mandibular injuries
advertisement

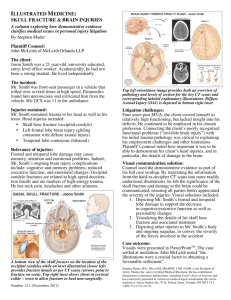
MANDIBULAR INJURIES DISLOCATION: Anterior Extreme opening eg yawn/laughter, large bite, oral sex, GA, tonsillectomy Other types Require traumatic injury Muscle spasm then traps mandible out of position Temporalis, pterygoid, masseter Risks: Shallow glenoid fossa Increased muscle tone (including dystonic reactions) Loss of joint capsule (previous trauma) Hyper-mobility: Marfan’s, Ehlers-Danlos Unilateral – jaw deviates to opposite side Bilateral – more common Anterior – most common Posterior – rare, direct blow, condylar head may prolapse into ext auditory canal Lateral – often associated with # Superior – blow to partially open mouth, condylar head upward, assoc with cerebral contusions, facial nerve palsy, deafness Clinical: Pain Mal-occlusion Drooling Speech/swallowing difficulty Unilateral – jaw deviates to opposite side (NB bilateral more common) Anterior: pre-auricular depression Posterior – examine ext auditory canal, check hearing Lateral- always signs of # Superior – check for head/neck/CNS injury Investigations Spontaneous, anterior, atraumatic – clinical Dx OPG usually suffices More trauma/suspicion of head injury – CT DDx Fracture Haemarthrosis TMJ Locking of TMJ TMJ dysfunction Complications: Recurrent dislocation Ear/auditory canal injuries C-spine/head injuries Dental injuries Nerve injuries – facial, mandibular Treatment: (after # excluded0 Analgesia Reduction under sedation Can try: Local anaesthetic injected into joint space 2ml of 2% lignocaine Reduction: 1) Sitting: Gloved thumbs over molars, fingers supporting body Downward & backward pressure, slight opening may help 2) Supine Standing behind patient Gloved thumbs over molars, fingers supporting body Downward & backward pressure May wrap gauze around thumbs in case masseter spasm causes clenching on reduction Post-reduction xrays not required if Atraumatic reduction Able to open/close mouth without significant pain Complications of reduction – rare Fracture Avulsion of articular cartilage Disposition: Uncomplicated Anterior Discharge post reduction Soft diet for 2 weeks (& Avoid opening mouth > 2cm) Support mandible with hand when yawning NSAIDS Maxillofacial review as outpatient Recurrent dislocations may require operation Comlications: refer to Facio-maxillary surgeon urgently Open Superior Fracture Nerve injury Irreducible FRACTURE Usually traumatic – assaults/falls 2nd most common facial fracture (after nose) Ring shape – often multiple #’s Associated injuries: Head/c-spine # temporal bone ) from transmitted force Perforated eardrum ) Dental injuries Nerve injuries – facial, mandibular Clinical: Pain Mal-occlusion Drooling Gingival lacerations (may be hidden between teeth) Ecchymosis under tongue – sensitive for mandible # Signs of associated injuries – dental, nerve, head, c-spine Investigations OPG: Orthopantomogram PA/oblique xrays “Towne view” xray – limited to condyle/neck CT – if high suspicion but xrays NAD (especially condylar #) Treatment: consult with Facio-Max Open Fractures Admission IV antibiotics Closed fractures May be Mx as outpatients