Rheumatoid arthritis ( RA ) is a chronic systemic autoimmune
advertisement
 is a chronic systemic autoimmune")
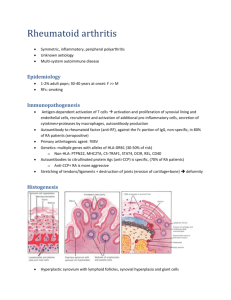
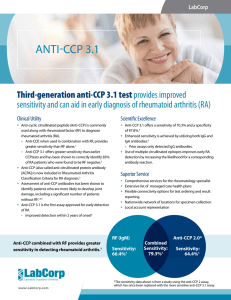
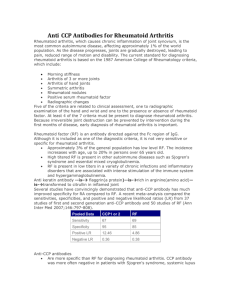
Administrative Office St. Joseph's Hospital Site, L301-10 50 Charlton Avenue East HAMILTON, Ontario, CANADA L8N 4A6 PHONE: (905) 521-6141 FAX: (905) 521-6142 http://www.fhs.mcmaster.ca/hrlmp/ Issue No. 85 QUARTERLY NEWSLETTER February 2006 Anti-Cyclic Citrullinated Peptide ( Anti-CCP ) Rheumatoid arthritis ( RA ) is a chronic systemic autoimmune disease that causes inflammation, stiffness, pain and destructive changes in the hands, feet and other joints in the body. It is the most frequent autoimmune rheumatic disease affecting approximately 1 - 2 % of the population in North America. While the etiology of the disease remains unknown, several risk factors have been identified. The disease occurs more frequently in females than in males( 3:1 ratio). Genetic studies have demonstrated that a genetic predisposition resides in the HLA-DR Locus. There are studies which demonstrate that environmental factors, such as smoking, oral contraceptives and infectious agents may play a role. Although RA is diagnosed primarily according to clinical manifestations, it has been demonstrated that the serum of patients with RA contains a spectrum of autoantibodies. However these autoantibodies are not specific for RA and may be detected in other autoimmune conditions. These antibodies include Rheumatoid factor (RF), Anti - RA33 antibodies, Anticalpastin, Sa Protein, heavy Chain Binding Protein (p68), Glucose-6-phosphate Isomerase, Antifilaggrin antibody and Anti Cyclic Citrullinated Peptide, (AntiCCP). Rheumatoid factor has been the serological test used to aid in the diagnosis of rheumatoid arthritis and to distinguish it from other arthritic and inflammatory conditions for over 75 years. The sensitivity of RF for Rheumatoid Arthritis has historically been very good, > 98%, but it has always had low specificity, approximately 60% and has been demonstrated in healthy elderly individuals, immunized subjects and in patients with other auto immune diseases and chronic infections. A new serological test, the Anti-Citrullinated Cyclic peptide (Anti-CCP), was developed in 1998. It has been reported to have equivalent sensitivity to RF, but demonstrates greater specificity for the diagnosis of RA, particularly in patients with early disease. Citrulline is an amino acid formed by post-translational modification of arginine residues. The arginine residues are converted into citrulline by the enzyme peptidylarginine deiminase. Anti-CCP for Diagnosis Antibodies directed against Citrullinated proteins appear to provide a useful serological marker for the diagnosis of RA during the early stages of the disease when not all clinical symptoms are present. The most sensitive assay to detect these antibodies is the Anti-CCP ( IgG)Elisa assays. The current literature indicates that the Anti-CCP antibodies have essentially the same Sensitivity as the Rheumatoid Factor for RA, (77% vs. 74% in one study), while Anti-CCP demonstrates greater Specificity, (97% vs. 78%). Results from a review by Vossenaar et al1 are summarized below. 2x2 Tables of Diagnostic Performance of Anti-CCP and RF1 Rheumatoid Arthritis Pos Neg Pos 865 79 Neg 252 2218 Anti-CCP Rheumatoid Arthritis Rheumatoid Factor Pos Neg Pos 827 374 Neg 292 1294 Overview of CCP and RF sensitivity (%), specificity (%) and likelihood ratios (95% CI)1 Sensitivity Specificity LR Pos LR Neg Anti-CCP 77 (74 - 79) 96 (95 - 97) 22.5 (18 - 28) 0.23 (0.21 - 0.26) RF 73 (71 -76) 77 (75 - 79) 3.2 (2.9 - 3.6) 0.34 (0.30 - 0.37) Anti-CCP is Present in Early Disease Recent studies (summarized in review by Vossenaar1) provide evidence that Anti-CCP may be present in the plasma of Rheumatoid Arthritis patients before the onset of clinical symptoms and before the appearance of IgM-RF. Anti-CCP detects more positive subjects, longer before the onset of clinical symptoms and with greater specificity than IgM-RF. Anti-CCP Predicts Erosive Disease Anti-CCP antibodies are able to predict erosive and progressive disease. A prospective study by Vencovsky et al4 measured baseline levels of several autoantibodies. They report that differences in disease progression were detected by, amongst others, the presence of Anti-CCP antibodies. The best prediction was obtained by combined analysis of Anti-CCP and IgM-RF. Anti-CCP (IgG) ELISA Assay Sample: 0.5 mL Serum (only). <8 h room temperature, 8 - 48 h 2º - 8º C, > 48 h freeze -20º C Reference Interval: Negative: < 20 U/L Weak Positive: 20 - 39 U/L Positive: 40 - 59 U/L Strong Positive: >= 60 U/L Anti-CCP values obtained with different manufacturers' assay methods may not be used interchangeably. The magnitude of the reported IgG levels cannot be correlated to an end point titre. The Hamilton Regional Laboratory Medicine Program began offering this test in 2005. References: 1. Vossenaar ER, Van Venrooij WJ. Anti -CCP antibodies, a highly specific marker for (early) rheumatoid arthritis. Clinical and Applied Immunological Reviews 4, 239 - 262, 2004. 2. Nijenhuis S, Zendman AJW, Vossenaar ER et al. Autoantibodies to Citrullinated proteins in rheumatoid arthritis: clinical performance and biochemical aspects of an RA specific marker. Clinica Chimica Acta 350, 17-34, 2004. 3. Van Boekel MMA, Vossenaar ER, Van den Hoogen, FHJ. Auto antibody systems in rheumatoid arthritis: specificity, sensitivity and diagnostic value. 4. Vencovsky J., Machá ek S, edová L, Kafková J, Gatterová J, Pe áková V and R i ková . Autoantibodies can be prognostic markers of erosive disease in early rheumatoid arthritis. Ann Rheum Dis. 2003:62 427430 Mark Donahoe, BSc, ART, Manager Stephen Hill, PhD, FCACB, Clinical Biochemist Discipline of Special Chemistry/Immunology