Cerebrospinal fluid
advertisement

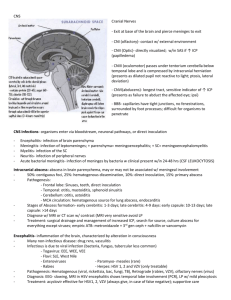
Inflammations & infections of CNS and Cerebrospinal fluid Dr Aarathi Rau Infections of the CNS Meninges,brain,both Meningitis Pachymeningitis:Epidural and subdural infections Leptomeningitis-Subarachnoid Brain Cerebral abscess-focal inflammation Encephalitis-diffuse inflammation Formation,circulation,function of CSF Formation-500 ml/day Ultrafilteration & secretion –choroid plexus, ependymal lining of ventricles Circulation: ventricular system-foraminasubarachnoid space Function of CSF Protects, lubricates the brain Provides nutrients, removes waste 90-150 ml adult 10-60 ml in newborn Blood brain barrier – homeostasis;electrolytes Urea,glucose ,protein,creatinine passively along concentration gradient Normal CSF Thin, colourless, clear fluid Pressure 90-180mm WATER (10-100 neonates) 0-5 WBC’s /mm3 (neonates 0-30/ mm3 ) Lymphocytes & monocytes Occasional ependymal or choroid plexus cells Protein 15-45mg/dl Glucose 50-80mg/dl Chloride 113-130 mEq/L Sterile Meningitis Def: inflammatory process of the leptomeninges & CSF within the subarachnoid space Meningoencephalitis =+inflammation of brain parenchyma Classification Acute Aseptic Chronic Pyogenic meningitis pathogenesis Blood borne Direct-sinuses,mastoid,middle ear,dural venous sinuses,direct trauma,fracture skull Neonates:E Coli,Strep pneumoniae, Adolescents: N Meningitides, H influenzae Adults: N Meningitides, Strep pneumoniae type 3 Elderly :Listeria monocytogenes,strep pneumoniae type 3 Clinical features General Headache,altered Neck stiffness consciousness,vomiting Gross Pus in the subarachnoid space Meningeal vessels engorged Location-Pneumococcal-convexities Tracks along vessels, ventriculitis Microscopy PMN in SA space,> meningial vessels Thrombosis of superficial vessels & Cerebral ischemic damage CSF in Pyogenic Meningitis Increased pressure Purulent/cloudy ↑protein ↓ glucose Leucocytosis Neutrophils ++ Gram stain Culture Sequele Resolution Cerebritis,hemorrhagic Fibrosing infarction of brain meningitis Hydrocephalus Chronic adhesive arachnoiditis (Aseptic)Lymphocytic meningitis Viral usually (Coxsackie, EBV, ECHO) Less fulminant than bacterial Usually recover Few specimens Mild lymphocytic infiltrate of the meninges CSF in Viral meningitis Clear appearance Mild pleocytosis Lymphocytes + Protein↑ Glucose –WNL Culture sterile Virological exam-Coxsackie, EBV, ECHO Tubercular meningitis Hematogenic spread Gross:Thickening & opacity of leptomeniges Basal meningitis, encasing cranial N’s Discrete white granules on the meninges +/ Microscopy-granulomas, lymphoplasmacytic infiltrate Obliterative endarteritis Tubercular meningitis Sequele-adhesive, fibrous, arachnoiditis, Hydrocephalus Infarction following endarteritis Tuberculoma-intraparenchymal CSF in Tubercular meningitis Moderate pleocytosis Lymphocytosis (early –neutrophilia) Glucose ↓ (< pyogenic ) Protein +++ Cobweb appearance /clot AFB, culture, PCR. Atypical mycobacteria Syphilis Meningovascular neurosyphilis:Chronic meningitis Base of brain Cerebral convexities+/-, Spinal leptomeninges Cerebral Gumma Microscopy-endarteritis obliterans (Heubner arteritis) with plasma cell cuffing Cerebral abscess Def: Focal inflammation of the parenchyma of the brain Routes of infection Secondary to meningitis Local spread (middle ear,mastoid) Hematogenous-BE,cyanotic heart disease,bronchiectasis Trauma GROSS MORPHOLOGY Ill defined local swelling preferred sites frontal lobe,parietal lobe cerebellum depending on aetiology C/S fibrous capsule soft central liquefactive necrosis surrounding oedema Morphology Microscopy Abscess containing necrosis surrounded by granulation tissue ,fibrosis & gliosis Microbiology:mixed bacteria + anaerobes Encephalitis Diffuse brain inflammation Causative org: viral,rickettsia,bacteria (listeria) Death of neurons HIV associated Neurologic disorders Primary: CNS Primary HIV encephalopathies Giant cell encephalitis, leucoencepalopathy, gray matter disease Myelopathy Lymphocytic Meningitis-seroconversion PNS Skeletal muscle myositis HIV associated Neurologic disorders Associated with immune supressed condition Opportunistic infections Lymphoma CSF in AIDS Aseptic HIV meningitis-lymphocytic meningitis Infections M. tuberculosis less reactive Mycobacterium avium intracellulare Cryptococci Neurosyphilis Malignancies OTHER INFECTIONS Prion disease (CJD) Fungal infections Parasitic infections malaria, toxoplasmosis,Echinococcus,cysticercosis Typical Cerebrospinal Fluid Findings in Various Types of Meningitis Test Bacterial Viral Fungal Tubercular Opening pressure Elevated Usually normal Variable Variable White blood cell count >=1,000 per mm3 <100 per mm3 Variable Variable Cell differential Predominance Predominance of PMNs of lymphocytes Predominance Predominance of of lymphocytes lymphocytes Protein Mild to marked elevation Normal to elevated Elevated Elevated CSF-to-serum glucose ratio Normal to marked decrease Usually normal Low Low Intracranial hemorrhage Intracerebral hematoma-associated with hypertension,(AV malformations,tumour ) Subarachnoid hemorrhage Any age group Associated with rupture of Berry aneurysm Hemorrhagic tap Traumatic Clear supernatant Clearing from tube 1 to 3 Fresh RBC’s Subarachnoid hemorrhage Xanthochromia>4 hrs upto 2-4 weeks Same appearance in 1,2 & 3 Crenated RBC’s Lumbar puncture Diagnostic Meningitis;bacterial,TB,fungal, viral *,syphilis encephalitis Guillain Barre Syndrome Matastasis lymphoma,leukaemia,breast,lung Haemorrhage Any disorder affecting the nervous system! Therapeutic Administer dye for imaging studies Administer medications eg CT,anaesthesia Processing Method of collection 3 sterile bottles Biochemistry & immunology-blood glucose Microbiology Cell count,cytology Send QUICKLY