ordered
advertisement

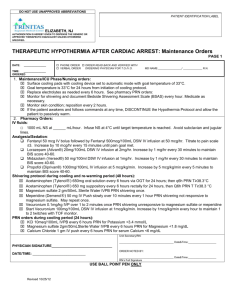
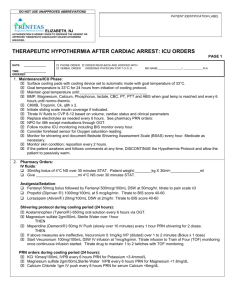
DO NOT USE UNAPPROVED ABBREVIATIONS PATIENT IDENTIFICATION LABEL ELIZABETH, NJ AUTHORIZATION IS HEREBY GIVEN TO DISPENSE THE GENERIC OR APPROVED THERAPEUTIC EQUIVALENT UNLESS OTEHRWISE SPECIFIED. THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST: Initial Orders PAGE 1 DATE: _______________ PHONE ORDER ORDER READ BACK AND VERIFIED WITH VERBAL ORDER ORDERING PHYSICIAN FOR T.O./V.O. MD NAME:________________/ _____________ R.N. TIME: _______________ ORDERED 1. Inclusion criteria: Age ≥ 18 yrs. ROSC within 60 minutes of starting effective CPR and within 12 hours of event Comatose/unresponsive/no purposeful movement (GCS ≤ 8) Ventilator dependent 2. Exclusion criteria: ROSC after 60minutes from starting effective CPR or more than12 hours after event Purposeful movement; follows simple commands Baseline impaired cognitive function DNR status End-stage terminal illness Coma unrelated to arrest (sepsis, CVA, intoxication, ICH, SAH) Uncontrollable bleeding Major head trauma or significant trauma, especially intra-abdominal Initial temperature <30° C 3. Determine if patient requires emergent cardiac cath. If yes, initiate STEMI protocol. 4. Determine if patient requires emergent CT scan to R/O ICH or PE. If yes, STAT CT scan 5. Initiate Code Frosty. Notify Sharing Network if patient meets referral triggers. 1-800-541-0075. 6. Initial management: ■ Toxicology screen ■ Baseline lab studies STAT: ■ EKG ■ Complete metabolic panel ■ Chest X-ray ■ CBC, PT, PTT ■ Insert Foley catheter ■ Type and screen ■ Insert OG tube ■ Troponin, CKMB, CK , BNP ■ Establish IV access: peripheral or central. ■ Lactate ■ Implement Ventilator order set ■ UA, urine pregnancy ■ Insert radial arterial line, if feasible ■ ABG’s 7. Cooling Implementation/Nursing orders: Ice bags: to neck, axilla, and groin; replace as needed; remove when goal temp is reached. Insert temperature probe; record temperature every 30 minutes until therapeutic temperature is reached. Apply surface cooling pads and set to automatic mode to goal temperature of 33° C. Vital signs every 15minutes x 1hour; then hourly. Start analgesia and sedation on initiation of cooling. Unit Secretary/RN: PHYSICIAN SIGNATURE________________________________ DATE/TIME: ____________________________ _____________________________________ Date&Time:___________________ ORDER NOTED BY: _____________________________________ Date&Time:___________________ RN’s Full Signature USE BALL POINT PEN ONLY Revised 10/25/2012 DO NOT USE UNAPPROVED ABBREVIATIONS PATIENT IDENTIFICATION LABEL ELIZABETH, NJ AUTHORIZATION IS HEREBY GIVEN TO DISPENSE THE GENERIC OR APPROVED THERAPEUTIC EQUIVALENT UNLESS OTEHRWISE SPECIFIED. THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST: Initial ORDERS PAGE 2 DATE: _______________ PHONE ORDER ORDER READ BACK AND VERIFIED WITH VERBAL ORDER ORDERING PHYSICIAN FOR T.O./V.O. MD NAME:________________/ _____________ R.N. TIME: _______________ ORDERED 8. Pharmacy Orders: IV fluids: 30 mL/kg bolus of 4°C NS over 30 minutes STAT. Patient weight:________kg X 30 mL/kg=______________mL Give ____________________mL 4°C NS over 30 minutes STAT. Analgesia/Sedation: Fentanyl 50 mcg IV bolus followed by Fentanyl 500mcg/100mL D5W IV infusion at 50 mcg/hr. Titrate to pain scale ≤3. Increase by 10 mcg/hr every 15 minutes until pain goal met. Lorazepam (Ativan®) 20mg/100mL D5W IV infusion at 2mg/hr. Increase by 1 mg/hr every 30 minutes to maintain BIS score 40-60. Midazolam (Versed®) 50 mg/100ml D5W IV infusion at 1mg/hr. Increase by 1 mg/hr every 30 minutes to maintain BIS score 40-60. Propofol (Diprivan®) 1000mg/100mL IV infusion at 5 mcg/kg/min. Increase by 5 mcg/kg/min every 5 minutes to maintain BIS score 40-60. Shivering protocol during cooling and re-warming period (48 hours): Acetaminophen (Tylenol®) 650mg oral solution every 6 hours via OGT for 24 hours; then q6h PRN T≥38.3°C Acetaminophen (Tylenol®) 650 mg suppository every 6 hours rectally for 24 hours, then Q6h PRN T T≥38.3 °C Magnesium sulfate 2 gm/50mL Sterile Water IVPB PRN shivering once. Meperidine (Demerol®) 50 mg IV Push slowly over 10 minutes every 1 hour PRN shivering not responsive to magnesium sulfate. May repeat once. Vecuronium 0.1mg/kg IVP over 1 to 2 minutes once PRN shivering unresponsive to magnesium sulfate or meperidine Start Vecuronium 100mg/100mL D5W IV infusion at 1mcg/kg/min. Increase by 1mcg/kg/min every hour to maintain 1 to 2 twitches with TOF monitor. 9. Other Orders Unit Secretary/RN: _____________________________________ Date&Time:___________________ PHYSICIAN SIGNATURE________________________________ DATE/TIME: ____________________________ ORDER NOTED BY: _____________________________________ Date&Time:___________________ RN’s Full Signature USE BALL POINT PEN ONLY Revised 10/25/2012