to open the MS Word version of the Quarterly Action Agenda
advertisement

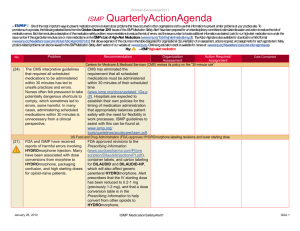
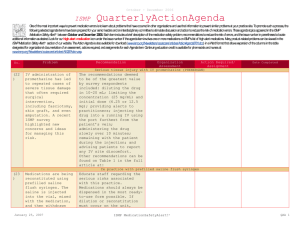
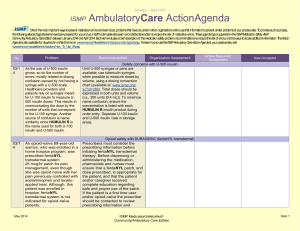
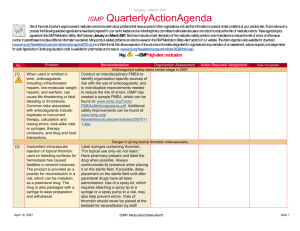
July - September 2013 ISMP QuarterlyActionAgenda One of the most important ways to prevent medication errors is to learn about problems that have occurred in other organizations and to use that information to prevent similar problems at your practice site. To promote such a process, the following selected items from the July-September 2013 issues of the ISMP Medication Safety Alert! have been prepared for an interdisciplinary committee to stimulate discussion and action to reduce the risk of medication errors. Each item includes a brief description of the medication safety problem, a few recommendations to reduce the risk of errors, and the issue number to locate additional information as desired. Look for our high-alert medication icon under the issue number if the agenda item involves one or more medications on ISMP’s List of High-Alert Medications (www.ismp.org/Tools/highalertmedications.pdf). The Action Agenda is also available for download in a Microsoft Word format (www.ismp.org/Newsletters/acutecare/articles/ActionAgenda1304.doc) that allows expansion of the columns in the table designated for organizational documentation of an assessment, actions required, and assignments for each agenda item. Many product-related problems can also be viewed in the ISMP Medication Safety Alert! section of our website at: www.ismp.org. Continuing education credit is available for nurses at: www.ismp.org/Newsletters/acutecare/actionagendas.asp. Key: No. Problem (16) A 15-month-old child who had been sleeping with his mother gained access to her fentaNYL patch, ingested it, and was found unresponsive when his mother awoke. He later died. Similar events prior to this have been just as tragic, yet little has been done to assure patient education about proper use and storage of fentaNYL patches. Until every healthcare professional and health system accepts personal responsibility for promoting safe use of this drug, we are exposing one of the most troubling examples of bystander apathy in healthcare: a belief that we don’t need to intervene because others will. (18) —ISMP high-alert medication Organization Assessment FentaNYL patch fatalities linked to “bystander apathy” Recommendation Action Required/ Assignment Date Completed No patient should walk out of a doctor’s office, hospital, clinic, or pharmacy without face-to-face instructions on the use of fentaNYL patches and related safety concerns. All health professionals must individually instruct patients and caregivers and not rely on others to do it. ISMP has developed a FREE patient education checklist and consumer leaflet for use during consumer education that can then be given to the patient for reference (download the checklist/leaflet at: www.ismp.org/AHRQ/default.asp [must register for initial access]). Death and neurological devastation when IV vinca alkaloids are given intrathecally Results from the ISMP International Dispense IV vinca alkaloids in a minibag of Medication Safety Self Assessment for a compatible solution and never dispense Oncology revealed that only 54% of US and/or administer these drugs using a hospitals dispense vinCRIStine in a minibag syringe. Prohibit IV vinca alkaloids in areas of compatible solution to prevent accidental where intrathecal medications are intrathecal administration. To date, there are administered and/or stored. Confirm that 120 published cases of administration of any prescribed intrathecal medications vinCRIStine by the intrathecal route when the have been administered before dispensing drug was dispensed in a syringe, and zero IV vinca alkaloids. For more cases when dispensed in a minibag. Most recommendations, visit: www.ismp.org/ events were related to mistaking IV newsletters/acutecare/showarticle.asp?id= vinCRIStine for an intrathecal medication 58. (e.g., methotrexate, cytarabine). October 3, 2013 ISMP MedicationSafetyAlert! QAA 1 July - September 2013 ISMP Problem No. (14) (19) QuarterlyActionAgenda Organization Assessment Recommendation Action Required/ Assignment Date Completed Stock ketamine in a lower concentration (10 mg/mL) in the emergency department (ED) A pediatric patient received a 10-fold In the ED, ketamine is often administered IV, overdose of ketamine in the ED. A small so a lower concentration (10 mg/mL) should volume (0.175 mL) of ketamine (100 mg/mL) be stocked. Concentrated ketamine products, was needed for the child’s dose. The nurse which result in lower dosing volumes, may be doubted that such a small volume was more appropriate for IM or intranasal (offneeded and drew up 1.75 mL, which he label) use since larger doses are needed with considered to be a more “normal volume.” these routes. Automated maximum dose alerts with hard stops for amphotericin B, methotrexate, and fentaNYL ISMP has often written about mix-ups Design hard stops in order entry between conventional and lipid-based computers for doses of conventional amphotericin B, accidental daily dosing of oral amphotericin B greater than 1.5 mg per kg methotrexate, and dosing errors with IV or catastrophic limits, and for daily dosing fentaNYL. Recent errors with these drugs led of oral methotrexate without a stop date to the death of a patient who received after 5 days or less. Program hard stops in conventional amphotericin B in a dose for the smart infusion pumps to detect pump lipid-based product, and serious injuries to programming errors that would lead to two toddlers—one of whom received catastrophic doses with fentaNYL. The methotrexate daily for 7 days and the other intent is to halt the process or allow for a an IV fentaNYL overdose after a pump brief period of investigation to ensure misprogramming error. safety. (16) Experts agree that hepatitis B can be eliminated in the US with proper vaccination. Yet, one in three newborns leaves the hospital without receiving this vaccination, and 800 become infected with hepa-titis B each year because of perinatal exposure. Help end hepatitis B by vaccinating newborns Ensure that hepatitis B vaccine birth doses are included in standard order sets, universally administered before hospital discharge, and that proper follow-up occurs with a total of 3 or 4 doses at properly spaced intervals. (14) A pharmacy technician mixed 0.27 mL of a diluent with 5.13 mL of magnesium sulfate, mixing up the volumes required (0.27 mL magnesium, 5.13 mL diluent). The syringe Syringe pull-back method of verifying IV admixtures unreliable ISMP’s compounding safety guidelines strongly dis-courage the syringe pull-back method of verifying the contents of admixtures, particularly for compounded sterile products October 3, 2013 ISMP MedicationSafetyAlert! QAA 2 July - September 2013 ISMP Problem No. QuarterlyActionAgenda Organization Assessment Recommendation Action Required/ Assignment Date Completed pull-back method was used for checking the admixture, so the error went unnoticed because it was not clear which syringe was associated with which vial. The syringe pull-back method for checking admixtures is unreliable. (17) with high-alert drugs (www.ismp.org/sc?id=251). The contents of these solutions should be verified immediately before adding them to the diluent, and syringes should be labeled if verification is not completed shortly after drawing the solution into the syringe. Developing productive partnerships with technology and device vendors to improve staff training Staff training is critical to optimize the use of Work collaboratively with technology vendors new technology, employ all its safety features, to deliver initial staff training and periodic and prevent misuse that might lead to errors. follow-up training. Make sure your purchasing But users rarely read the vendors’ directions agreement clearly details the training to be for use, and organizations may not have the provided. Develop written expectations to set depth of knowledge to teach staff how to the ground rules (e.g., no marketing beyond properly use the technology. Users tend to agreed scope). Conduct a failure mode and first learn what they need to know to do their effects analysis and use the results to plan the jobs, and then all that is feasible with the training. All training should be coordinated by technology. This second wave of training also the pharmacy or nurse educators in may be more effective when partnering with collaboration with the vendor. the vendor. Dinoprostone dosage forms (PROSTIN E2 and CERVIDIL) confused (17) A PROSTIN E2 20 mg vaginal suppository was cut in half and used in place of a CERVIDIL 10 mg vaginal insert intended to promote cervical ripening in a pregnant women. The Cervidil insert provides a gradual release of the drug and can be removed. The suppositories, which cause tetanic contractions, are used to evacuate uterine contents after a missed abortion or fetal death. In this case, fetal heart deceleration led to an emergency C-section. (14) Certain procedures performed in utero may require administering drugs directly to the Prostin E2 should not be available on nursing units and should only be dispensed from the pharmacy after the indicated use has been verified. Staff who might encounter pregnant women should be warned that, although the generic name for both products is the same, Prostin E2 should only be used for intrauterine fetal death and termination of pregnancy, not for cervical ripening. In utero medication administration to fetus presents unique safety challenges October 3, 2013 Establish a process for prescribing fetal medications (e.g., temporary record, ISMP MedicationSafetyAlert! QAA 3 July - September 2013 ISMP QuarterlyActionAgenda Organization Assessment Problem Recommendation fetus. Because the fetus may not have a medical record, drugs intended for the baby are sometimes ordered on the mother’s chart. In preparation for an intrauterine transfusion to a fetus, a neuromuscular blocking agent was ordered for the fetus to keep the baby still. The medication, which had been ordered on the mother’s chart, was administered IV to the mother, leading to respiratory arrest. The mother died and the infant sustained CNS impairment. generic record for Baby Doe using the mother’s identifier). Avoid prescribing fetal drugs on the mother’s record. Develop order sets for fetal medications. Pharmacy preparation and labeling should make it clear that the drug is intended for the fetus. Require a “time-out” process to verify all information before fetal drug administration. No. (18) Errors involving 10-fold topotecan overdoses have been reported. Several of these errors have occurred because the decimal point in the dose was overlooked (e.g., “.7 mg” dose misread as 7 mg; “2.5 mg” dose misread as 25 mg) or because a trailing zero was used after a whole number dose (“4.0 mg” misunderstood as 40 mg). Avoiding topotecan 10-fold overdoses Always include a leading zero (e.g., 0.7 mg) and avoid using trailing zeros (e.g., 2 mg, not 2.0 mg) when expressing doses. Include the intended dose in mg/m 2 and the total calculated dose to allow other clinicians to verify the dose. Consider the use of standardized order sets to avoid topotecan dosage confusion. (16) Several bleeding reversal products have been referred to as “Prothrombin Complex Concentrate” or “PCC,” but there is a new product, KCENTRA, with the proper name of Prothrombin Complex Concentrate. The use of “Prothrombin Complex Concentrate” or “PCC” may result in confusion regarding which drug is intended. Confusion a “factor” with “PCC” orders Determine which of these reversal products will be on the formulary and educate staff about each agent and the risk of confusion when using the terms “Prothrombin Complex Concentrate” or “PCC.” Always clarify orders for “Prothrombin Complex Concentrate” or “PCC” in order to determine the specific brand name. (15) Action Required/ Assignment Date Completed FLEET ENEMA SALINE (dibasic and monobasic sodium phosphate) contains phosphates, not plain saline Fleet Enema Saline contains sodium Avoid Fleet enemas in elderly patients with October 3, 2013 ISMP MedicationSafetyAlert! QAA 4 July - September 2013 ISMP (19) Organization Assessment Problem Recommendation phosphate monohydrate 19 g and dibasic sodium phosphate 7 g. Because the label states “saline,” the phosphate content may be overlooked. Phosphate toxicity is possible from even a single enema, although elderly patients with renal insufficiency, those using more than one enema per 24 hours, and patients with decreased intestinal motility are more at risk. renal insufficiency and those with diseases that slow intestinal motility. When used for other patients, the enema should be immediately expelled, and a second dose within 24 hours should not be administered. Patients should be warned to carefully follow label directions and to avoid using more than one enema in 24 hours. No. (15) QuarterlyActionAgenda Action Required/ Assignment Date Completed Protecting vulnerable patients during handoffs to long-term care (LTC) Medication errors in a LTC facility often Establish a list of drugs that are often not originate in the hospital. For example, continued after hospitalization and refer to the unnecessarily including the strength of insulin list during discharge medication reconciliation (100 units per mL) without the actual dose on to determine if clarifications are needed. a transfer form led a LTC nurse to Require prescribers to verify transcribed misunderstand a new resident’s dose as 100 discharge sum-maries, and coordinate units, which led to his death. Studies show completion of the transfer/ referral form with inconsistencies between medications on the discharge summary to ensure discharge summaries and transfer forms, consistency. Have pharmacists review the leading to error rates of 21% or more during prescribed medications for patients being transitions between hospitals and LTC, transferred to LTC facilities. particularly with warfarin, insulin, opioids, and cardiovascular drugs. Pump resumes patient-controlled analgesia (PCA) dosing when turned off then on again A young patient was transitioned from If you use these pumps, disconnect the morphine PCA, using a CADD-Solis patient from the pump and/or remove the Ambulatory Infusion Pump, to medication cassette if PCA is discontinued. oxyCODONE as needed for pain. The Another option is to reset the PCA dose and nurse stopped the infusion and turned the continuous infusion rate to “zero” prior to pump off, but left the patient connected in shutting off the pump, so if it is turned back case the transition from PCA was not on, a security code is needed to modify the tolerated. These pumps do not feature an pump settings. You can also remove the auto-lock function, allowing the patient to battery pack, although this option may lead to turn the pump back on and administer lost batteries and delayed therapy. bolus doses every 15 minutes. Drug shortage leads to preparation of wrong strength of levothyroxine (14) A pharmacy was unable to obtain vials of October 3, 2013 Hospitals should have a plan in place for ISMP MedicationSafetyAlert! QAA 5 July - September 2013 ISMP QuarterlyActionAgenda Organization Assessment Problem Recommendation levothyroxine 500 mcg and ordered 100 mcg vials instead. Upon reconstituting the drug with 5 mL, a tech-nician failed to notice the strength and prepared the drug as usual. He labeled the vial as containing 100 mcg/mL but it contained 20 mcg/mL. how product replacements are used during a shortage, and how changes are communicated to staff. For additional strategies to avoid errors during drug shortages, visit: www.ismp.org/ Newsletters/acutecare/articles/20101007.a sp. No. October 3, 2013 ISMP MedicationSafetyAlert! Action Required/ Assignment Date Completed QAA 6