New Patient History
advertisement

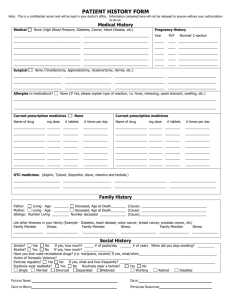
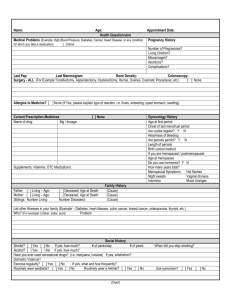
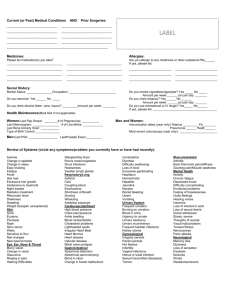
NEW PATIENT HISTORY Name: ____________________________________ Date of Birth: _________________ Age: __________ Reason for today’s visit: ________________________________________________ Date: ____________ Medical History (High Blood Pressure, Diabetes, Asthma, Cancer, Heart Disease, etc) Menstrual History None Pregnancy History Age at first menstruation Duration of bleeding (days) Number of tampons/pads a day Date of last normal period Number of days from the start of one period to the start of the next Premenstrual Symptoms? Severe Cramps? Hot Flashes? ________________ ________________ ________________ ________________ ________________ ________________ ________________ ________________ Do you think you are pregnant? Number of pregnancies (including current) Number of full term pregnancies Number of living children Any complications with pregnancies or deliveries? ____Y ____N __________ __________ __________ ____Y ____N Gynecological History What are you currently doing, if anything, to prevent pregnancy? Have you ever used birth control pills? Any complications with the pill? Have you ever had an abnormal pap smear? __________________________________________ ____Y ____N ____Y ____N ____Y ____N Surgical History (Tonsillectomy, Appendectomy, Gall Bladder, Hysterectomy, etc) Allergies to Medications? stomach, etc) None None (If yes, please explain type of reaction i.e. hives, wheezing, upset Current Prescription Medicines Name of Drug /mg dose /# tablets /#times per day Current Prescription Medicines Name of Drug /mg dose /# tablets /# times per day Over the counter medicines (Aspirin, Tylenol, Ibuprofen, Aleve, vitamins, herbals, etc) NEW PATIENT HISTORY Name: ______________________________________________________ Date: _____________ Family History Father: Mother: Siblings: Living Age: ___ Living Age: ___ Living Age: ___ Deceased, Age at Death: ___ Deceased, Age at Death: ___ Deceased, Age at Death: ___ Cause: ____________________ Cause: ____________________ Cause: ____________________ List other illnesses in your family: (Example: Diabetes, Heart Disease, Hypertension, Cancer, etc) Family Member Illness Family Member Illness Family Member Illness Social History Smoke? No Yes If yes, how much? ____# packs/day ____ # of years. When did you stop smoking? ________ Alcohol? No Yes If yes, how much? ___________________ History of Substance Abuse? No Yes Occupation: ____________________________ Marital Status (circle) Married Single Widowed Divorced Exercise routinely? No Yes If yes, what and how frequently? ______________________________________ Review of Symptoms Are you currently or have you in the past experienced any of the following symptoms? Constitutional Symptoms Comments Urinary Comments Weight change Chills Sleep Disorder Other Y N Y N Y N Eyes Double Vision Glaucoma Cataracts Other Involuntary loss of urine Urinary frequency Urinary pain Blood in urine Other N N N N Genital Y N Y N Y N Frequent infections Painful intercourse Abnormal bleeding Other Ears/Nose/Throat/Mouth Sexual Hearing changes Sore throat Sinus problems Other Change in sex drive Multiple partners STD exposure Other Y N Y N Y N Cardiovascular Chest pain Irregular heart beat Swelling in ankles Other Y Y Y Y Y N Y N Y N Y N Y N Y N Musculoskeletal Y N Y N Y N Bone pain Joint pain Muscle pain Other Y N Y N Y N NEW PATIENT HISTORY Name: ______________________________________________________ Date: _____________ Psychological Are you generally happy? Do you feel depressed Do you feel anxious? Other Comments Y N Y N Y N Endocrine Excessive thirst Too hot/cold Tired/sluggish Other Y N Y N Y N Comments Y Y Y Y N N N N Tremors Dizzy spells Seizures Other Y N Y N Y N Respiratory Y N Y N Y N Allergic/Immunologic Hay fever Drug allergies Food allergies Other Rash Lumps or Bumps Moles, skin tags Varicose veins Other Neurological Hematologic Swollen glands Blood clotting problems Bruising Other Skin Wheezing Frequent cough Shortness of breath Other Y N Y N Y N Gastrointestinal Y N Y N Y N Abdominal pain Nausea/vomiting Indigestion/heartburn Other Y N Y N Y N Physician/provider signature: _________________________________________ Date: _______ Reviewed/Updated:_____________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________ ______________________________________________________________________________