Referral Form - Suffolk Community Healthcare
advertisement

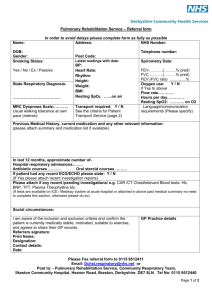
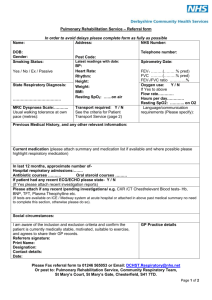
Pulmonary Rehabilitation Referral Form Date of referral: Thank you for referring your patient to Pulmonary Rehabilitation provided by Suffolk Community Healthcare. Criteria for referral to Pulmonary Rehabilitation The patient must have the following: Confirmed diagnosis of COPD which is being optimally treated Patient Details Name: Address: The following conditions will exclude someone from a rehabilitation programme: Severe musculoskeletal conditions MI within last 6 weeks Uncontrolled hypertension Unstable angina Acute LVF Uncontrolled cardiac arrhythmias Aortic stenosis Uncontrolled diabetes NHS no: CRN no: DOB: Tel no: Mobile no: GP Details: Relevant Medical History/co-morbidities: Date spirometry performed: FEV1: FVC: FEV1/FVC: Current Medication (FP10 may be attached) SpO2 on air on LO 2 Oxygen therapy No LTOT SBOT AO Exercise tolerance: Additional information: Person referring: Contact details: Signer/interpreter required (please specify): Position: Tel no: Please return this form to: Suffolk Community Healthcare, Care Coordination Centre Fax 01473 276470/1/2/3/4 We will contact the patient to arrange an assessment. October 2013