Lab DI Final Information:
advertisement

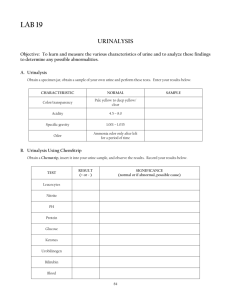
Lab DI (Urinalysis) : Red to brownish red Hematuria Hemoglobinuria Myoglobinuria Reddish brown to brown Met haemoglobin Hemoglobinuria Myoglobinuria Greenish tint Bilirubinuria -excessive turbidity = presence of suspected particles in the urine (increased RBC and WBC / numerous crystals / bacteria / lipiduria / mucus / semen) pH pH = normal (6 to 7.4) -raise pH = age of specimen / presence of contaminant or pathogenic bacteria (urea to ammonia) (pH >8 = erythrocytes / leukocytes / casts) (precipitation of urine crystals = in supersaturated urine) -meaningful evaluation of acid-base status = blood gas analysis / clinical sign consideration -pH test = blood gas analysis = specific for the detection of hydronim ions (contains indicators methyl red / phenolphthalein / bromthymol blue) Specific Gravity (USG) -measurement of the density of urine compared to pure water / # of molecules in urine / MW / size -increase in temp = decrease urine density -urine osmolality = (last 2 digits of USG) x 36 -normal USG = 1.002 - 1.035 -Bowman’s space USG = 1.007 – 1.010 -generalized renal impairment or nephrogenic DI = USG not > 1.022 after 12 hr without eating or drinking -end-stage renal disease USG = 1.007 to 1.010 -urine contamination / high level of glucose / pt received high density RO dye intravenously = USG >1.035 -USG test = detect [ion] of urine / cation present => produce a colour change (blue => bromethymol blue) (blue-green => yellow) Protein -whole urine = dipstick screening test -semi-quantitative tests for urine protein = supernatant of centrifuged urine -trace to 1+ rxn in very dilute urine = significant proteinuria [ hazy appearance] -(1+) 200 to 500 mg (2+) 0.5 to 1.5 gm (3+) 2 to 5 gm (4+) 7 gm (all per 24 hr) -dipstick protein rxn >2 = significant proteinuria -normal total protein excretion = below 150 mg / 24 hr or 10 mg / 100 ml -more than this value = proteinuria -proteinuria > 3.5 gm / 24 hrs = severe = nephritic syndrome -protein test: (1) “protein error of pH indicator dyes” = ability of amino groups in proteins to bind / alter colour of A-B indicator) (albumin: very sensitive / globulin: less sensitive / B-J’s protein: insensitive) (2) sulfosalicylic acid test = more sensitive precipitation test (detect albumin / globulin / B-J’s protein at low concentration) -cause of proteinuria beside KD: (1) prostural (orthostatic) = pass excess protein during day (healthy adult) (2) functional (albuminuria) = fever / cold exposure / stress / pregnancy / eclampsia / CHF / shock / severe exercise (3) drugs Glucose -glucosuria = diabetes mellitus = a result of prior hyperglycemia to a level in excess of the renal threshold for reabsorption -benign low renal glucose threshold = Cushing’s syndrome / severe stress / drugs -glucose test = Glucose Oxidase Method = measures glucose glucose + glucose oxidase => nascent oxygen // Potassium iodide === iodine => brown colour change -many drugs increase urine glucose measurement -false positive (trace to 1+) = dipstick jar being left uncapped for a few days / hypochlorite (bleach) -false negative (drugs) = ascorbic acid / levodopa / phenothiazines / tetracycline Ketones -ketonuria = deranged energy metabolism such that fat is used in excess of carbohydrate -ketone test = Legal’s test = acetone and acetoacetic acid react with sodium nitroprusside in alkaline solution => violet color (phenylketones / phthalein) -positive reaction confirm test = Acetest = contains lactulose useful for semi-quantitatively measuring ketone in other fluids (plasma / serum / milk) -false positive = captopril / MESNA / other substance containing sulfhydryl groups -metabolic abnormalites = uncontrolled diabetes or glycogen storage ds -abnormal nutritional conditions = starvation / fasting / anorexia / high protein diets / low carb diets -protracted vomiting -disorders of increased metabolism = hyperthyroidism / fever / acute or severe illness / burns / pregnancy / lactation / surgery Nitrite -the reaction indirectly detects the presence of nitrite-forming organisms in the urine -nitrite test = Griess’s test = specific for nitrite (determines total nitric oxide based on the enzymatic conversion of nitrate to nitrite by nitrate reductase) (colorimetric detection of nitrite as an azo dye product of the Griess rxn) -organisms convert dietary nitrate to nitrite / causing UTIs (pink color for +ve) = E.coli / most urinary pathogens -negative result (even in presence of bacteriuria) = bacteria not containing nitrate reductase / diet with low nitrate content / high diuresis / high content of ascorbic acid / insufficient incubation of urine in bladder -false positive = stale urine (nitrate has been formed by contamination of specimen / urine containing dyes -to check children for UTI: Clean-catch voided urine = > 10 to power of 5 colony forming units / mL Catheter-obtained voided urine = >10 to power of 4 colony forming units / mL Urine obtained by suprapubic aspiration = > 10 to power of 3 colony forming unites / mL Leukocyte -the reaction detects the presence of esterases that occur in granulocytes (esterase cleave an indoxyl ester => indoxyl reacts with a diazonium salt => violet dye) -pyuria = urine sample contains damaged or lysed WBC’s Bilirubin -breakdown of RBCs by phagocytic cells => haemoglobin broken down => globin – heme => heme converted to bilirubin => bilirubin + albumin => to liver -bilirubin – glucuronic acid = conjugated bilirubin (direct bilirubin) => excrete into the bile by liver => stored in gall bladder -bilirubin + bacteria in intestine => urobilin (color of the feces) -bilirubin reabsorbed => urobilinogen (appear in urine) -obstructed bile duct = direct bilirubin build up => show up in urine -hepatobiliary disease = lead to bilirubinuria (conjugated bilirubin levels in blood are elevated) Bilirubinuria indicates cholestasis Bilirubinuria may be secondary to the hemolysis without any evidence of cholestasis -bilirubin test = multireagent dipstick = sensitive to 0.2 to 0.4 mg/dL of conjugated bilirubin -false negative = large amount of vit C or nitrite / long exposure of the sample to direct light Blood -blood test = based on detection of the “peroxidise-like” activity inherent in molecules of heme -hematuria (RBCs lyse on contact with reagent pad) = inflammation / trauma / neoplasia / hemostatic disorders -hemoglobinuria (free Hb filtered into urine) = intravascular hemolysis of any cause = immune –mediated / toxic / infectious No RBC on the urine sediment / urine supernatant will be red -myoglobinuria (free Mb filtered into urine) = myocyte injury allowing release of myglobin High CK and high AST, reflecting muscle injury (Summary table): pH USG Protein Test Blood gas analysis Protein error of pH indicator dyes Sulfosalicylic acid test Glucose Ketones Glucose oxidase method Legal’s test Nitrite Acetest (positive rxn confirm test) Griess’s test Leukocyte Bilirubin Multireagent dipstick Blood Detect Hydronim ion Ion concentration in urine Sensitivity: Albumin > globulin > B-J’s protein Detect albumin / globulin / B-J’ protein at low concentration Measure urine glucose Acetone & AAacid react with sodium nitroprusside to detect urine ketone level Measuring ketone in plasma / serum / milk Specific for nitrite Determine total nitric oxide Presence of esterases Sensitive to 0.2 to 0.4 mg/dL of conjugated bilirubin Detection of the “peroxidise-like” activity inherent in molecules of heme (info from pony): -routine urinalysis is comprised of tests for = glucose / blood / protein => but not calcium -normal range of USG = 1.005 to 1.030 -in normal healthy individuals the USG of a random urine sample reflect fluid intake -urine turbidity or cloudiness = large amount of bacteria / urates / fat => but not protein -pink / red colour of urine => due to myoglobin / haemoglobin / RBCs => not pseudomonal infection -urine pH = an accurate measurement of urine requires a freshly voided specimen -urine pH or 9.5 = may represent Protease contamination of the sample -bleach / coumadin / aspirin = cause blood urine test to be positive (true or false positive) -hematuria = same as occult RBC in urine -proteinuria = single most important indication of renal ds -nephrotic syndrome = urine protein concentration >3.5 g / 24 hr -ketone is the urine associate with = fever / starvation / DM -normal volume of urine production per 24 hr = 600 to 2500 mL -effective screening protocol = appropriate population for screening must be able to be identified procedure must be cost effective and reliable -urine nitrate test = may be truly negative despite the presence of large amounts of bacteria in a pt with a true UTI -biological fluid can be shown to urine by virtue of its high concentration of creatinine -only formed element found in the urine that is unique to the kidney is casts -orthostatic proteinuria = most often occurs in healthy, young adults reticulocyte count / serum iron / Schillings test CRP / antinuclear antibody test / rheumatoid factor assay C-reactive protein test serum glucose ALT / bilirubin / prothrombintime serum calcium / alkaline phosphatase / urine protein Anemia Arthritis Heart ds renal ds / neurologic ds / heart ds Liver ds Bone ds Casts Fatty cast Granular cast WBC cast Tamm-Horsfalls protein RBD cast Only formed element found in urine that is unique to kidney Nephritic syndrome Pyleonephritis Pyleonephritis Major protein of casts Acute glomerulonephritis