famotidine) 20 mg po x 1 dose pre-procedure Other: _________________________________________ 10. Gastrointestinal prophylaxis: 11. Antiemetics: 12. Antibiotics (30 min prior to procedure): Rocephin (ceftriaxone) 1gm IVPB x 1 dose or Penicillin AND Cephalosporin allergic patients: Cipro 400 mg IV x 1 dose or Other: __________________________________________________________________ Zofran (ondansetron) 16 mg IV x 1 dose 30 min prior to procedure Other: ____________________________________________________________ ADDITIONAL ORDERS: ______________________________________________________________________________________ ______________________________________________________________________________________ ______________ Date ___________________ Time _________________________________ Physician Signature __________ PID Number Send copy to pharmacy *1-16243* FORM 1-16243 REV. 07/2012 Page 1 of 1