Child Profiling Discussion Paper
advertisement

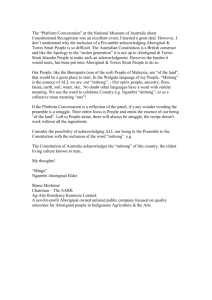
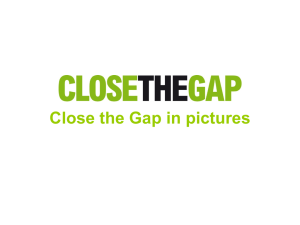
Community Services Directorate Child Profiling Discussion Paper March 2014 Contents 1. Purpose ....................................................................................................................................... 3 2. Background ................................................................................................................................. 3 3. Child Profiling Tool ...................................................................................................................... 3 4. Validation .................................................................................................................................... 5 5. Results ......................................................................................................................................... 6 6. Discussion.................................................................................................................................. 10 7. Conclusion ................................................................................................................................. 13 Attachment A: Child Complexity Tool – Jurisdiction Analysis ........................................................... 15 Attachment B: Complexity Assessment Tool (CAT) .......................................................................... 18 Attachment C: Counting Rules .......................................................................................................... 22 Attachment D: Case Study ................................................................................................................ 23 Attachment E: Reference list ............................................................................................................ 26 2 1. Purpose The purpose of the Child Profiling project was to gain a population measure of all children and young people in out of home care in respect to their current levels of need and the complexity of their behaviours. The project is a key deliverable to develop the five year Out of Home Care Strategy (Strategy) and the findings will be used to design future service models and interventions. Further discussions about the results will be held throughout the course of the Strategy’s development in order to deliver a more targeted and individualised system that best meets the needs of children and young people in the ACT. The paper also seeks to explain the methodology utilised to complete the project and provide a baseline for future research to ensure the out of home care system adapts to the population over time. 2. Background The Child Profiling project was part of a suite of research and data activities undertaken to inform the development of the Strategy. The project aimed to address the limited understanding about the needs and behaviours of children and young people in out of home care as a population group. It was recognised individual children and young people are assessed regularly through case planning activities however there were limited assessments, other than for national reporting requirements, to look at the out of home care population as a whole. Furthermore, national reporting often looks at outputs and activity based reporting through quantitative data, this project sought to look qualitatively at the needs of children in care and what conclusions might be drawn from the findings about their needs when mapped against some basic demographic information. 3. Child Profiling Tool The child profiling project started in May 2013 and was undertaken by two Care and Protection Services senior practitioners. At the start of the project the purpose was: • To identify a tool that could be used to create a profile of children and young people in out of home care. The data would aim to reflect relative levels of need and complexity by percentage of population. The data would support the development of the Out of Home Care Strategy. • Gain a population measure of all children and young people in care according to their level of behavioural complexity and needs. In order to meet the first purpose Australian jurisdictions were contacted to ascertain if they conducted any child profiling assessments. An overview of feedback from other jurisdictions is provided in a report at Attachment A. The findings from the analysis recommended the use of the Complexity Assessment Tool (CAT) which was authored by Professor Paul Delfabbrio for Families SA. Families SA agreed to give the ACT permission to use the tool for their analysis. The CAT is at Attachment B. The CAT is a standardised screening instrument for assessing the complexity of children and young people and was developed for Families SA to use when children and young people enter out of home care, when they change placement, at the time of the Annual Review and when there is a review of the carers subsidy. 3 The CAT is split into the following components: Part A: Children’s behavioural complexity • Substance use • Sexualised behaviour • Offending behaviour • School behaviour • General behaviour Part B: Children’s special needs • Physical health • Child development and intellectual health • Mental health • Physical disability For each component the assessor scores the child or young person using a severity rating (A-E), the score is assessed using a guide that describes behaviours a child would exhibit to be considered for each severity rating. A formula is then used to add the severity ratings together to provide a single assessment score in one of the following levels: • Level 1: Minor or no problems • Level 2: Moderate problems • Level 3: Significant problems • Level 4: Extreme problems South Australia identified the range of supports needed to assist children and young people in the various levels. These supports ranged from interventions for the child, the placement or the carer. In terms of children assessed at a level 1 their needs were identified as those similar to the general population and included needs such as food, clothing, shelter, safety, love, nurturance, stability, spirituality, educational, psychological and maintained connections with families. Level 1 children needed an environment that is consistently responsive, nurturing and has a therapeutically supportive parenting environment. The carer is expected to act as any other parent and attend meetings, routine appointments and facilitate social, recreational and cultural activities. Children who were assessed at a level 2 were identified as displaying more challenging behaviours, may have moderate developmental delays, disability or have additional health needs. The additional needs for the child may include additional supervision, additional educational support (tutoring, classroom support), therapeutic interventions and more frequent care planning reviews and assessments. These additional needs mean the carers should be more on hand to participate in various meetings and reviews and be generally more available to the child or young person. Children who were assessed at a level 3 were identified as having a significant level of challenging behaviour that placed themselves or others at risk and/or they have significant developmental delays, disability and health or educational issues. The aim of the placement would be to assist the child’s recovery and help them to gain stability in relation to the management of their behaviours. A child in this level would need close supervision, alternative or structured educational programs, developmental programs, ongoing assessments and often have an emergency safety plan. A carer of 4 a child in level 3 would need to maintain close communication with their case worker, participate in intensive therapeutic intervention plans and implement the emergency safety plan. Children who were assessed at a level 4 were identified as having severe developmental delays, disability and health or educational issues and/or whose behaviours place themselves or others at extreme risk of significant harm. The aim of the placement would be to assist recovery in the child or young person and enable them to function in a less intensive/restrictive environment. Carers of these children would need to offer intensive supervision, monitoring and highly structured activities. Carers would need to be available to attend all appointments, maintain close communication with their case worker, implement the emergency safety plan and facilitate connection to a less restrictive environment. The South Australian system operates on the premise that all carers for children and young people in out of home care should offer a therapeutically supportive parenting environment. At 25 June 2013, there were 578 children and young people residing in out of home care in the ACT. However, from this total number 102 were assessed as not meeting the criteria to be included in the profiling exercise. Therefore, a total of 476 children and young people were assessed for the purposes of this project. Reasons for children and young people not being assessed included children subject to an Enduring Parental Responsibility Order, young people who had self placed with birth family and children and young people who were going through an active reunification process at the time of the assessment. The following criteria were applied for inclusion: • Residing in out of home care including, residential, foster care, kinship care, living independent or in a refuge; and • Were in the full or shared care of the Director-General; and • Were under the age of 18 years at 25 June 2013. A full list of the counting rules is at Attachment C. At the same time the assessor completed the CAT the following data was collected: • • • • • • • • • • • • • • Name; CHYPS ID; Date of Birth; Aboriginal and Torres Strait Islander status; Cultural background; Placement type; Gender; Number of siblings; Number of siblings in care; Length of Order; Age at assessment; Age child came into care; CAT level; and Current subsidy level. 4. Validation There were limitations to the way the assessments were conducted. The assessments were based on the opinion of two senior practitioners conducting the project and heavily relied on the quality of 5 documents used about the child or young person. The main documents used for the assessment were the Annual Review, Care Plan and/or Child Protection Assessment Report (CPAR). The senior practitioners undertook a range of processes to provide additional validity to the project. The processes included: 1. the senior practitioners undertook random samples of each other’s assessments; 2. the senior practitioners verified 127 assessments with caseworkers and there were only two instances where the caseworker recommended a higher or lower complexity level; and 3. the senior practitioners asked caseworkers to identify the children or young people they thought would be in level 3 and 4 and reassessed these children. Following the third validation exercise the level of need rating was adjusted for 13 per cent of children. These changes have compromised the validity on this small cohort of the project somewhat as the senior practitioner in the third validation sought information from a wider range of sources than what was used in the original assessment. The wider range of documents included affidavits, Child at Risk Health Unit (CARHU) reports and agency reports. The quality of all the documentation used for the assessments was highly variable and when additional documents were reviewed it was clear to see the story of the child or young person was a lot more complex that what is often portrayed in an Annual Review or Care Plan. A finding for the next evaluation will be to use a consistent document that is more holistic in nature and includes results of standardised testing. 5. Results For most of the analysis presented, those with levels of need above minor are considered as a single group. This is because of the low number of children with higher levels of need. The main findings from the analysis include: Level of need A total of 476 children and young people were assessed as they presented at 25 June 2013. The numbers of children and young people in care was non-linear in terms of declining numbers through the four levels. Table 1: Level of need Data Item Group Number Level 1: Minor Level of need Percent* 382 80.3 Level 2: Moderate 46 9.7 Level 3: Significant 22 4.6 Level 4: Extreme 26 5.5 * These figures do not add to 100% because they were rounded up. Sex 6 There were more males 258 (54.2%) than females 218 (45.8%) in the assessment. Cultural background There were 44 children and young people (9.2%) from culturally diverse backgrounds. The children were identified as culturally from 18 different countries. The highest proportion of children came from countries in Europe with the exception of Sudan. Placement Type The majority of children and young people were placed in kinship care 257 (54%). There were 183 (38.5%) children and young people in foster care and 36 (7.6%) in residential care or living independently. Children in kinship care were less likely to be identified as having a level of need above minor (10%) than children in foster care (21%) or residential care (75%). Siblings in care The majority of children have all of their siblings in care; this equates to 231 (65.1%). Children in out of home care who had two siblings not in care were less likely to have a level of need above minor – 71% compared to 82% for all other children with sibling information. Age child came into care A large proportion of children came into care when they were 4 years and under (66%) – under 1 year - 127 (26.7%); 1-2 years - 106 (22.3%), 3-4 years - 81 (17.0%). This means 34% were aged over 5 years at entry to care. Aboriginal and Torres Strait Islander children and young people At the time of the assessment Aboriginal and Torres Strait Islander children and young people made up 28.4% of the out of home care population. There is double the number of Aboriginal and Torres Strait Islander males (90) than Aboriginal and Torres Strait Islander females (45) in the care system. Aboriginal and Torres Strait Islander males make up 34.9% of the male population and Aboriginal and Torres Strait Islander females make up 20.6% of the female population. Aboriginal and Torres Strait Islander children are more likely than non-Indigenous children to have a level of need above minor (27% to 17%). Aboriginal and Torres Strait Islander males are almost twice as likely to have a higher level of need (32%) than both Aboriginal and Torres Strait Islander females (16%) and non-Indigenous males (17%). Two-thirds of Aboriginal and Torres Strait Islander males in the oldest age group (15-18 years) had a level of need above minor. 7 Figure 1: Proportion of the total number of Aboriginal and Torres Strait Islander children and nonIndigenous children per complexity level Length of time in care Over 80% of children had been in the care system for less than nine years. Out of the total number of children and young people who had been in care for at least nine years, children in this age group were more likely to have a level of need above minor (33%) compared to all other age groups (17%). Five of the 13 Aboriginal and Torres Strait Islander males in care for at least nine years were in the extreme level of need category. In contrast, only two of 39 non-Indigenous males in care for at least nine years were in the extreme level of need category. Young people aged at least 15 showed significant variance in terms of the length of time they have been in care and if they had a level of need above minor. For example, 41% of such young people with 2-3 years care before assessment, 56% with 4-5 years, 28% with 6-8 years and 46% with at least 9 years care before assessment. Figure 2: Young people aged 15 years and their CAT level versus the number of years they have been in care 8 Age of children in care at assessment Children who came into care aged 9-18 years were more likely to have a level of need above minor (36%) than those who came into care at younger ages (17%). Of these children, Aboriginal and Torres Strait Islanders were only slightly more likely (40%) to have higher levels of need than non-Indigenous children (35%). A significant proportion of children aged 15-18 years when assessed (43%) had levels of need above minor. This compares with only 15% for younger children. Subsidy payment The majority of children who were assessed at a minor level of need were paid a standard payment (317). There were 56 children whose carers were being paid at a higher subsidy rate than standard who have been assessed as having minor needs. Of the 56 children whose carers are being paid a higher subsidy rate than standard and who have been assessed as having minor needs 36 children are in foster care and 16 are in kinship care. Alternatively, there were 22 children assessed at a level higher than minor who are only on a standard payment. Of these six children were in foster care and seven were in kinship care. Table 2: Subsidy level versus CAT level Standard Care Level 1 Care Level 2 Intensive Other* Total Minor 317 20 30 6 9 382 Moderate 14 4 8 9 11 46 Significant 3 1 1 7 10 22 9 Extreme 5 1 0 9 11 Total 339 26 39 31 41 26 *Other includes negotiated rates, residential, payment by other state, therapeutic – On Track or no payment 6. Discussion There is significant research that evidences the negative impact on a child or young person’s long term outcomes when they have resided in out of home care. There is continued debate about whether the poor outcomes are related to pre-care adversities, the placement in out of home care or a combination of both (Wade et al, 2011). Alarming research coming from the United States is showing children who are exposed to multiple trauma episodes have a life expectancy of 20 years less than the general population (Griffen, 2014). Reading through the case documents to undertake these assessments it is clear that the majority of children and young people who enter care have already experienced multiple trauma events and often experience additional trauma whilst in care as a result of continuing service failures including placement breakdowns and discontinuities of caseworker personnel. The personal, financial and social impacts of abuse, neglect and out of home care is well documented in national and international research. As noted in the Australian Institute of Family Studies (2013) information paper on the costs of out of home care, adverse impacts include: future drug and alcohol abuse; mental illness; poor health; homelessness; juvenile offending; criminality; and incarceration The research to date simply highlights the need to ensure children have safe and stable placements where they can grow and develop into healthy adults. The ACT has very little population data for children and young people in care as it is generally only collected at an individual level. Ongoing individual case planning considers the child’s wellbeing and placement needs throughout the child’s time in care. This case planning information is used to inform decision making about whether a child should be reunified with their birth parents, the type of placement they require, what supports the carer will need to care for the child and whether the child’s placement should become permanent. This information is not able to be aggregated readily by the current child protection information system and as a result Care and Protection Services has had limited ability to understand the complexity of the needs of children and young people in care as a cohort and whether this has changed as a result of Care and Protection Services intervention. This is the first project of its kind in the ACT. The project found that at the time of the assessment 80% of children and young people in care had a minor level of need. In contrast, this means 20% of children and young people fell in a level higher 10 than minor. Interestingly, the level of complexity for children was non-linear in terms of the decrease from minor through to extreme needs. There were more children in the extreme behaviour category as opposed to the next level down, the significant level. This means there were more children exhibiting extremely complex behaviours that required very intensive interventions and needed additional assistance to support their placements than those with significantly complex needs. A case study for each level of need is provided at Attachment D. Children and young people found in the extreme level of need appeared to have some very similar characteristics. The majority of children in the extreme level are adolescents (76% are 12 years or above) and many present with the following characteristics: Multiple diagnoses including: - Foetal Alcohol Syndrome - Attention Deficit Disorder - Attention Deficit Hyperactivity Disorder - Post Traumatic Stress Disorder - Obsessive Compulsive Disorder - High levels of anxiety Were older when they came into care (>8 years); Multiple placements moving back and forth between birth family, kinship carers, foster carers, residential care and Bimberi Youth Detention Centre; Engagement in criminal activity Drug and alcohol abuse Disengaged from education Exposure to domestic violence and parental drug and alcohol abuse as young children These characteristics should pose as early warning signs for other children who are moving into adolescence and starting to engage in similar behaviours. There are a number of children assessed as having lower levels of need in the moderate or significant categories that were brought into care when they were older children, are now starting to disengage from school, are participating in low level criminal activity and are in unstable placement situations. These children are at high risk of their needs escalating as they become teenagers. Although the assessments were not undertaken to generate an understanding of how much it might cost to care for a child or young person with complex needs the comparison data between the CAT assessment and subsidy level is worth discussing. The majority of children who were assessed at a minor level received a standard payment to their carer. However, there were 56 children and young people whose carers were being paid a higher subsidy even though their needs were assessed as minor. One reason for this was a policy decision made in 2006-2007 to not reduce a carer’s higher level payment, regardless of whether the child's needs stabilised or decreased. Also, of the 56 children, a large proportion was in foster care. This is consistent with research whereby foster carers are often provided with a higher level of payment than kinship carers (Yardley, Mason & 11 Watson, 2009). Kinship carers generally do not ask for more assistance and can be concerned there may be repercussions if they identify problems within the placement (Yardley, Mason & Watson, 2009). These findings raise important questions about equity of access to financial and other supports for children in kinship placement who now comprise the majority of children in out of home care in the ACT (53%). Another interesting finding was the age children and young people upon entry to care. The care population at the time of assessment showed a large proportion of children came into care when they were four years and under (66%) and half (49% when they were aged two years and under. There is qualification to this finding as some older children would have been excluded from the population for the project if they were self placed or returned to birth family. On the other hand all children who are on an Enduring Parental Responsibility were also excluded and a proportion of these children are under 10 years. This finding should elicit increased focus on developing policies for addressing the impact of trauma on children in care aged five years and under for two reasons - the majority of children are entering care in this age group; and there was another finding which showed children who had been in the care system for nine years or more were still showing high levels of complexity. The ACT service system needs to be more responsive to young children and be designed to create opportunities to move young children into stable placements, either back at home with family or into a permanent arrangement, as quickly as possible. The second reason may be demonstrating that young children who are entering the ACT care system are not receiving the attention they require at an early age to address the impact of abuse and neglect on children. Research shows that exposure to repeated adverse experiences can alter a child’s brain resulting in enduring emotional, behavioural, cognitive, social and physical problems which often don’t present until later in a child or adolescent’s life (Perry, 2006; as cited in Webb, 2006). Further support to focus early on young children is that older children aged 12 years or more are highly vulnerable with a significant proportion of young people aged 15-18 years (43%) showing level of needs above minor. Young people in care, even if they have been in care for a long time, may still display trauma behaviours related to trauma in their early years. Conversely, any findings about 15 year olds must be considered in light of normal adolescent behaviour as well. Adolescents do not develop higher order thinking until late into their teens and early 20’s as their pre frontal cortex undergoes significant development (Blakemore & Choudhury, 2006). The majority of 15 year olds in the general population also engage in a range of exploratory and risk taking behaviours. The result that children and young people in kinship care are less likely to have a level of need above minor is consistent with other research in this field. There are some qualifications for this finding including that the results should not be taken at face value as kinship carers demonstrate continual underreporting of issues and often tolerate more episodes of difficult behaviour (Yardley, Mason & Watson, 2009). Therefore, the service system should not underestimate the complexity of children’s needs in kinship care based on self reporting from carers alone. Another consideration for understanding this finding is that children and young people with more complex behaviours may be placed in foster care because there isn’t an appropriate placement with family or that children in kinship care stabilise in the placement at a greater rate because they are with their kin. The findings clearly show the system needs to have a greater focus on Aboriginal and Torres Strait Islander children and young people in terms of developing services that offer targeted support, particularly to male children and young people with very complex needs. Aboriginal and Torres Strait Islander children are overrepresented in the care system and interestingly there is double the number of male Aboriginal children to female Aboriginal children in out of home care. Aboriginal children were more likely than non-indigenous children to have a higher complexity level (27% to 17%) and this is further compounded for Aboriginal males who are almost twice as likely to have a 12 higher level of need to Aboriginal females and non-Indigenous children. Aboriginal male young people seem particularly vulnerable in the care system, as 75% of Aboriginal males between the ages 15-18 years had a level of need above minor and 38% were in the extreme level of need. There appear to be different effects of being in care long term for non Indigenous and Aboriginal males. Aboriginal males who had been in care for nine years or more were much more likely to have an extreme level of need (38%) than non-Indigenous males (5%). Non-Indigenous males often showed a higher level of needs than minor but there were only 2 out of 39 that were in the extreme level of need. Interestingly, 15 year olds who came into care when they were 7-8 years old or 12-13 years old displayed lower needs than 15 year olds who had been in care since they were six years old and under. This finding should be considered carefully and further researched. The finding may be showing that the placements continue to be vulnerable regardless of the age the child came into care or the length they have been in care. 7. Conclusion The purpose of the Child Profiling project was to gain a population measure of all children and young people in out of home care in respect to their current levels of need and the complexity of their behaviours. The findings will be used to design future service models and interventions that are more targeted and individualised to best meet the needs of children and young people in the ACT. Several aspects of the findings are worthy of note. The ACT’s system is made up predominantly of children who come into care at a very young age ie. prior to school commencement with 49% two years old and under. One of the implications for the service system is that it needs to be more strongly focused on meeting the needs of very young children coming into care - treating effects of trauma, attempting reunification and finding permanent placements for those children who cannot return to live with their birth families. In developing a new system of out of home care, particular attention should also be paid to addressing the needs of those children and young people found to be in the significant or extreme level of needs. New, creative and more flexible solutions are required. In particular this exercise suggests that without powerful intervention, male Aboriginal and Torres Strait Islander children and young people are at high risk for continuing difficulties that will result in poor outcomes. The exercise assessed 135 Aboriginal and Torres Strait Islander children and young people in care and found that there are many more Aboriginal and Torres Strait Islander male children and young people than female and Aboriginal and Torres Strait Islander children and young people were overrepresented at the higher needs levels. The exercise also found that children and young people in long term care are still displaying high level of needs and require a service response beyond the first few years in care. The extent to which initial trauma contributed to these poor outcomes versus adverse events in care is unclear. It would be extremely beneficial to undertake the assessments on a regular basis to start to gain a picture of the impact of out of home care on the overall population and specific cohorts to ensure that there is a current understanding of the needs of children and young people in out of home care in the ACT. 13 14 Attachment A: Child Complexity Tool – Jurisdiction Analysis Background A review was undertaken to gather information from states and territories in Australia, national and international research about child profiling. Although there are endless articles on out of home care (out of home care) past and present practices, it was difficult to find assessment tools that have been or are being used in current practice with the purpose of understanding the out of home care populations level of complexity. Australian Capital Territory Assessment tools on Children and Young People System (CHYPS) which are used for Care and Protection Services (CPS) and Early Intervention and Prevention Services (EIPS) include Being a Parent Scale, Depression Anxiety Stress Scales (DASS), DASS 21, Edinburgh Postnatal Depression Scale, Family Activity Scale 206, Family Activity Scale 7 – 12, Parenting Daily Hassles, Recent Life Events, Strengths Difficulties Questionnaire, socio economic information, Winterberry scale and the Family Support Scale. Currently across the Office for Children, Youth and Family Support (OCYFS) and the funded service providers the following information tools are in use, Looking After Children (LAC) by out of home care providers, Child and Family Centre (CFC) Intake Form, CPS Child Protection Child Concern Report (CPCC), CPS Child Protection Assessment Report (CPAR), Common Assessment Framework (CAF). New South Wales Many research projects have been conducted in NSW and most recently the Children in Care Study conducted in 2007 found that children in care were found to have multiple and complex mental health problems and placement insecurity. Children in the study were reported as having exceptionally poor mental health and social competence. The Child Assessment Tool has been utilised in NSW from 2012, and is designed to identify the most appropriate level of care from general foster care to intensive residential care based on the child’s behaviour, health and development issues. The tool: Determines the level of care that will best meet the needs of the child, Enhances transparency and consistency of placement decisions, Improves the matching of a child’s specific needs with a particular placement and Creates a common framework for placement decisions, which is shared between Department of Community Services (DoCS) and non government services. Queensland In 2005, as part of its reform of child protection the Department of Child Safety introduced the Structured Decision Making model, a licensed trademark. The Child Strengths and Needs Assessment (CSNA) which forms part of the Structured Decision Making model and involves the use of eight assessment and decision making tools from intake information received about a child protection concern, screening criteria, response priorities, safety assessment, family risk evaluation, child strength and needs assessment, parental strengths and needs assessment, family risk reevaluation and family reunification assessment. South Australia 15 A standardised screening instrument for assessing complexity in children entering out of home care, is being utilised in South Australia, and that is the Complexity Assessment Tool (CAT). The CAT measures the behavioural and special needs of children and young people. It assesses and then scores children across specific areas to identify high and complex needs in order to assist in placement planning and service provision. South Australia undertook a research project, with the aim to differentiate children in terms of their level of need so that services and funding can be apportioned more strategically. As children entered care, an assessment would be completed, their level of need would be identified and services would be matched to their needs. Northern Territory Northern Territory has used the South Australian CAT tool as an audit of children in out of home care. Like South Australia, they are now looking at using this tool further to link it with the financial subsidy given to carers linked directly to the identified needs of the child/ren in their care, from the CAT assessment. Victoria Victoria were undertaking a similar project to the ACT. Research from Victoria shows increasingly, families with multiple and complex needs have become the primary client group of modern child protection services. Recent research has shown that they typically have five or more disadvantages including living with poverty, unemployment, poor quality housing and disabilities. Further to that, data shows family violence, substance abuse and mental illness as commonly co-occurring difficulties for families involved with child protection, a pattern also reflected in the analysis of child death reviews. A comprehensive family assessment is undertaken which balances the strengths and protective factors versus the pattern and severity of harm and likelihood of harm. In July 2004, the Victorian Department of Human Services participated in a national research project regarding children with high support needs in alternative care. Questions asked were “What were the profiles? What were the pathways into care? What were the interventions? and what were the histories of young people in care who experienced repeated placement breakdown?” It was proposed that the research would contribute to greater placement stability and positive outcomes for high needs and at risk children. It was shown that trauma was the universal, underlying theme of children’s challenging behaviours caused by experiences of repeated multiple forms of abuse and neglect which led to the development of conduct and attachment disorder type behaviours and developmental delays. A recommendation from the project was that prevention was to be predicated by a three pronged approach that is: timely intervention , available expertise, coordination, one stop shop; holistic whole family needs assessment; and stability of care to be achieved by expertise that informs assessment, planning and the development of therapeutic placement options and support. The longitudinal study on young people leaving care is a long term research project about the lives of young people in out of home care and their experiences transitioning from care in Victoria. The study will be conducted over five years and is the first of its kind to be conducted in Victoria. Data collection commenced in 2013 and will run until 2017 and the Australian Institute of Family Studies is taking carriage of this study. 16 The purpose of the study is to inform government policy in supporting more effective transitions for young people when leaving out of home care. In particular, it will aim to improve young peoples’ move towards interdependent relationships and eventual independence by: Providing insights into the critical success factors associated with transition from; Proposing ways of enhancing out of home care; Proposing improvements in the transition from care; and Proposing improvements post transition from care. Western Australia Since 2008, Western Australia have utilised the Signs of Safety as a child protection practice framework. Each child in out of home care has a child history folder, which incorporates the child’s care needs, history, development and progress. The Signs of Safety framework incorporates strengths based principles alongside an exploration of danger and risk. Tasmania In Tasmania, the Common Assessment Framework is currently used to assist and support professionals in consistently assessing, planning and responding to the needs of children and young people. This tool is designed to make an effective assessment which involves collecting a range of information to support the decision making process. The information gathered through the assessment process is often used to identify and address the presence of risks and support needs in the areas of health, safety, development and wellbeing. Nationally From research nationally, the seven domains of child wellbeing indicators of health, emotional and behaviour development, self care and wellbeing, education, identity, family and social relationships as well as social presentation are common indicators currently used. Australian Research Alliance for Children and Youth (ARACY) in 2010 undertook a review and piloted a national tool known as the Common Approach to Assessment, Referral and Support (CAARS). The role of the CAARS taskforce was to decide on a process for the development of a national approach to the prevention of child abuse and neglect, supported by common assessment and referral as well as to guide the development of common approach components. Profiling/Needs Assessment Tools Australian Capital Territory Western Australia Tasmania Victoria New South Wales Queensland South Australia Northern Territory In process of choosing a tool Signs of Safety Common Assessment Framework (CAF) In progress of establishing a tool Child Assessment Tool (CAT) Structured Decision making model incorporating Childs Strength and Needs Assessment (CSNA) Complexity Assessment Tool (CAT) Reviewing current practice, have completed an audit of children in out of home care using the CAT 17 Attachment B: Complexity Assessment Tool (CAT) Reproduced with permission from Families SA. The Complexity Assessment Tool (CAT) is a screening instrument that measures the behavioural and special needs of children and young people. It assesses and scores children across specific areas of behaviour and need to assist in identifying what services and supports are required to facilitate successful placement in alternative care. Children are grouped according to their level of need as belonging to one of four groups. These are: Level 1: Minor or no problems Level 2: Moderate problems Level 3: Significant problems Level 4: Extreme problems This level-of-need classification system corresponds to the most suitable placement option for the child. For example, a child assessed as Level 1 would require less intensive forms of care and support than a child assessed as Level 4, who would require very intensive, specialised support and care. These levels are explained in the following section. Level 1: Minor or no problems The child or young person in this category is generally well-functioning, e.g.: attends school and is able to form positive connections with family, community and culture. The level of supervision required is at a general (age appropriate) level only. Level 2: Moderate problems The characteristics of the child or young person at this level includes: moderate developmental delays, disability and health, behavioural or educational issues, requiring ongoing review and/or treatment. The child or young person does not require intense supervision and with structures in place is able to attend school and form positive connections with family, community and culture (although there may be intermittent conflicts which require periodic intervention). Level 3: Significant problems The child or young person at this level has major health or disability issues that affect everyday functioning and/or the child or young person's existing and/or prior living arrangements or placements are continually in crisis as a result of the young person's challenging behaviours. Additional supervision, support and liaison with specialist services are required to: maintain the young person’s stability of placement; sustain engagement in education, employment or training; and cultivate the young person’s connections with family, culture, personal interests and community integration. Level 4: Extreme problems The child or young person has severe problems in one or more areas of functioning that present an imminent and critical danger of harm to self or others. Their existing and/or prior living arrangements or placements are continually in crisis. 18 Intensive supervision, support and liaison with specialist services are required to: maintain the young person living in alternative care accommodation; reconnect and sustain engagement in education, employment or training; and cultivate the young person’s connections with family, culture, personal interests and community integration. Part A Behavioural complexity Part A of the CAT assesses the child or young person’s behaviour across five categories, specifically: 1. Substance use 2. Sexualised behaviour 3. Offending behaviour 4. School behaviour 5. General behaviour Within each of the above categories of behaviour select the A to E select the description which best describes the behaviour being assessed. Behaviour Substance use Sexualised behaviour Offending behaviour School behaviour General behaviour Severity Rating A-E Numerical Score Next, in the column headed 'Numerical Score' allocate a numerical score for each A to E rating where A =1, B =2, C =3, D=4, E =5. Part B Special needs complexity Part B of the CAT assesses the child or young person’s special needs complexity across four categories, specifically: 1. Physical health 2. Child development and intellectual health 2. Mental health 3. Physical disability As in Part A, within each of the above categories of behaviour a series of descriptors, ranked A to E, are available to choose from. From the available options, select the descriptor which best describes the special need being assessed. Assess the four special needs and select the A-E rating which best describes each one. Then, enter the A-E rating for each special need in Table 2, Part B of the CAT in the column headed 'Severity Rating A-E. Next, in the column headed 'Numerical Score' allocate a numerical score for each A to E rating where A =1, B =2, C =3, D=4, E=5. 19 Special Needs Physical health Child development and intellectual ability Mental health Physical disability Severity Rating A-E Numerical Score Part C Calculate overall complexity In Step 3, we combine the results from Step 1 and Step 2 to produce a final CAT score. 3.1 Square the value obtained in Step 1 I.E.: =2x2 =4 3.2 Square the value obtained in Step 2 I.E.: =3x3 =9 3.3 Add these values together I.E.: =4+9 = 13 3.4 Divide this value by 50 to convert into a proportion I.E.: = 13/50 = 0.26 3.5 Record the final value I.E.: = 0.26 Interpreting scores The following table describes the way in which scores are to be interpreted. The lower the score obtained, the less complex are the needs of the child. Conversely, the higher the score, the more complex are the needs of the child. Up to 0.20 0.21 - 0.36 0.37 - 0.50 0.51 - 1.0 Interpretation of scores Level 1 Level 2 Level 3 Level 4 Minor or no problems Moderate problems Significant problems Extreme problems 20 Assessor’s critique ATSI Cultural background Siblings in family Siblings in care Placement type Length of order Age child came into care Childs’s name Child’s date of birth Name of document used to make assessment Name of persons spoken to (child, young person, carer, caseworker etc.) Level of complexity of need Justification for this level Assessors name Date of assessment 21 Attachment C: Counting Rules The review was based on the latest version of the Annual Review, Care Plan or Child Protection Assessment Report. The counting rules are as follows: • If a child or young person resides with their birth families they are not counted. • Children who were going through an active reunification process were not counted. • If a child or young person has self- placed with their birth families for longer than 12 months at the time of the review they will not be counted. • If a child or young person is on an Order and paid by an interstate jurisdiction but is residing in the ACT they are counted. • If a child is on an Enduring Parental Responsibility, Adoption Order or in permanent care they are not counted. • If a child has siblings over the age of 18 years (adult) they are not counted. • Young people who are on a Care Order who are in Bimberi were counted. • If a child is on a Voluntary Care Agreement they were not counted. • Children on Interim Orders and Final Orders were counted. • Young people over the age of 18 years were not counted. • Half siblings are counted as being ‘siblings’. This means some siblings are not in out of home care because they are placed with a different parent to the child being assessed. Step siblings or other children residing in the placement (biological children of carers) were not counted as siblings. • Children who are not in the care of the Director-General were not counted. • Age when child entered care was counted from the date the child was first placed on a Care Order and were placed away from their birth parents. This date may then include periods of time when the child was restored to their birth parents. • Cultural background as written in the document used to make the assessment. • The assessments used the latest version of the Annual Review Report, Care Plan or Child Protection Assessment Report (in lieu of an Annual Review Report). • Age at assessment was taken at a single point in time – 25 June 2013. • Placement was categorised using the CHYPS identifier. 22 Attachment D: Case Study Level 1: Minor needs The child is three years old and was born four weeks prematurely and showed some symptoms of drug withdrawal at the time of birth. The child was removed from their parents at three months of age when both parents were incarcerated. The child was placed with their grandmother where their two siblings were already residing. The child is accessing services on a monthly basis to assist the child’s speech delay. The child attends child care two days a week and really enjoys story time and playdough. The child is meeting their age milestones and no longer needs adjustments because of their premature birth. The child looks to their carer when they are hurt or tired and sometimes throws tantrums when they are told ‘no’. The child requires supervision at the same level as any other three year old child. Level 2: Moderate needs The child is nine years old and Care and Protection Services have been involved since the child was born. There were concerns the child was exposed to physical abuse and neglect when living at home. The child’s mother had been diagnosed with a moderate intellectual disability and bi polar disorder and refused to engage in mental health treatment. After six years the child and their younger sibling was removed. After three years and four placement changes the child was placed on long term orders and moved to a long term foster placement. The child is approximately six months behind their peers academically and attended two different primary schools. The child has established some positive friendships but has some difficulty regulating their emotions and has occasional outbursts. The child’s needs are closely monitored using an Individual Learning Plan by the school and the carer is required to attend monthly school meetings. The child participates in a special reading group twice a week and has tutoring once a week in response to their educational delay. The child has moderate level asthma that requires regular three monthly reviews by the GP but no other health issues. Level 3: Significant needs The child is a 12 year old Aboriginal child who has been known to Care and Protection Services since they were four years old. The child is one of five children all of whom were placed in care when the child was seven years. The child was removed and placed in foster care due to exposure to ongoing domestic violence towards their mother by several male partners and parental drug and alcohol abuse. Reunification was attempted over the course of twelve months when the child was eight years however was unsuccessful. The child and the siblings had been separated as the some siblings were placed with their kin and others in foster care. Following a kinship assessment the child moved to reside with their maternal aunt however this placement only lasted six months before the aunt was unable to care for the child. The child moved to another foster care placement with one of their siblings. The child was born with hearing difficulties which has impacted their speech and cognitive development. The child has been to four different primary school because of their placement changes and is reading and writing two years below their peers. The child has become oppositional in the classroom and refuses to undertake certain classroom activities. The child has been assessed as needing learning support but the child refuses to work with a teacher’s aide claiming they don’t want to stand out from the other students. The child has issues forming relationships in the classroom, displays bullying behaviour, frequently swears and due to non-compliant behaviour has 23 been suspended three times in the past 12 months. The carers have difficulty getting the child to school every morning because of the child’s school refusal. The school is planning to transition the child to high school however they are concerned this will further disengage the child from schooling even further. The child demonstrates very challenging behaviour at home which is triggered by poor self regulatory behaviours. The child’s carers use respite every second weekend whereby the child is placed with different carers as many respite carers are unable to cope with the child’s challenging behaviours. The child has had difficulty attaching to their most recent carers and the carers are concerned the child will not settle with them. The child frequently runs away, has uncontrolled bursts of anger that are triggered by seemingly innocuous events and has damaged the carers property numerous times. The child has been cautioned twice by the police for shoplifting and graffiti. The child is due to see their birth mother once a week however this contact is often cancelled at the last minute by the mother. The child becomes withdrawn and the problem behaviours escalate when this occurs. Level 4: Extreme needs The young person is now 16 years old and has been known to child protection services since they were five years old. Over the course of six years a number of child protection reports were received in relation to the young person’s repeated exposure to domestic violence. When the young person was 11 years old the young person’s mother agreed for the young person to come into care through a Voluntary Care Agreement and final Care and Protection Orders were made three years later. Following entry into care the young person experienced multiple placement changes moving from kinship care, back to birth family, foster care, residential care and youth detention. Many later placement changes were initiated by the young person and were not approved by Care and Protection. The young person has not been able to manage residing in home-based placements for some years although they continue to return to their birth family and kinship carers even after significant relationship breakdowns. The young person has been diagnosed with a multitude of mental health disorders including Obsessive Compulsive Disorder, Oppositional Defiance Disorder and Attention Deficit Hyperactivity Disorder. The young person has intermittent depressive tendencies, suicidal ideations and demonstrates erratic and violent behaviours when stressed or anxious. The young person’s behaviour problems impair their every day functioning to a significant degree. The young person doesn’t have any physical disabilities but when they were young they were developmentally delayed manifesting through a speech delay and poor fine and gross motor development. The young person disengaged from education when transitioning to high school, the young person has engaged in a number of training programs in youth detention and enjoys hands on learning including arts and crafts. The young person is unable to read and write and has the same cognitive skills as seen in Year 4 students. The young person has engaged in escalating forms of criminal behaviour and frequently breaches their bail conditions. The criminal behaviour is linked to peer pressure and using drugs. The young person admits to using drugs and alcohol over the course of several years and this has a significant impact on their violent behaviour both when using drugs and when trying to obtain drugs. The young person is connected with peers who also engage in risk taking behaviour including using drugs however the young person has difficulty in sustaining peer relationships due to displaying 24 behaviours that can intimidate others. They frequently fail to show any empathy or remorse for their actions. The young person has had one serious romantic relationship which was described as controlling and volatile. The young person has a child who they see on a supervised and infrequent basis. The young person has no real aspirations at this stage, they can’t identify any potential career path and the only desire they articulate as having is to not return to youth detention. 25 Attachment E: Reference list 1. Australian Institute of Family Studies. (2013). The economic costs of child abuse and neglect. Retrieved from: http://www.aifs.gov.au/cfca/pubs/factsheets/a142118/ 2. Australian Institute of Health and Wellbeing. (2013). Child protection Australia 2011-2012. Canberra, Australia: AIHW. 3. Blakemore, S.-J. and Choudhury, S. (2006). Development of the adolescent brain: implications for executive function and social cognition. Journal of Child Psychology and Psychiatry, 47: 296–312. 4. Family and Community Services. (2013). A Safe Home for Life. Sydney, Australia: Family Community Services. Retrieved from: http://www.facs.nsw.gov.au/__data/assets/file/0018/279000/A_Safe_Home_For_Life_Cons ultation_Report.pdf 5. Griffin, E. (2014). Trauma Informed Care in the US Child Protection System. Responsive Pathways to Vulnerable Children Conference. Sydney, Australia. 6. Webb, S.A. (2006). Social Work in a risk society: Social and Political Perspectives. London, Pelgrave, MacMillian. 7. Yardley, A., Mason, J. And Watson, E. (2009). Kinship Care in NSW: Finding a way forward. Sydney, Australia: Social Justice and Social Justice Change. 26