oshu-case - UCSD Department of Pediatrics
advertisement

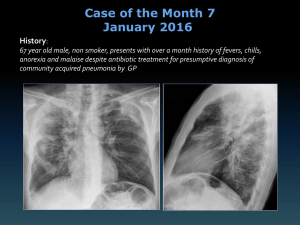
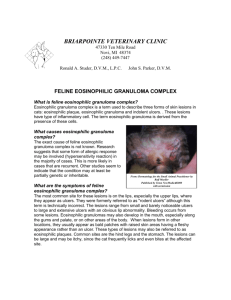
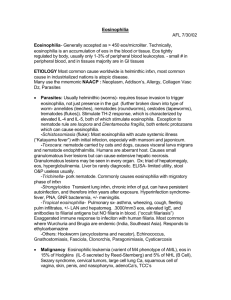
A Challenging Clinical Case Holger Link, MD Liz Levine, M.D. PGY 2 Doernbecher Pediatric Pulmonary Program Disclosures None HPI 16 yo teenage boy presented with worsening wheezing, coughing, shortness of breath. 1 mo PTA: Fever, coughing, dx with walking PNA, treated with Azithromycin for 5 days with some improvement Cough gradually worsened with acute onset of SOB, wheezing. In ED SpO2 82’%. Tx with Duoneb, Dexamethasone, and transferred to DCH PICU. Further history: PMHx: Term infant, no hospitalizations prior to those mentioned. No surgeries. No atopy or hx of asthma. 2 episodes of PNA 2 years ago, both tx as an outpatient. Fully vaccinated. Fam Hx: No asthma, eczema, allergies. No other respiratory problems. Social: Junior in HS, quite active usually, plays football. Smokes MJ “few times per month” over past 2 yrs, denies all other drug use, including tobacco. Has been sexually active in past, not in last 8-9 mo. Travel: none out of Oregon in last 2 years Animals/Exposures: Denies inhaled dust, smoke, chemicals, no pets, birds, farm, or other animal exposure Meds: Albuterol MDI prn Allergies: NKA PICU Needing oygen, continuous nebs, mag sulfate, IV steroids, bronchodilators gradually weaned, transferred to floor after 2 days. Pulm consult: recommended CT given unusual presentation for asthma. **Had received 2 days of IV steroids at time of CT CXR day of admission Inspiratory chest CT Inspiratory chest CT Expiratory chest CT Expiratory chest CT Expiratory chest CT Clinical course + tests CT initial read: significant amount of air trapping, GG opacities and concern for a potential bronchiolitis obliterans w/cryptogenic pneumonia. Workup: AFB neg, Legionella neg, HIV neg, Resp Viral panel neg, Hypersensitivity Pneumonitis panel neg, Mycoplasma pneumoniae IgM neg, IgG positive. He improved from a respiratory standpoint. PFT’s with FEV1 102% day of discharge Discharged home with a tapering course of oral prednisone, albuterol prn and azithromycin. CBC + Diff After discharge: Continued to improved while on tapering course of Prednisone, just about back to baseline F/up in Pulm clinic 3 weeks later: doing well, excellent PFT's (FEV1 of 124%), and his azithromycin was discontinued However… After finishing course of steroids: increasing cough, using albuterol more often, no other cold-like sx. Also notes occasional night sweats, weight loss of 15-20 lbs over past few months. Cough worsens, increasing SOB, wheezing, chest pain. Re-admitted to hospital 2 months after initial PICU admission. Physical exam VS: Temp 36.8 °C BP 112/69, HR 98, RR 24, SpO2 94% Wt 60.6 kg Gen: awake, alert, NAD HEENT, CV, Abd, Neuro: normal Resp: Non-labored, no retractions or nasal flaring, currently on 0.5L. Chest shape is normal. Auscultation of lungs: slight tachypnea, prolonged expiration with wheezing (both insp and exp) in all lung fields. Ext: WWP, no clubbing. Skin: no rashes, several linear striae noted over lower back. On admission: Initially required 2-5 L O2 via NC to maintain sat’s. Albuterol every 2-4 hrs was helping some. Labs: WBC: 22.8 (Poly 20, lymph 12, mono 4, Eos 64%) Lytes, LFT’s ,H/H, plt wnl ESR 25, CRP <0.5 UDS: +Cannabinoids, all others negative Imaging: CXR: airway thickening, hyperinflation Pulmonology consult requested CXR second admission Bronchoscopy results + course Labs: IgE elevated at 867, rest of immunoglobulins wnl. Bronchoscopy: Mucosa: mild erythema Secretions: thick whitish-yellowish secretions in bilateral airways. No blood. Eosinophilia of 91% on BAL Started on Solumedrol x 1 day, followed by Prednisone 60 mg daily On discharge also started on ICS BAL findings BAL histology Pulmonary Eosinophilic Syndromes Primary Secondary Acute eosinophilic PNA Asthma Chronic eosinophilic PNA ABPA Churg-Strauss Syndrome Bronchocentric granulomatosis Hypereosinophilic syndrome Collagen vascular diseases Eosinophilic granuloma Drug/toxin reaction Infection: parasite (Loeffler’s syndrome), helminthic, TB, coccidiodes, others BOOP Hypersensitivity pneumonitis Malignancies Chronic Eosinophilic Pneumonia Rare disorder of unclear etiology resulting in insidious onset of respiratory symptoms accompanied by pulmonary consolidation and accumulation of large numbers of eosinophils in the lungs, blood and in BAL fluid. Diagnosis Based on history, imaging, eosinophilia Proposed criteria: 1) Resp symptoms >2 weeks 2) Alveolar eosinophilia (>25%, esp >40%) or blood eosinophilia (>1000 eos/mm3) 3) Pulmonary infiltrates on CXR, usually peripheral 4) Exclusion of other causes of eosinophilic lung disease Etiology Unknown initiating stimulus/insult results in accumulation of eosinophils in the lungs TH2 lymphocytes activatedIL-5, important role in recruiting eosinophils, and inhibiting their apoptosis. Other chemokines involved: elevated TARC (thymus and activation regulated chemokine), eotaxin and RANTES act as other chemoattractants of eosinophils Epidemiology: Female nonsmokers, mean age of 45 yrs Female/male ratio 2.1/1 in 1 review article Age range 18 to 80 yrs in same article Most patients do have asthma (52%), atopy in general 63-75% Clinical Presentation: Gradual , subacute onset of symptoms which can include: Respiratory: cough (+/- productive), wheezing, SOB, chest pain Systemic: low grade fevers, weight loss, night sweats, malaise Acute respiratory failure, significant hypoxemia seen in acute eosinophilic pneumonia Rarely, arthralgias, neuropathy, skin findings, GI sx reported Physical findings On exam, non specific findings Expiratory wheezing in 50% Occasionally inspiratory crackles Labs Peripheral eosinophilia usually found first 90% patients had >30% eosinophils Elevated inflammatory markers Elevated IgE PFT’s: inconsistent 1/3 no abnormality, 1/3 restrictive, 1/3 obstructive BAL fluid: >25% eosinophils Mean close to 60% Normal <2% Imaging: CXR “Photographic negative of pulmonary edema” (though <25% with this finding) Bilateral peripheral opacities, often in upper lobes Infiltrates can range from ground-glass, migratory to dense consolidation Imaging: CT May help detect small ground glass opacities not seen on film Study of high resolution CT scan in 81 patients, physicians unable to distinguish between CEP and bronchiolitis obliterans Treatment: Spontaneous remission in 10% Oral corticosteroids: prednisone 0.3-1 mg/kg/day Usually have dramatic response with cessation of symptoms Marked decrease in peripheral eosinophilia (and BAL fluid) Recommended course: gradual taper between 6-12 months, though some suggest trying 6-8 weeks Prognosis: >50% relapse, requiring prolonged courses of CS for months-years Aside from potential for relapse after cessation of steroids, general prognosis is quite good with full resolution of symptoms and no long-term sequelae Individual reports of pulmonary fibrosis Rare cases have been associated with cutaneous T cell lymphoma, sarcoidosis, Churg-strauss Final twist… “Oil red O stain indicates a 95% positivity for lipid laden macrophages. There are numerous Charcot-Leyden eosinophilic crystals and a few scattered benign goblet cells suggestive of an asthma-like respiratory process.” No hx of reflux, choking, GERD symptoms After this obtained normal MBSS Stool O&P obtained, but unable to be processed due to presence of barium BAL histology References: Alam, M. and N. Burki. Chronic eosinophilic pneumonia: a review. Southern Medical Journal 2007, 100: 49-53. Cakir, C. et al. Chronic eosinophilic pneumonia with mucous plugs in a child. Pediatric Pulmonology 2010, 45: 1040-1042. Katz, U. and Y. Shoeneld. Pulmonary eosinophilia. Clinic Rev Allergy Immunol, 2008, 34:367-371. Uptodate Weschler, M. Pulmonary eosinophilic syndromes. Immonol Allergy Clin N Am, 2007, 27: 477-492. Wubbel, C. et al. Chronic eosinophilic pneumonia: a case report and national survey. Chest 2003, 123; 1763-1766.