Eosinophilic meningitis is defined by a
advertisement

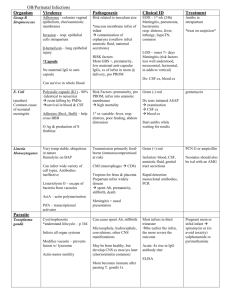
Eosinophilic meningitis Mary Naguit Eosinophilic meningitis is a rare entity. The key criteria is that the cerebrospinal fluid shows the presence of an increased number of eosinophil in a patient with clinical manifestations of meningitis. The most common causes of eosinophilic meningitis worldwide are the parasitic infections caused by nematodes. Etiologies Eosinophilic meningitis due to parasites is most often seen as sporadic cases in Southeast Asia, South Pacific and the Caribbean. The most widely reported cause is Angiostrongylus cantonensis. The larvae of this rat lung nematode are ingested in undercooked seafood such as crabs, prawns and snails. Gnasthoma spinigerum is an intestinal nematode of cats and dogs, which is acquired by eating undercooked fish. The increase in world travel and ship-borne dispersal of infected rats leads to more cases being reported outside Southeast Asia. In the United States, Baylisascaris procyonis is the most common parasitic cause of eosinophilic meningitis; this infection is acquired by accidental ingestion of raccoon feces. Coccidiodes immitis is often cited as the most common nonparasitic infectious cause of eosinophilic meningitis, but such an occurrence is still uncommon. A case report by Almoujahed et al(2001) showed occasional eosinophils in the CSF with a 55 year old African-American male with a history of VP shunt placement. It turned out that the patient had a history of travel to California and developed pulmonary Coccidioidomyosis which disseminated to the central nervous system complicated by hydrocephalus. The disease remained indolent after the VP shunt placement and was diagnosed incidentally 3 years after during a shunt malfunction. Myeloproliferative disease in the form of hematologic malignancies or metastatic cancer should be ruled out if an infectious etiology is not found. Procedures involving the spinal cord including contrast myelography and ventriculoperitoneal shunts can also cause an increase in eosinophilia in the CSF. In the pediatric age group, eosinophilic meningitis is most commonly caused by a ventriculoperitoneal shunt. A study by Fulkerson et al in 2008 described the risk factors, relationship to infection, and clinical significance of CSF eosinophilia in a large group of shunt-treated pediatric patients. Eosinophils were recognized during a follow-up shunt evaluation in 31% of 300 patients after preliminary placement. They concluded that cerebrospinal fluid 1 eosinophilia is a common occurrence in the pediatric age group with shunts. Patients with CSF eosinophilia leads to more shunt malfunction. Patients with Propionibacterium acnes-induced shunt infections have higher eosinophil percentages than are found in infections associated with other organisms. The researchers suggested anaerobic culture studies to be performed in suspected cases of eosinophilic meningitis in patients with shunts. An interesting case of allergic Aspergillus sinusitis causing eosinophilic meningitis was reported in the National University Hospital in Singapore. The patient presented with cavernous sinus thrombosis leading to abducens nerve palsy and CSF eosinophilia. The latter was deemed not a consequence of a concomitant CSF infection caused by Angiostrongylus or other parasites because of the negative epidemiologic risk factors. Clinical features noted are the products of the inflammatory contents of the sinus eroding through the sinus wall with leakage into the venous sinuses and subarachnoid space. Erosion through the intraethmoid septae, the lamina papyracea, through the cribriform plate or posterior wall of the frontal sinus into the epidural space was noted. The process is thought to be caused by bone resorption secondary to the expanding allergic mucin mass. Another interesting but rare case is CSF eosinophils in an infant. A report in University of Virginia Health Sciences Center by Hewett and Hendley. There were noted two cases of rapidly occurring CSF eosinophilia caused by GBS meningitis in 2-week-old infants, they concluded that the influx of white blood cells in response to GBS in the subarachnoid space may be particularly likely to proceed along the humoral or antibody mediated pathway in infants two weeks of age and less. Clinical Manifestations Severe headache is the most common complaint and has been attributed to intracranial pressure. Nausea, vomiting and neck stiffness are frequent. Paresthesias of the thorax and extremities are seen. Altered consciousness and generalized weakness are rare. Fever is not a prominent symptom even in infection. Other nonspecific symptoms include visual disturbances, photophobia, vomiting, arthralgias, myalgias, GI and respiratory symptoms. 2 Laboratory Diagnosis The definition of eosinophilic meningitis is presence of eosinophilia in the CSF, either greater than 10 eosinophils/mm3 or greater than 10% of the total CSF leukocytes, in a patient with symptoms of meningitis. The CSF shows leukocyte counts in the range of 20-5000 cells (usually 150-2000). Wrights solution or Giemsa stain is commonly used to visualize the CSF eosinophilia. Peripheral blood eosinophilia does not correlate with CSF eosinophilia. CSF eosinophilia is usually 20 – 70% with normal or minimally low glucose and slightly elevated CSF Protein. In eosinophilic meningitis due to parasites, eosinophila pleocytosis peaks at weeks 1-2 and then gradually resolves over several months. To note, invasion by helminths of the central nervous system is the most recurrent cause of eosinophilic pleocytosis in the CSF. CSF opening pressure is variable and should be performed to determine if measures to decrease intracranial pressure are warranted. For Angiostrongylus cantonensis, CSF ELISA and Serum ELISA have the highest accuracy. Monoclonal antibody against CSF antigens is useful, if available. CNS imaging should be performed to exclude other potential causes of meningitis. Focal lesions are not expected on CT or MRI. Ophthalmologic evaluation should be performed to screen for the presence of elevated intracranial pressure. In patients with parasites, larvae may be seen in the eye. 3 Therapy The disease is usually self-limiting if the cause is infectious or due to spinal cord manipulation, although some symptoms including headache may persist for > 4 weeks. Most of the patients affected with eosinophilic meningitis can be adequately managed with supportive therapy with analgesics plus rehydration. NSAIDs should be avoided since they are occasionally the direct cause of CSF pleocytosis and headache. In patients with increased intracranial pressure, serial lumbar punctures may produce major clinical improvement. Antihelminthic agents are commonly prescribed for parasitic infections although neurological symptoms often worsen because of larvae death within the CSF. Corticosteroid therapy provides symptomatic relief of headaches. In a double-blind placebo controlled trial of 129 adult (> 15 years old) patients with eosinophilic meningitis and who were admitted in a Thai hospital were studied. A 2 week course of prednisolone was efficacious in treating headaches refractory to supportive therapy. The dose used was 60mg prednisolone/day (Chotmongkol V, CID 2000). Albendazole or mebendazole was also thought to be effective in the pediatric age groups but should be used with caution as it may exacerbate neurologic symptoms especially if the larvae has matured in the Conclusion Eosinophilic meningitis is a manifestation of an underlying illness. It is a syndrome with varied etiologies, including parasitic infections. While rare, the worldwide incidence of these organisms should make a clinician have a high index of suspicion. Presence of persistent headache and eosinophilia in travelers coming from developing countries or residents of Asia should raise the index of suspicion for eosinophilic meningitis due to parasites (Leone 2007, Kirsh 2008). A thorough travel and food history is thus should be performed on all patients with eosinophilic meningitis. After infectious diseases, especially parasitic diseases have been ruled out, a search for an underlying hematological disease by examination of peripheral blood smear and bone marrow aspiration is indicated if infection cannot be confirmed and if no evidence of spinal cord or CSF manipulation has occurred. 4 If eosinophilic meningitis was found to be caused by a parasite, there is currently no vaccine is available to prevent this infection. As with any other form of parasitic disease, people exposed to sources of these infections should watch out for fresh produce that have been contaminated by snails, slugs or raccoon feces. Thorough cleaning however does not eliminate the larvae so caution in intake of these foods is important. Undercooked mollusks, prawns, fish and crabs should also be avoided. 5 Reading List 1. Almoujahed MO, et al. Coccidioidal meningitis: incidental diagnosis 3 y after ventriculoperitoneal shunt placement for hydrocephalus. Scand J Infect Dis. 2002;34(2):142-3. 2. Barry M, Thanassi W. Meningitis, Eosinophilic. Encyclopedia of the Neurological Sciences. p102-105. 3. Chan YC et al. Eosinophilic meningitis secondary to allergic Aspergillus sinusitis. J Allergy Clin Immunol - 01-JUL-2004; 114(1): 194-5 4. Chotmongkol V, Sawanyawisuth K, Thavornpitak Y. Corticosteroid for eosinophilic meningitis. Clin Infect Dis. 2000;31:660–2. 5. Chotmongkol V, Sawanpanitch K, Sawanyawisuth K, Louhawilai S, Limpawattana P. Treatment of eosinophilic meningitis with a combination of prednisolone and mebendazole. Am J Trop Med Hyg 2006;74:1122-1124. 6. Chotmongkol. V et al. SE Asian J Trop Med Pub Health. 2004; 35:172-174. 7. Eosinophilic meningitis in a neonate. Clin Pediatr Eosinophilic Meningitis. Infectious Disease Epidemiology Section. Office of Public Health, Louisiana Dept of Health & Hospitals. 8. Fulkerson DH et al. Cerebrospinal fluid eosinophilia in children with ventricular shunts. J Neurosurg Pediatr. 2008 Apr;1(4):288-95. 9. Hewett FA 2nd and Hendley JO. (Phila). 2002 May;41(4):269-71. Department of Pediatrics, University of Virginia Health Sciences Center, Charlottesville 22901, USA. 10. Kirsch S, Dekumyoy P, Loescher T, Roman L, Haberl. A Case of Eosinophilic Meningitis in Germany. J Neurol (2008) 255:1102–1103. DOI 10.1007/s00415-008-0846-2. 11. Sebastiano Leone S, De Marco M, Ghirga P, Nicastri E, Esposito M, Narciso P. Eosinophilic Meningitis in a Returned Traveler From Santo Domingo: Case Report and Review. Journal of Travel Medicine. Vol 14 Is 6, p407 – 410. 12. Slom TJ et al. An outbreak of eosinophilic meningitis caused by Angiostrongylus cantonensis in travelers returning from the Caribbean. N Engl J Med. 2002;346(9):668-75. 13. Weller P, "Chapter 209. Trichinella and Other Tissue Nematodes" (Chapter). Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J: Harrison's Principles of Internal Medicine, 17th Edition: http://www.accessmedicine.com/content.aspx?aID=2896618. 6 Table: Causes of Eosinophilic Meningitis( Barry and Thanassi, 2003) Parasites: Common - Angiostrongylus cantonensis - Gnasthoma spinigerum - Baylisascaris procyonis Less Common - Taenia solium(neurocysticercosis) - Schistosomiasis(ectopic CNS/spinal) - Paragonimiasis(ectopic CNS/spinal) - Toxocariasis(migrating larvae) - Strongyloidiasis(migrating larvae) - Onchocerciasis - Ascariasis(migrating larvae) - Echinococcosis(ectopic CNS cysts) - Trichinosis - Fascioliasis - Coenurosis(ectopic CNS cysts) Nonparasitic infectious etiologies - Coccidiomycosis - Cryptococcosis(rare) - Myiasis (ectopic CNS penetration) - Other bacterial, rickettsial, or viral meningitis (very rare with low-level CSF eosinophilia) - Meningeal tuberculosis (rare) Drugs - Antimicrobials: Ciprofloxacin, Cotrimoxazole - Intraventricular Gentamicin/Vancomycin - NSAIDS, Ibuprofen 7 Myeloproliferative diseases - Hypereosinophilic syndrome - Hodgkin’s disease - Leukemia - Lymphoma - Disseminated glioblastoma - Paraneoplastic syndrome associated with lung cancer Procedures involving the spinal cord and CSF - Contrast myelography - Ventriculoperitoneal shunts Miscellaneous conditions - Sarcoidosis - Eosinophilic granuloma - Multiple sclerosis - Allergic Aspergillus Sinusitis(Chan et al 2004) 8