1017 - South West Yorkshire Partnership NHS Foundation Trust
advertisement

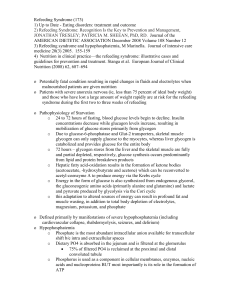
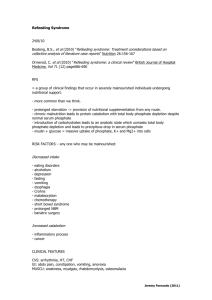
Information sheet for medical staff working on in-patient units to be used for service users at risk of Refeeding Syndrome, summarised from NICE Guidelines (CG32, 6.6) 1. What is Refeeding Syndrome? Refeeding syndrome is not a singular condition but a group of clinical symptoms and signs that can occur in the malnourished or starved individual upon the reintroduction of nutrition. In this service user group, over-rapid and unbalanced provision of oral, enteral or parenteral nutrition can result in shifts in fluid and electrolytes. These biochemical abnormalities can result in a spectrum of presentations from fluid retention to cardiac arrhythmias, respiratory insufficiency and ultimately death. 2. Who may develop Refeeding Syndrome? Criteria for determining a service users level of refeeding risk: AT RISK: - Any service user who has eaten very little or nothing for more than 5 days. Biochemical monitoring is recommended on day 3 of increased dietary intake. AT HIGH RISK: Any service user who has one or more of the following: - BMI less than 16kg/m2. - Unintentional weight loss greater than 15% within the last 3-6 months. - Little or no nutritional intake for more than 10 days. - Low levels of potassium, phosphate or magnesium prior to feeding. Or any service user who has two or more of the following: - BMI less than 18.5kg/m2. - Unintentional weight loss greater than 10% within the last 3-6 months. - Little or no nutritional intake for more than 5 days. - A history of alcohol abuse or drugs including insulin, chemotherapy, antacids or diuretics. It is recommended to follow biochemical and prescription advice as detailed in points 3 and 4 stated below. AT EXTREMELY HIGH RISK: - - Any service user who has a BMI of less than 14kg/m 2. Any service user who has had a negligible intake for more than 15 days. It is recommended that these service users are transferred to the local acute hospital for continuous monitoring of cardiac rhythm during feeding. This advice also applies to any other service users who are at risk of refeeding syndrome who already have or develop any cardiac arrhythmias. Date Produced: January 2013 3. What should be prescribed for those at high risk of Refeeding Syndrome? Additional vitamin supplementation should be provided immediately before and during the first 10 days of feeding: - Oral Thiamine 200 – 300mg daily. - Vitamin B Compound Strong 1 or 2 tablets three times a day (or full dose daily intravenous vitamin B preparation, if necessary). - A balanced multi vitamin and trace element supplement once daily. 4. What should be monitored in those at high risk of Refeeding Syndrome? As a service user undergoes refeeding there is a switch from a starved state to the fed state causing a switch from fat to carbohydrate metabolism. As a result, potassium, phosphorus and magnesium are driven into cells causing levels of these electrolytes in the blood to drop. If these electrolytes drop below critical levels, death can result. Hypocalcaemia may also occur secondary to magnesium deficiency and may also be worth monitoring. Recommendations during feeding include: - Monitoring of potassium, magnesium, phosphate and calcium daily for the first 3 days until stable, then 3 times a week until stable. If blood results are abnormal, replete according to the NICE Guidelines (2006) by providing oral, enteral or intravenous supplements of: - Potassium (likely requirement 2-4mmol/kg/day). Phosphate (likely requirement 0.3-0.6mmol/kg/day). Magnesium (likely requirement 0.2mmol/kg/day intravenous, 0.4mmol/kg/day oral) NB: Please liaise with a general medical doctor from your local acute hospital should further advice on replenishment of electrolytes be required. 5. All service users at risk of Refeeding Syndrome should be referred to a Dietitian to assess and recommend an appropriate dietetic care plan (this does not include prescription, monitoring and replacement advice as documented above and is the responsibility of medical staff). In cases where a Dietitian is not available (i.e. out of hours) introduce food and/ or nutritional drinks gradually, avoid large increases in energy intake and avoid food and drinks high in sugar (e.g. lucozade). This Information sheet was developed by the Dietetic Service at South West Yorkshire Partnership NHS Foundation Trust in accordance with the National Institute for Clinical Excellence (NICE). Nutrition Support in Adults, 2006 and The Parenteral and Enteral Nutrition Group of The British Dietetic Association. A Pocket Guide to Clinical Nutrition, 2011. It will be updated when the NICE guidelines are next updated. Date Produced: January 2013