International Journal of Cardiology xxx (2012) xxx–xxx
Contents lists available at SciVerse ScienceDirect
International Journal of Cardiology
journal homepage: www.elsevier.com/locate/ijcard
Reduced number and impaired function of circulating endothelial progenitor cells in patients with
abdominal aortic aneurysm
Shih-Hsien Sung
Chun-Che Shih
b,c,d,1
a,d,e
, Tao-Cheng Wu
a,c,d
d,f
g
a,c,d
, Jia-Shiong Chen , Yung-Hsiang Chen , Po-Hsun Huang
, Shing-Jong Lin
a,c,d
,
a,d,f,
, Jaw-Wen Chen ⁎
a
Division of Cardiology, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwan Division of
b
Cardiovascular Surgery, Department of Surgery, Taipei Veterans General Hospital, Taipei, Taiwan Institute of Clinical Medicine,
National Yang-Ming University School of Medicine, Taipei, Taiwan
d
Cardiovascular Research Center, National
Yang-Ming University School of Medicine, Taipei, Taiwan
e
Institute of Pharmacology, National
Graduate Institute of Integrated Medicine, College of Chinese Medicine, China
Institute of Public Health, National Yang-Ming University School of Medicine, Taipei, Taiwan
Yang-Ming University School of Medicine, Taipei, Taiwan
g
f
Medical University, Taichung, Taiwan
article info
Article history:
Received 16 July 2011 Received in revised form
29 May 2012 Accepted 1 November 2012
Available online xxxx
Keywords:
Abdominal aortic aneurysm Endothelial function
Endothelial progenitor cells
abstract
different, it shares some risk factors with CAD. Therefore, the correlation between EPCs and AAA was investigated. Methods and
results: Seventy-eight subjects (age 77.2±7.8 years) with suspected AAA were prospectively enrolled. Cut-off values (men, 3.5–5.5
cm; women, 3–5 cm) were used to define normal aorta, small AAA, and large AAA on thoraco-abdominal computer tomography.
Endothelial function was measured by flow-mediated vasodilation (FMD). Flow cytometry and colony-forming units (CFUs) were
used to evaluate circulating EPC numbers. Circulating EPCs were defined as mononuclear cells with low CD45 staining and
double-positive staining for KDR, CD34, or CD133. Late out-growth EPCs were cultured from six patients with large AAAs and six
age-and sex-matched controls to evaluate proliferation, adhesion, migration, tube formation, and senescence. FMD was significantly
lower with large (5.26%±3.11%) and small AAAs (6.31%±3.66%) than in controls (8.88%±4.83%, P=0.008). Both CFUs (normal
38.39±12.99, small AAA 21.22±7.14, large AAA 6.98±1.97; P=0.026) and circulating EPCs (CD34 /KDR and
+
Aim: Circulating endothelial progenitor
cells (EPCs) are associated with coronary
artery disease (CAD) and predict its
outcome. Although the pathophysiology
of abdominal aortic aneurysm (AAA) is
+
CD133 /KDR )weresignificantly fewer in AAA patients than in controls. On multivariate analysis, CFUs and circulating
+
+
EPCs (CD34 /KDR ) were independently, inversely correlated to AAA diameter. Proliferation, adhesion, migration, tube
formation, and senescence of late EPCs were significantly impaired in AAA patients. Conclusion: The number and function of EPCs
were impaired in AAA patients, suggesting their potential role in AAA.
© 2012 Elsevier Ireland Ltd. All rights reserved.
+
+
1. Introduction
Abdominal aortic aneurysm (AAA) accounts for more than 15,000 annual
deaths in the US and is one of the leading causes of mortality in men aged more
than 50 year-old [1]. Its prevalence increases with increasing age, and the risk of
rupture increases with increasing aneurysm diameter. Once the aneurysm ruptures,
only 18% of the patients survive. The presence of AAA shares similar risks, such
as smoking, hypertension, and hypercholesterolemia, with atherosclerotic
cardiovascular
⁎ Corresponding author at: Division of Cardiology, Department of Medicine, Taipei Veterans General
Hospital, No. 201, Sec. 2, Shih-Pai Road, Taipei 112, Taiwan. Tel.: +886 2 2875 7511; fax: +886 2 2871
1601.
E-mail address: jwchen@vghtpe.gov.tw (J.-W. Chen).
Co-corresponder.
0167-5273/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ijcard.2012.11.002
disease [2,3]. However, the managements of these risk factors failed to prevent the
progression of AAA. AAA development and progression appear to be related to
an imbalance between destructive and restorative vascular wall processes.
Aneurysmal dilatation characteristically shows destruction of elastin and collagen
in the media and adventitia, loss of medial smooth muscle cells, vessel wall
thinning, and transmural lymphocyte and macrophage infiltration [4,5]. In addition,
the loss of endothelial integrity was also noted in AAA from histological
examination, which was also the fundamental cause of mural thrombosis
[6].Moreover, in a small series study of 30 patients with AAA, the endothelial
function reflected by endothelium dependent vasodilation has a negative and linear
correlation with the aneurysm diameter [7]. In an experimental AAA model,
creation of high aortic flow status by creating AV fistula promoted
re-endothelization of AAA and reduced its progression, when comparing with
normal or low aortic flow status [8].It
Please cite this article as: Sung S-H, et al, Reduced number and impaired
function of circulating endothelial progenitor cells in patients with abdominal
aortic
aneurysm,
Int
J
Cardiol
(2012),
http://dx.doi.org/10.1016/j.ijcard.2012.11.002
seems that the endothelial injury was associated with the occurrence of AAA and
the recovery of endothelial integrity correlated with the progression of AAA. Since
the circulating endothelial progenitor cells (EPCs) are a cellular reservoir to repair
or replace dysfunctional endothelium at vascular injury sites and restore
endothelial function [9–11]. The number of circulating EPCs may predict adverse
events and mortality in patients with different cardiovascular diseases [12,13]. It is
believed that the circulating EPCs might be associated with the presence and
progression of AAA. However, the only published data demonstrated an
unexpected result. The circulating EPCs defined by positive surface markers of
CD133 and/or CD34 increased in 25 subjects with AAA, comparing with 18
age-matched controls [14].Therefore, we would like to investigate the associations
of circulating EPCs as well as endothelial function with the progression of AAA in
the present study.
2.6. EPC culture
Peripheral blood samples (20 mL) were obtained in heparin-coated tubes from six patients with large AAAs
and six age-and sex-matched patients with normal aortas to study late EPCs in culture. MNCs were isolated
by density gradient centrifugation with Histopaque-1077 (Sigma), and the serum was preserved [17]. Briefly,
6
MNCs (5×10 )
were plated in 2-mL of endothelial growth medium (EGM-2 MV Cambrex, East Rutherford,
NJ, USA), with 15% individual serum on fibronectin-coated, 6-well plates. After 4 days of culturing, the
medium was changed, and nonadherent cells were removed; attached early EPCs appeared elongated with
spindle shapes. Some MNCs were allowed to grow into colonies of late (out-growth) EPCs, which emerged
2–3 weeks after the start of MNC culture. The late EPCs exhibited a ‘cobblestone’ morphology and
monolayer growth pattern typical of mature endothelial cells at confluence. Late EPCs were collected for the
functional assays.
2.7. EPC characterization
Early EPCs were characterized as adherent cells, double-positive for acetylated LDL uptake and lectin
binding by direct fluorescent staining, as previously described [17]. Briefly, the adherent cells were first
2. Methods
incubated
2.1. Study population
Subjects referred for a thoraco-abdominal computer tomogram (CT) with suspected AAA were eligible.
Patients with unstable angina, decompensated heart failure, inflammatory disease, ongoing infections, severe
renal failure, and who were allergic to contrast medium were excluded. Written, informed consent, as approved
by our Institutional Review Board, was obtained from each patient before enrolment. After overnight fasting,
patients were studied in a quiet, temperature-controlled room. Blood pressures (BPs) were obtained by
averaging three different measurements taken after a 15-minute rest. Serum and plasma samples were acquired
for plasma creatinine (PCr), fasting glucose, lipid profiles, and high-sensitivity C-reactive protein (hsCRP).
Height, weight, history, demographics, and prescribed medications were recorded. Estimated glomerular
filtration rate (eGFR) was calculated from plasma creatinine (PCr) using a modified Modification of Diet in
Renal Disease equation for the Chinese population: eGFR (mL/min/1.73 m
2
)= ×age ×(0.79 if
− 1.234
− 0.179
175×PCr female) [15]. Serum hsCRP was
determined by particle-enhanced immunoturbidimetry using latex agglutination (Toshiba, Tokyo, Japan).
with
2.4
mg/mL
1,1 ′
-dioctadecyl-3,3,
-tetramethylindocarbocyanine
2.8.1. EPC adhesion assay
4
EPCs' ability to adhere to the injured site to initiate the repair process was evaluated by plating 1×10
late
EPCs onto a fibronectin-coated, 6-well plate and incubating for 30 minutes. Gentle washing with PBS three
times was performed after a 30 min adhesion, and adherent cells in six random, high-power (×100)
microscopic fields (HPF) of each well were counted by independent, blinded investigators.
2.8.2. EPC proliferation assay
The proliferation of EPCs was determined by 3-(4,5-dimethylthiazol-2-yl)-2,5, diphenyltetrazolium bromide
4
The maximal abdominal aorta diameter was measured by reviewing each coronal CT section. Cut-off
values (men, 3.5–5.5 cm; women, 3–5 cm) were used to define normal aorta, small AAA, and large AAA.
,3 ′
2.8. EPC functional assays
(MTT) assay [17]. After being cultured with 1×10
2.2. AAA definitions
3 ′
perchlorate-acetylated LDL (DiI-acLDL; Molecular Probes, Eugene, OR, USA) for 1 h, then fixed in 2%
paraformaldehyde and counterstained with 10 mg/mL FITC-labeled lectin from Ulex europaeus (UEA-1;
Sigma). The late EPC-derived outgrowth endothelial cell population was characterized by
immunofluorescence staining for expressions of vascular endothelial (VE)-cadherin, platelet/endothelial cell
adhesion molecule-1 (PECAM-1, CD-31), and CD34 (Santa Cruz). Fluorescent images were recorded under a
laser scanning confocal microscope.
late EPCs in fibronectin-coated 24-well plates for 3 days,
the EPCs were supplemented with MTT (0.5 mg/mL; Sigma) and incubated for 4 h for the proliferation assay.
The blue formazen was dissolved with dimethyl sulfoxide and measured at 550/650 nm. In addition,
simultaneous culturing with human aortic endothelial cells (HAECs) served as the internal control [19]. The
EPC proliferation activity was presented as the ratio to HAECs.
2.3. Determination of endothelial function
2.8.3. EPC migration assay
EPC migration was evaluated by a modified Boyden chamber assay (Transwell, Coster; Corning Inc., Acton,
Endothelial function was measured by endothelium-dependent flow-mediated vasodilatation (FMD) using
a 7.5-MHz linear array transducer (Sonos 5500; Hewlett-Packard, Andover, MA, USA) to scan the brachial
artery [16]. The procedure was performed in a quiet, air-conditioned room (22–25 °C) by an experienced
technician blinded to the clinical data. The left arm was stabilized with a cushion, and a sphygmomanometric
cuff was placed on the forearm. A baseline image was acquired, and blood flow was estimated by
time-averaging the pulsed Doppler velocity signals from a mid-artery sample volume. Then, the cuff was
MA, USA) [17]. Isolated EPCs were detached as described above with trypsin/EDTA, and 3×10
inflated to ≥ 50 mm Hg above systolic pressure to occlude the arteries for 5 min and released abruptly. A
mid-artery pulsed Doppler signal was obtained immediately upon cuff release, and brachial artery diameters
were obtained at 30, 60, 90, 120, and 150 s after deflation. FMD was calculated as maximal post-occlusion
brachial artery diameter relative to averaged baseline diameters.
2.4. Circulating EPC assay
+
+
for
+
CD34
+
low
+
+
low
and
low
2.5. EPC colony-forming assay
Isolated mononuclear cells (MNCs) were resuspended in growth medium (EndoCult; StemCell Technologies,
6
Vancouver, Canada), and 5×10
MNCs were preplated onto a fibronectin-coated six-well plate in duplicate
[18]. After 48 h, nonadherent cells were collected by pipetting the medium in each well up and down three
6
times, and 1×10
2.8.4. EPC tube-formation assay
In vitro tube formation was assayed using the In Vitro Angiogenesis Assay Kit (Chemicon) [17]. ECMatrix
gel solution was thawed at 4 °C overnight, mixed with ECMatrix diluent buffer, and placed in a 96-well plate
at 37 °C for 1 h to allow the matrix solution to solidify. EPCs were harvested as described above with
4
KDR CD45 , CD34 CD133 CD45 ,
KDR CD133 CD45 , respectively. (Fig. 1).
defined
cells were replated onto a fibronectin-coated 24-well plate. On day 5 of the assay, the
colony-forming units (CFUs) per well for each sample were counted manually in a minimum of three wells by
two independent observers.
EPCs
were placed in the upper chambers of 24-well transwell plates with polycarbonate membranes (8-mm pores)
that contained serum-free EGM; vascular endothelial growth factor (VEGF, 50 ng/mL) was added to the
medium in the lower chambers. After incubation for 24 h, the membrane was washed briefly with PBS and
fixed with 4% paraformaldehyde. The upper side of the membrane was wiped gently with a cotton ball. The
membrane was stained using hematoxylin solution and carefully removed. The number of migratory late
EPCs was evaluated by counting the migrated cells in six random HPFs.
trypsin/ EDTA, then 1×10
The method for assessing the number of circulating EPCs has been previously described [17,18]. Briefly,
a 10-mL volume of peripheral blood was incubated for 30 min in the dark with monoclonal antibodies against
human kinase insert domain-conjugating receptor (KDR; R&D, Minneapolis, MN, USA) followed by
phycoerythrin (PE)-conjugated secondary antibody, with fluorescein isothiocyanate (FITC)-labeled monoclonal
antibodies against human CD45 (Becton Dickinson, Franklin Lakes, NJ, USA), with PE-conjugated
monoclonal antibody against human CD133 (Miltenyi Biotec, Bergisch Gladbach, Germany), and
FITC-conjugated or PE-conjugated monoclonal antibodies against human CD34 (Serotec, Raleigh, NC, USA)
and KDR (Sigma, St Louis, MI, USA). Isotype-identical antibodies served as controls (Becton Dickinson).
After incubation, cells were lysed, washed with phosphate-buffered saline (PBS), and fixed in 2%
paraformaldehyde before analysis. Each analysis included 100,000 events. The numbers of circulating EPCs
were
4
EPCs were placed on matrix solution with EGM-2 MV medium with glucose or
mannitol, and incubated at 37 °C for 16 h. Tubule formation was inspected under an inverted light
microscope (×100). Four representative fields were taken, and the average total area of complete tubes formed
by cells was compared using Image-Pro Plus software (Media Cybernetics, Inc., MD, USA).
Please cite this article as: Sung S-H, et al, Reduced number and impaired
function of circulating endothelial progenitor cells in patients with abdominal
aortic
aneurysm,
Int
J
Cardiol
(2012),
http://dx.doi.org/10.1016/j.ijcard.2012.11.002
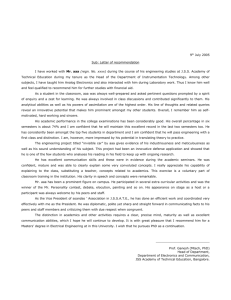
Fig. 1. Representative flow-cytometry analysis for quantifying the number of circulating endothelial
and KDR CD133 CD45 , respectively.
+
+
low
progenitor cells (EPCs). Mononuclear cells (MNCs) were gated by forward/ sideward scatter (FSC/SSC). The
+
numbers of circulating EPCs were defined for CD34
CD133 CD45 , CD34 KDR CD45 ,
+
low
+
+
low
2.8.5. EPC senescence assay
Cellular aging was quantified using a Senescence Cell Staining Kit (Sigma) [17]. EPCs were plated in
12-well plates and cultured for 4 days. After washing with PBS, EPCs were fixed for 6 min in 2%
formaldehyde and 0.2% glutaraldehyde in PBS, and then incubated for 12 h at 37 °C without CO2 with fresh
X-gal staining solution. Green-stained cells and total cells were counted in six random HPFs, and the percentage of β -galactosidase-positive cells was calculated.
2.9. Statistical analysis
A total of seventy-eight patients (72 men; mean age, 77.2±
7.8 years) were enrolled; 15 had normal aortas, 27 had small AAAs, and 36 had
large AAAs. Baseline characteristics are shown in Table 1. In brief, while systolic
and diastolic BPs were similar in the three groups, large AAA patients had the
lowest pulse pressures. Compared to controls, AAA patients more frequently
received beta-blockers, and large AAA patients had lower eGFR. Other
characteristics did not differ among the groups.
Means, standard deviations, and percentages were used to describe the participants' characteristics.
Comparisons of continuous variables among three groups were performed by analysis of variance using
oneway ANOVA and Bonferroni's post-hoc test. Subgroup comparisons of categorical variables were
assessed by the chi-square or Fisher's exact test. Correlations of various factors with maximum AAA diameter
were determined with bivariate Pearson correlation. Independent risk factors associated with maximum AAA
diameters were identified using a multivariate linear regression model. The late
Table 1
Subjects' baseline characteristics.
EPCs' functions were compared between AAA and normal aorta subjects, using Student's t-test. Pb0.05 was
considered significant; all analyses were carried out with SPSS 15.0 (SPSS Inc. Chicago, IL, USA).
3. Results
Normal aorta
N=15
Small AAA
N=27
Large AAA
N=36
P value
Age, years
Male sex, N (%)
BMI, kg/m2
SBP, mm Hg
DBP, mm Hg
78.13±7.02
15 (100)
22.88±3.92
140.7±16.8
77.7±8.6
77.22±6.40
25 (92.6)
27.91±22.09
136.3±21.4
75.3±10.2
76.83±9.16
32 (88.9)
23.90±3.38
129.6±15.8
76.2±11.2
0.867
0.397
0.427
0.152
0.795
Pulse pressure, mm Hg
63.0±10.7
61.0±18.0
53.4±10.38⁎,†
26 (72.2)
4 (11.1)
19 (52.8)
12 (33.3)
0.051
8 (53.3)
3 (20)
5 (33.3)
3 (20)
Hypertension, N (%)
Diabetes, N (%)
CAD, N (%)
Smoker, N (%)
2.99±0.35
20 (74.1)
2 (7.4)
10 (37.0)
8 (29.6)
4.70±0.60⁎
WBC,/cm3
Hemoglobin, mg/dL
Creatinine, mg/dL
eGFR, mL/min/1.73 m2
Lipid profiles, mg/dL
6307±1634
13.27±1.35
1.03±0.24
82.85±23.14
6470±1511
13.16±1.97
1.27±0.41
66.58±23.60
6.76±1.02⁎,†
6578±2620
12.32±2.12
1.59±1.52
63.64±27.84⁎
b0.001
0.916
0.142
0.196
0.052
Total cholesterol
Triglyceride
HDL
LDL
Fasting glucose, mg/dL
HsCRP, mg/dL
LVEF, %
Medications, N (%)
179.00±37.80
96.69±38.15
59.00±29.40
95.90±40.29
106.58±21.99
0.44±0.44
54.8±8.9
171.72±30.77
108.64±55.97
52.36±24.05
104.36±29.65
101.92±24.93
1.03±2.33
53.4±8.2
172.25±34.63
108.92±62.67
45.97±14.63
109.50±30.33
94.97±17.72
0.92±1.65
51.9±8.6
0.797
0.785
0.164
0.470
0.197
0.528
0.678
Anti-platelet
Beta-blocker
12 (80)
0 (0)
23 (85.2)
10 (37)
27 (75)
10 (27.8)
ACEI/ARB
Statin
Normal aorta
12 (44.4)
6 (22.2)
14 (38.9)
5 (13.9)
Small AAA
9 (60)
1 (6.7)
Large AAA
N=15
N=27
Diameter, cm
0.328
0.470
0.309
0.636
0.611
0.029
0.385
0.385
P
value
N=36
FMD, %
8.88±4.83
6.31±3.66⁎
5.26±3.11⁎
0.008
Data are displayed as means±standard deviation or number (%). AAA: abdominal aortic aneurysm; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin II receptor blocker; BMI: body mass index; CAD: coronary
Progenitor cells,%
artery disease; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HDL: high-density lipoprotein; HsCRP: highsensitivity C-reactive protein; LDL: low-density lipoprotein; LVEF: left ventricular ejection
fraction;
pressure; WBC: white
blood cell.
CD34 SBP: systolic blood2.1±0.9
2.3±1.5
2.2±0.9
0.890
⁎CD34/CD133
Pb 0.05 compared to controls
in post hoc analysis.
0.510±0.878
0.272±0.345
†CD34/KDR
0.246±0.256⁎
0.500±0.590
0.064±0.099⁎
CD133/KDR
0.208±0.342
Pb 0.05 compared to small AAA group in post hoc analysis.
24.78±12.12⁎
EPC CFU/well
34.67±13.36
0.250±0.213
0.174±0.255⁎
0.011
0.164
0.045±0.074⁎
0.007
12.58±8.01⁎,†
b0.00
Please cite this article as: Sung S-H, et al, Reduced number and impaired 1function of circulating endothelial progenitor cells in patients with abdominal aortic aneurysm,
Systolic blood pressure, mm Hg
− 0.256
0.035
Pulse pressure, mm Hg
− 0.297
0.014
Int J Cardiol (2012), http://dx.doi.org/10.1016/j.ijcard.2012.11.002
3.1. Endothelial function and EPCs
Normal aorta
N=15
Controls had better endothelial function, reflected by FMD, than AAA patients
(Table 2). The level of circulating CD34+ cells was similar among the 3 groups.
However, AAA patients had significantly fewer circulating EPCs, reflected by
double-positive stainings of CD34/KDR and CD133/KDR, but not CD34/CD133.
In addition, AAA patients had fewer EPC CFUs.
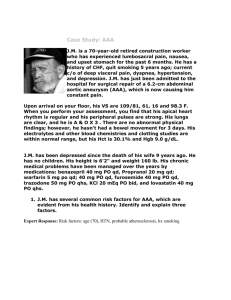
3.2. Factors associated with maximal AAA diameter
Systolic BP, pulse pressure, hemoglobin, and eGFR were negatively
associated, and serum creatinine positively associated, with maximal aortic
diameter (Table 3). FMD was negatively correlated to aneurysm diameter (Fig.
2A). Both the numbers of circulating CD34 /KDR EPCs and EPC CFUs were
negatively associated with AAA diameter (Fig. 2B, C). After adjusting for systolic
BP, pulse pressure, hemoglobin, and eGFR in a multivariate linear regression
+
+
model, the numbers of CD34 /KDR EPCs and EPC CFUs remained
independently associated with aortic diameter (Table 3). Standardized coefficients
+
+
were − 0.231 (P=0.048) and − 0.443 (Pb0.001), respectively.
3.3. Characterization of late EPCs
Small AAA
N=27
Age, years
Male sex, N (%)
BMI, kg/m2
SBP, mm Hg
DBP, mm Hg
78.13±7.02
15 (100)
22.88±3.92
140.7±16.8
77.7±8.6
77.22±6.40
25 (92.6)
27.91±22.09
136.3±21.4
75.3±10.2
Pulse pressure, mm Hg
63.0±10.7
61.0±18.0
Hypertension, N (%)
8 (53.3)
Diabetes, N (%)
3 (20)
CAD, N (%)
5 (33.3)
Smoker, N (%)
3 (20)
Table 3
Diameter, cm
2.99±0.35
Correlation coefficients of the maximum abdominal aortic aneurysm diameters and other variables.
WBC,/cm3
6307±1634
Hemoglobin, mg/dL
13.27±1.35
Coefficients
P
value
Creatinine, mg/dL
1.03±0.24
eGFR, mL/min/1.73 m2
82.85±23.14
Lipid profiles, mg/dL
20 (74.1)
2 (7.4)
10 (37.0)
8 (29.6)
4.70±0.60⁎
6470±1511
13.16±1.97
1.27±0.41
66.58±23.60
Total
179.00±37.80
CFU:cholesterol
colony-forming unit; eGFR: estimated glomerular filtration
rate; EPC: endothelial progenitor cell; FMD: 171.72±30.77
Triglyceride
96.69±38.15
108.64±55.97
flow-mediated vasodilation.
HDL
59.00±29.40
52.36±24.05
LDL
95.90±40.29
104.36±29.65
Fasting glucose, mg/dL
106.58±21.99
101.92±24.93
HsCRP, mg/dL
0.44±0.44
1.03±2.33
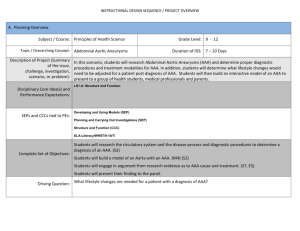
3.4.4.
Tube
formation
LVEF, %
54.8±8.9
53.4±8.2
Late
EPC
tube
formation
on
ECMatrix
gel
was
lower
in
AAA
patients
(22.15±7.63
Medications, N (%)
tubes/well) than in controls (41.49±17.74 tubes/well; P =0.042) (Fig. 4D).
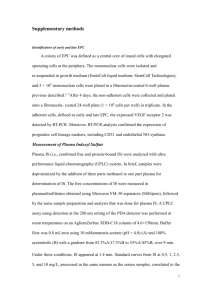
The peripheral blood MNCs seeded on fibronectin-coated wells were initially
round (Fig. 3A) [17]. After changing the medium on day 4, attached early EPCs
appeared elongated with spindle shapes (Fig. 3B). Late EPCs with
cobblestone-like morphology similar to mature endothelial cells were grown to
confluence (Fig. 3C). Late EPC characterization was performed by
immunohistochemical staining; most cells expressed VE-cadherin, PECAM-1, and
CD34; critical markers of outgrowth endothelial cell-producing late EPCs (Fig. 3D,
E, F).
Anti-platelet
Beta-blocker
3.4.5. Senescence
ACEI/ARB
Statin
AAA patients tended
Normal aorta
12 (80)
0 (0)
23 (85.2)
10 (37)
9 (60)
12 (44.4)
6 (22.2)
1 (6.7) of senescence-associated, β
to have higher percentages
Small AAA
Large AAA
P
-galactosidase-positive EPCs (63.32%±13.72%) than controls (48.77%±8.52%;
P
value
N=15
N=27
N=36
=0.052) (Fig. 4E).
FMD, %
3.4.6. Senescence
8.88±4.83
6.31±3.66⁎
5.26±3.11⁎
0.008
Progenitor cells,%
AAA patients also have higher percentages of senescence-associated, β
2.3±1.5
2.2±0.9
0.890
(65.6%±10.2%)
than controls
(48.8%±8.5%;
P=0.011)
0.272±0.345
0.250±0.213
0.164
(Fig.
4E).
0.246±0.256⁎
0.174±0.255⁎
CD34/KDR
0.500±0.590
0.011
CD34
2.1±0.9
-galactosidase-positive
EPCs
CD34/CD133
0.510±0.878
3.4. In vitro AAA EPC functions
3.4.1. Adhesion
After a 30-min incubation, patients with normal aorta had more adherent cells
than large AAA patients (49.8±13.9 cells/HPF and
31.1±9.4 cells/HPF, respectively; P =0.021) (Fig. 4A).
CD133/KDR
0.208±0.342
4. Discussion
EPC CFU/well
34.67±13.36
0.064±0.099⁎
0.045±0.074⁎
0.007
24.78±12.12⁎
12.58±8.01⁎,†
b0.00
1
0.035
comprehensively− 0.256
the endothelial function,
circulating
Pulse
mm Hg
− 0.297
0.014
EPCpressure,
number
by 2 distinct methods, and biological
functions of late
outgrowth
Hemoglobin,
− 0.245
0.032 function,
EPCs. Themg/dL
data showed that patients with AAA
had impaired endothelial
3.4.2. Proliferation
Creatinine,
mg/dL
0.001
measured
by flow-mediated vasodilation and 0.362
reduced number of circulating
EPCs,
After a 3 day culture, significantly attenuated EPC proliferation activity was
eGFR,
mL/min/1.73
m2
− 0.303
measured
by both
flow cytometry and colony-forming
units. In 0.007
addition, the
noted in patients with AAA group than in patients with normal aorta (Fig. 4B).
FMD,
% functions of late EPCs cultured from
− 0.319
0.005impaired,
in-vitro
AAA patients were also
CD34
+/CD133+ EPCs, %
0.088
−
0.196
comparing
with
those
from
subjects
with
normal
aorta.
Furthermore,
the numbers
3.4.3. Migration
CD34
+/KDR+ EPCs, %
− 0.230
of circulating
EPCs and EPC CFUs were independently
associated 0.045
with maximal
After a 24 h incubation, less EPCs cultured from AAA patients appeared to
CD133
+ EPCs, %
0.092
0.193pulse pressure, hemoglobin,
AAA+/KDR
diameters,
after accounting for systolic− BP,
and
migrate to the lower chambers (37.1±18.6 cells/HPF) than those from controls
EPC-CFU/well
b0.001
eGFR. Although this is a cross-sectional− 0.542
study, it firstly demonstrated
the
(65.2±22.9 cells/HPF; P =0.042) (Fig. 4C).
consistent and independent associations of circulating EPCs with clinical AAA, to
the best of our knowledge. These findings may explain the potential impact of
circulating EPCs in AAA development and progression, and support the future
target of endothelial function for the prevention and potential adjunct treatment of
Normal aorta
SmallAAA.
AAA
Large AAA
P value
N=15
N=27
Age, years
Male sex, N (%)
BMI, kg/m2
SBP, mm Hg
DBP, mm Hg
78.13±7.02
15 (100)
22.88±3.92
140.7±16.8
77.7±8.6
Pulse pressure, mm Hg
63.0±10.7
Hypertension, N (%)
8 (53.3)
Diabetes, N (%)
3 (20)
TableN2(%)
CAD,
5 (33.3)
Smoker,
N (%)
3 (20)
Endothelial
function, endothelial progenitor cells, and systemic inflammation
by group.
Diameter, cm
2.99±0.35
WBC,/cm3
6307±1634
Hemoglobin, mg/dL
13.27±1.35
Creatinine,
mg/dL aortic aneurysm; CFU: colony-forming unit;
1.03±0.24
AAA: abdominal
EPC: endothelial progenitor cell; FMD:
eGFR,
mL/min/1.73
m2
82.85±23.14
flow-mediated
vasodilation.
Lipid
profiles,
mg/dL to controls in post hoc analysis.
⁎ Pb
0.05 compared
†
Systolic
blood pressure,
Hg
The present
studymmaccessed
Total cholesterol
179.00±37.80
Triglyceride
96.69±38.15
Pb0.05 compared to small AAA group in post hoc analysis.
HDL
59.00±29.40
LDL
95.90±40.29
N=36
4.1. Endothelial and vascular damage
in AAA
76.83±9.16
77.22±6.40
25 (92.6)
27.91±22.09
Different, and
136.3±21.4
found in AAA
75.3±10.2
32 (88.9)
risk23.90±3.38
factors
129.6±15.8
may76.2±11.2
include
0.867
0.397
0.427
to those of atherosclerosis
have been
0.152
old age, male gender, current
smoking,
0.795
even opposite,
patients, which
hypertension, and dyslipidemia,53.4±10.38⁎,†
but not diabetes mellitus [20]. Moreover,
while
61.0±18.0
0.051
smoking and aneurysm diameter 26are(72.2)
risk factors for aneurysm expansion,
low
20 (74.1)
0.328
2 (7.4)
4 (11.1)
ankle-brachial index—amarkerof peripheral
arterial disease—prevents0.470
progression,
10 (37.0)
19 (52.8)
0.309
suggesting that local factors such 12
as (33.3)
regional hemodynamic and/or local
vascular
8 (29.6)
0.636
injury rather than systemic pathology
affect disease progressionb0.001
[21].Thus, a
4.70±0.60⁎
6.76±1.02⁎,†
complex interaction of different mechanisms,
including vascular inflammation
and
6470±1511
6578±2620
0.916
13.16±1.97
12.32±2.12
0.142 AAA is
hemodynamic and genetic factors,
may cause AAA [22]. Although
1.27±0.41
1.59±1.52
0.196
generally caused by a primary process
involving the media, which is0.052
the cellular
66.58±23.60
63.64±27.84⁎
dysfunction of smooth muscle cells,
171.72±30.77
Please cite
108.64±55.97
function of
52.36±24.05
104.36±29.65
172.25±34.63
0.797
109.50±30.33
0.470
this article as: Sung
S-H, et al, Reduced number and0.785
impaired
108.92±62.67
circulating endothelial
progenitor cells in patients with 0.164
abdominal
45.97±14.63
aortic
aneurysm,
Int
J
http://dx.doi.org/10.1016/j.ijcard.2012.11.002
Cardiol
(2012),
Fig. 2. The association of abdominal aortic aneurysm diameter with endothelial function (flow-mediated
vasodilation), the level of circulating endothelial progenitor cells (EPCs, CD34
/KDR ),
+
+
and EPC
colony-forming units (CFUs). The graphs show the distribution of maximum aneurysmal diameter and
flow-mediated vasodilation (A), CD34
/KDR EPCs (B), and EPC CFUs (C) in 78 participants.
+
+
fragmentation of elastic fibers, and collagen degradation through various proteolytic enzymes, particularly matrix metalloproteinase (MMP) [23], further hemodynamic effects
of BP and mechanical wall stress are essential to the progressive enlargement. Therefore, the endothelial cells, which modulate the vasodilatation and the inflammation as well
as the activity of proteolytic enzymes in the arterial walls [24,25], might be associated with the remodeling of arterial medial layer and the progression of aortic aneurysm.
The aortic endothelium may also be injured not only due to traditional atherosclerosis risk factors, but also due to increased mechanical wall stress associated with the changing aortic wall structure [24,26]. While the integrity and functional activity of the endothelial monolayer are important in atherogenesis [27], a defective vascular endothelium
leading to an uninhibited inflammatory responses appears to contribute to aneurysm formation [24].In addition, Knipp et al. demonstrated impaired vasoreactivity despite
higher plasma nitrite in AAA patients than in peripheral arterial disease patients, suggesting desensitization of the systemic vasculature to normal vasodilatory stimuli [28]. In
line with previous findings, the present study showed that forearm FMD, which reflects systemic vascular endothelial function, was inversely and linearly associated with
AAA diameter, suggesting that vascular endothelial dysfunction and AAA development and/or progression are linked.
4.2. EPCs' potential role in AAA development and progression
Circulating EPCs may play an important role in endothelial repair of vascular damage. Endothelial function and the level of circulating EPCs have been associated in various
populations [9,29]. Although it has been showed that patients with AAA would have impaired endothelial function, the expected negative correlation of the present AAA and
circulating CD34 /CD133 EPC number did not exist in the only published study [7,14]. However, CD34 and/or CD133 might not be adequate surface markers to identify
+
+
EPCs [30]. In addition, Parietti et al. illustrated that the level of CD34 /KDR EPCs was inversely related to aneurysm diameter in 27 patients with thoracic aortic aneurysm
[31]. But the pathologic features of thoracic aortic aneurysm might not be identical to AAA. In this study, in addition to FMD, the numbers of EPC CFUs and circulating
EPCs were significantly inversely and linearly correlated to aortic diameter, and remained independent even after adjusting for BP, hemoglobin, and renal function. Since
+
+
CD34 is a surface marker of stem cells and the circulating CD34 progenitor cells are similar between groups, it supports that the diminished EPC number in the patients
with AAA is not due to bone marrow dysfunction and related poor production. Further, the present data also showed impaired function of late EPCs in AAA
+
Fig. 3. Morphology and characterization of human endothelial progenitor cells (EPCs) from peripheral blood. Mononuclear cells (MNCs) were plated on a fibronectin-coated culture dish on the first day (A). Four days after plating,
adherent early EPCs with spindle shapes are seen (B). Three weeks after plating, late (outgrowth) EPCs with a cobblestone-like morphology were selected, reseeded, and grown to confluence (C). Immunofluorescence detection of
1,1′ -dioctadecyl-3,3,3′ ,3′ -tetramethylindocarbocyanine perchlorate-acetylated LDL (DiI-acLDL, red), VE-cadherin (green) (D), platelet/endothelial cell adhesion molecule-1 (CD31, green) (E), and CD34 (green) (F) for late
EPCs. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
Please cite this article as: Sung S-H, et al, Reduced number and impaired function of circulating endothelial progenitor cells in patients with abdominal aortic aneurysm,
Int J Cardiol (2012), http://dx.doi.org/10.1016/j.ijcard.2012.11.002
Fig. 4. Functional assays (including in vitro migration, reactive oxygen species production, cellular senescence, and apoptosis) of late endothelial progenitor cells (EPCs) cultured from six patients with large abdominal aortic
4
aneurysms (AAAs) and from six age-and sex-matched controls. After incubation of 1×10
late EPCs for 30 min, the EPC adhesion in AAA patients is significantly fewer than in the normal aorta (A). After incubation of 1×10 late
4
EPCs for 3 days, the EPC proliferation activity is significantly less in AAA patients than in the normal aorta (B). A modified Boyden chamber assay with vascular endothelial growth factor (VEGF) as a chemoattractant factor was
used to assess EPC migration. Representative photos are shown; the small dots are holes in the barrier membrane. The migrated cells are stained with hematoxylin and counted under the microscope. The migration function of EPCs
from AAA patients is significantly less than in the normal aorta (C). An in vitro angiogenesis assay for late EPCs was used with ECMatrix gel. The average total numbers of complete tubes formed by cells were compared by
computer software. The in vitro tube formation is significantly impaired in late EPCs cultured from AAA patients compared to normal aorta (D). Compared to patients with normal aorta, incubated EPCs from AAA patients have a
significantly increased percentage of senescence-associated β -galactosidase-positive EPCs (E). (Data expressed as means±standard error).
patients, suggesting that vascular and endothelial repair fails not only high flow conditions may stabilize aortic integrity and limit aneurysm due to fewer EPCs, but also due
to inefficacious late EPCs in AAA pa-growth [26]. These findings highlight EPCs' potential protective role tients. In experimental aneurysm models, enhanced cellularities of
in vascular repair during AAA development. Thus, a possible theraendothelial cells and smooth muscle cells in the arterial wall under peutic strategy with statins and other
medications may improve
Please cite this article as: Sung S-H, et al, Reduced number and impaired function of circulating endothelial progenitor cells in patients with abdominal aortic aneurysm,
Int J Cardiol (2012), http://dx.doi.org/10.1016/j.ijcard.2012.11.002
endothelial cells or even EPC function and modulate AAA progression [32,33].
Conversely, decreased and/or dysfunctional smooth muscle cells in the arterial
media might be the sentinel changes related to MMP activation and extracellular
matrix reduction. Sporadic studies have demonstrated an overexpression of
proangiogenic cytokine and abundant neovascularization in the media of
aneurysm rupture edge, compared to the normal aorta [34]. Given the circulating
EPC potential role in neovascularization with vascular occlusion, they might be
involved in aortic aneurysm rupture. However, since no patients had ruptured
AAAs in our study, its findings might not relate to patients with relatively stable
AAA.
Plaque neovascularization is thought not only to participate intimately in the
growth and progression of human atherosclerosis but also to play a role in plaque
destabilization, causing plaque rupture [35]. However, recent clinical trials in
acute or chronic CAD patients showed no increased incidence of plaque
progression and/or rupture after cell therapy with vascular progenitor cells
including EPCs [35,36]. Given the similar trends of circulating EPCs for disease
progression in CAD and in AAA, circulating EPCs may contribute to aortic
endothelial repair and vascular protection rather than to vascular injury and medial
neovascularization in clinical AAA.
4.3. BP, pulse pressure, and hemodynamics in AAA development and
progression
Hemodynamic conditions affect AAA progression clinically, suggesting the
need for adequate BP control [8]. However, whether BP lowering therapy
prevents aneurysm progression is unknown [21]. In the present study, there was
no difference in the presence of hypertension, baseline systolic and diastolic BPs,
and the use of antihypertensives among the three groups, except that beta-blockers
were more frequently used in patients with AAAs. On the other hand, pulse
pressure, a surrogate of arterial stiffness, is associated with the incidence and
clinical outcomes of cardiovascular diseases [37]. Although a high pulse pressure
is generally considered a risk factor, patients with large AAAs tended to have a
lower pulse pressure than patients with small AAAs. Given that low pulse
pressure may be associated with low shear stress, our findings are partially
compatible with previous in vivo findings that flow conditions may affect CD34+
cell localization and differentiation in experimental AAA. In rat AAA models,
low flow and shear stress reduced endothelial proliferation, luminal surface
re-endothelialization, and mural smooth muscle proliferation, and increased
transmural macrophage infiltration, while promoting AAA progression. However,
high flow limits AAA progression [38]. Accordingly, in our patients, both the
impaired EPCs and low pulse pressure might have contributed to the poor differentiation and maturation of EPCs, persistent vascular inflammation, and medial
hypocellularity, causing AAA progression.
4.4. Study limitations
Some study limitations should be addressed. First, the patient sample was
relatively small, and the presence of co-morbidities might affect circulating EPC
levels. However, there was no significant heterogeneity of baseline characteristics
among the study population, except for beta-blocker use. Furthermore, circulating
EPC levels were evaluated comprehensively by different methods that showed
similar EPC reductions in AAA patients. Since the controversies remain to
identify circulating EPCs using flow cytometry or CFUs, while vast majority of
these cells are thought to be hematopoietic lineage cells, future works are needed
to calculate the true vasculogenic late outgrowth EPCs in peripheral circulating.
Although it would be more interesting to measure the circulating mesenchymal
stem cells and its association with EPCs since AAA is primarily a medial
pathology, numerous studies continue to struggle in the definition. Second, late
EPC functions were examined in a limited number of patients. However,
age-matched cohorts were compared, and the data consistently showed impaired
late EPC function by distinct functional assays. Moreover, the success rate of the
current method for culturing late EPCs is over 80% in our laboratory. Both of the
above may minimize potential selection bias. Finally, given this study's
cross-sectional nature, no causal relationship can be inferred between impaired
circulating EPCs and AAA. However, the correlations of EPCs and AAA were
consistently and independently demonstrated by using different assays in this
study, which might be applied to a longitudinal follow-up and potential cell
therapy.
5. Conclusions
Circulating EPC levels were reduced and the function of late EPCs was impaired
in AAA patients. Though the underlying mechanisms were not elucidated, the
current findings are the first to demonstrate the clinical connections between injury
and repair of the vascular endothelium and AAA development and progression.
Our findings also support the hypothesis that vascular progenitor cells such as
EPCs might be a novel therapeutic target for AAA [38]. Future clinical studies,
particularly longitudinal cohort studies with or without EPC-targeted pharmacological intervention, may be warranted.
Funding
This work was partly supported by research grants from the National Science
Council (95-2314-B-010-024-MY3 to Chen JW, and UST-UCSD International
Center of Excellence in Advanced Bio-engineering NSC99-2911-I-009-101 to
Chen JW & Lin SJ) and from Taipei Veterans General Hospital (V97ER2-003 and
VN 9803 to Chen JW, and V99B1003 to Sung SH), and also by a grant from the
Ministry of Education “Aim for the Top University” Plan.
Conflict of interest statement
None declared.
Acknowledgments
The authors of this manuscript have certified that they comply with the Principles
of Ethical Publishing in the International Journal of Cardiology [39].
References
[1] Lederle FA, Johnson GR, Wilson SE, et al. Prevalence and associations of abdominal aortic
aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans
Affairs Cooperative Study Group. Ann Intern Med 1997;126: 441-9.
[2] Blanchard JF, Armenian HK, Friesen PP. Risk factors for abdominal aortic aneurysm: results of a
case–control study. Am J Epidemiol 2000;151:575-83.
[3] Forsdahl SH, Singh K, Solberg S, Jacobsen BK. Risk factors for abdominal aortic aneurysms: a
7-year prospective study: the Tromso Study, 1994–2001. Circulation 2009;119:2202-8.
[4] Davies MJ. Aortic aneurysm formation: lessons from human studies and experimental models.
Circulation 1998;98:193-5.
[5] Freestone T, Turner RJ, Coady A, Higman DJ, Greenhalgh RM, Powell JT. Inflammation and
matrix metalloproteinases in the enlarging abdominal aortic aneurysm. Arterioscler Thromb Vasc Biol
1995;15:1145-51.
[6] Touat Z, Ollivier V, Dai J, et al. Renewal of mural thrombus releases plasma markers and is
involved in aortic abdominal aneurysm evolution. Am J Pathol 2006;168:1022-30.
[7] Medina F, de Haro J, Florez A, Acin F. Relationship between endothelial dependent vasodilation
and size of abdominal aortic aneurysms. Ann Vasc Surg 2010;24: 752-7.
[8] Sho E, Sho M, Nanjo H, Kawamura K, Masuda H, Dalman RL. Hemodynamic regulation of
CD34+ cell localization and differentiation in experimental aneurysms. Arterioscler Thromb Vasc Biol
2004;24:1916-21.
[9] Hill JM, Zalos G, Halcox JP, et al. Circulating endothelial progenitor cells, vascular function, and
cardiovascular risk. N Engl J Med 2003;348:593-600.
Please cite this article as: Sung S-H, et al, Reduced number and impaired
function of circulating endothelial progenitor cells in patients with abdominal
aortic
aneurysm,
Int
J
Cardiol
(2012),
http://dx.doi.org/10.1016/j.ijcard.2012.11.002
[10] Kaushal S, Amiel GE, Guleserian KJ, et al. Functional small-diameter neovessels created using
endothelial progenitor cells expanded ex vivo. Nat Med 2001;7:1035-40.
[11] Walter
DH, Rittig K, Bahlmann FH, et al. Statin therapy accelerates reendothelialization: a novel
effect involving mobilization and incorporation of bone marrow-derived endothelial progenitor cells.
Circulation 2002;105:3017-24.
[12] Michowitz Y, Goldstein E, Wexler D, Sheps D, Keren G, George J. Circulating endothelial progenitor
cells and clinical outcome in patients with congestive heart failure. Heart 2007;93:1046-50.
[13] Werner N, Kosiol S, Schiegl T, et al. Circulating endothelial progenitor cells and cardiovascular
outcomes. N Engl J Med 2005;353:999–1007.
[14] Dawson J, Tooze J, Cockerill G, Choke E, Loftus I, Thompson MM. Endothelial progenitor cells and
abdominal aortic aneurysms. Ann N Y Acad Sci 2006;1085: 327-30.
[15] Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese
patients with chronic kidney disease. J Am Soc Nephrol 2006;17: 2937-44.
[16] Corretti MC, Anderson TJ, Benjamin EJ, et al. Guidelines for the ultrasound assessment of
endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International
Brachial Artery Reactivity Task Force. J Am Coll Cardiol 2002;39:257-65.
[17] Chen YH, Lin SJ, Lin FY, et al.
High glucose impairs early and late endothelial progenitor
cells by modifying nitric oxide-related but not oxidative stress-mediated mechanisms. Diabetes
2007;56:1559-68.
[18] Huang PH, Huang SS, Chen YH, et al. Increased circulating CD31+/annexin V+ apoptotic microparticles
and decreased circulating endothelial progenitor cell levels in hypertensive patients with
microalbuminuria. J Hypertens 2010;28: 1655-65.
[19] Chen JW, Chen YH, Lin FY, Chen YL, Lin SJ. Ginkgo biloba extract inhibits tumor necrosis
factor-alpha-induced reactive oxygen species generation, transcription factor activation, and cell
adhesion molecule expression in human aortic endothelial cells. Arterioscler Thromb Vasc Biol
2003;23:1559-66.
[20] Golledge J, Muller J, Daugherty A, Norman P. Abdominal aortic aneurysm: pathogenesis and
implications for management. Arterioscler Thromb Vasc Biol 2006;26: 2605-13.
[21] Brady AR, Thompson SG, Fowkes FG, Greenhalgh RM, Powell JT. Abdominal aortic aneurysm
expansion: risk factors and time intervals for surveillance. Circulation 2004;110:16-21.
[22] Shibamura H, Olson JM, van Vlijmen-Van Keulen C, et al. Genome scan for familial abdominal aortic
aneurysm using sex and family history as covariates suggests genetic heterogeneity and identifies
linkage to chromosome 19q13. Circulation 2004;109:2103-8.
[23] van Laake LW, Vainas T, Dammers R, Kitslaar PJ, Hoeks AP, Schurink GW. Systemic dilation diathesis
in patients with abdominal aortic aneurysms: a role for matrix metalloproteinase-9? Eur J Vasc
Endovasc Surg 2005;29:371-7.
[24] Jamous MA, Nagahiro S, Kitazato KT, et al. Endothelial injury and inflammatory response
induced by hemodynamic changes preceding intracranial aneurysm formation: experimental study in
rats. J Neurosurg 2007;107:405-11.
[25] Roan JN, Yeh CY, Chiu WC, et al. Functional dilatation and medial remodeling of the renal artery
in response to chronic increased blood flow. Kidney Blood Press Res 2011;34:447-56.
[26] Hoshina K, Sho E, Sho M, Nakahashi TK, Dalman RL. Wall shear stress and strain modulate
experimental aneurysm cellularity. J Vasc Surg 2003;37:1067-74.
[27] Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and
the acute coronary syndromes (2). N Engl J Med 1992;326:310-8.
[28] Knipp BS, Peterson DA, Rajagopalan S, et al. Impaired vasoreactivity despite an increase in
plasma nitrite in patients with abdominal aortic aneurysms. J Vasc Surg 2002;35:363-7.
[29] Huang PH, Chen YH, Chen YL, Wu TC, Chen JW, Lin SJ. Vascular endothelial function and
circulating endothelial progenitor cells in patients with cardiac syndrome X. Heart 2007;93:1064-70.
[30] Bertolini F, Shaked Y, Mancuso P, Kerbel RS. The multifaceted circulating endothelial cell in
cancer: towards marker and target identification. Nat Rev Cancer 2006;6: 835-45.
[31] Parietti E, Pallandre JR, Deschaseaux F, et al. Presence of circulating endothelial progenitor cells
and levels of stromal-derived factor-1alpha are associated with ascending aorta aneurysm size. Eur J
Cardiothorac Surg 2011;40:e6-12.
[32] Schouten O, van Laanen JH, Boersma E, et al. Statins are associated with a reduced infrarenal
abdominal aortic aneurysm growth. Eur J Vasc Endovasc Surg 2006;32: 21-6.
[33] Sukhija R, Aronow WS, Sandhu R, Kakar P, Babu S. Mortality and size of abdominal aortic
aneurysm at long-term follow-up of patients not treated surgically and treated with and without statins.
Am J Cardiol 2006;97:279-80.
[34] Choke E, Thompson MM, Dawson J, et al. Abdominal aortic aneurysm rupture is associated with
increased medial neovascularization and overexpression of proangiogenic cytokines. Arterioscler
Thromb Vasc Biol 2006;26:2077-82.
[35] Finn AV, Jain RK. Coronary plaque neovascularization and hemorrhage: a potential target for
plaque stabilization? JACC Cardiovasc Imaging 2010;3:41-4.
[36] Ma ZL, Mai XL, Sun JH, et al. Inhibited atherosclerotic plaque formation by local administration
of magnetically labeled endothelial progenitor cells (EPCs) in a rabbit model. Atherosclerosis
2009;205:80-6.
[37] Franklin SS, Khan SA, Wong ND, Larson MG, Levy D. Is pulse pressure useful in predicting risk
for coronary heart disease? The Framingham heart study. Circulation 1999;100:354-60.
[38] Sho E, Sho M, Nanjo H, Kawamura K, Masuda H, Dalman RL. Hemodynamic regulation of
CD34+ cell localization and differentiation in experimental aneurysms. Arterioscler Thromb Vasc Biol
2004;24:1916-21.
[39] Coats AJ, Shewan LG. Ethics in the authorship and publishing of scientific articles. Int J Cardiol
2011;153:239-40.
Please cite this article as: Sung S-H, et al, Reduced number and impaired function
of circulating endothelial progenitor cells in patients with abdominal aortic
aneurysm, Int J Cardiol (2012), http://dx.doi.org/10.1016/j.ijcard.2012.11.002